
Clinical Characteristics of Individuals with Interstitial Lung Diseases and Indication of End-of-Life Care

 ,
,  ,
,  , and
, and
Abstract
1. Introduction
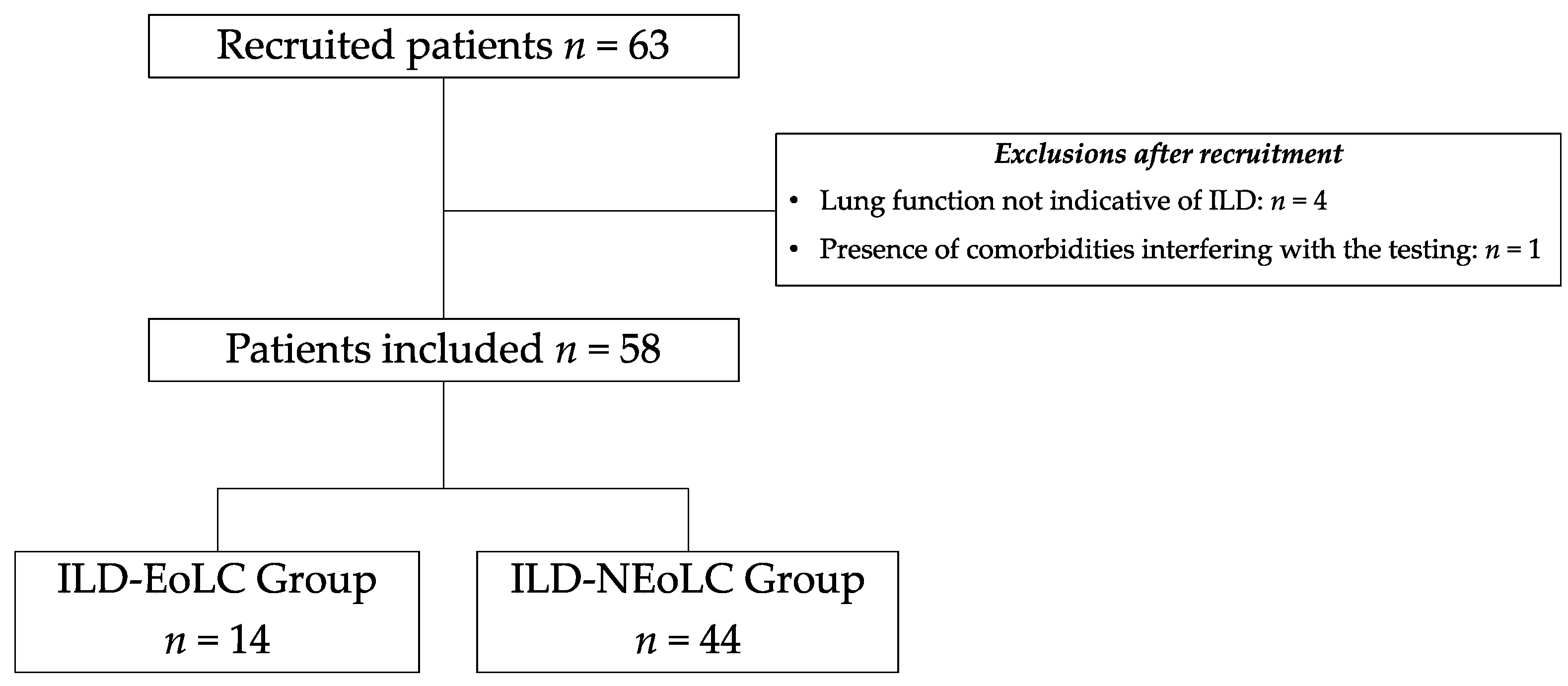
2. Materials and Methods
2.1. Study Design and Ethical Aspects
2.2. Sample Characteristics
2.3. Assessments
2.4. Indication for End-of-Life Care
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Guedes Baldi, B.; Alberto, C.; Pereira, C.; Rubin, A.S.; Nicodemos, A.; Santana, C.; Costa, N.; Roberto, C.; Carvalho, R.; Algranti, E.; et al. Destaques das Diretrizes de Doenças Pulmonares Intersticiais da Sociedade Brasileira de Pneumologia e Tisiologia. J. Bras. Pneumol. 2012, 38, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of idiopathic pulmonary fibrosis An Official ATS/ERS/JRS/ALAT Clinical practice guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef] [PubMed]
- Rajala, K.; Lehto, J.T.; Sutinen, E.; Kautiainen, H.; Myllärniemi, M.; Saarto, T. Marked deterioration in the quality of life of patients with idiopathic pulmonary fibrosis during the last two years of life. BMC Pulm. Med. 2018, 18, 172. [Google Scholar] [CrossRef] [PubMed]
- Aronson, K.I.; Swigris, J.J.; Bajwah, S.; Bianchi, P.; Corte, T.J.; Danoff, S.K.; Lee, J.S.; Lindell, K.O.; Maher, T.; Martinez, F.J.; et al. Patient-centered outcomes research in interstitial lung disease: An official american thoracic society research statement. Am. J. Respir. Crit. Care Med. 2021, 204, E3–E23. [Google Scholar] [CrossRef]
- Rajala, K.; Lehto, J.T.; Saarinen, M.; Sutinen, E.; Saarto, T.; Myllärniemi, M. End-of-life care of patients with idiopathic pulmonary fibrosis. BMC Palliat. Care 2016, 15, 1–6. [Google Scholar] [CrossRef]
- Kreuter, M.; Bendstrup, E.; Russell, A.M.; Bajwah, S.; Lindell, K.; Adir, Y.; Brown, C.E.; Calligaro, G.; Cassidy, N.; Corte, T.J.; et al. Palliative care in interstitial lung disease: Living well. Lancet Respir. Med. 2017, 5, 968–980. [Google Scholar] [CrossRef] [PubMed]
- Marsaa, K.; Gundestrup, S.; Jensen, J.U.; Lange, P.; Løkke, A.; Roberts, N.B.; Shaker, S.B.; Sørensen, A.R.; Titlestad, I.L.; Thomsen, L.H.; et al. Danish respiratory society position paper: Palliative care in patients with chronic progressive non-malignant lung diseases. Eur. Clin. Respir. J. 2018, 5, 1530029. [Google Scholar] [CrossRef] [PubMed]
- Chai, G.T.; Neo, H.Y.; Abisheganaden, J.; Hum, A.Y.M. Impact of Palliative Care in End-of-Life of Fibrotic Interstitial Lung Disease Patients. Am. J. Hosp. Palliat. Med. 2022, 39, 1443–1451. [Google Scholar] [CrossRef]
- World Health Organization. National Cancer Control Programmes: Policies and Managerial Guidelines; WHO Library: Geneva, Switzerland, 2002; Volume 2, pp. 1–181. [Google Scholar]
- National Institute for Health and Care Excellence. Guidelines. End of Life Care for Adults: Service Delivery; NICE: London, UK, 2019; pp. 1–17. [Google Scholar]
