

Comparison of Fibrinogen Concentrate and Cryoprecipitate on Major Thromboembolic Events after Living Donor Liver Transplantation

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
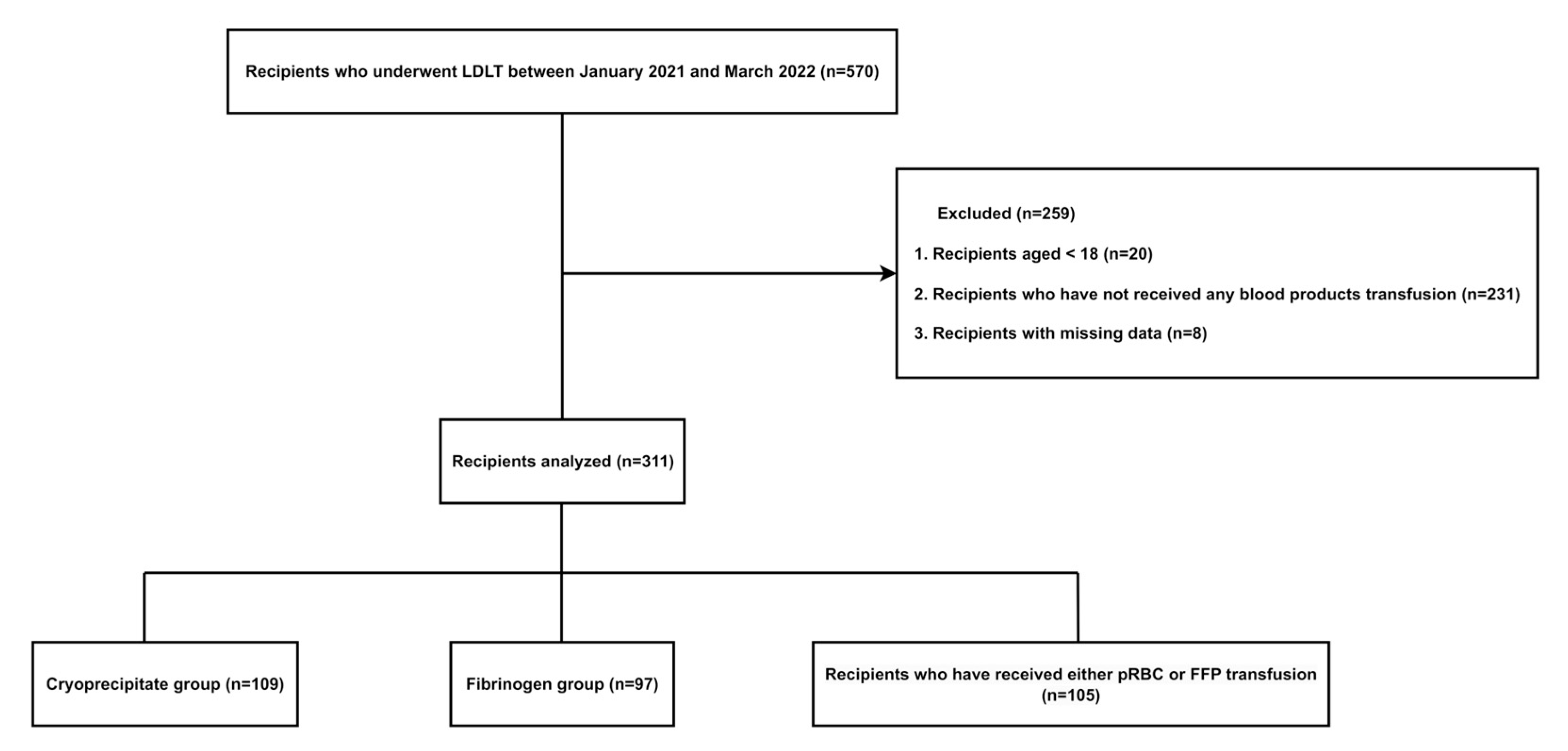
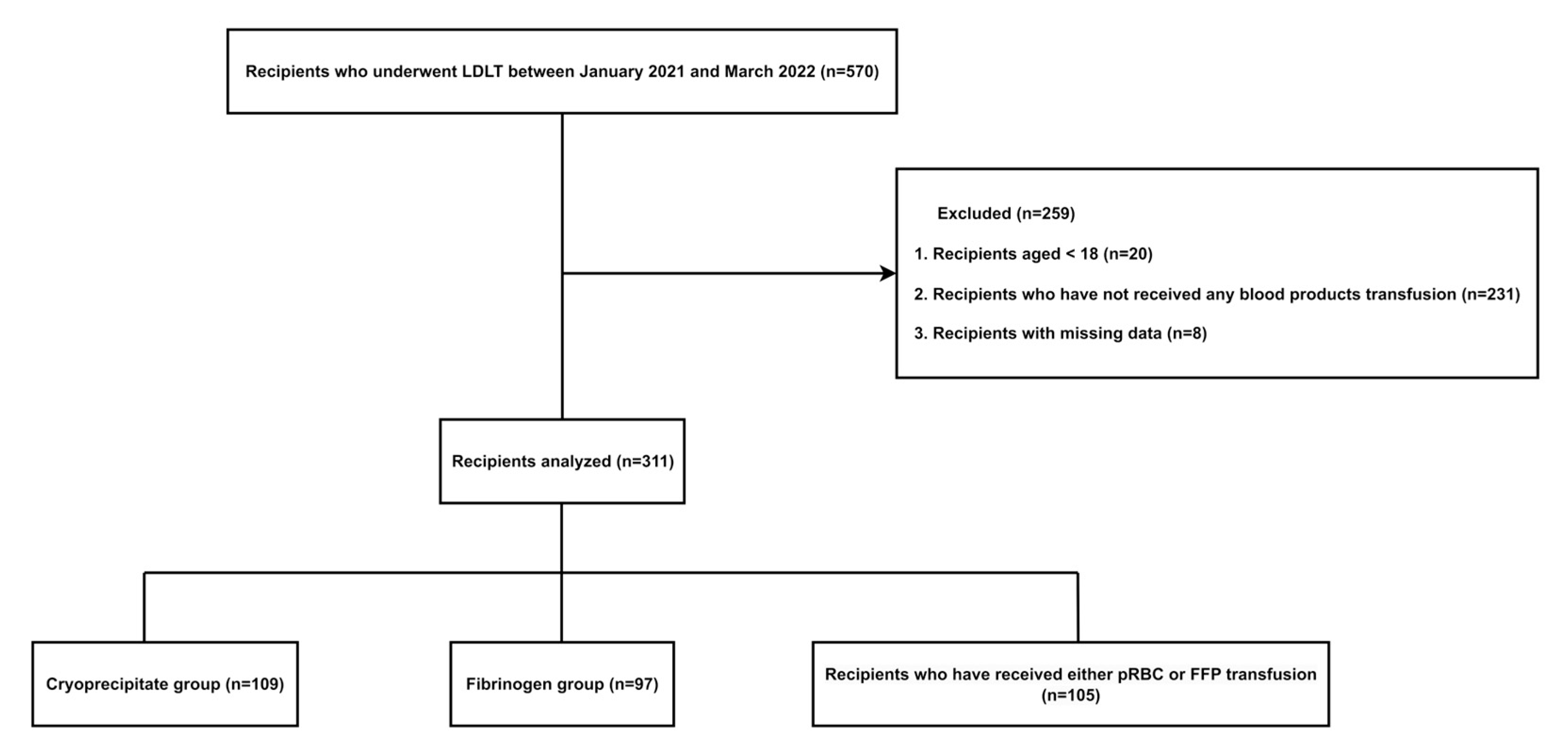
2.1. Study Design and Population
2.2. Data Collection
2.3. Transfusion Technique
2.4. Primary and Secondary Outcomes
2.5. Statistical Analysis
3. Results
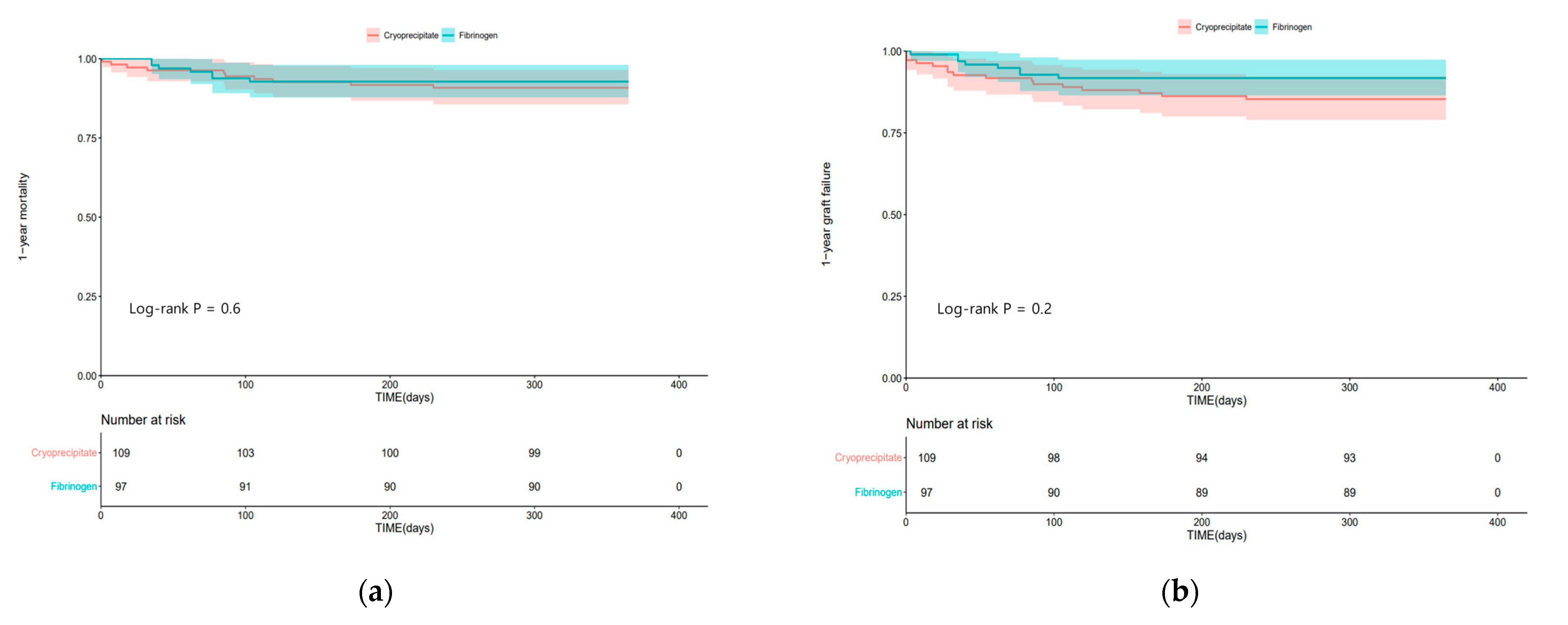
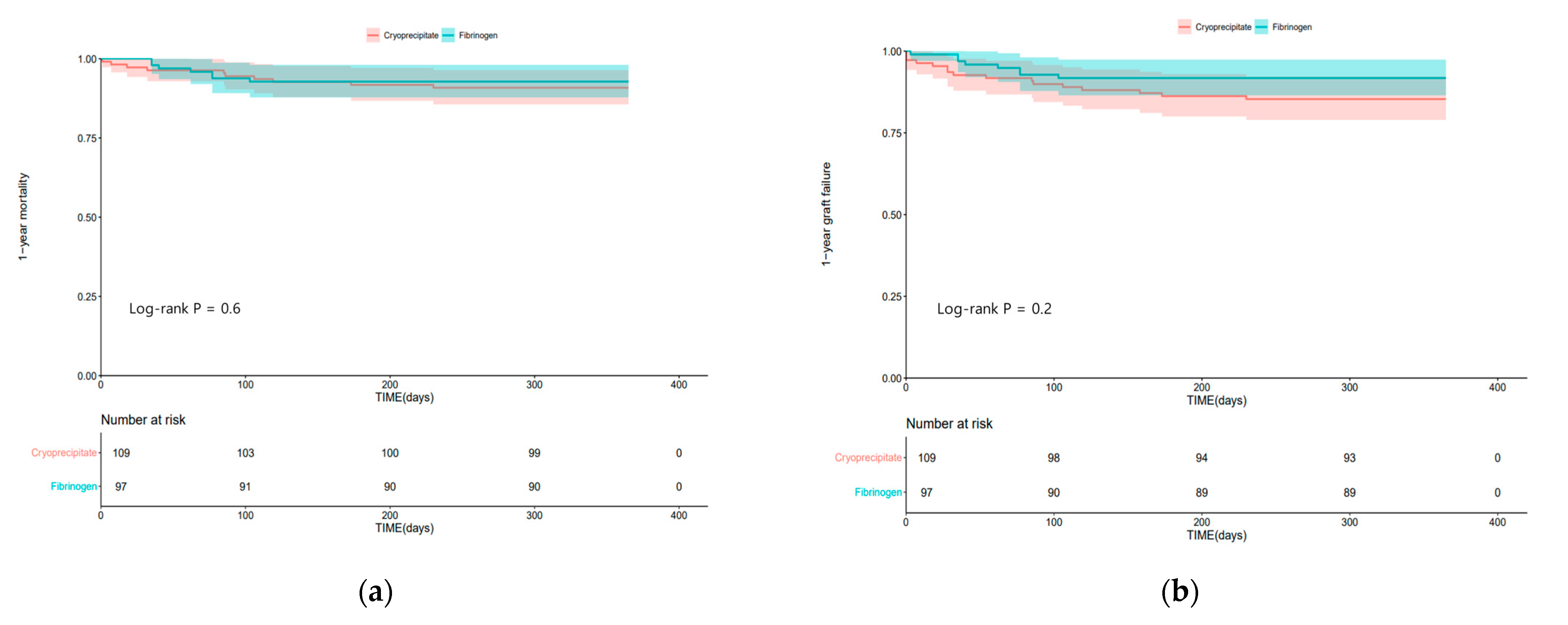
3.1. Primary Outcome
3.2. Secondary Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pandey, C.K.; Singh, A.; Kajal, K.; Dhankhar, M.; Tandon, M.; Pandey, V.K.; Karna, S.T. Intraoperative blood loss in orthotopic liver transplantation: The predictive factors. World J. Gastrointest. Surg. 2015, 7, 86–93. [Google Scholar] [CrossRef]
- Cleland, S.; Corredor, C.; Ye, J.J.; Srinivas, C.; McCluskey, S.A. Massive haemorrhage in liver transplantation: Consequences, prediction and management. World J. Transplant. 2016, 6, 291–305. [Google Scholar] [CrossRef]
- Levy, J.H.; Szlam, F.; Tanaka, K.A.; Sniecienski, R.M. Fibrinogen and hemostasis: A primary hemostatic target for the management of acquired bleeding. Anesth. Analg. 2012, 114, 261–274. [Google Scholar] [CrossRef] [PubMed]
- Chow, J.H.; Lee, K.; Abuelkasem, E.; Udekwu, O.R.; Tanaka, K.A. Coagulation Management During Liver Transplantation: Use of Fibrinogen Concentrate, Recombinant Activated Factor VII, Prothrombin Complex Concentrate, and Antifibrinolytics. Semin. Cardiothorac. Vasc. Anesth. 2018, 22, 164–173. [Google Scholar] [CrossRef] [PubMed]
