
Novel Hematological Parameters in the Assessment of the Extent of Cardiac Implantable Electronic Device-Related Infections

 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Study Group
2.2. Definitions
2.3. Laboratory Markers
2.4. Statistical Analysis
2.5. Approval of the Bioethics Committee
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khaloo, P.; Uzomah, U.A.; Shaqdan, A.; Ledesma, P.A.; Galvin, J.; Ptaszek, L.M.; Ruskin, J.N. Outcomes of Patients Hospitalized With Cardiovascular Implantable Electronic Device-Related Infective Endocarditis, Prosthetic Valve Endocarditis, and Native Valve Endocarditis: A Nationwide Study, 2003 to 2017. J. Am. Heart Assoc. 2022, 11, e025600. [Google Scholar] [CrossRef] [PubMed]
- Pokorney, S.D.; Zepel, L.; Greiner, M.A.; Fowler, V.G., Jr.; Black-Maier, E.; Lewis, R.K.; Hegland, D.D.; Granger, C.B.; Epstein, L.M.; Carrillo, R.G.; et al. Lead Extraction and Mortality Among Patients with Cardiac Implanted Electronic Device Infection. JAMA Cardiol. 2023, 18, e233379. [Google Scholar] [CrossRef] [PubMed]
- Mateos Gaitán, R.; Boix-Palop, L.; Muñoz García, P.; Mestres, C.A.; Marín Arriaza, M.; Pedraz Prieto, Á.; de Alarcón Gonzalez, A.; Gutiérrez Carretero, E.; Hernández Meneses, M.; Goenaga Sánchez, M.Á.; et al. Infective endocarditis in patients with cardiac implantable electronic devices: A nationwide study. Europace 2020, 22, 1062–1070. [Google Scholar] [CrossRef] [PubMed]
- Sandoe, J.A.; Barlow, G.; Chambers, J.B.; Gammage, M.; Guleri, A.; Howard, P.; Olson, E.; Perry, J.D.; Prendergast, B.D.; Spry, M.J.; et al. Report of a joint Working Party project on behalf of the BritishSociety for Antimicrobial Chemotherapy (BSAC, host organization), BritishHeart Rhythm Society (BHRS), British Cardiovascular Society (BCS), BritishHeart Valve Society (BHVS) and British Society for Echocardiography (BSE). J. Antimicrob. Chemother. 2015, 70, 325–359. [Google Scholar] [PubMed]
- Polewczyk, A.; Jacheć, W.; Polewczyk, A.M.; Tomasik, A.; Janion, M.; Kutarski, A. Infectious complications in patients with cardiac implantable electronic devices: Risk factors, prevention, and prognosis. Pol. Arch. Intern. Med. 2017, 127, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Uslan, D.Z.; Sohail, M.R.; St Sauver, J.L.; Friedman, P.A.; Hayes, D.L.; Stoner, S.M.; Wilson, W.R.; Steckelberg, J.M.; Baddour, L.M. Permanent pacemaker and implantable cardioverter defibrillator infection: A population-based study. Arch. Intern. Med. 2007, 167, 669–675. [Google Scholar] [CrossRef]
