

Prognostic Value of the Baseline and Early Changes in Monocyte-to-Lymphocyte Ratio for Short-Term Mortality among Critically Ill Patients with Acute Kidney Injury

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Population Selection Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Subject Characteristics
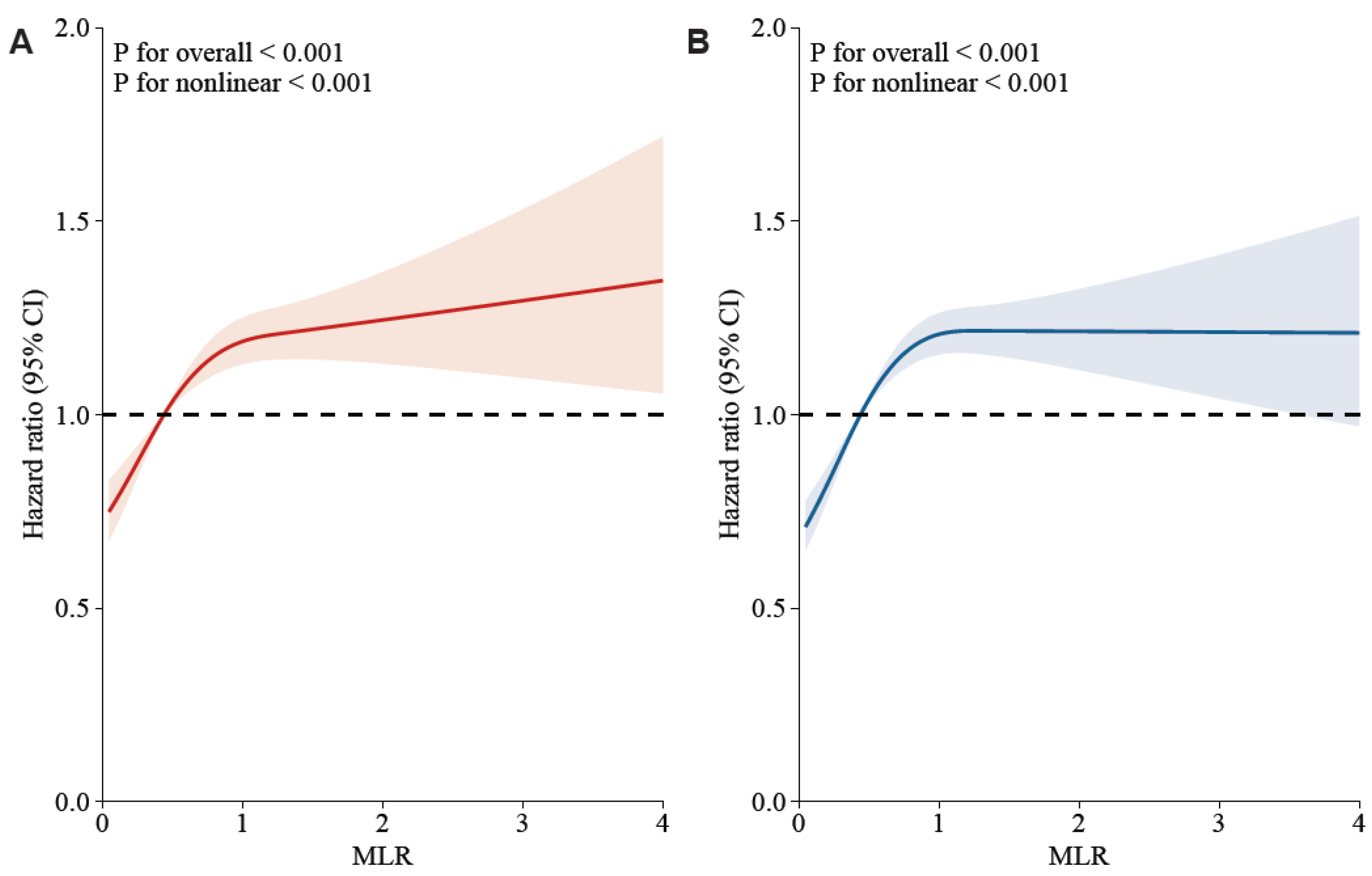
3.2. Association between Monocyte-to-Lymphocyte and 30-Day and 90-Day Outcomes
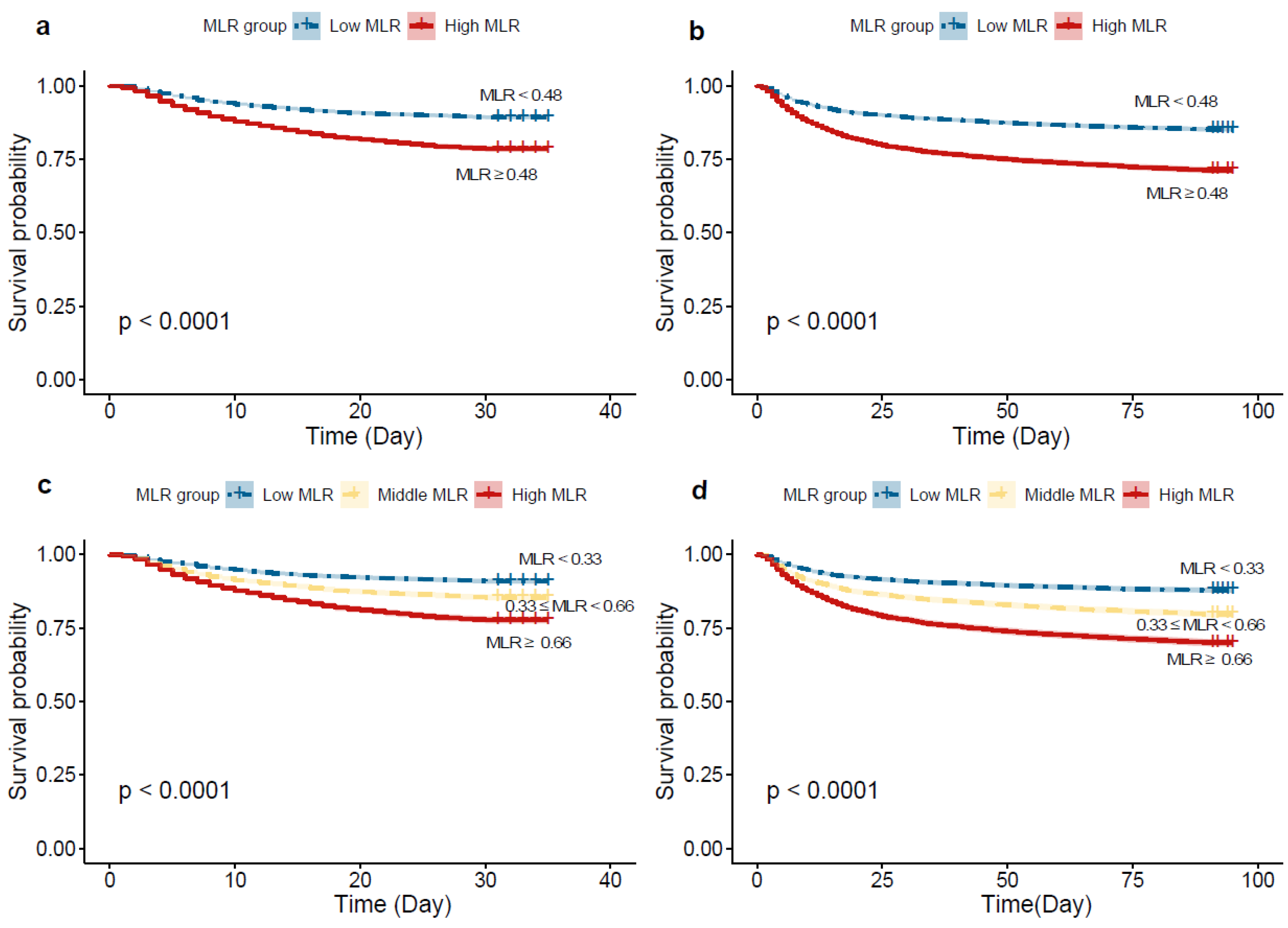
3.3. ROC Curve Analysis and Kaplan–Meier Survival Curve Analysis
3.4. Subgroup Analyses
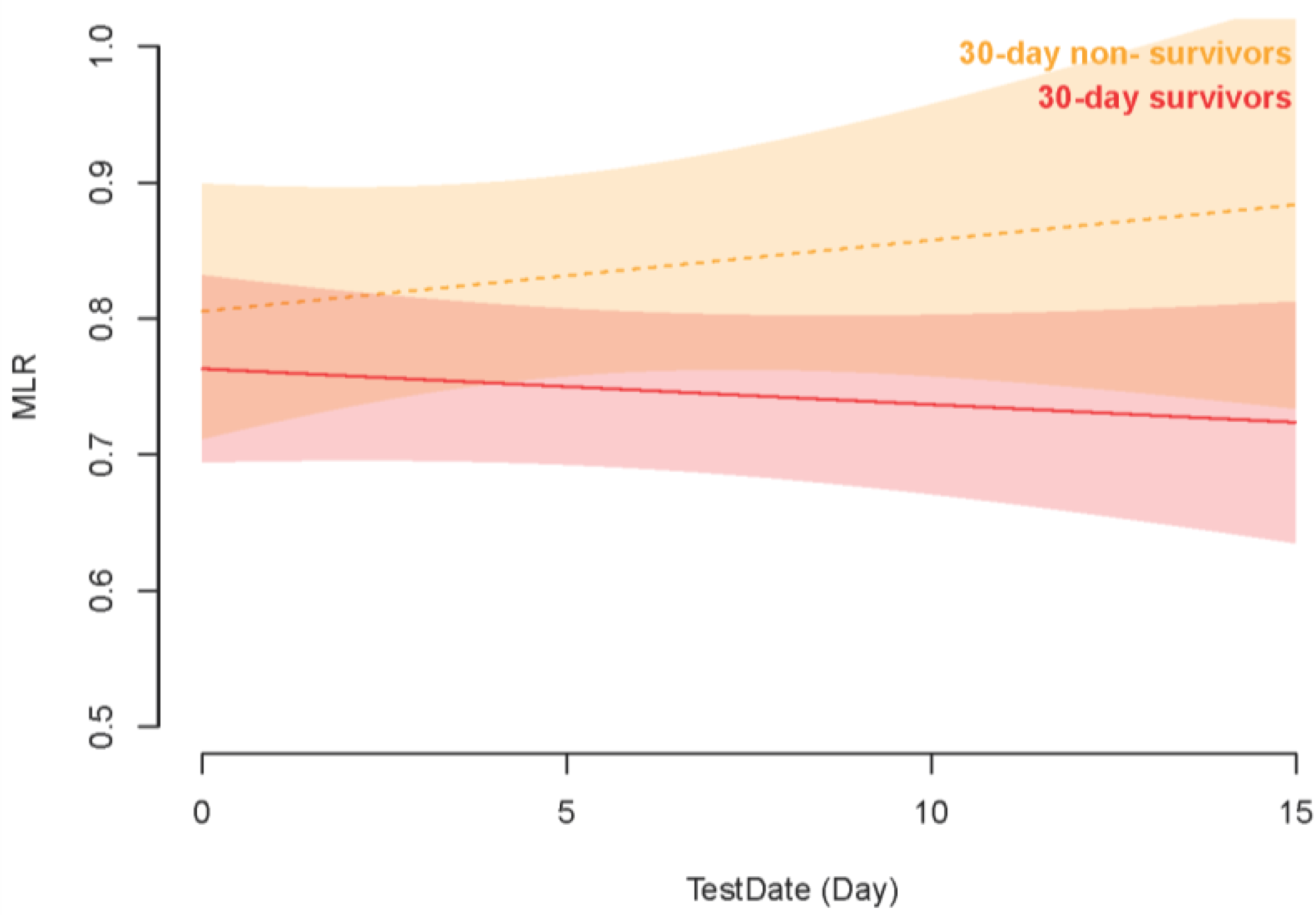
3.5. Association between Early Changes in MLR and Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ronco, C.; Bellomo, R.; Kellum, J.A. Acute kidney injury. Lancet 2019, 394, 1949–1964. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Xing, G.; Wang, L.; Wu, Y.; Li, S.; Xu, G.; He, Q.; Chen, J.; Chen, M.; Liu, X.; et al. Acute kidney injury in China: A cross-sectional survey. Lancet 2015, 386, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Cerdá, J.; Burdmann, E.A.; Tonelli, M.; García-García, G.; Jha, V.; Susantitaphong, P.; Rocco, M.; Vanholder, R.; Sever, M.S.; et al. International Society of Nephrology’s 0by25 initiative for acute kidney injury (zero preventable deaths by 2025): A human rights case for nephrology. Lancet 2015, 385, 2616–2643. [Google Scholar] [CrossRef]
- Haase, M.; Bellomo, R.; Devarajan, P.; Schlattmann, P.; Haase-Fielitz, A.; NGAL Meta-Analysis Investigator Group. Accuracy of Neutrophil Gelatinase-Associated Lipocalin (NGAL) in Diagnosis and Prognosis in Acute Kidney Injury: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2009, 54, 1012–1024. [Google Scholar] [CrossRef] [PubMed]
- Westhoff, J.H.; Seibert, F.S.; Waldherr, S.; Bauer, F.; Tönshoff, B.; Fichtner, A.; Westhoff, T.H. Urinary calprotectin, kidney injury molecule-1, and neutrophil gelatinase-associated lipocalin for the prediction of adverse outcome in pediatric acute kidney injury. Eur. J. Pediatr. 2017, 176, 745–755. [Google Scholar] [CrossRef] [PubMed]