- Callum, J.; Farkouh, M.E.; Scales, D.C.; Heddle, N.M.; Crowther, M.; Rao, V.; Hucke, H.P.; Carroll, J.; Grewal, D.; Brar, S.; et al. Effect of Fibrinogen Concentrate vs Cryoprecipitate on Blood Component Transfusion After Cardiac Surgery: The FIBRES Randomized Clinical Trial. JAMA 2019, 322, 1966–1976. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Buckley, C.; Gao, W.; Agopian, V.; Wray, C.; Steadman, R.H.; Xia, V.W. Major Thromboembolic Complications in Liver Transplantation: The Role of Rotational Thromboelastometry and Cryoprecipitate Transfusion. Transplantation 2021, 105, 1771–1777. [Google Scholar] [CrossRef]
- Mourad, M.M.; Liossis, C.; Gunson, B.K.; Mergental, H.; Isaac, J.; Muiesan, P.; Mirza, D.F.; Perera, M.T.; Bramhall, S.R. Etiology and management of hepatic artery thrombosis after adult liver transplantation. Liver Transpl. 2014, 20, 713–723. [Google Scholar] [CrossRef]
- Hensley, N.B.; Mazzeffi, M.A. Pro-Con Debate: Fibrinogen Concentrate or Cryoprecipitate for Treatment of Acquired Hypofibrinogenemia in Cardiac Surgical Patients. Anesth. Analg. 2021, 133, 19–28. [Google Scholar] [CrossRef]
- Galas, F.R.; de Almeida, J.P.; Fukushima, J.T.; Vincent, J.L.; Osawa, E.A.; Zeferino, S.; Camara, L.; Guimaraes, V.A.; Jatene, M.B.; Hajjar, L.A. Hemostatic effects of fibrinogen concentrate compared with cryoprecipitate in children after cardiac surgery: A randomized pilot trial. J. Thorac. Cardiovasc. Surg. 2014, 148, 1647–1655. [Google Scholar] [CrossRef]
- Tanaka, K.A.; Bader, S.O.; Gorlinger, K. Novel approaches in management of perioperative coagulopathy. Curr. Opin. Anaesthesiol. 2014, 27, 72–80. [Google Scholar] [CrossRef]
- Nascimento, B.; Goodnough, L.T.; Levy, J.H. Cryoprecipitate therapy. Br. J. Anaesth. 2014, 113, 922–934. [Google Scholar] [CrossRef] [PubMed]
- Curry, N.; Wong, H. Cryoprecipitate transfusion: Current perspectives. Int. J. Clin. Transfus. Med. 2016, 4, 89–97. [Google Scholar] [CrossRef]