- Polewczyk, A.; Janion, M.; Podlaski, R.; Kutarski, A. Clinical manifestations of lead-dependent infective endocarditis: Analysis of 414 cases. Eur. J. Clin. Microbiol. Infect. Dis. 2014, 33, 1601–1608. [Google Scholar] [CrossRef]
- Wyllie, D.H.; Bowler, I.C.; Peto, T.E. Relation between lymphopenia and bacteraemia in UK adults with medical emergencies. J. Clin. Pathol. 2004, 57, 950–955. [Google Scholar] [CrossRef]
- Meshaal, M.S.; Nagi, A.; Eldamaty, A.; Elnaggar, W.; Gaber, M.; Rizk, H. Neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) as independent predictors of outcome in infective endocarditis (IE). Egypt. Heart J. 2019, 71, 13. [Google Scholar] [CrossRef]
- Blomström-Lundqvist, C.; Traykov, V.; Erba, P.A.; Burri, H.; Nielsen, J.C.; Bongiorni, M.G.; Poole, J.; Boriani, G.; Costa, R.; Deharo, J.C.; et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections—Endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID), and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 41, 2012–2032. [Google Scholar]
- Nowosielecka, D.; Jacheć, W.; Polewczyk, A.; Tułecki, Ł.; Kleinrok, A.; Kutarski, A. The role of transesophageal echocardiography in predicting technical problems and complications of transvenous lead extractions procedures. Clin. Cardiol. 2021, 44, 1233–1242. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Ruegamer, T.; Brochhausen, C.; Menhart, K.; Hiergeist, A.; Kraemer, L.; Hellwig, D.; Maier, L.S.; Schmid, C.; Jantsch, J.; et al. Infective Endocarditis: Predictive Factors for Diagnosis and Mortality in Surgically Treated Patients. J. Cardiovasc. Dev. Dis. 2022, 9, 467. [Google Scholar] [CrossRef] [PubMed]
- Neul-Bom, Y.; Choonhee, S.; Soo-Jung, U. Role of the Neutrophil-Lymphocyte Count Ratio in the Differential Diagnosis between Pulmonary Tuberculosis and Bacterial Community-Acquired Pneumonia. Ann. Lab. Med. 2013, 33, 105–110. [Google Scholar]
- Ishizuka, M.; Shimizu, T.; Kubota, K. Neutrophil-to-Lymphocyte Ratio Has a Close Association With Gangrenous Appendicitis in Patients Undergoing Appendectomy. Int. Surg. 2012, 97, 299–304. [Google Scholar] [CrossRef]