- Alberto, C.; Pereira, C.; Sato, T.; Rodrigues, S.C. New reference values for forced spirometry in white adults in Brazil. J. Bras. Pneumol. 2007, 33, 397–406. [Google Scholar]
- Crapo, R.O.; Morris, A.H. Standardized Single Breath Normal Values for Carbon Monoxide Diffusing Capacity. Am. Rev. Respir. Dis. 1981, 123, 185–189. [Google Scholar]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European respiratory society/American thoracic society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef]
- Britto, R.R.; Probst, V.S.; Dornelas De Andrade, A.F.; Samora, G.A.R.; Hernandes, N.A.; Marinho, P.E.M.; Karsten, M.; Pitta, F.; Parreira, V.F. Reference equations for the six-minute walk distance based on a Brazilian multicenter study. Braz. J. Phys. Ther. 2013, 17, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Byrom, B.; Rowe, D.A. Measuring free-living physical activity in COPD patients: Deriving methodology standards for clinical trials through a review of research studies. Contemp. Clin. Trials 2016, 47, 172–184. [Google Scholar] [CrossRef] [PubMed]
- Podsiadlo, D.; Richardson, S. The Timed Up and Go: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Murray, S.M.; Chapman, K.; Munro, B.; Tiedemann, A. Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Zamboti, C.L.; Gonçalves, A.F.L.; Garcia, T.; Krinski, G.G.; Bertin, L.D.; Almeida, H.d.S.; Pimpão, H.A.; Fujisawa, D.S.; Ribeiro, M.; Pitta, F.; et al. Functional performance tests in interstitial lung disease: Impairment and measurement properties. Respir. Med. 2021, 184, 106413. [Google Scholar] [CrossRef] [PubMed]
- Furlanetto, K.C.; Correia, N.S.; Mesquita, R.; Morita, A.A.; do Amaral, D.P.; Mont’Alverne, D.G.B.; Pereira, D.M.; Pitta, F.; Dal Corso, S. Reference Values for 7 Different Protocols of Simple Functional Tests: A Multicenter Study. Arch. Phys. Med. Rehabil. 2022, 103, 20–28.e5. [Google Scholar] [CrossRef] [PubMed]
- Hopkinson, N.S.; Tennant, R.C.; Dayer, M.J.; Swallow, E.B.; Hansel, T.T.; Moxham, J.; Polkey, M.I. A prospective study of decline in fat free mass and skeletal muscle strength in chronic obstructive pulmonary disease. Respir. Res. 2007, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kendall, F.P.; McCreary, E.; Provance, P.; Rodgers, M.; Romani, W. Músculos Provas e Funções, 5th ed.; MANOLE: Barueri, Brazil, 2007. [Google Scholar]
- Hyatt, R.; Black, L. Maximal Respiratory Pressures: Normal Values and relationship to age and sex. Am. Rev. Respir. Dis. 1969, 99, 696–702. [Google Scholar]
- Neder, J.A.; Andreoni, S.; Lerario, M.C.; Nery, L.E. Muscle respiratory strength in healthy subjects. Braz. J. Med. Biol. Res. 1999, 32, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C. Methods for the assessment of human body composition: Traditional and new. Am. J. Clin. Nutr. 1987, 46, 537–556. [Google Scholar] [CrossRef]