- Kim, K.S.; Kwon, H.M.; Jung, K.W.; Sang, B.H.; Moon, Y.J.; Kim, B.; Jun, I.G.; Song, J.G.; Hwang, G.S. Markedly prolonged QTc interval in end-stage liver disease and risk of 30-day cardiovascular event after liver transplant. J. Gastroenterol. Hepatol. 2021, 36, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Lippi, G. Fibrinogen replacement therapy: A critical review of the literature. Blood Transfus. 2012, 10, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Kujovich, J.L. Hemostatic defects in end stage liver disease. Crit. Care Clin. 2005, 21, 563–587. [Google Scholar] [CrossRef] [PubMed]
- American Society of Anesthesiologists Task Force on Perioperative Blood Management. Practice guidelines for perioperative blood management: An updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Management. Anesthesiology 2015, 122, 241–275. [Google Scholar] [CrossRef]
- Jensen, N.H.; Stensballe, J.; Afshari, A. Comparing efficacy and safety of fibrinogen concentrate to cryoprecipitate in bleeding patients: A systematic review. Acta Anaesthesiol. Scand. 2016, 60, 1033–1042. [Google Scholar] [CrossRef]
- Whyte, C.S.; Rastogi, A.; Ferguson, E.; Donnarumma, M.; Mutch, N.J. The Efficacy of Fibrinogen Concentrates in Relation to Cryoprecipitate in Restoring Clot Integrity and Stability against Lysis. Int. J. Mol. Sci. 2022, 23, 2944. [Google Scholar] [CrossRef]
- Spahn, D.R.; Bouillon, B.; Cerny, V.; Duranteau, J.; Filipescu, D.; Hunt, B.J.; Komadina, R.; Maegele, M.; Nardi, G.; Riddez, L.; et al. The European guideline on management of major bleeding and coagulopathy following trauma: Fifth edition. Crit. Care 2019, 23, 98. [Google Scholar] [CrossRef]