- Kahramanca, S.; Ozgehan, G.; Seker, D.; Gökce, E.I.; Seker, G.; Tunç, G.; Küçükpınar, T.; Kargıcı, H. Neutrophil-to-lymphocyte ratio as a predictor of acute appendicitis. Ulus. Travma Acil Cerrahi Derg 2014, 20, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Kekilli, M.; Tanoglu, A.; Sakin, Y.S.; Kurt, M.; Ocal, S.; Bagci, S. Is the neutrophil to lymphocyte ratio associated with liver fibrosis in patients with chronic hepatitis B? World J. Gastroenterol. 2015, 21, 5575. [Google Scholar] [CrossRef] [PubMed]
- de Jager, C.P.; van Wijk, P.T.; Mathoera, R.B.; de Jongh-Leuvenink, J.; van der Poll, T.; Wever, P.C. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit. Care 2010, 14, R192. [Google Scholar] [CrossRef]
- Gharebaghi, N.; ValizadeHasanloei, M.A.; MedizadehKhalifani, A.; Pakzad, S.; Lahooti, D. Neutrophil-to-lymphocyte ratio in patients with gram-negative sepsis admitted to intensive care unit. Anaesthesiol. Intensive Ther. 2019, 51, 11–16. [Google Scholar] [CrossRef]
- Naess, A.; Nilssen, S.S.; Mo, R.; Eide, G.E.; Sjursen, H. Role of neutrophil to lymphocyte and monocyte to lymphocyte ratios in the diagnosis of bacterial infection in patients with fever. Infection 2017, 45, 299–307. [Google Scholar] [CrossRef]
- Afari, M.E.; Bhat, T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: An update. Expert Rev. Cardiovasc. Ther. 2016, 14, 573–577. [Google Scholar] [CrossRef]
- Hong, D.; Choi, K.H.; Song, Y.B.; Lee, J.M.; Park, T.K.; Yang, J.H.; Hahn, J.Y.; Choi, J.H.; Choi, S.H.; Kim, S.M.; et al. Prognostic implications of post-percutaneous coronary intervention neutrophil-to-lymphocyte ratio on infarct size and clinical outcomes in patients with acute myocardial infarction. Sci. Rep. 2019, 9, 9646. [Google Scholar] [CrossRef]
- Lo, R.; D’Anca, M.; Cohen, T.; Kerwin, T. Incidence and prognosis of pacemaker lead-associated masses: A study of 1569 transesophageal echocardiograms. J. Invasive Cardiol. 2006, 18, 599–601. [Google Scholar]
- Downey, B.C.; Juselius, W.E.; Pandian, N.G.; Downey, B.C.; Juselius, W.E.; Pandian, N.G.; Estes, N.M.; Link, M.S. Incidence and significance of pacemaker and implantable cardioverter-defibrillator lead masses discovered during transesophageal echocardiography. Pacing Clin. Electrophysiol. 2011, 34, 679–683. [Google Scholar] [CrossRef]
- Dundar, C.; Tigen, K.; Tanalp, C.; Izgi, A.; Karaahmet, T.; Cevik, C.; Erkol, A.; Oduncu, V.; Kirma, C. The prevalence of echocardiographic accretions on the leads of patients with permanent pacemakers. J. Am. Soc. Echocardiogr. 2011, 24, 803–807. [Google Scholar] [CrossRef]
