

Restoration of Over-Ground Walking via Non-Invasive Neuromodulation Therapy: A Single-Case Study

 , , ,
, , ,  , and
, and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participant
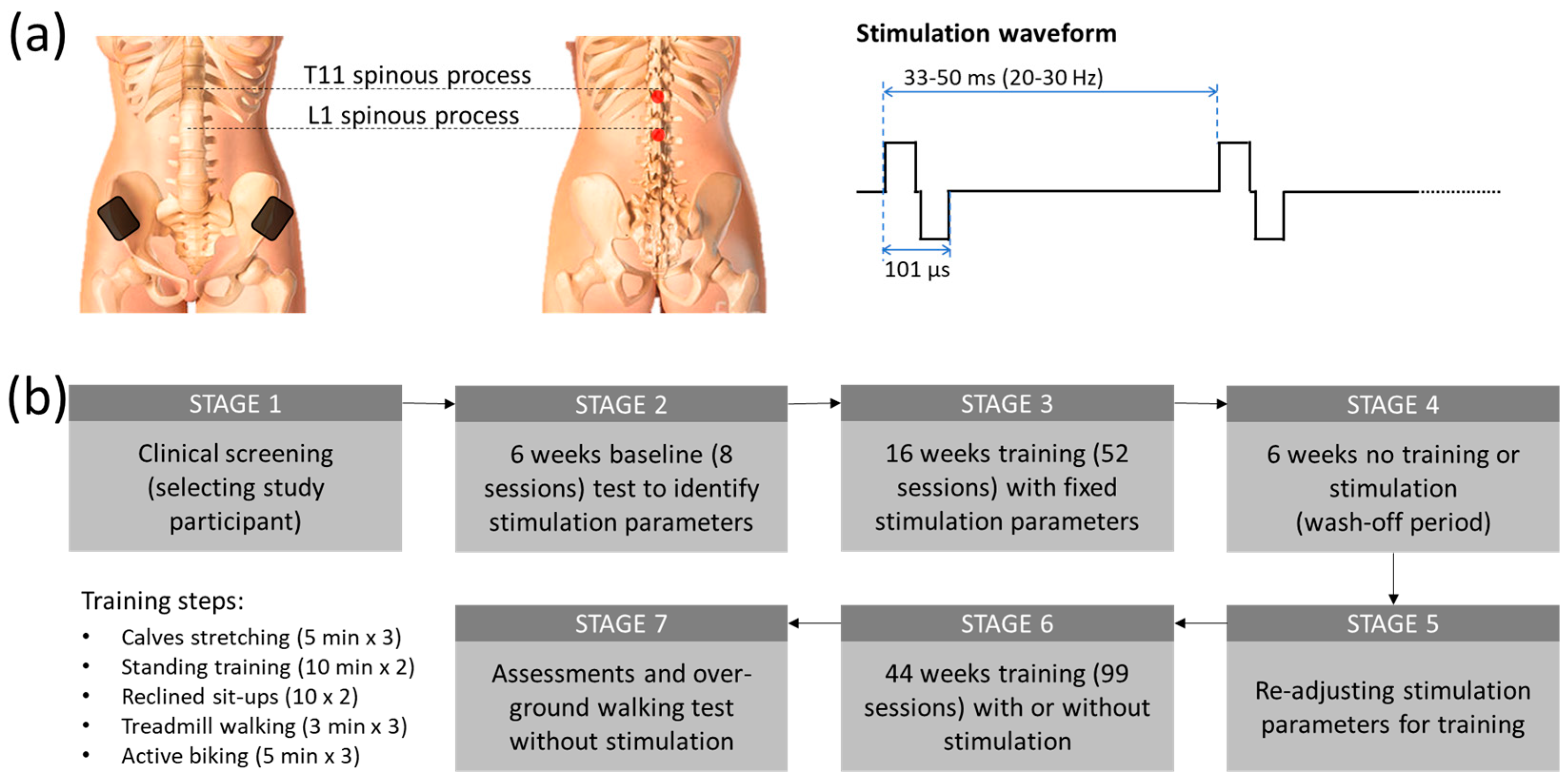
2.2. Stimulation Protocol
2.3. Study Procedure
2.4. Standing and Functional Reaching Training with tES
2.5. Reclined Sit-Ups with tES
2.6. Treadmill Walking Training with tES
2.7. Active Biking Training with tES
2.8. Testing of Over-Ground Walking with and without tES
2.9. Data Analysis and Statistics
3. Results
3.1. Improvement in Sensory and Motor Functions
3.2. Restoration of Overground Walking Ability
3.3. Improvement of Forward Biking Ability with tES
3.4. Secondary Functional Improvements
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alam, M.; Zheng, Y.P. Motor neuroprosthesis for injured spinal cord: Who is an ideal candidate? Neural Regen. Res. 2017, 12, 1809–1810. [Google Scholar] [CrossRef]
- Cripps, R.A.; Lee, B.B.; Wing, P.; Weerts, E.; Mackay, J.; Brown, D. A global map for traumatic spinal cord injury epidemiology: Towards a living data repository for injury prevention. Spinal Cord 2011, 49, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.G.; Karabukayeva, A.; Rainey, C.; Kelly, R.J.; Patterson, J.; Wade, J.; Feldman, S.S. Perspectives on life following a traumatic spinal cord injury. Disabil. Health J. 2021, 14, 101067. [Google Scholar] [CrossRef] [PubMed]
- Anjum, A.; Yazid, M.D.; Fauzi Daud, M.; Idris, J.; Ng, A.M.H.; Selvi Naicker, A.; Ismail, O.H.R.; Athi Kumar, R.K.; Lokanathan, Y. Spinal Cord Injury: Pathophysiology, Multimolecular Interactions, and Underlying Recovery Mechanisms. Int. J. Mol. Sci. 2020, 21, 7533. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.; He, J. Lower-Limb Neuroprostheses: Restoring Walking after Spinal Cord Injury. In Emerging Theory and Practice in Neuroprosthetics; Naik, G.R., Guo, Y., Eds.; IGI Global: Hershey, PA, USA, 2014; pp. 153–180. [Google Scholar]
- Sezer, N.; Akkuş, S.; Uğurlu, F.G. Chronic complications of spinal cord injury. World J. Orthop. 2015, 6, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Koukoulithras, I.; Alkhazi, A.; Gkampenis, A.; Stamouli, A.; Plexousakis, M.; Drousia, G.; Xanthi, E.; Roussos, C.; Kolokotsios, S. A Systematic Review of the Interventions for Management of Pain in Patients after Spinal Cord Injury. Cureus 2023, 15, e42657. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.A.; Ichikawa, J.K.; Bombardier, C.H.; Hammond, F.M. Association Between Anxiety Symptoms, Depression Symptoms, and Life Satisfaction among Individuals 1 Year after Spinal Cord Injury: Findings from the SCIRehab Project. Arch. Rehabil. Res. Clin. Transl. 2022, 4, 100211. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.; Tran, Y.; Middleton, J. Psychological morbidity and spinal cord injury: A systematic review. Spinal Cord 2009, 47, 108–114. [Google Scholar] [CrossRef]
- Kennedy, P.; Lude, P.; Taylor, N. Quality of life, social participation, appraisals and coping post spinal cord injury: A review of four community samples. Spinal Cord 2006, 44, 95–105. [Google Scholar] [CrossRef]