- Sabate, A.; Dalmau, A. Fibrinogen: A Clinical Update on Liver Transplantation. Transplant. Proc. 2015, 47, 2925–2928. [Google Scholar] [CrossRef]
- Lisman, T.; Porte, R.J. Rebalanced hemostasis in patients with liver disease: Evidence and clinical consequences. Blood 2010, 116, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Caballero, M.; Sabate, A.; Gutierrez, R.; Beltran, J.; Perez, L.; Pujol, R.; Viguera, L.; Costa, M.; Reyes, R.; Martinez, A.; et al. Blood component requirements in liver transplantation: Effect of 2 thromboelastometry-guided strategies for bolus fibrinogen infusion-the TROMBOFIB randomized trial. J. Thromb. Haemost. 2023, 21, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Downey, L.A.; Andrews, J.; Hedlin, H.; Kamra, K.; McKenzie, E.D.; Hanley, F.L.; Williams, G.D.; Guzzetta, N.A. Fibrinogen Concentrate as an Alternative to Cryoprecipitate in a Postcardiopulmonary Transfusion Algorithm in Infants Undergoing Cardiac Surgery: A Prospective Randomized Controlled Trial. Anesth. Analg. 2020, 130, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Harrity, C.; Johnson, S.; Varadkar, S.; McMorrow, S.; Fanning, R.; Flynn, C.M.; JM, O.R.; Byrne, B.M. The efficacy of fibrinogen concentrate compared with cryoprecipitate in major obstetric haemorrhage—An observational study. Transfus. Med. 2012, 22, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Obaid, O.; Anand, T.; Nelson, A.; Reina, R.; Ditillo, M.; Stewart, C.; Douglas, M.; Friese, R.; Gries, L.; Joseph, B. Fibrinogen Supplementation for the Trauma Patient: Should You Choose Fibrinogen Concentrate Over Cryoprecipitate? J. Trauma. Acute Care Surg. 2022, 93, 453–460. [Google Scholar] [CrossRef]