- Golzio, P.G.; Errigo, D.; Peyracchia, M.; Gallo, E.; Frea, S.; Castagno, D.; Budano, C.; Giustetto, C.; Rinaldi, M. Prevalence and prognosis of lead masses in patients with cardiac implantable electronic devices without infection. J. Cardiovasc. Med. 2019, 20, 372–378. [Google Scholar] [CrossRef]
- Kołodzińska, A.; Kutarski, A.; Koperski, Ł.; Grabowski, M.; Małecka, B.; Opolski, G. Differences in encapsulating lead tissue in patients who underwent transvenous lead removal. Europace 2012, 14, 994–1001. [Google Scholar] [CrossRef]
- Kolodzińska, K.; Kutarski, A.; Grabowski, M.; Jarzyna, I.; Małecka, B.; Opolski, G. Abrasions of the outer silicone insulation of endocardial leads in their intracardiac part: A new mechanism of lead-dependent endocarditis. Europace 2012, 14, 903–910. [Google Scholar] [CrossRef]
- Novak, M.; Dvorak, P.; Kamaryt, P.; Slana, B.; Lipoldova, J. Autopsy and clinical context in deceased patients with implanted pacemakers and defibrillators: Intracardiac findings near their leads and electrodes. Europace 2009, 11, 1510–1516. [Google Scholar] [CrossRef]
- Rodríguez-Alfonso, B.; Mitjavila Casanovas, M.; Castro Urda, V.; Cobo Marcos, M.; Sánchez Romero, I.; Ramos-Martínez, A. PET/CT with 18 F-FDG in suspected intracardiac device-related infections: Analysis of performance and diagnostic usefulness. Rev. Esp. Cardiol. 2021, 74, 238–246. [Google Scholar] [CrossRef]
- Erba, P.A.; Sollini, M.; Conti, U.; Bandera, F.; Tascini, C.; De Tommasi, S.M.; Zucchelli, G.; Doria, R.; Menichetti, F.; Bongiorni, M.G.; et al. Radiolabeled WBC scintigraphy in the diagnostic workup of patients with suspected device-related infections. JACC Cardiovasc. Imaging 2013, 6, 1075–1086. [Google Scholar] [CrossRef]
- Gürol, G.; Çiftci, İ.H.; Terizi, H.A.; Atasoy, A.R.; Ozbek, A.; Köroğlu, M. Are There Standardized Cutoff Values for Neutrophil-Lymphocyte Ratios in Bacteremia or Sepsis? J. Microbiol. Biotechnol. 2015, 25, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ye, L.J.; Wu, Y.; Shen, B.Z.; Zhang, F.; Qu, Q.; Qu, J. Neutrophil-Lymphocyte Ratio in Predicting Infective Endocarditis: A Case-Control Retrospective Study. Mediat. Inflamm. 2020, 2020, 8586418. [Google Scholar] [CrossRef]
- Bozbay, M.; Ugur, M.; Uyarel, H.; Cicek, G.; Koroglu, B.; Tusun, E.; Sunbul, M.; Murat, A.; Sari, I.; Eren, M. Neutrophil-to-lymphocyte ratio as a prognostic marker in infective endocarditis: In-hospital and long-term clinical results. J. Heart Valve Dis. 2014, 23, 617–623. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients n = 2909 | |