- Jiang, L.; Wang, Z.; Wang, L.; Liu, Y.; Chen, D.; Zhang, D.; Shi, X.; Xiao, D. Predictive value of the serum anion gap for 28-day in-hospital all-cause mortality in sepsis patients with acute kidney injury: A retrospective analysis of the MIMIC-IV database. Ann. Transl. Med. 2022, 10, 1373. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.; Liao, L.; Pan, L.; Pinhu, L. Association between the Central Venous Pressure and All-Cause Mortality in Critically Ill Patients with Acute Kidney Injury. Int. J. Gen. Med. 2021, 14, 8019–8027. [Google Scholar] [CrossRef]
- Liu, K.D.; Goldstein, S.L.; Vijayan, A.; Parikh, C.R.; Kashani, K.; Okusa, M.D.; Agarwal, A.; Cerdá, J. AKI!Now Initiative: Recommendations for Awareness, Recognition, and Management of AKI. Clin. J. Am. Soc. Nephrol. 2020, 15, 1838–1847. [Google Scholar] [CrossRef]
- Schrezenmeier, E.V.; Barasch, J.; Budde, K.; Westhoff, T.; Schmidt-Ott, K.M. Biomarkers in acute kidney injury—Pathophysiological basis and clinical performance. Acta Physiol. 2017, 219, 556–574. [Google Scholar] [CrossRef]
- Rabb, H.; Griffin, M.D.; McKay, D.B.; Swaminathan, S.; Pickkers, P.; Rosner, M.H.; Kellum, J.A.; Ronco, C. Inflammation in AKI. J. Am. Soc. Nephrol. 2016, 27, 371–379. [Google Scholar] [CrossRef]
- Fu, Y.; Xiang, Y.; Li, H.; Chen, A.; Dong, Z. Inflammation in kidney repair: Mechanism and therapeutic potential. Pharmacol. Ther. 2022, 237, 108240. [Google Scholar] [CrossRef] [PubMed]
- Tadagavadi, R.; Reeves, W.B. Neutrophils in cisplatin AKI—Mediator or marker? Kidney Int. 2017, 92, 11–13. [Google Scholar] [CrossRef] [PubMed]
- Jansen, M.P.B.; Florquin, S.; Roelofs, J.J.T.H. The role of platelets in acute kidney injury. Nat. Rev. Nephrol. 2018, 14, 457–471. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.-F.; Liu, W.-Y.; Zeng, F.-F.; Zheng, M.-H.; Shi, H.-Y.; Zhou, Y.; Pan, J.-Y. Prognostic value of platelet-to-lymphocyte ratios among critically ill patients with acute kidney injury. Crit. Care 2017, 21, 238. [Google Scholar] [CrossRef]
- Yue, S.; Zhang, J.; Wu, J.; Teng, W.; Liu, L.; Chen, L. Use of the Monocyte-to-Lymphocyte Ratio to Predict Diabetic Retinopathy. Int. J. Environ. Res. Public Health 2015, 12, 10009–10019. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Long, W.; Li, P.-F.; Lin, Y.-B.; Liang, Y. An Elevated Peripheral Blood Monocyte-to-Lymphocyte Ratio Predicts Poor Prognosis in Patients with Primary Pulmonary Lymphoepithelioma-like Carcinoma. PLoS ONE 2015, 10, e0126269. [Google Scholar] [CrossRef]