- Choi, H.J. Current status and outcome of liver transplantation in South Korea. Clin. Mol. Hepatol. 2022, 28, 117–119. [Google Scholar] [CrossRef]
- Maeda, T.; Miyata, S.; Usui, A.; Nishiwaki, K.; Tanaka, H.; Okita, Y.; Katori, N.; Shimizu, H.; Sasaki, H.; Ohnishi, Y.; et al. Safety of Fibrinogen Concentrate and Cryoprecipitate in Cardiovascular Surgery: Multicenter Database Study. J. Cardiothorac. Vasc. Anesth. 2019, 33, 321–327. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Cryoprecipitate Group (n = 109) | Fibrinogen Group (n = 97) | Total (n = 206) | p-Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Age | 55.0 (48.0–61.0) | 58.0 (52.0–63.0) | 56.0 (50.0–62.0) | 0.046 |
| Sex, male | 75 (68.1) | 72 (74.2) | 147 (71.4) | 0.481 |
| BMI | 22.9 (20.2–26.0) | 23.7 (21.3–26.9) | 23.2 (20.6–26.4) | 0.101 |
| Diabetes | 32 (29.4) | 31 (32.0) | 63 (30.6) | 0.800 |
| Hypertension | 23 (21.1) | 22 (22.7) | 45 (21.8) | 0.916 |
| CKD | 5 (4.6) | 3 (3.1) | 8 (3.9) | 0.847 |
| CAD | 3 (2.8) | 2 (2.1) | 5 (2.4) | 1.000 |
| CVA | 3 (2.8) | 2 (2.1) | 5 (2.4) | 1.000 |
| MELD-Na score | 18.0 (10.0–27.0) | 15.0 (11.0–21.0) | 17.0 (10.0–24.0) | 0.368 |
| CTP score | 9.0 (7.0–11.0) | 9.0 (7.0–10.0) | 9.0 (7.0–11.0) | 0.538 |
| Cause for LT | ||||
| HBV LC | 43 (39.5) | 37 (38.1) | 80 (38.8) | 0.961 |
| HCV LC | 5 (4.6) | 6 (6.2) | 11 (5.3) | 0.842 |
| Alcoholic LC | 50 (45.9) | 39 (40.2) | 89 (43.2) | 0.497 |
| HCC | 40 (36.7) | 40 (41.2) | 80 (38.8) | 0.600 |
| HCC with HBV | 27 (24.8) | 23 (23.7) | 50 (24.3) | 0.989 |
| HCC with HCV | 4 (3.7) | 6 (6.2) | 10 (4.9) | 0.521 |
| HCC with Alcoholic LC | 7 (6.4) | 12 (12.4) | 19 (9.2) | 0.218 |
| Laboratory variables | ||||
| Hemoglobin, g/dL | 9.3 (8.2–11.0) | 10.2 (8.4–12.0) | 9.9 (8.3–11.7) | 0.052 |
| Platelet, /L | 59.0 (42.0–88.0) | 58.0 (38.0–79.0) | 58.0 (38.0–82.0) | 0.462 |
