
Lipid Profile in Olympic Athletes: Proposal for a “Lipid Athlete Score” as a Clinical Tool to Identify High-Risk Athletes

 ,
, 

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
- (1)
- Power (strength disciplines): weightlifting, Greco-Roman wrestling, judo, javelin, shot-putting, bobsleigh, skeleton, snowboard, swimming (<800 mt), alpine skiing, athletics (sprinting, shot putting, and discus), and luge.
- (2)
- Skills (technical disciplines): archery, equestrian, golf, shooting, figure skating, sailing, curling, diving, and equestrian sports.
- (3)
- Endurance (primarily dynamic components): cycling, rowing, canoeing, triathlon, long-distance running, long-distance swimming (>800 mt), cross-country skiing, pentathlon, biathlon, speed-skating, and Nordic combined.
- (4)
- Mixed disciplines (alternate dynamic and strength components): soccer, volleyball, basketball, tennis, fencing, water polo, rhythmic gymnastics, taekwondo, badminton, beach volley, and softball.
- Family history for atherosclerosis (ATH): fatal or non-fatal CV events or/and established diagnosis of CV disease in first-degree male relatives before 55 years of age, or female relatives before 65 years of age [12], or evidence of carotid/peripheral atherosclerotic disease in first-degree relatives;
- Family history for dyslipidemia: first-degree relative in treatment (pharmacological or nutraceutical);
- Cigarette smoking: defined as regular smokers of at least one cigarette per day;
- Overweight: in order to avoid misclassifying subjects with increased muscular mass and high BMI as overweight, our definition of “overweight” was a waist circumference of >94 cm for men or >80 cm for women [12], or a BMI over 30;
- Fat mass: normal values were identified as 10% to 22% body fat in males and 20% to 32% in females [14];
- Hypertension: systolic blood pressure ≥ 140mm Hg and/or diastolic ≥ 90 mm Hg, or subjects on pharmacological antihypertensive therapy [12];
- Diabetes: diagnosis was made in case of fasting glucose ≥126 mg/dL or current treatment with insulin or antidiabetic drugs [15];
- Hypertriglyceridemia: triglycerides (TG) values superior to 150 mg/dL [16];
- Alcohol intake: we used a binary classification: “none” if the athlete did not drink and “user” if assumed at least one glass of wine/beer or super-alcoholic for week.
3. Statistical Analysis
4. Results
5. Lipid Profile Analysis
6. Identification of a Cut-Off for Dyslipidemia
7. Univariate and Multivariate Analyses
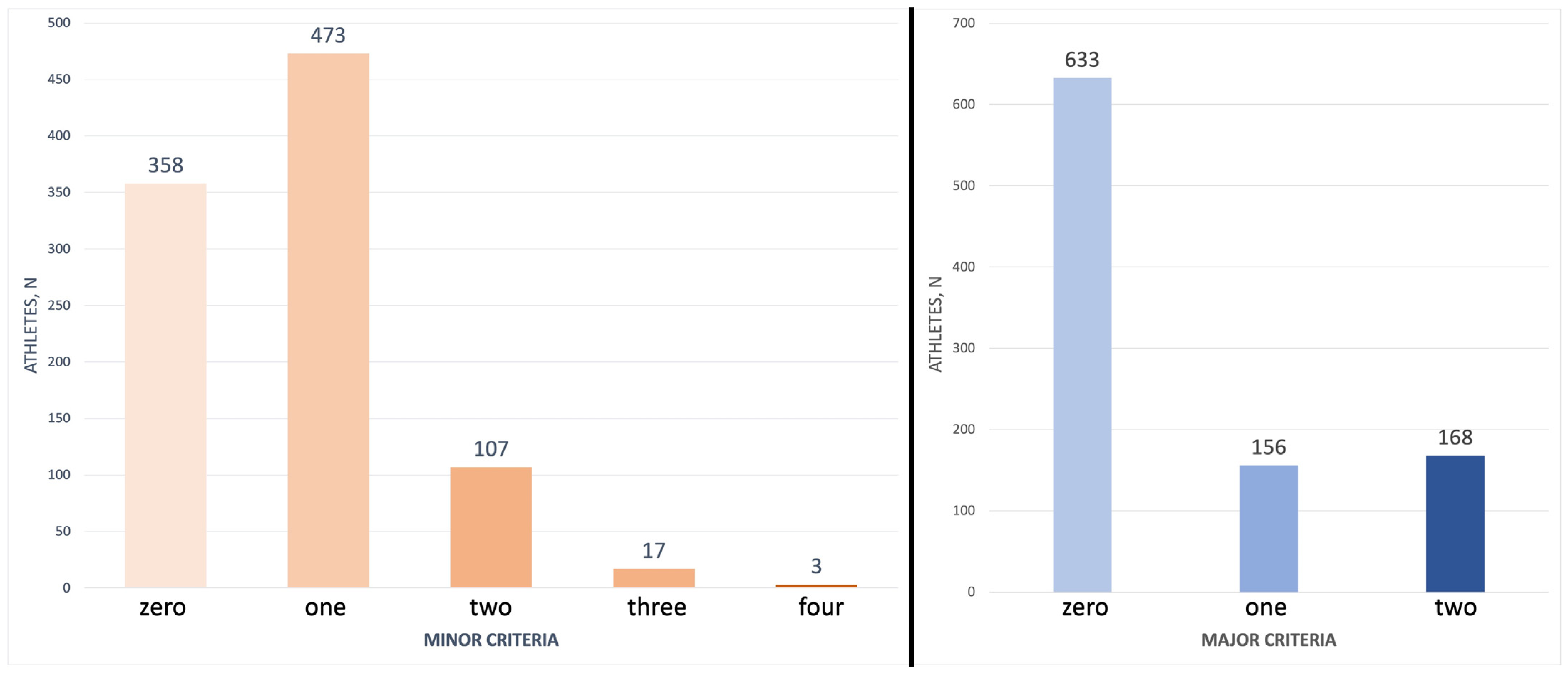
8. Lipid Athlete Score
9. Discussion
10. Limitations
11. Future Perspectives
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Whayne, T.F., Jr. Atherosclerosis: Current status of prevention and treatment. Int. J. Angiol. 2011, 20, 213–222. [Google Scholar] [CrossRef]