- Djordjevic, D.; Rondovic, G.; Surbatovic, M.; Stanojevic, I.; Udovicic, I.; Andjelic, T.; Zeba, S.; Milosavljevic, S.; Stankovic, N.; Abazovic, D.; et al. Neutrophil-to-Lymphocyte Ratio, Monocyte-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, and Mean Platelet Volume-to-Platelet Count Ratio as Biomarkers in Critically Ill and Injured Patients: Which Ratio to Choose to Predict Outcome and Nature of Bacteremia? Mediat. Inflamm. 2018, 2018, 3758068. [Google Scholar] [CrossRef]
- Tian, T.; Wei, B.; Wang, J. Study of C-reactive protein, procalcitonin, and immunocyte ratios in 194 patients with sepsis. BMC Emerg. Med. 2021, 21, 81. [Google Scholar] [CrossRef]
- Chen, H.; Wu, X.; Wen, Z.; Zhu, Y.; Liao, L.; Yang, J. The Clinicopathological and Prognostic Value of NLR, PLR and MLR in Non-Muscular Invasive Bladder Cancer. Arch. Esp. De Urol. 2022, 75, 467. [Google Scholar] [CrossRef]
- Hepokoski, M.; Singh, P. Mitochondria as mediators of systemic inflammation and organ cross talk in acute kidney injury. Am. J. Physiol. Ren. Physiol. 2022, 322, F589–F596. [Google Scholar] [CrossRef]
- Jiang, F.; Lei, J.; Xiang, J.; Chen, Y.; Feng, J.; Xu, W.; Ou, J.; Yang, B.; Zhang, L. Monocyte-to-lymphocyte ratio: A potential novel predictor for acute kidney injury in the intensive care unit. Ren. Fail. 2022, 44, 1004–1011. [Google Scholar] [CrossRef]
- Su, X.; Wang, J.; Lu, X. The association between Monocyte-to-Lymphocyte ratio and postoperative delirium in ICU patients in cardiac surgery. Clin. Lab. Anal. 2022, 36, e24553. [Google Scholar] [CrossRef] [PubMed]
- Jiang, F.; Shi, Z.; Liu, X.; Xiang, J.; Lei, J.; Yang, B.; Lei, X.; Li, X. The Role of the Monocyte-to-Lymphocyte Ratio in Acute Ischemic Stroke Patients with Acute Kidney Injury. Mediat. Inflamm. 2022, 2022, 7911033. [Google Scholar] [CrossRef] [PubMed]