| INR | 1.49 (1.23–1.86) | 1.38 (1.24–1.65) | 1.42 (1.23–1.75) | 0.110 |
| AST | 38.0 (28.0–56.0) | 37.0 (26.0–52.0) | 38.0 (27.0–54.0) | 0.347 |
| ALT | 21.0 (15.0–34.0) | 21.0 (14.0–28.0) | 21.0 (15.0–32.0) | 0.369 |
| Total bilirubin | 2.9 (1.2–7.7) | 2.0 (1.2–3.4) | 2.2 (1.2–5.2) | 0.082 |
| Albumin, g/dL | 3.0 (2.6–3.4) | 2.9 (2.5–3.4) | 2.9 (2.6–3.4) | 0.496 |
| Sodium | 138.0 (134.0–140.0) | 138.0 (134.0–141.0) | 138.0 (134.0–141.0) | 0.850 |
| Creatinine, mg/dL | 0.85 (0.72–1.15) | 0.78 (0.61–0.98) | 0.82 (0.66–1.06) | 0.036 |
| Intraoperative variables | ||||
| Operation time, hour | 12.5 ± 2.2 | 12.6 ± 1.9 | 12.6 ± 2.1 | 0.816 |
| Crystalloid, mL | 6200.0 (4400.0–8900.0) | 7200.0 (5200.0–9700.0) | 6450.0 (4700.0–9050.0) | 0.187 |
| Colloid, mL | 3600.0 (2800.0–4800.0) | 4000.0 (2800.0–5600.0) | 3600.0 (2800.0–5200.0) | 0.190 |
| Urine output, mL | 1570.0 (1010.0–2350.0) | 2000.0 (1400.0–2690.0) | 1755.0 (1200.0–2580.0) | 0.006 |
| Cryoprecipitate Group (n = 109) | Fibrinogen Group (n = 97) | Total (n = 206) | p-Value | |
|---|---|---|---|---|
| Intraoperative transfusion | ||||
| pRBC (unit) | 10.0 (6.0–18.0) | 10.0 (5.0–17.0) | 10.0 (6.0–18.0) | 0.757 |
| FFP (unit) | 10.0 (4.0–14.0) | 10.0 (6.0–18.0) | 10.0 (5.0–16.0) | 0.461 |
| Platelet apheresis (unit) | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | 1.0 (0.0–1.0) | 0.990 |
| Fibrinogen (g) | 0.0 (0.0–0.0) | 2.0 (2.0–4.0) | 0.0 (0.0–2.0) | <0.001 |
| Cryoprecipitate (unit) | 10.0 (10.0–10.0) | 0.0 (0.0–0.0) | 5.0 (0.0–10.0) | <0.001 |
| Massive transfusion | 57 (52.3) | 54 (55.7) | 111 (53.9) | 0.730 |
| Baseline | ||||
| Fibrinogen in plasma (mg/dL) | 75.0 (60.0–86.0) | 78.0 (62.0–96.0) | 77.0 (60.0–91.0) | 0.206 |