|---|---|
| Patient’s age during TLE [years] median (Q1–Q3) | 69 (59–77) |
| Patient’s age during first system implantation [years] median (Q1–Q3) | 61 (51–69) |
| Female (n, %) | 1340 (46.06) |
| LVEF median (Q1–Q3) | 54 (36.00–60.00) |
| Renal failure (any) (n, %) | 885 (28.70) |
| Diabetes type 2 (n, %) | 775 (26.64) |
| Carlson’s comorbidity index [number of points] median, (Q1–Q3) | 4.00 (2.00–6.00) |
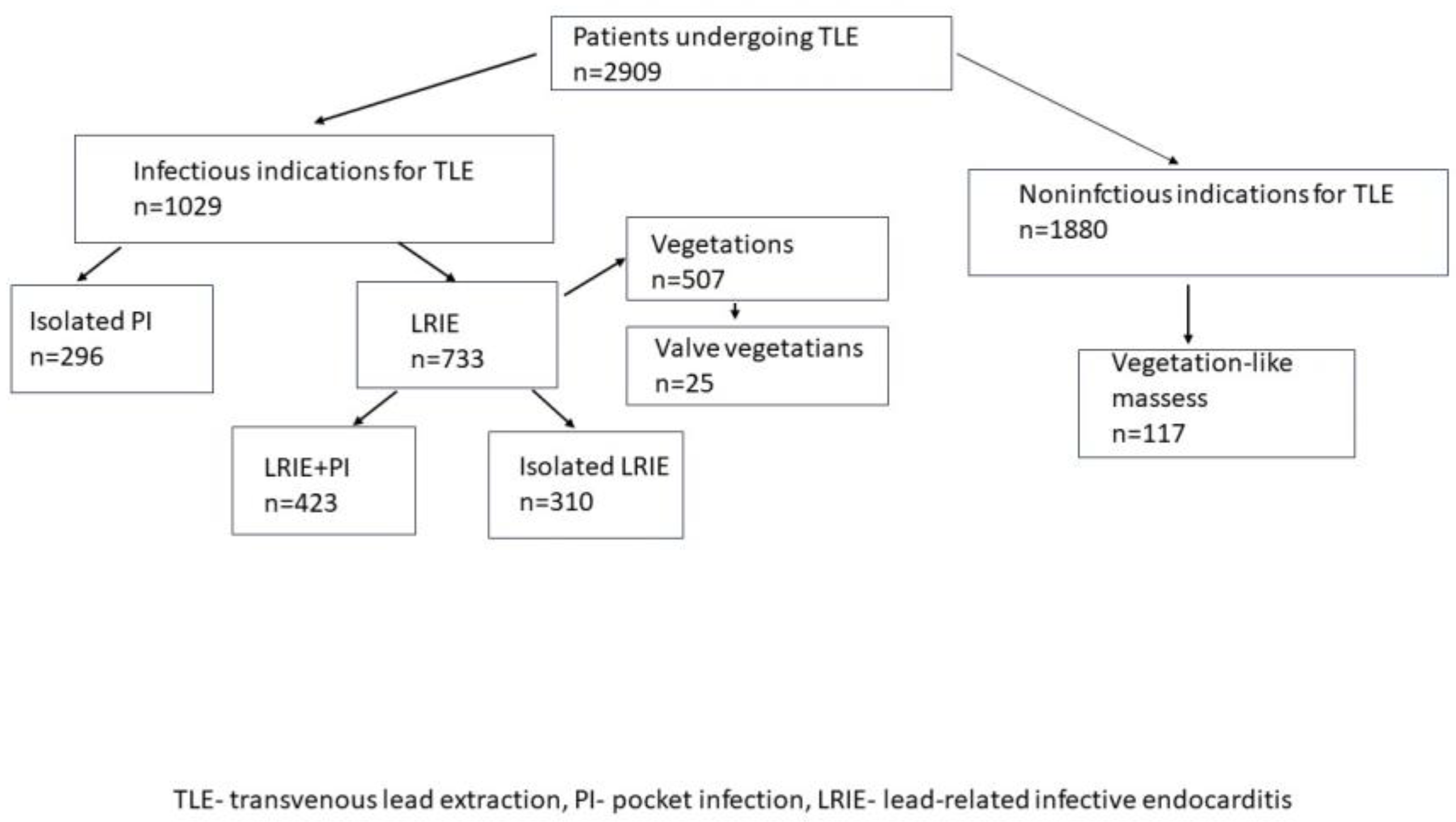
| Infectious indications for TLE (n, %) | 1029 (36.37) |
| Isolated pocket infections (n, %) | 296 (10.18) |
| LRIE (with and without pocket infection) (n, %) | 733 (25.20) |
| Positive blood cultures (n, %) | 273 (37.24%) |
| Vegetations (n, %) | 507 (17.40) |
| Non-infectious indications for TLE (n, %) | 1880 (64.63) |
| Vegetations-like masses (n, %) | 117 (4.02) |
| Infectious Indications for TLE n = 1029 | Non-Infectious Indications for TLE n = 1880 | p | |
|---|---|---|---|
| Patient’s age during TLE [years] median (Q1–Q3) | 70 (61–78) | 68 (58–76) | <0.001 |
| Patient’s age during first system implantation [years] median (Q1–Q3) | 63 (54–71) | 60 (48–68) | <0.001 |
| Sex (% of female patients) (n, %) | 306 (29.74) | 828 (44.04) | 0.001 |
| LVEF [%] median (Q1–Q3) | 50 (36.60) | 55 (35.–60.) | <0.001 |
| Renal failure (any) (n, %) | 271 (26.34) | 352 (18.72) | <0.001 |
| Diabetes type 2 (n, %) | 232 (22.55) | 332 (17.66) | <0.001 |
| Carlson’s comorbidity index [number of points] median, (Q1–Q3) | 4.00 (3.00–7.00) | 4.00 (2.00–5.50) | <0.001 |
| Hemoglobin (g/dL) (lowest) (mean, SD) | 12.5 (11.0–13.30) | 13.30 (12.10–14.40) | <0.001 |
| Hematocrit (%) (lowest) median (Q1–Q3) | 37.20 (33.00–40.90) | 39.90 (36.20–42.90) | <0.001 |
| Platelets/µL (lowest) median Q1–Q3) | 210.0 (164.0–272.0) | 197.0 (160.0–241.0) | 0.420 |
| Max WBC/µL (mean.SD) | 8185 (6600–10360) | 7210 (6070–8630) | 0.032 |
| Neutrophil count/uL (max) median (Q1–Q3) | 5.29 (3.90–7.40) | 4.30 (3.50–5.50) | 0.018 |
| Neutrophil% median (Q1–Q3) | 66.15 (58.60–74.00) | 62.90 (56.60–69.10) | 0.002 |
| Lymphocyte count/µL (max) median (Q1–Q3) | 1.60 (1.30–2.30) | 1.70 (1.30–2.19) | <0.001 |
| Lymphocyte% median (Q1–Q3) | 22.30 (16.20–29.10) | 24.60 (19.20–30.50) | <0.001 |
| Max ESR (mm/h) median (Q1–Q3) | 25.00 (1.00–50.00) | 11.00 (6.00–20.00) | <0.001 |