- Lameire, N.H.; Levin, A.; Kellum, J.A.; Cheung, M.; Jadoul, M.; Winkelmayer, W.C.; Stevens, P.E.; Caskey, F.J.; Farmer, C.K.; Fuentes, A.F.; et al. Harmonizing acute and chronic kidney disease definition and classification: Report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Int. 2021, 100, 516–526. [Google Scholar] [CrossRef] [PubMed]
- Harre, F.E.; Lee, K.L.; Pollock, B.G. Regression Models in Clinical Studies: Determining Relationships between Predictors and Response. JNCI J. Natl. Cancer Inst. 1988, 80, 1198–1202. [Google Scholar] [CrossRef] [PubMed]
- Fan, L.L.; Wang, Y.J.; Nan, C.J.; Chen, Y.H.; Su, H.X. Neutrophil-lymphocyte ratio is associated with all-cause mortality among critically ill patients with acute kidney injury. Clin. Chim. Acta 2019, 490, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Schiffl, H.; Lang, S.M. Neutrophil-to-lymphocyte ratio—A new diagnostic and prognostic marker of acute kidney injury. Barriers to broad clinical application. Int. Urol. Nephrol. 2023, 55, 101–106. [Google Scholar] [CrossRef]
- Lee, S.; Huen, S.; Nishio, H.; Nishio, S.; Lee, H.K.; Choi, B.-S.; Ruhrberg, C.; Cantley, L.G. Distinct Macrophage Phenotypes Contribute to Kidney Injury and Repair. J. Am. Soc. Nephrol. 2011, 22, 317–326. [Google Scholar] [CrossRef]
- Lin, S.L.; Castaño, A.P.; Nowlin, B.T.; Lupher, M.L.; Duffield, J.S. Bone Marrow Ly6Chigh Monocytes Are Selectively Recruited to Injured Kidney and Differentiate into Functionally Distinct Populations. J. Immunol. 2009, 183, 6733–6743. [Google Scholar] [CrossRef]
- Kielar, M.L.; John, R.; Bennett, M.; Richardson, J.A.; Shelton, J.M.; Chen, L.; Jeyarajah, D.R.; Zhou, X.J.; Zhou, H.; Chiquett, B.; et al. Maladaptive Role of IL-6 in Ischemic Acute Renal Failure. J. Am. Soc. Nephrol. 2005, 16, 3315–3325. [Google Scholar] [CrossRef]
- Guo, C.; Fan, Y.; Cheng, J.; Deng, Y.; Zhang, X.; Chen, Y.; Jing, H.; Li, W.; Liu, P.; Xie, J.; et al. AFM negatively regulates the infiltration of monocytes to mediate sepsis-associated acute kidney injury. Front. Immunol. 2023, 14, 1049536. [Google Scholar] [CrossRef] [PubMed]
- Kinsey, G.R.; Sharma, R.; Huang, L.; Li, L.; Vergis, A.L.; Ye, H.; Ju, S.-T.; Okusa, M.D. Regulatory T Cells Suppress Innate Immunity in Kidney Ischemia-Reperfusion Injury. J. Am. Soc. Nephrol. 2009, 20, 1744–1753. [Google Scholar] [CrossRef] [PubMed]