| FIBTEM | ||||
| MA 10 (mm) | 4.0 (3.0–6.0) | 4.0 (3.0–6.0) | 4.0 (3.0–6.0) | 0.521 |
| MCF (mm) | 4.0 (3.0–7.0) | 5.0 (4.0–7.0) | 5.0 (3.0–7.0) | 0.479 |
| After treatment for acquired hypofibrinogenemia | ||||
| Fibrinogen in plasma (mg/dL) | 97.0 (78.0–120.0) | 100.0 (81.0–116.0) | 98.0 (80.0–118.0) | 0.838 |
| FIBTEM | ||||
| MA 10 (mm) | 4.0 (3.0–6.0) | 5.0 (3.0–6.0) | 5.0 (3.0–6.0) | 0.033 |
| MCF (mm) | 4.0 (3.0–6.0) | 5.0 (4.0–7.0) | 5.0 (3.0–7.0) | 0.019 |
| Fibrinogen administered | ||||
| Preanhepatic | 21 (19.3) | 25 (25.8) | 46 (22.3) | 1.000 |
| Anhepatic | 12 (11.0) | 2 (2.1) | 14 (6.8) | |
| Postreperfusion | 76 (69.7) | 70 (72.2) | 146 (70.9) | |
| Cryoprecipitate Group (n = 109) | Fibrinogen Group (n = 97) | Total (n = 206) | p-Value | |
|---|---|---|---|---|
| MTE | 16 (14.7) | 14 (14.4) | 30 (14.6) | 1.000 |
| Portal and hepatic vein thrombosis | 14 (12.8) | 13 (13.4) | 27 (13.1) | 1.000 |
| Hepatic artery thrombosis | 2 (1.8) | 0 (0) | 2 (1.0) | 0.529 |
| Ischemic stroke | 0 (0) | 1 (1.0) | 1 (0.5) | 0.953 |
| 30-day MACE | 24 (22.0) | 13 (13.4) | 37 (18.0) | 0.154 |
| 1-year mortality | 10 (9.2) | 7 (7.2) | 17 (8.3) | 0.798 |
| 1-year graft failure | 16 (14.7) | 8 (8.3) | 24 (11.7) | 0.223 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Age (yr) | 0.99 | 0.96–1.02 | 0.540 | |||
| Male sex | 2.71 | 1.09–6.92 | 0.031 | 2.43 | 0.97–6.11 | 0.058 |
| Diabetes | 1.85 | 0.92–3.71 | 0.083 | 1.79 | 0.88–3.66 | 0.110 |
| Hypertension | 1.36 | 0.64–2.89 | 0.427 | |||
| Coronary artery disease | 1.32 | 0.28–6.21 | 0.723 | |||
| Cerebral vascular disease | 1.20 | 0.14–10.27 | 0.866 | |||
| Chronic kidney disease | 0.64 | 0.08–5.13 | 0.677 | |||
| Massive transfusion | 1.38 | 0.69–2.73 | 0.358 | |||