- D’Ascenzi, F.; Caselli, S.; Alvino, F.; Digiacinto, B.; Lemme, E.; Piepoli, M.; Pelliccia, A. Cardiovascular risk profile in Olympic athletes: An unexpected and underestimated risk scenario. Br. J. Sports Med. 2019, 53, 37–42. [Google Scholar] [CrossRef]
- Lippi, G.; Schena, F.; Salvagno, G.L.; Montagnana, M.; Ballestrieri, F.; Guidi, G.C. Comparison of the lipid profile and lipoprotein(a) between sedentary and highly trained subjects. Clin. Chem. Lab. Med. 2006, 44, 322–326. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Borrazzo, C.; Maestrini, V.; D’Ascenzi, F.; Caselli, S.; Lemme, E.; Squeo, M.R.; Di Giacinto, B. Determinants of LV mass in athletes: The impact of sport, constitutional traits and cardiovascular risk factors. Eur. J. Appl. Physiol. 2022, 123, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Perk, J.; De Backer, G.; Gohlke, H.; Graham, I.; Reiner, Z.; Verschuren, M.; Albus, C.; Benlian, P.; Boysen, G.; Cifkova, R.; et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur. Heart J. 2012, 33, 1635–1701. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B., Sr.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2935–2959. [Google Scholar] [CrossRef] [PubMed]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2889–2934. [Google Scholar] [CrossRef]
- Virani, S.S.; Wang, D.; Woodard, L.D.; Chitwood, S.S.; Landrum, C.R.; Zieve, F.J.; Ballantyne, C.M.; Petersen, L.A. Non-high-density lipoprotein cholesterol reporting and goal attainment in primary care. J. Clin. Lipidol. 2012, 6, 545–552. [Google Scholar] [CrossRef]
- Kinosian, B.; Glick, H.; Garland, G. Cholesterol and coronary heart disease: Predicting risks by levels and ratios. Ann. Intern. Med. 1994, 121, 641–647. [Google Scholar] [CrossRef]
- Ridker, P.M.; Stampfer, M.J.; Rifai, N. Novel risk factors for systemic atherosclerosis: A comparison of C-reactive protein, fibrinogen, homocysteine, lipoprotein(a), and standard cholesterol screening as predictors of peripheral arterial disease. JAMA 2001, 285, 2481–2485. [Google Scholar] [CrossRef] [PubMed]
- Task Force Members; Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. J. Prev. Cardiol. 2016, 23, NP1–NP96. [Google Scholar] [CrossRef] [PubMed]
- Mosteller, R.D. Simplified calculation of body-surface area. N. Engl. J. Med. 1987, 317, 1098. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine; Thompson, W.R.; Gordon, N.F.; Pescatello, L.S. ACSM’s Guidelines for Exercise Testing and Prescription, 8th ed.; Color Illustrations; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010; p. xxi. 380p. [Google Scholar]
- American Diabetes, A. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37 (Suppl. S1), S81–S90. [Google Scholar] [CrossRef] [PubMed]