- de Jager, C.P.; van Wijk, P.T.; Mathoera, R.B.; de Jongh-Leuvenink, J.; van der Poll, T.; Wever, P.C. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit. Care 2010, 14, R192. [Google Scholar] [CrossRef] [PubMed]
- Robbins, C.S.; Swirski, F.K. The multiple roles of monocyte subsets in steady state and inflammation. Cell. Mol. Life Sci. 2010, 67, 2685–2693. [Google Scholar] [CrossRef]
- Drewry, A.M.; Samra, N.; Skrupky, L.P.; Fuller, B.M.; Compton, S.M.; Hotchkiss, R.S. Persistent Lymphopenia after Diagnosis of Sepsis Predicts Mortality. Shock 2014, 42, 383–391. [Google Scholar] [CrossRef]
- Jiang, F.; Liu, J.; Yu, X.; Li, R.; Zhou, R.; Ren, J.; Liu, X.; Zhao, S.; Yang, B. The Monocyte-to-Lymphocyte Ratio Predicts Acute Kidney Injury after Acute Hemorrhagic Stroke. Front. Neurol. 2022, 13, 904249. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Xu, Y.; Lu, P.; Zhou, H.; Yang, M.; Xiang, L. The prognostic value of monocyte-to-lymphocyte ratio in peritoneal dialysis patients. Eur. J. Med. Res. 2023, 28, 152. [Google Scholar] [CrossRef]
- Xiang, F.; Chen, R.; Cao, X.; Shen, B.; Liu, Z.; Tan, X.; Ding, X.; Zou, J. Monocyte/lymphocyte ratio as a better predictor of cardiovascular and all-cause mortality in hemodialysis patients: A prospective cohort study. Hemodial. Int. 2018, 22, 82–92. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Russu, E.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Arbănași, E.M.; Voidăzan, S.T. The Predictive Value of NLR, MLR, and PLR in the Outcome of End-Stage Kidney Disease Patients. Biomedicines 2022, 10, 1272. [Google Scholar] [CrossRef]
- Liberski, P.S.; Szewczyk, M.; Krzych, Ł.J. Haemogram-Derived Indices for Screening and Prognostication in Critically Ill Septic Shock Patients: A Case-Control Study. Diagnostics 2020, 10, 638. [Google Scholar] [CrossRef]
- Hsu, Y.-C.; Yang, Y.-Y.; Tsai, I.-T. Lymphocyte-to-monocyte ratio predicts mortality in cirrhotic patients with septic shock. Am. J. Emerg. Med. 2021, 40, 70–76. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Monocyte-to-Lymphocyte Ratio | p Value | ||