| Max CRP (mg/dL) median (Q1–Q3) | 17.57 (5.07–60.40) | 2.00 (0.60–7.17) | <0.001 |
| Max Procalcitonin (µg/L) median (Q1–Q3) | 0.10 (0.06–0.30) | 0.07 (0.04–0.125) | 0.154 |
| NLR median (Q1–Q3) | 3.07 (2.12–4.91) | 2.59 (1.86–3.57) | <0.001 |
| NLR% median (Q1–Q3) | 3.07 (2.12–4.84) | 2.57 (1.86–3.58) | <0.001 |
| NPR median (Q1–Q3) | 0.02 (0.02–0.04) | 0.01 (0.01–0.03) | 0.008 |
| LPR% median (Q1–Q3) | 0.10 (0.07–0.15) | 0.13 (0.10–0.17) | 0.001 |
| LPR (median IQR) | 0.01 (0.01–0.01) | 0.01 (0.01–0.01) | 0.003 |
| Parameters | Presence of Vegetation-Like Masses | Presence of Vegetations | p |
|---|---|---|---|
| Hemoglobin (mg/dL) (lowest) median (Q1–Q3) | 13.70 (11.90–14.70) | 11.90 (10.30–13.20) | <0.001 |
| Hematocrit (%) (lowest) median (Q1–Q3) | 40.20 (36.00–43.90) | 35.90 (31.20–39.70) | <0.001 |
| Platelets/µL (lowest) median (Q1–Q3) | 200.0 (163.0–252.0) | 215.0 (157.0–278.0) | 0.063 |
| Max WBC/µL median (Q1–Q3) | 7440 (6060–8640) | 8880 (7000–11,400) | <0.001 |
| Neutrophil count/µL (max) median (Q1–Q3) | 4.50 (3.56–5.54) | 5.70 (4.10–8.30) | <0.001 |
| Neutrophil% median (Q1–Q3) | 63.40 (54.80–69.80) | 67.70 (60.40–76.20) | <0.001 |
| Lymphocyte count/µL (max) median (Q1–Q3) | 1.65 (1.38–2.10) | 1.60 (1.20–2.20) | 0.927 |
| Lymphocyte% median (Q1–Q3) | 24.30 (18.70–31.90) | 19.80 (13.60–26.10) | <0.001 |
| Max ESR (mm/h) median (Q1–Q3) | 10.50 (5.00–19.50) | 30.00 (13.00–54.00) | <0.001 |
| Max CRP (mg/dL) median (Q1–Q3) | 3.00 (0.67–10.75) | 32.58 (9.30–90.00) | <0.001 |
| Max Procalcitonin (µg/L) median (Q1–Q3) | 0.05 (0.04–1.52) | 0.12(0.07–0.50) | 0.581 |
| NLR median (Q1–Q3) | 2.61 (1.72–3.67) | 3.37 (2.35–5.55) | <0.001 |
| NLR% median (Q1–Q3) | 2.61 (1.70–3.81) | 3.39 (2.37–5.56) | <0.001 |
| NPR median (Q1–Q3) | 0.02 (0.02–0.03) | 0.03 (0.02–0.04) | 0.008 |
| LPR% median (Q1–Q3) | 0.13 (0.09–0.18) | 0.09 (0.06–0.14) | 0.025 |
| LPR median (Q1–Q3) | 0.01(0.01–0.01) | 0.01 (0.01–0.01) | 0.937 |
| Parameters | LRIE | Isolated Pocket Infection | p |
|---|---|---|---|
| Hemoglobin (g/dL) (lowest) median (Q1–Q3) | 11.90 (10.50–13.30) | 13.20 (12.00–14.30) | <0.001 |
| Hematocrit (%) (lowest) median (Q1–Q3) | 33.95 (29.15–37.80) | 39.30 (35.90–42.10) | <0.001 |
| Platelets/µL (lowest) median (Q1–Q3) | 222.0 (159.0–293.0) | 202.00 (166.0–250.5) | 0.001 |
| Max WBC/µL (mean.SD) | 10,100 (7550–13,300) | 7370 (6280–8900) | <0.001 |