- Cholesterol Treatment Trialists’ (CTT) Collaborators; Mihaylova, B.; Emberson, J.; Blackwell, L.; Keech, A.; Simes, J.; Barnes, E.H.; Voysey, M.; Gray, A.; Collins, R.; et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: Meta-analysis of individual data from 27 randomised trials. Lancet 2012, 380, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Qin, P.; Shi, J.; Cao, L.; Li, X.; Lou, Y.; Wang, C.; Ma, J.; Wang, L.; Peng, X.; Chen, H.; et al. Low-Density Lipoprotein Cholesterol/High-Density Lipoprotein Cholesterol Ratio and Carotid Intima-Media Thickness: A Cohort Study in China. Lipids 2021, 56, 59–68. [Google Scholar] [CrossRef]
- Duntas, L.H. Thyroid disease and lipids. Thyroid 2002, 12, 287–293. [Google Scholar] [CrossRef]
- Lloyd-Jones, D.M.; Wilson, P.W.; Larson, M.G.; Beiser, A.; Leip, E.P.; D’Agostino, R.B.; Levy, D. Framingham risk score and prediction of lifetime risk for coronary heart disease. Am. J. Cardiol. 2004, 94, 20–24. [Google Scholar] [CrossRef]
- Murray, C.J.; Lauer, J.A.; Hutubessy, R.C.; Niessen, L.; Tomijima, N.; Rodgers, A.; Lawes, C.M.; Evans, D.B. Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: A global and regional analysis on reduction of cardiovascular-disease risk. Lancet 2003, 361, 717–725. [Google Scholar] [CrossRef]
- Briana, D.D.; Malamitsi-Puchner, A. Coronary Intimal Thickening Begins in Fetuses: Proof of Concept for the “Fetal Origins of Adult Disease” Hypothesis. Angiology 2020, 71, 89. [Google Scholar] [CrossRef]
- Guerri-Guttenberg, R.; Castilla, R.; Cao, G.; Azzato, F.; Ambrosio, G.; Milei, J. Coronary Intimal Thickening Begins in Fetuses and Progresses in Pediatric Population and Adolescents to Atherosclerosis. Angiology 2020, 71, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Tucker, A.M.; Vogel, R.A.; Lincoln, A.E.; Dunn, R.E.; Ahrensfield, D.C.; Allen, T.W.; Castle, L.W.; Heyer, R.A.; Pellman, E.J.; Strollo, P.J., Jr.; et al. Prevalence of cardiovascular disease risk factors among National Football League players. JAMA 2009, 301, 2111–2119. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.A.; Croft, L.B.; Belanger, A.R.; Romero-Corral, A.; Somers, V.K.; Roberts, A.J.; Goldman, M.E. Prevalence of metabolic syndrome in retired National Football League players. Am. J. Cardiol. 2008, 101, 1281–1284. [Google Scholar] [CrossRef] [PubMed]
- Malina, R.M.; Morano, P.J.; Barron, M.; Miller, S.J.; Cumming, S.P.; Kontos, A.P.; Little, B.B. Overweight and obesity among youth participants in American football. J. Pediatr. 2007, 151, 378–382. [Google Scholar] [CrossRef]
- McKinney, J.; Moulson, N.; Morrison, B.N.; Phulka, J.S.; Yeung, P.; Isserow, S.; Wood, D.A. Do athletes play by different rules? Obstructive coronary artery disease in asymptomatic competitive Masters athletes: A case series. Eur. Heart J. Case Rep. 2020, 4, 1–5. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Back, M.; Borjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef]