|---|---|---|---|---|
| All Patients | <0.48 | ≥0.48 | ||
| MLR | 0.44 [0.25, 0.77] | 0.26 [0.18, 0.36] | 0.80 [0.61, 1.19] | <0.001 |
| Age, years | 67.56 (15.83) | 67.03 (15.52) | 68.17 (16.16) | <0.001 |
| Sex, n (%) | 0.953 | |||
| Female | 6648 (41.6) | 3585 (41.8) | 3063 (41.3) | |
| Ethnicity | 0.001 | |||
| White, n (%) | 10,820 (67.7) | 5784 (67.4) | 5036 (68.0) | |
| Black, n (%) | 1381 (8.6) | 807 (9.4) | 574 (7.7) | |
| Other, n (%) | 3785 (23.7) | 1986 (23.2) | 1799 (24.3) | |
| SBP, mmHg | 123.1 (24.8) | 122.3 (24.4) | 124.0 (25.3) | 0.002 |
| DBP, mmHg | 67.6 (18.2) | 66.5 (17.5) | 69.0 (18.9) | <0.001 |
| Heart rate, beats/minute | 86.0 [76.0, 100.0] | 82.0 [74.0, 95.0] | 86.0 [76.0, 100.0] | <0.001 |
| Respiratory rate, /minute | 19.3 (6.0) | 18.3 (5.7) | 20.4 (6.3) | <0.001 |
| Temperature, °C | 36.64 (0.85) | 36.54 (0.84) | 36.75 (0.85) | <0.001 |
| SpO2, % | 98.00 [96.00, 100.00] | 99.00 [96.00, 100.00] | 98.00 [95.00, 100.00] | <0.001 |
| Vasoactive use (%) | 7774 (48.6) | 4339 (50.6) | 3435 (46.4) | <0.001 |
| Ventilator use (%) | 8681 (54.3) | 4770 (55.6) | 3911 (52.8) | 0.006 |
| Comorbidities | ||||
| Hypertension, n (%) | 9365 (58.6) | 5089 (59.3) | 4276 (57.7) | 0.040 |
| Diabetes, n (%) | 5253 (32.9) | 2946 (34.3) | 2307 (31.1) | <0.001 |
| Coronary artery disease, n (%) | 5969 (37.3) | 3736 (43.6) | 2233 (30.1) | <0.001 |
| COPD, n (%) | 1860 (11.6) | 836 (9.7) | 1024 (13.8) | <0.001 |
| Malignancy, n (%) | 1636 (10.2) | 589 (6.9) | 1047 (14.1) | <0.001 |
| Liver disease, n (%) | 2413 (15.1) | 965 (11.3) | 1448 (19.5) | <0.001 |
| Deficiency anemias, n (%) | 8097 (50.7) | 4280 (49.9) | 3817 (51.5) | 0.043 |
| Atrial fibrillation (%) | 2940 (18.4) | 1405 (16.4) | 1535 (20.7) | <0.001 |
| Shock (%) | 2474 (15.5) | 946 (11.0) | 1528 (20.6) | <0.001 |
| Sepsis (%) | 9921 (62.1) | 4746 (55.3) | 5175 (69.8) | <0.001 |
| Laboratory parameters | ||||
| Hematocrit, % | 33.30 [28.10, 38.80] | 32.60 [27.70, 38.40] | 34.00 [28.70, 39.20] | <0.001 |
| Hemoglobin, g/dL | 10.90 [9.20, 12.80] | 10.80 [9.10, 12.70] | 11.10 [9.30, 12.90] | <0.001 |
| Platelet count, 109/L | 196.00 [140.00, 267.00] | 187.00 [135.00, 257.00] | 205.00 [148.00, 278.00] | <0.001 |