| MELD-Na score | 0.99 | 0.95–1.03 | 0.678 | |||
| Duration of surgery (hour) | 1.22 | 1.05–1.43 | 0.012 | 1.22 | 1.04–1.44 | 0.014 |
| Cause for LT | ||||||
| HBV LC | 0.86 | 0.43–1.71 | 0.662 | |||
| HCV LC | 3.09 | 0.92–10.41 | 0.068 | |||
| Alcoholic LC | 0.95 | 0.47–1.91 | 0.881 | |||
| HCC | 1.53 | 0.77–3.01 | 0.223 | |||
| Blood products | ||||||
| a No transfusion | (reference) | |||||
| Cryoprecipitate | 2.09 | 0.85–5.11 | 0.107 | |||
| Fibrinogen concentrate use | 2.05 | 0.82–5.12 | 0.126 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-H.; Kim, K.-S.; Kwon, H.-M.; Kim, S.-H.; Jun, I.-G.; Song, J.-G.; Hwang, G.-S. Comparison of Fibrinogen Concentrate and Cryoprecipitate on Major Thromboembolic Events after Living Donor Liver Transplantation. J. Clin. Med. 2023, 12, 7496. https://doi.org/10.3390/jcm12237496
Kim J-H, Kim K-S, Kwon H-M, Kim S-H, Jun I-G, Song J-G, Hwang G-S. Comparison of Fibrinogen Concentrate and Cryoprecipitate on Major Thromboembolic Events after Living Donor Liver Transplantation. Journal of Clinical Medicine. 2023; 12(23):7496. https://doi.org/10.3390/jcm12237496
Chicago/Turabian StyleKim, Jae-Hwan, Kyoung-Sun Kim, Hye-Mee Kwon, Sung-Hoon Kim, In-Gu Jun, Jun-Gol Song, and Gyu-Sam Hwang. 2023. "Comparison of Fibrinogen Concentrate and Cryoprecipitate on Major Thromboembolic Events after Living Donor Liver Transplantation" Journal of Clinical Medicine 12, no. 23: 7496. https://doi.org/10.3390/jcm12237496
APA StyleKim, J.-H., Kim, K.-S., Kwon, H.-M., Kim, S.-H., Jun, I.-G., Song, J.-G., & Hwang, G.-S. (2023). Comparison of Fibrinogen Concentrate and Cryoprecipitate on Major Thromboembolic Events after Living Donor Liver Transplantation. Journal of Clinical Medicine, 12(23), 7496. https://doi.org/10.3390/jcm12237496