- Yorke, J.; Jones, P.W.; Swigris, J.J. Development and validity testing of an ipf-specific version of the St George’s respiratory questionnaire. Thorax 2010, 65, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, W.F.; Mantoani, L.C.; Silva, H.; Zamboti, C.L.; Garcia, T.; Cavalheri, V.; Ribeiro, M.; Yorke, J.; Pitta, F.; Camillo, C.A. Translation, cross-cultural adaptation, and measurement properties of the Brazilian-Portuguese version of the idiopathic pulmonary fibrosis-specific version of the Saint George’s Respiratory Questionnaire (SGRQ-I) for patients with interstitial lung disea. Braz. J. Phys. Ther. 2021, 25, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Eakin, E.G.; Resnikoff, P.M.; Prewitt, L.M.; Ries, A.L.; Kaplan, R.M. Validation of a new dyspnea measure: The UCSD Shortness of Breath Questionnaire. Chest 1998, 113, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Silva, H.; Mantoani, L.C.; Zamboti, C.L.; Aguiar, W.F.; Ries, A.L.; Gonçalves, A.F.L.; da Silva, T.G.; Ribeiro, M.; Pitta, F.; Camillo, C.A. Validation of the Brazilian Portuguese version of the University of California San Diego Shortness of Breath Questionnaire in patients with interstitial lung disease. J. Bras. Pneumol. 2021, 47, e20210172. [Google Scholar] [CrossRef] [PubMed]
- Snaith, R.; Zigmond, A. The hospital anxiety anddepression scale. Br. Med. J. 1986, 1, 344–345. [Google Scholar] [CrossRef]
- Botega, N.J.; Bio, M.R.; Zomignani, M.A.; Garcia, C., Jr.; Pereira, W.A.B. Transtornos do humor em enfermaria de clínica médica e validação de escala de medida (HAD) de ansiedade e depressão. Rev. Saude Publica 1995, 29, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Zou, R.H.; Nouraie, M.; Chen, X.; Saul, M.I.; Kaminski, N.; Gibson, K.F.; Kass, D.J.; Lindell, K.O. Assessing Patterns of Palliative Care Referral and Location of Death in Patients with Idiopathic Pulmonary Fibrosis: A Sixteen-Year Single-Center Retrospective Cohort Study. J. Palliat. Med. 2019, 22, 538–544. [Google Scholar] [CrossRef]
- Zou, R.H.; Kass, D.J.; Gibson, K.F.; Lindell, K.O. The Role of Palliative Care in Reducing Symptoms and Improving Quality of Life for Patients with Idiopathic Pulmonary Fibrosis: A Review. Pulm. Ther. 2020, 6, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Caminati, A.; Bianchi, A.; Cassandro, R.; Rosa Mirenda, M.; Harari, S. Walking distance on 6-MWT is a prognostic factor in idiopathic pulmonary fibrosis. Respir. Med. 2009, 103, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Lederer, D.J.; Arcasoy, S.M.; Wilt, J.S.; D’Ovidio, F.; Sonett, J.R.; Kawut, S.M. Six-minute-walk distance predicts waiting list survival in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2006, 174, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Dowman, L.; Fiore, J.; Brazzale, D.; Hill, C.J.; McDonald, C.F. Cardiorespiratory responses to 6-minute walk test in interstitial lung disease: Not always a submaximal test. BMC Pulm. Med. 2014, 14, 136. [Google Scholar] [CrossRef] [PubMed]