| WBC, 109/L | 11.60 [8.40, 15.90] | 10.50 [7.80, 14.20] | 13.00 [9.60, 17.90] | <0.001 |
| RDW, % | 14.30 [13.30, 15.80] | 14.00 [13.20, 15.30] | 14.60 [13.50, 16.30] | <0.001 |
| MCV, fL | 92.00 [88.00, 96.00] | 91.00 [87.00, 95.00] | 92.00 [88.00, 97.00] | <0.001 |
| INR | 1.30 [1.10, 1.50] | 1.30 [1.10, 1.50] | 1.30 [1.10, 1.60] | <0.001 |
| Serum creatinine, mg/dL | 1.00 [0.80, 1.60] | 1.00 [0.80, 1.40] | 1.10 [0.80, 1.80] | <0.001 |
| BUN, mg/dL | 20.00 [14.00, 33.00] | 18.00 [13.00, 28.00] | 23.00 [16.00, 39.00] | <0.001 |
| Glucose, mg/dL | 130.00 [107.00, 167.00] | 126.00 [106.00, 158.00] | 136.00 [110.00, 177.00] | <0.001 |
| Serum sodium, mmol/L | 139.00 [136.00, 141.00] | 139.00 [136.00, 141.00] | 138.00 [135.00, 141.00] | <0.001 |
| Serum chloride, mmol/L | 104.00 [99.00, 108.00] | 105.00 [101.00, 109.00] | 102.00 [98.00, 106.00] | <0.001 |
| Serum bicarbonate, mmol/L | 23.00 [20.00, 25.00] | 23.00 [21.00, 25.00] | 23.00 [20.00, 25.00] | <0.001 |
| Anion gap, mmol/L | 15.00 [12.00, 18.00] | 14.00 [12.00, 17.00] | 16.00 [13.00, 19.00] | <0.001 |
| Serum potassium, mmol/L | 4.20 [3.80, 4.70] | 4.20 [3.80, 4.60] | 4.30 [3.80, 4.80] | <0.001 |
| Scoring systems | ||||
| GCS | 14.00 [10.00, 15.00] | 14.00 [10.00, 15.00] | 13.00 [9.00, 15.00] | <0.001 |
| SOFA | 5.00 [3.00, 8.00] | 5.00 [3.00, 7.00] | 6.00 [3.00, 9.00] | <0.001 |
| Renal function | ||||
| Urine output, mL/24 h | 1802 (1205.03) | 1889.77 (1145.03) | 1686.52 (1270.25) | <0.001 |
| AKI KDIGO stage, n (%) | <0.001 | |||
| Stage-1 | 4053 (25.4) | 2477 (28.9) | 1576 (21.3) | |
| Stage-2 | 8034 (50.3) | 4464 (52.0) | 3570 (48.2) | |
| Stage-3 | 3899 (24.4) | 1636 (19.1) | 2263 (30.5) | |
| Renal replacement therapy, n (%) | 849 (5.3) | 335 (3.9) | 514 (6.9) | <0.001 |
| Monocyte-to-Lymphocyte Ratio | No. of Patients/Deaths | Model 1 | Model 2 | ||
|---|---|---|---|---|---|
| HR (95% CIs) | p Value | HR (95% CIs) | p Value | ||
| 30-Day mortality | |||||
| Fitted groups | |||||
| <0.48 | 8577/1076 | 1.00 | 1.00 | ||
| ≥0.48 | 7409/1874 | 2.11 (1.96–2.28) | <0.001 | 1.33 (1.24–1.45) | <0.001 |
| Tertiles | |||||
| <0.33 | 5329/568 | 1.00 | 1.00 | ||