- Tsai, I.; Graves, D.E.; Chan, W.; Darkoh, C.; Lee, M.-S.; Pompeii, L.A. Environmental barriers and social participation in individuals with spinal cord injury. Rehabil. Psychol. 2017, 62, 36–44. [Google Scholar] [CrossRef]
- Angeli, C.A.; Boakye, M.; Morton, R.A.; Vogt, J.; Benton, K.; Chen, Y.; Ferreira, C.K.; Harkema, S.J. Recovery of over-Ground Walking after Chronic Motor Complete Spinal Cord Injury. N. Engl. J. Med. 2018, 379, 1244–1250. [Google Scholar] [CrossRef]
- Wagner, F.B.; Mignardot, J.-B.; Le Goff-Mignardot, C.G.; Demesmaeker, R.; Komi, S.; Capogrosso, M.; Rowald, A.; Seáñez, I.; Caban, M.; Pirondini, E.; et al. Targeted neurotechnology restores walking in humans with spinal cord injury. Nature 2018, 563, 65–71. [Google Scholar] [CrossRef]
- Patel, S.K.; Gozal, Y.M.; Saleh, M.S.; Gibson, J.L.; Karsy, M.; Mandybur, G.T. Spinal cord stimulation failure: Evaluation of factors underlying hardware explantation. J. Neurosurg. Spine 2019, 32, 133–138. [Google Scholar] [CrossRef]
- Caylor, J.; Reddy, R.; Yin, S.; Cui, C.; Huang, M.; Huang, C.; Ramesh, R.; Baker, D.G.; Simmons, A.; Souza, D.; et al. Spinal cord stimulation in chronic pain: Evidence and theory for mechanisms of action. Bioelectron. Med. 2019, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Hofstoetter, U.S.; Freundl, B.; Lackner, P.; Binder, H. Transcutaneous Spinal Cord Stimulation Enhances Walking Performance and Reduces Spasticity in Individuals with Multiple Sclerosis. Brain Sci. 2021, 11, 472. [Google Scholar] [CrossRef] [PubMed]
- Kumru, H.; García-Alén, L.; Ros-Alsina, A.; Albu, S.; Valles, M.; Vidal, J. Transcutaneous Spinal Cord Stimulation Improves Respiratory Muscle Strength and Function in Subjects with Cervical Spinal Cord Injury: Original Research. Biomedicines 2023, 11, 2121. [Google Scholar] [CrossRef] [PubMed]
- Salavatian, S.; Kuwabara, Y.; Wong, B.; Fritz, J.R.; Howard-Quijano, K.; Foreman, R.D.; Armour, J.A.; Ardell, J.L.; Mahajan, A. Spinal neuromodulation mitigates myocardial ischemia-induced sympathoexcitation by suppressing the intermediolateral nucleus hyperactivity and spinal neural synchrony. Front. Neurosci. 2023, 17, 1180294. [Google Scholar] [CrossRef]
- Steadman, C.J.; Grill, W.M. Spinal cord stimulation for the restoration of bladder function after spinal cord injury. Healthc. Technol. Lett. 2020, 7, 87–92. [Google Scholar] [CrossRef]
- DiMarco, A.F.; Geertman, R.T.; Tabbaa, K.; Nemunaitis, G.A.; Kowalski, K.E. Effects of Lower Thoracic Spinal Cord Stimulation on Bowel Management in Individuals with Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2021, 102, 1155–1164. [Google Scholar] [CrossRef]
- Qian, Q.; Ling, Y.T.; Zhong, H.; Zheng, Y.-P.; Alam, M. Restoration of arm and hand functions via noninvasive cervical cord neuromodulation after traumatic brain injury: A case study. Brain Inj. 2020, 34, 1771–1780. [Google Scholar] [CrossRef]