- Mancuzo, E.V.; Soares, M.R.; Pereira, C.A.d.C. Six-minute walk distance and survival time in patients with idiopathic pulmonary fibrosis in Brazil. J. Bras. Pneumol. 2018, 44, 267–272. [Google Scholar] [CrossRef]
- Rocha, V.; Paixão, C.; Marques, A. Physical activity, exercise capacity and mortality risk in people with interstitial lung disease: A systematic review and meta-analysis. J. Sci. Med. Sport 2022, 25, 903–910. [Google Scholar] [CrossRef]
- Wallaert, B.; Monge, E.; Le Rouzic, O.; Wémeau-Stervinou, L.; Salleron, J.; Grosbois, J.M. Physical activity in daily life of patients with fibrotic idiopathic interstitial pneumonia. Chest 2013, 144, 1652–1658. [Google Scholar] [CrossRef]
- Puhan, M.A.; Siebeling, L.; Zoller, M.; Muggensturm, P.; Riet, G. Ter Simple functional performance tests and mortality in COPD. Eur. Respir. J. 2013, 42, 956–963. [Google Scholar] [CrossRef]
- Marquis, K.; Debigaré, R.; Lacasse, Y.; Leblanc, P.; Jobin, J.; Carrier, G.; Maltais, F. Midthigh muscle cross-sectional area is a better predictor of mortality than body mass index in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2002, 166, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Matsunuma, R.; Takato, H.; Takeda, Y.; Watanabe, S.; Waseda, Y.; Murakami, S.; Kawaura, Y.; Kasahara, K. Patients with end-stage interstitial lung disease may have more problems with dyspnea than end-stage lung cancer patients. Indian J. Palliat. Care 2016, 22, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Bosi, M.; Milioli, G.; Parrino, L.; Fanfulla, F.; Tomassetti, S.; Melpignano, A.; Trippi, I.; Vaudano, A.E.; Ravaglia, C.; Mascetti, S.; et al. Quality of life in idiopathic pulmonary fibrosis: The impact of sleep disordered breathing. Respir. Med. 2019, 147, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.G.; Teoh, A.; Roberts, M.; Wheatley, J. The prevalence of poor sleep quality and its associated factors in patients with interstitial lung disease: A cross-sectional analysis. ERJ Open Res. 2019, 5, 00062. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Indications of EOLC for Individuals with ILD |
|---|
|
| Variables | ILD-EOLC (n = 14) | ILD-nEOLC (n = 44) | p |
|---|---|---|---|
| Sex, female (%) | 8 (57%) | 25 (59%) | 0.89 |
| Age, years | 62 ± 10 | 60 ± 10 | 0.27 |
| Time since diagnosis, months | 60 [24–102] | 72 [36–132] | 0.18 |
| Home oxygen therapy, n | 6 (42%) | 8 (18%) | 0.02 |
| Deaths, number | 11 (78%) | 3 (7%) | <0.0001 |
| Time of death, months | 3 [2–11] | 7 [5–10] | 0.14 |