| 0.33–0.66 | 5328/946 | 1.65 (1.48–1.85) | <0.001 | 1.20 (1.07–1.33) | 0.007 |
| ≥0.66 | 5329/1436 | 2.55 (2.30–2.83) | <0.001 | 1.36 (1.23–1.52) | <0.001 |
| 90-Day mortality | |||||
| Fitted groups | |||||
| <0.48 | 8577/1426 | 1.00 | 1.00 | ||
| ≥0.48 | 7409/2398 | 2.09 (1.96–2.23) | <0.001 | 1.34 (1.25–1.44) | <0.001 |
| Tertiles | |||||
| <0.33 | 5329/729 | 1.00 | 1.00 | ||
| 0.33–0.66 | 5328/1269 | 1.81 (1.65–1.98) | <0.001 | 1.28 (1.16–1.40) | <0.001 |
| ≥0.66 | 5329/1826 | 2.73 (2.51–2.98) | <0.001 | 1.44 (1.31–1.58) | <0.001 |
| Unadjusted β (95% CI) | p-Value | Adjusted Model I β (95% CI) | p-Value | Adjusted Model II β (95% CI) | p-Value | |
|---|---|---|---|---|---|---|
| 30-day mortality | −0.176 (−0.230, −0.123) | <0.001 | −0.146 (−0.201, −0.091) | <0.001 | −0.079 (−0.137, −0.029) | 0.006 |
| Day | 0.205 (0.195, 0.214) | <0.001 | 0.119 (0.091, 0.146) | <0.001 | 0.252 (0.024, 0.480) | 0.029 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, X.; Wan, D.; Xia, R.; Liao, R.; Su, B. Prognostic Value of the Baseline and Early Changes in Monocyte-to-Lymphocyte Ratio for Short-Term Mortality among Critically Ill Patients with Acute Kidney Injury. J. Clin. Med. 2023, 12, 7353. https://doi.org/10.3390/jcm12237353
Luo X, Wan D, Xia R, Liao R, Su B. Prognostic Value of the Baseline and Early Changes in Monocyte-to-Lymphocyte Ratio for Short-Term Mortality among Critically Ill Patients with Acute Kidney Injury. Journal of Clinical Medicine. 2023; 12(23):7353. https://doi.org/10.3390/jcm12237353
Chicago/Turabian StyleLuo, Xinyao, Dingyuan Wan, Ruoxin Xia, Ruoxi Liao, and Baihai Su. 2023. "Prognostic Value of the Baseline and Early Changes in Monocyte-to-Lymphocyte Ratio for Short-Term Mortality among Critically Ill Patients with Acute Kidney Injury" Journal of Clinical Medicine 12, no. 23: 7353. https://doi.org/10.3390/jcm12237353
APA StyleLuo, X., Wan, D., Xia, R., Liao, R., & Su, B. (2023). Prognostic Value of the Baseline and Early Changes in Monocyte-to-Lymphocyte Ratio for Short-Term Mortality among Critically Ill Patients with Acute Kidney Injury. Journal of Clinical Medicine, 12(23), 7353. https://doi.org/10.3390/jcm12237353