- Rahman, M.A.; Tharu, N.S.; Gustin, S.M.; Zheng, Y.-P.; Alam, M. Trans-spinal electrical stimulation therapy for functional rehabilitation after spinal cord injury. J. Clin. Med. 2022, 11, 1550. [Google Scholar] [CrossRef] [PubMed]
- Tharu, N.S.; Alam, M.; Ling, Y.T.; Wong, A.Y.; Zheng, Y.-P. Combined Transcutaneous Electrical Spinal Cord Stimulation and Task-Specific Rehabilitation Improves Trunk and Sitting Functions in People with Chronic Tetraplegia. Biomedicines 2023, 11, 34. [Google Scholar] [CrossRef] [PubMed]
- Martin, R. Utility and Feasibility of Transcutaneous Spinal Cord Stimulation for Patients with Incomplete SCI in Therapeutic Settings: A Review of Topic. Front. Rehabil. Sci. 2021, 2, 724003. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.; Ling, Y.T.; Wong, A.Y.; Zhong, H.; Edgerton, V.R.; Zheng, Y.P. Reversing 21 years of chronic paralysis via non-invasive spinal cord neuromodulation: A case study. Ann. Clin. Transl. Neurol. 2020, 7, 829–838. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Ratamess, N.A. Fundamentals of resistance training: Progression and exercise prescription. Med. Sci. Sports Exerc. 2004, 36, 674–688. [Google Scholar] [CrossRef]
- Peña Pino, I.; Hoover, C.; Venkatesh, S.; Ahmadi, A.; Sturtevant, D.; Patrick, N.; Freeman, D.; Parr, A.; Samadani, U.; Balser, D.; et al. Long-Term Spinal Cord Stimulation after Chronic Complete Spinal Cord Injury Enables Volitional Movement in the Absence of Stimulation. Front. Syst. Neurosci. 2020, 14, 35. [Google Scholar] [CrossRef]
- Pêgo, A.P.; Kubinova, S.; Cizkova, D.; Vanicky, I.; Mar, F.M.; Sousa, M.M.; Sykova, E. Regenerative medicine for the treatment of spinal cord injury: More than just promises? J. Cell. Mol. Med. 2012, 16, 2564–2582. [Google Scholar] [CrossRef]
- Turczyn, P.; Wojdasiewicz, P.; Poniatowski, Ł.A.; Purrahman, D.; Maślińska, M.; Żurek, G.; Romanowska-Próchnicka, K.; Żuk, B.; Kwiatkowska, B.; Piechowski-Jóźwiak, B.; et al. Omega-3 fatty acids in the treatment of spinal cord injury: Untapped potential for therapeutic intervention? Mol. Biol. Rep. 2022, 49, 10797–10809. [Google Scholar] [CrossRef]
- Tefertiller, C.; Rozwod, M.; VandeGriend, E.; Bartelt, P.; Sevigny, M.; Smith, A.C. Transcutaneous Electrical Spinal Cord Stimulation to Promote Recovery in Chronic Spinal Cord Injury. Front. Rehabil. Sci. 2022, 2, 740307. [Google Scholar] [CrossRef]
- Aout, T.; Begon, M.; Jegou, B.; Peyrot, N.; Caderby, T. Effects of Functional Electrical Stimulation on Gait Characteristics in Healthy Individuals: A Systematic Review. Sensors 2023, 23, 8684. [Google Scholar] [CrossRef]
- Gerasimenko, Y.P.; Lu, D.C.; Modaber, M.; Zdunowski, S.; Gad, P.; Sayenko, D.G.; Morikawa, E.; Haakana, P.; Ferguson, A.R.; Roy, R.R.; et al. Noninvasive Reactivation of Motor Descending Control after Paralysis. J. Neurotrauma 2015, 32, 1968–1980. [Google Scholar] [CrossRef]
- Samejima, S.; Caskey, C.D.; Inanici, F.; Shrivastav, S.R.; Brighton, L.N.; Pradarelli, J.; Martinez, V.; Steele, K.M.; Saigal, R.; Moritz, C.T. Multisite Transcutaneous Spinal Stimulation for Walking and Autonomic Recovery in Motor-Incomplete Tetraplegia: A Single-Subject Design. Phys. Ther. 2022, 102, pzab228. [Google Scholar] [CrossRef] [PubMed]