- Bille, K.; Figueiras, D.; Schamasch, P.; Kappenberger, L.; Brenner, J.I.; Meijboom, F.J.; Meijboom, E.J. Sudden cardiac death in athletes: The Lausanne Recommendations. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 859–875. [Google Scholar] [CrossRef]
- Hurst, R.T.; Burke, R.F.; Wissner, E.; Roberts, A.; Kendall, C.B.; Lester, S.J.; Somers, V.; Goldman, M.E.; Wu, Q.; Khandheria, B. Incidence of subclinical atherosclerosis as a marker of cardiovascular risk in retired professional football players. Am. J. Cardiol. 2010, 105, 1107–1111. [Google Scholar] [CrossRef]
- Baggish, A.L.; Levine, B.D. Coronary Artery Calcification Among Endurance Athletes: “Hearts of Stone”. Circulation 2017, 136, 149–151. [Google Scholar] [CrossRef]
- Merghani, A.; Maestrini, V.; Rosmini, S.; Cox, A.T.; Dhutia, H.; Bastiaenan, R.; David, S.; Yeo, T.J.; Narain, R.; Malhotra, A.; et al. Prevalence of Subclinical Coronary Artery Disease in Masters Endurance Athletes With a Low Atherosclerotic Risk Profile. Circulation 2017, 136, 126–137. [Google Scholar] [CrossRef]
- Aengevaeren, V.L.; Mosterd, A.; Braber, T.L.; Prakken, N.H.J.; Doevendans, P.A.; Grobbee, D.E.; Thompson, P.D.; Eijsvogels, T.M.H.; Velthuis, B.K. Relationship Between Lifelong Exercise Volume and Coronary Atherosclerosis in Athletes. Circulation 2017, 136, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Parry-Williams, G.; Obaid, D.; Miles, C.; Basu, J.; MacLachlan, H.; Moser, J.; Vlahos, I.; O’Driscoll, J.; Chis Ster, I.; Papadakis, M. Determinants of high-risk coronary artery disease in ostensibly healthy male master endurance athletes. Eur. Heart J. 2021, 42, ehab724.2709. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Back, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Reamy, B.V.; Thompson, P.D. Lipid disorders in athletes. Curr. Sport. Med. Rep. 2004, 3, 70–76. [Google Scholar] [CrossRef]
- Chaudhry, W. Treating Lipid Disorders in Athletes. In Exercise and Sports Cardiology: Volume 2: Specific Diseases and Athletes; World Scientific: Singapore, 2018; pp. 25–48. [Google Scholar]
- Tsopanakis, C.; Kotsarellis, D.; Tsopanakis, A. Lipoprotein and lipid profiles of elite athletes in Olympic sports. Int. J. Sports Med. 1986, 7, 316–321. [Google Scholar] [CrossRef]
- McHugh, C.; Hind, K.; Cunningham, J.; Davey, D.; Wilson, F. A career in sport does not eliminate risk of cardiovascular disease: A systematic review and meta-analysis of the cardiovascular health of field-based athletes. J. Sci. Med. Sport 2020, 23, 792–799. [Google Scholar] [CrossRef]
- Steinberg, D. The Cholesterol Wars: The Skeptics vs the Preponderance of Evidence; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Steinberg, D.; Glass, C.K.; Witztum, J.L. Evidence mandating earlier and more aggressive treatment of hypercholesterolemia. Circulation 2008, 118, 672–677. [Google Scholar] [CrossRef]