| Diagnosis | |||
| Idiopathic pulmonary fibrosis, n | 11 (79%) | 17 (39%) | 0.01 |
| Connective-tissue-disease-associated ILD, n | 3 (21%) | 22 (50%) | 0.07 |
| Sarcoidosis, n | 0 (0%) | 2 (5%) | 0.99 |
| Asbestosis, n | 0 (0%) | 1 (2%) | 0.99 |
| Non-specific interstitial pneumonia, n | 0 (0%) | 1 (2%) | 0.99 |
| Other ILD, n | 0 (0%) | 1 (2%) | 0.99 |
| Disease Staging | |||
| GAP I, % | 1 (7%) | 33 (75%) | |
| GAP II, % | 8 (57%) | 11 (25%) | |
| GAP III, % | 5 (36%) | 0 (0%) | <0.0001 |
| Comorbidities, n | |||
| 0–3 | 4 (29%) | 21 (48%) | |
| 4–6 | 7 (50%) | 11 (25%) | |
| ≥7 | 3 (21%) | 12 (27%) | 0.20 |
| Pharmacological treatment | |||
| Antifibrotics | 1 (7%) | 1 (2%) | 0.42 |
| Corticosteroids | 5 (35%) | 17 (38%) | 0.93 |
| Immunosuppressants | 5 (35%) | 21 (47%) | 0.54 |
| Variables | ILD-EOLC (n = 14) | ILD-nEOLC (n = 44) | p |
|---|---|---|---|
| Hospitalized in the last year, n | 11 (78%) | 10 (22%) | 0.0009 |
| Peripheral oxygen saturation < 88% at rest, n | 6 (42%) | 5 (11%) | 0.016 |
| Diagnosis of pulmonary hypertension, n | 1 (7%) | 8 (18%) | 0.43 |
| Lung Function | |||
| FVC, % of predicted | 52 ± 24 | 77 ± 18 | 0.002 |
| FEV1, % of predicted | 56 ± 24 | 77 ± 18 | 0.003 |
| DLCO, % of predicted | 22 ± 10 | 50 ± 13 | <0.0001 |
| TLC, % of predicted | 51 [34–70] | 74 [64–93] | 0.009 |
| FRC, % of predicted | 58 [43–95] | 64 [56–81] | 0.13 |
| IC, % of predicted | 51 [34–70] | 77 [63–93] | 0.002 |
| RV, % of predicted | 75 [54–88] | 78 [54–111] | 0.21 |
| Exercise Capacity | |||
| 6MWT, meters | 399 ± 106 | 468 ± 100 | 0.0004 |
| 6MWT, % of predicted | 64 ± 20 | 87 ± 16 | 0.0005 |
| Variables | ILD-EOLC (n = 14) | ILD-nEOLC (n = 44) | p |
|---|---|---|---|
| Physical Activity in Daily Life | |||
| Steps, n/day | 2727 ± 2243 | 5170 ± 2373 | 0.001 |
| Light activity, min/day | 194 ± 98 | 309 ± 103 | 0.001 |
| Moderate-to-vigorous physical activity, min/day | 1 [0.4–1] | 10 [3–19] | 0.0003 |
| Time standing, hours/day | 3.9 ± 1.2 | 5.3 ± 1.8 | 0.005 |
| Time sitting, hours/day | 6.8 ± 1.9 | 7.6 ± 1.7 | 0.14 |
| Time lying down, hours/day | 6.4 ± 1.6 | 4.4 ± 1.5 | 0.0004 |
| Functional performance | |||
| Timed-up-and-go usual, seconds | 11.1 [9.4–13.2] | 9.9 [9.4–11.5] | 0.19 |
| Timed-up-and-go usual,% of predicted | 80 ± 15 | 86 ± 18 | 0.10 |
| 1 min sit-to-stand test, repetitions | 20 ± 4 | 26 ± 7 | 0.01 |
| 1 min sit-to-stand test, % of predicted | 35 ± 8 | 45 ± 13 | 0.005 |
| 4-metre gait speed, m/s | 0.92 ± 0.21 | 1.05 ± 0.15 | 0.02 |
| 4-metre gait speed, % of predicted | 90 ± 20 | 105 ± 13 | 0.007 |
| Peripheral muscle strength | |||
| Deltoid, MVIC (N) | 91 [71–126] | 118 [97–167] | 0.01 |
| Pectoralis major, MVIC (N) | 78 [65–94] | 112 [71–128] | 0.02 |
| Latissimus dorsi, MVIC (N) | 52 [41–66] | 79 [58–114] | 0.008 |
| Biceps brachii, MVIC (N) | 177 [248–204] | 201 [164–243] | 0.09 |