- Dost, G.; Dulgeroglu, D.; Yildirim, A.; Ozgirgin, N. The effects of upper extremity progressive resistance and endurance exercises in patients with spinal cord injury. J. Back Musculoskelet. Rehabilit. 2014, 27, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, L.; Larsen, M.N.; Madsen, M.J.; Grey, M.J.; Nielsen, J.B.; Lundbye-Jensen, J. Long-term motor skill training with individually adjusted progressive difficulty enhances learning and promotes corticospinal plasticity. Sci. Rep. 2020, 10, 15588. [Google Scholar] [CrossRef]
- Singh, G.; Lucas, K.; Keller, A.; Martin, R.; Behrman, A.; Vissarionov, S.; Gerasimenko, Y.P. Transcutaneous Spinal Stimulation From Adults to Children: A Review. Top. Spinal Cord Inj. Rehabil. 2022, 29, 16–32. [Google Scholar] [CrossRef]
- Powell, M.P.; Verma, N.; Sorensen, E.; Carranza, E.; Boos, A.; Fields, D.P.; Roy, S.; Ensel, S.; Barra, B.; Balzer, J.; et al. Epidural stimulation of the cervical spinal cord for post-stroke upper-limb paresis. Nat. Med. 2023, 29, 689–699. [Google Scholar] [CrossRef]
- Tian, T.; Zhang, S.; Yang, M. Recent progress and challenges in the treatment of spinal cord injury. Protein Cell 2023, 14, 635–652. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Hong, L.; Liu, C.; Hong, S.; He, S.; Zhou, M.; Huang, G.; Chen, Q. Electrical stimulation enhances neuronal cell activity mediated by Schwann cell derived exosomes. Sci. Rep. 2019, 9, 4206. [Google Scholar] [CrossRef]
- Flores, Á.; López-Santos, D.; García-Alías, G. When Spinal Neuromodulation Meets Sensorimotor Rehabilitation: Lessons Learned From Animal Models to Regain Manual Dexterity after a Spinal Cord Injury. Front. Rehabil. Sci. 2021, 2, 755963. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alam, M.; Ling, Y.T.; Rahman, M.A.; Wong, A.Y.L.; Zhong, H.; Edgerton, V.R.; Zheng, Y.-P. Restoration of Over-Ground Walking via Non-Invasive Neuromodulation Therapy: A Single-Case Study. J. Clin. Med. 2023, 12, 7362. https://doi.org/10.3390/jcm12237362
Alam M, Ling YT, Rahman MA, Wong AYL, Zhong H, Edgerton VR, Zheng Y-P. Restoration of Over-Ground Walking via Non-Invasive Neuromodulation Therapy: A Single-Case Study. Journal of Clinical Medicine. 2023; 12(23):7362. https://doi.org/10.3390/jcm12237362
Chicago/Turabian StyleAlam, Monzurul, Yan To Ling, Md Akhlasur Rahman, Arnold Yu Lok Wong, Hui Zhong, V. Reggie Edgerton, and Yong-Ping Zheng. 2023. "Restoration of Over-Ground Walking via Non-Invasive Neuromodulation Therapy: A Single-Case Study" Journal of Clinical Medicine 12, no. 23: 7362. https://doi.org/10.3390/jcm12237362
APA StyleAlam, M., Ling, Y. T., Rahman, M. A., Wong, A. Y. L., Zhong, H., Edgerton, V. R., & Zheng, Y.-P. (2023). Restoration of Over-Ground Walking via Non-Invasive Neuromodulation Therapy: A Single-Case Study. Journal of Clinical Medicine, 12(23), 7362. https://doi.org/10.3390/jcm12237362