{kind=link}
| Power | Skills | Endurance | Mixed | p-Value (Pooled) | p-Value (Pairwise Analysis) | |
|---|---|---|---|---|---|---|
| n (%) | 311 (32.5) | 122 (12.8) | 264 (27.6) | 260 (27.1) | ||
| Age, years | 25.9 ± 4.6 | 28.6 ± 6.5 | 27.2 ± 4.5 | 27.6 ± 4.7 | 0.001 | “Power” significantly younger (p < 0.001 in all pairwise comparisons; other comparison with p > 0.05) |
| Male, n (%) | 173 (55.6) | 71 (58.1) | 161 (60.9) | 125 (48) | 0.025 | “Mixed” lower incidence of male sex (p = 0.001 in all comparisons) |
| Black, n (%) | 18 (5.8) | 0 (0) | 10 (3.8) | 6 (2.3) | 0.017 | - |
| Smokers, n (%) | 12 (3.8) | 16 (13.1) | 1 (0.4) | 48 (18.4) | 0.001 | “Endurance” lower incidence of smokers (all p = 0.001); “Mixed” higher incidence of smokers (all p = 0.001) |
| Familiarity for ATH, n (%) | 69 (22.1) | 36 (29.5) | 53 (20) | 67 (25.7) | 0.157 | - |
| Familiarity for dyslipidemia, n (%) | 20 (6.43) | 13 (10.6) | 21 (7.9) | 24 (9.2) | 0.445 | - |
| Weight, kg | 73.8 ± 15.5 | 72.1 ± 14.1 | 69.6 ± 13.7 | 76.6 ± 16.3 | 0.001 | “Endurance” significantly less weight (p < 0.001 in all pairwise comparisons; other comparison with p > 0.05) |
| BMI, kg/m2 | 23.3 3.6 | 23.9 ± 3.3 | 22.0 ± 2.6 | 23.4 ± 2.8 | 0.001 | “Endurance” significantly less BMI (p < 0.001 in all pairwise comparisons; other comparison with p > 0.05) |
| Fat mass, % | 15 ± 6.3 | 19.7 ± 7.4 | 13.3 ± 5.3 | 17.4 ± 6.4 | 0.001 | All pairwise comparisons have statistically significant differences |
| Waist, cm | 75.9 ± 8.7 | 75.5 ± 7.7 | 74.4 ± 7.5 | 77.9 ± 8.4 | 0.098 | - |
| W/H ratio | 0.78 ± 0.05 | 0.79 ± 0.06 | 0.78 ± 0.05 | 0.78 ± 0.06 | 0.541 | - |
| Kcal | 2893 ± 681 | 2231 ± 482 | 2811 ± 733 | 2508 ± 717 | 0.001 | Power vs. endurance, p = 0.353 “Power” and “Endurance” statistically significant differences with other groups (all p = 0.001) |
| Fat in diet, % | 29.3 ± 3.7 | 29.8 ± 6.5 | 29.2 ± 3.3 | 29.7 ± 3.2 | 0.231 | - |
| Alcohol, n (%) | 179 (57.5) | 67 (55) | 149 (56.4) | 160 (61.5) | 0.552 | - |
| TC, mg/dL | 175.6 ± 33.1 | 175.3 ± 34.7 | 180.3 ± 31.4 | 182.5 ± 32.3 | 0.075 | - |
| LDL, mg/dL | 97.8 ± 27.1 | 97.7 ± 29.2 | 95.1 ± 26.9 | 102 ± 28.1 | 0.100 | - |
| HDL, mg/dL | 62.8 ± 14.9 | 61 ± 16.5 | 71.6 ± 16.3 | 66.4 ± 14.6 | 0.001 | “Endurance” higher values (all comparison p = 0.001); no significant differences among other groups |
| TG, mg/dL | 75.7 ± 40.5 | 85.1 ± 56.9 | 68.6 ± 28.7 | 73.8 ± 36.4 | 0.009 | “Skills” higher values (all comparison p = 0.001); no significant differences among other groups |
| LDL/HDL | 1.6 ± 0.6 | 1.7 ± 0.7 | 1.4 ± 0.5 | 1.6 ± 0.6 | 0.264 | - |
| Total | p-Value | ||
|---|---|---|---|
| Male | Female | ||
| n (%) | 530 (55.4) | 427 (44.6) | |