| Neutrophil count/µL (max) median (Q1–Q3) | 6.80 (4.65–9.50) | 4.40 (3.60–5.80) | <0.001 |
| Neutrophil % median (Q1–Q3) | 71.10 (63.75–78.45) | 62.75 (56.25–70.50) | <0.001 |
| Lymphocyte count/µL (max) median (Q1–Q3) | 1.60 (1.02–2.2.0) | 1.70 (1.30–2.29) | 0.93 |
| Lymphocyte% median (Q1–Q3) | 17.00(11.45–23.30) | 24.70 (18.80–30.30) | <0.001 |
| Max ESR (mm/h)median (Q1–Q3) | 44.50 (22.00–68.00) | 15.00 (8.00–30.00) | <0.001 |
| Max CRP (mg/dL) median (Q1–Q3) | 65.00 (24.70–120.7) | 7.30 (2.20–19.20) | <0.001 |
| Max Procalcitonin (µg/L) median (Q1–Q3) | 0.23 (0.10–1.53) | 0.08 (0.05–0.10) | 0.03 |
| NLR median (Q1–Q3) | 4.11 (2.72–6.98) | 2.55 (1.85–3.70) | <0.001 |
| NLR% median (Q1–Q3) | 4.24 (2.75–6.93) | 2.56 (1.87–3.73) | <0.001 |
| NPR median (Q1–Q3) | 0.03 (0.02–0.05) | 0.02 (0.02–0.03) | <0.001 |
| LPR% median (Q1–Q3) | 0.08 (0.05–0.11) | 0.12 (0.08–0.16) | 0.001 |
| LPR median (Q1–Q3) | 0.01 (0.00–0.01) | 0.01 (0.01–0.01) | 0.41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polewczyk, M.; Jacheć, W.; Szczęśniak-Stańczyk, D.; Polewczyk, A.; Tomaszewski, A.; Brzozowski, W.; Nowosielecka, D.; Kutarski, A. Novel Hematological Parameters in the Assessment of the Extent of Cardiac Implantable Electronic Device-Related Infections. J. Clin. Med. 2023, 12, 7498. https://doi.org/10.3390/jcm12237498
Polewczyk M, Jacheć W, Szczęśniak-Stańczyk D, Polewczyk A, Tomaszewski A, Brzozowski W, Nowosielecka D, Kutarski A. Novel Hematological Parameters in the Assessment of the Extent of Cardiac Implantable Electronic Device-Related Infections. Journal of Clinical Medicine. 2023; 12(23):7498. https://doi.org/10.3390/jcm12237498
Chicago/Turabian StylePolewczyk, Maciej, Wojciech Jacheć, Dorota Szczęśniak-Stańczyk, Anna Polewczyk, Andrzej Tomaszewski, Wojciech Brzozowski, Dorota Nowosielecka, and Andrzej Kutarski. 2023. "Novel Hematological Parameters in the Assessment of the Extent of Cardiac Implantable Electronic Device-Related Infections" Journal of Clinical Medicine 12, no. 23: 7498. https://doi.org/10.3390/jcm12237498
APA StylePolewczyk, M., Jacheć, W., Szczęśniak-Stańczyk, D., Polewczyk, A., Tomaszewski, A., Brzozowski, W., Nowosielecka, D., & Kutarski, A. (2023). Novel Hematological Parameters in the Assessment of the Extent of Cardiac Implantable Electronic Device-Related Infections. Journal of Clinical Medicine, 12(23), 7498. https://doi.org/10.3390/jcm12237498