| Triceps brachii, MVIC (N) | 107 [97–138] | 138 [110–182] | 0.008 |
| Quadriceps femoris, MVIC (N) | 237 [211–303] | 319 [261–446] | 0.005 |
| Respiratory muscle strength | |||
| Maximal inspiratory pressure, mmHg | 71 ± 23 | 85 ± 35 | 0.14 |
| Maximal inspiratory pressure, % of predicted | 80 ± 30 | 92 ± 35 | 0.13 |
| Maximal expiratory pressure, mmHg | 99 ± 19 | 97 ± 44 | 0.28 |
| Maximal expiratory pressure, % of predicted | 110 ± 36 | 104 ± 40 | 0.42 |
| Body composition | |||
| BMI, kg/m2 | 25.2 ± 4.07 | 27.9 ± 5.5 | 0.08 |
| Body fat percentage, % | 25 ± 9 | 24 ± 9 | 0.35 |
| Percentage of lean mass, % | 42 ± 10 | 49 ± 10 | 0.08 |
| Basal metabolic rate, kcal | 1335 [−1162–1519] | 1424 [1166–1677] | 0.30 |
| Health-related quality of life | |||
| SGRQ-I totals, points | 71 ± 15 | 50 ± 20 | 0.0009 |
| SGRQ-I symptoms, points | 72 ± 19 | 61 ± 35 | 0.08 |
| SGRQ-I activity, points | 84 ± 22 | 59 ± 28 | 0.001 |
| SGRQ-I impacts, points | 62 ± 15 | 44 ± 21 | 0.005 |
| Dyspnea in daily life | |||
| UCSD-SOBQ, points | 63 [41–92] | 37 [17–53] | 0.006 |
| MRC, points | 4 [3–5] | 2 [2–3] | 0.001 |
| Anxiety and depression symptoms | |||
| HADS Anxiety, points | 6 [4–8] | 5 [3–8] | 0.19 |
| HADS Depression, points | 5 [3–7] | 4 [2–8] | 0.49 |
| Sleep quality and daytime sleepiness | |||
| PSQI, points | 7 [6–8] | 8 [6–10] | 0.20 |
| ESS, points | 5 [2–10] | 6 [4–10] | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krinski, G.; Bertin, L.D.; Pimpão, H.A.; Silva, H.; Tavares, B.L.; Lunardelli, L.; Alves do Prado, G.; Pitta, F.; Camillo, C.A. Clinical Characteristics of Individuals with Interstitial Lung Diseases and Indication of End-of-Life Care. J. Clin. Med. 2023, 12, 7314. https://doi.org/10.3390/jcm12237314
Krinski G, Bertin LD, Pimpão HA, Silva H, Tavares BL, Lunardelli L, Alves do Prado G, Pitta F, Camillo CA. Clinical Characteristics of Individuals with Interstitial Lung Diseases and Indication of End-of-Life Care. Journal of Clinical Medicine. 2023; 12(23):7314. https://doi.org/10.3390/jcm12237314
Chicago/Turabian StyleKrinski, Gabriela, Larissa Dragonetti Bertin, Heloise Angélico Pimpão, Humberto Silva, Brunna Luiza Tavares, Leonardo Lunardelli, Geovana Alves do Prado, Fabio Pitta, and Carlos Augusto Camillo. 2023. "Clinical Characteristics of Individuals with Interstitial Lung Diseases and Indication of End-of-Life Care" Journal of Clinical Medicine 12, no. 23: 7314. https://doi.org/10.3390/jcm12237314
APA StyleKrinski, G., Bertin, L. D., Pimpão, H. A., Silva, H., Tavares, B. L., Lunardelli, L., Alves do Prado, G., Pitta, F., & Camillo, C. A. (2023). Clinical Characteristics of Individuals with Interstitial Lung Diseases and Indication of End-of-Life Care. Journal of Clinical Medicine, 12(23), 7314. https://doi.org/10.3390/jcm12237314