| Age, years | 27.6 ± 5 | 26.4 ± 4.8 | 0.005 |
| Black, n (%) | 22 (4.1) | 12 (2.8) | 0.265 |
| Smokers, n (%) | 46 (8.7) | 31 (7.3) | 0.422 |
| Familiarity for ATH, n (%) | 125 (23.5) | 100 (23.4) | 0.952 |
| Familiarity for dyslipidemia, n (%) | 42 (7.9) | 36 (8.4) | 0.776 |
| Weight, kg | 81.6 ± 13.5 | 62.7 ± 10 | 0.001 |
| BMI, kg/m2 | 24.2 ± 3.2 | 21.7 ± 2.6 | 0.001 |
| Fat mass, % | 12.1 ± 3.2 | 20.2 ± 5.4 | 0.001 |
| Waist, cm | 81.4 ± 7 | 70 ± 4.8 | 0.001 |
| W/H ratio | 0.82 ± 0.04 | 0.74 ± 0.04 | 0.001 |
| Kcal | 2951 ± 706 | 2271 ± 519 | 0.001 |
| Alcohol | 326 (61.5) | 229 (53.6) | 0.014 |
| Fat, % | 29.6 ± 3.8 | 29.3 ± 4.2 | 0.245 |
| TC, mg/dL | 177 ± 32.5 | 181 ± 32.9 | 0.099 |
| LDL, mg/dL | 100.8 ± 29.4 | 95 ± 25.1 | 0.002 |
| HDL, mg/dL | 60.7 ± 14.8 | 72.4 ± 14.9 | 0.001 |
| TG, mg/dL | 79.5 ± 46.6 | 68.2 ± 27.1 | 0.001 |
| LDL/HDL | 1.76 ± 0.7 | 1.36 ± 0.5 | 0.001 |
| BMI | Fat Mass | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| <25 | 25–29.9 | 30–34.9 | ≥35 | p-Value | Male | p-Value | Female | p-Value | |||
| ≤22 | >22 | ≤32 | >32 | ||||||||
| n (%) | 739 (77.2) | 192 (20) | 19 (2) | 7 (0.7) | 504 (95.1) | 26 (4.9) | 417 (96.7) | 10 (2.3) | |||
| Age, years | 26.6 ± 4.8 | 28.6 ± 4.8 | 31.5 ± 5.5 | 32.1 ± 5.9 | 0.001 | 27.3 ± 4.8 | 33.8 ± 6 | 0.001 | 26.4 ± 4.7 | 30.1 ± 5.9 | 0.015 |
| Male, n (%) | 348 (47.1) | 160 (83.3) | 17 (89.5) | 5 (71.4) | 0.001 | 504 (100) | 26 (100) | - | 0 (0) | 0 (0) | - |
| Black, n (%) | 28 (3.8) | 5 (2.6) | 1 (5.3) | 0 (0) | 0.790 | 25 (5) | 0 (0) | 0.277 | 12 (2.9) | 0 (0) | 0.586 |
| Smokers, n (%) | 60 (9.5) | 15 (7.8) | 1 (5.3) | 1 (14.2) | 0.899 | 71 (14.1) | 2 (7.7) | 0.855 | 31 (7.4) | 0 (0) | 0.371 |
| Familiarity for ATH, n (%) | 174 (23.5) | 45 (23.4) | 5 (26.3) | 1 (14.2) | 0.937 | 166 (32.9) | 5 (19.2) | 0.592 | 97 (23.3) | 3 (30) | 0.619 |
| Familiarity for dyslipidemia, n (%) | 65 (8.8) | 10 (5.2) | 2 (10.6) | 1 (14.2) | 0.371 | 59 (11.7) | 4 (15.4) | 0.149 | 36 (8.6) | 0 (0) | 0.332 |
| Power, n (%) | 226 (30.6) | 73 (38) | 7 (36.8) | 5 (71.4) | 0.039 | 164 (32.5) | 9 (34.6) | 0.826 | 135 (32.4) | 3 (30) | 0.874 |
| Skills, n (%) | 87 (11.8) | 28 (14.6) | 6 (31.6) | 1 (14.2) | 0.064 | 59 (11.7) | 12 (46.1) | 0.001 | 47 (11.3) | 4 (40) | 0.006 |
| Endurance, n (%) | 231 (31.2) | 33 (17.2) | 0 (0) | 0 (0) | 0.001 | 161 (31.9) | 0 (0) | 0.001 | 103 (24.7) | 0 | 0.071 |
| Mixed, n (%) | 194 (26.2) | 59 (30.7) | 6 (31.6) | 1 (14.2) | 0.514 | 120 (23.8) | 5 (19.2) | 0.592 | 132 (31.7) | 3 (30) | 0.911 |
| Weight, kg | 68.1 ± 11.9 | 87.8 ± 10.4 | 102.7 ± 9.4 | 125.3 ± 12.9 | 0.001 | 80.8 ± 12.4 | 98.5 ± 20.8 | 0.001 | 62.1 ± 8.9 | 87.1 ± 17.9 | 0.001 |
| BMI, kg/m2 | 21.8 ± 1.9 | 26.6 ± 1.2 | 31.6 ± 1.5 | 37.2 ± 2.1 | 0.001 | 24 ± 2.7 | 28.9 ± 6.8 | 0.001 | 21.5 ± 2.2 | 29.9 ± 4.2 | 0.001 |
| Fat mass, % | 15.4 ± 6.2 | 16.1 ± 6.6 | 22.6 ± 9.8 | 29.7 ± 5.9 | 0.001 | 11.4 ± 4 | 26.2 ± 3.5 | 0.001 | 19.9 ± 4.8 | 36.5 ± 2.8 | 0.001 |
| Waist, cm | 73 ± 6.3 | 84.4 ± 6 | 92.3 ± 5.9 | 118 ± 3.4 | 0.001 | 81.1 ± 6.3 | 95.1 ± 16.2 | 0.001 | 69.8 ± 4.6 | 84.5 ± 2.5 | 0.001 |
| W/H ratio | 0.78 ± 0.05 | 0.82 ± 0.05 | 0.85 ± 0.05 | 0.93 ± 0.04 | 0.001 | 0.82 ± 0.04 | 0.88 ± 0.07 | 0.001 | 0.74 ± 0.04 | 0.8 ± 0.07 | 0.001 |
| TC, mg/dL | 178.9 ± 33.1 | 177.1 ± 31.2 | 186.8 ± 34.5 | 193.1 ± 23.1 | 0.353 | 176.2 ± 32.1 | 197.1 ± 33.7 | 0.001 | 180.5 ± 33.1 | 192.1 ± 42.1 | 0.272 |
| LDL, mg/dL | 96.9 ± 27.1 | 100.7 ± 28.3 | 114 ± 33.6 | 126.5 ± 27.3 | 0.001 | 99.6 ± 28.7 | 124.5 ± 31.8 | 0.001 | 94.7 ± 25.3 | 107.1 ± 23.5 | 0.126 |
| HDL, mg/dL | 68.2 ± 15.4 | 59.5 ± 15.5 | 52.6 ± 12.1 | 46.2 ± 4.8 | 0.001 | 61.2 ± 14.9 | 51.4 ± 10.8 | 0.001 | 72.6 ± 14.9 | 63.5 ± 14.6 | 0.056 |
| TG, mg/dL | 70.5 ± 31.4 | 85.5 ± 56.8 | 104.8 ± 62.5 | 103.5 ± 34.8 | 0.001 | 78.2 ± 46.6 | 106.9 ± 56.2 | 0.002 | 67.2 ± 24.9 | 110.8 ± 58.8 | 0.001 |
| LDL/HDL | 1.50 ± 0.5 | 1.8 ± 0.7 | 2.32 ± 0.9 | 2.81 ± 0.8 | 0.001 | 1.72 ± 0.6 | 2.51 ± 0.8 | 0.001 | 1.35 ± 0.5 | 1.74 ± 0.5 | 0.008 |
| Variable | |
|---|---|
| Major criteria (M) | LDL ≥ 115 mg/dL |
| LDL/HDL ratio ≥ 1.90 | |
| Minor criteria (m) | Male sex |
| BMI > 30 or fat mass > 22% for males and 32% for females | |
| Familiarity for dyslipidemia | |
| Cardiovascular risk factors (smoke, hypertension, and diabetes) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Gioia, G.; Buzzelli, L.; Maestrini, V.; Nenna, A.; Monosilio, S.; Squeo, M.R.; Lemme, E.; Pelliccia, A. Lipid Profile in Olympic Athletes: Proposal for a “Lipid Athlete Score” as a Clinical Tool to Identify High-Risk Athletes. J. Clin. Med. 2023, 12, 7449. https://doi.org/10.3390/jcm12237449
Di Gioia G, Buzzelli L, Maestrini V, Nenna A, Monosilio S, Squeo MR, Lemme E, Pelliccia A. Lipid Profile in Olympic Athletes: Proposal for a “Lipid Athlete Score” as a Clinical Tool to Identify High-Risk Athletes. Journal of Clinical Medicine. 2023; 12(23):7449. https://doi.org/10.3390/jcm12237449
Chicago/Turabian StyleDi Gioia, Giuseppe, Lorenzo Buzzelli, Viviana Maestrini, Antonio Nenna, Sara Monosilio, Maria Rosaria Squeo, Erika Lemme, and Antonio Pelliccia. 2023. "Lipid Profile in Olympic Athletes: Proposal for a “Lipid Athlete Score” as a Clinical Tool to Identify High-Risk Athletes" Journal of Clinical Medicine 12, no. 23: 7449. https://doi.org/10.3390/jcm12237449
APA StyleDi Gioia, G., Buzzelli, L., Maestrini, V., Nenna, A., Monosilio, S., Squeo, M. R., Lemme, E., & Pelliccia, A. (2023). Lipid Profile in Olympic Athletes: Proposal for a “Lipid Athlete Score” as a Clinical Tool to Identify High-Risk Athletes. Journal of Clinical Medicine, 12(23), 7449. https://doi.org/10.3390/jcm12237449