
The Effect of Iron Replacement Therapy on HbA1c Levels in Diabetic and Nondiabetic Patients: A Systematic Review and Meta-Analysis

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Selection Process
2.6. Data Collection Process
2.7. Study Risk of Bias Assessment
2.8. Statistical Analysis
3. Results
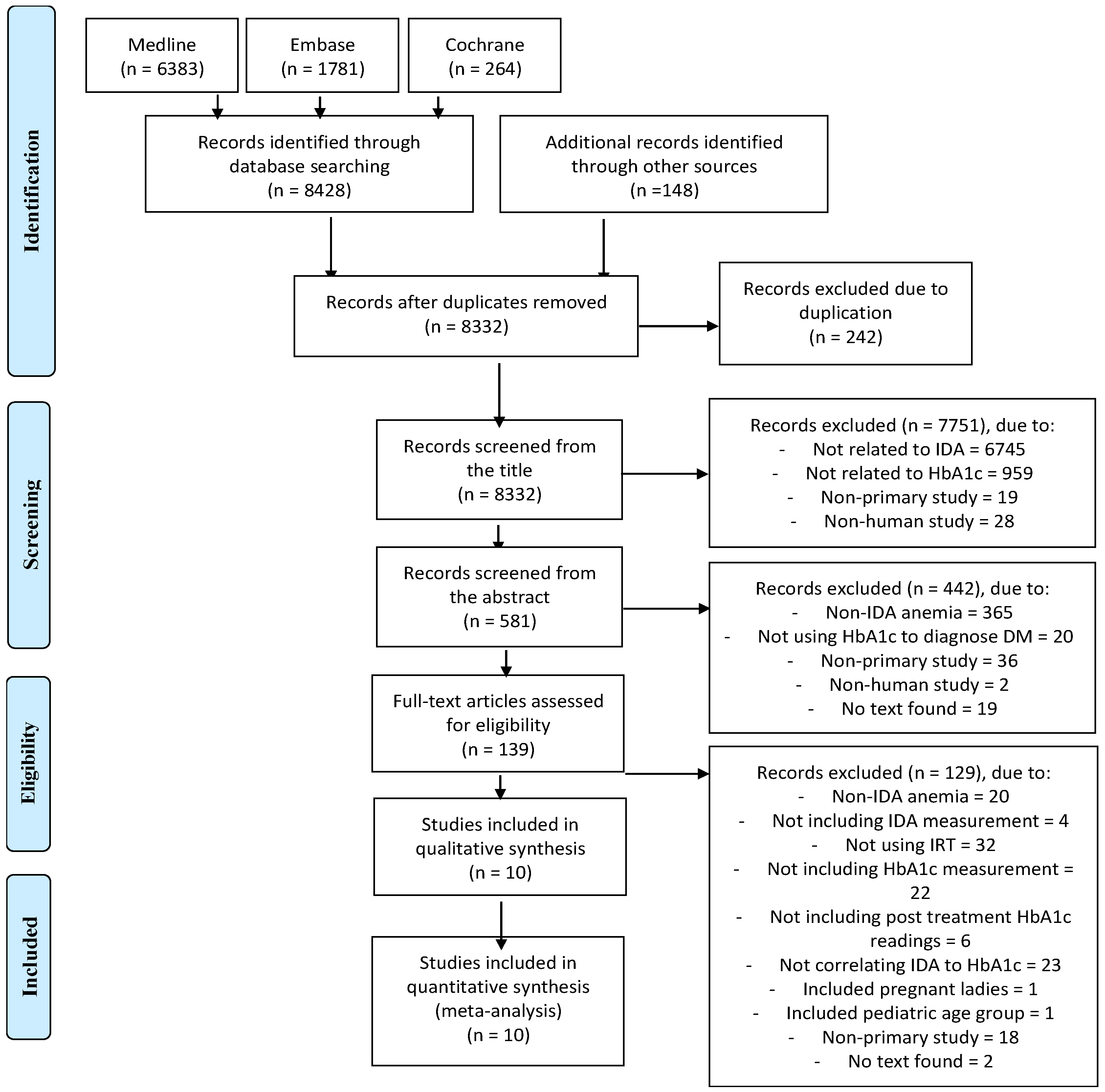
3.1. Study Selection
3.2. Bias Assessment
3.3. Study and Population Characteristics
3.4. IDA and DM Parameters before IRT
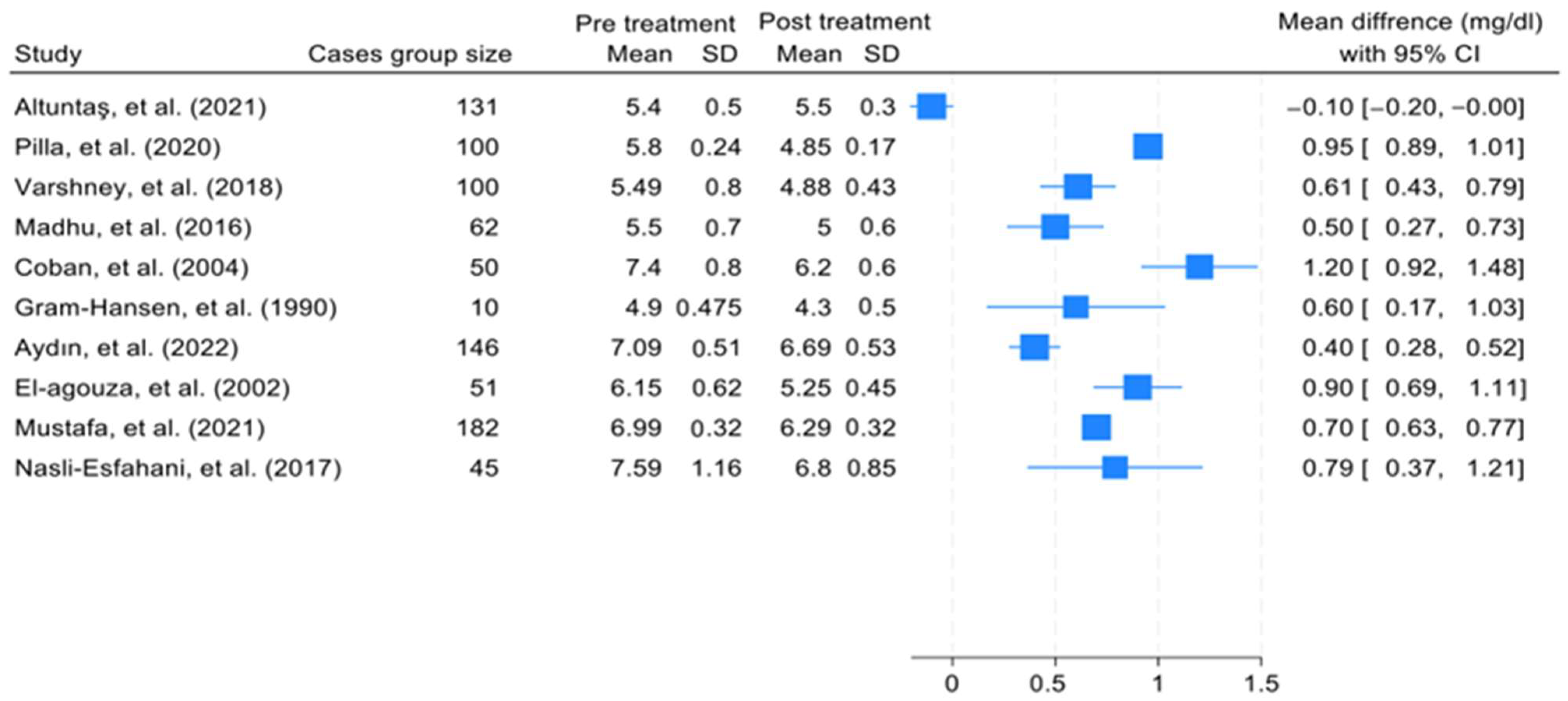
3.5. IRT and its Effect on HbA1c Levels
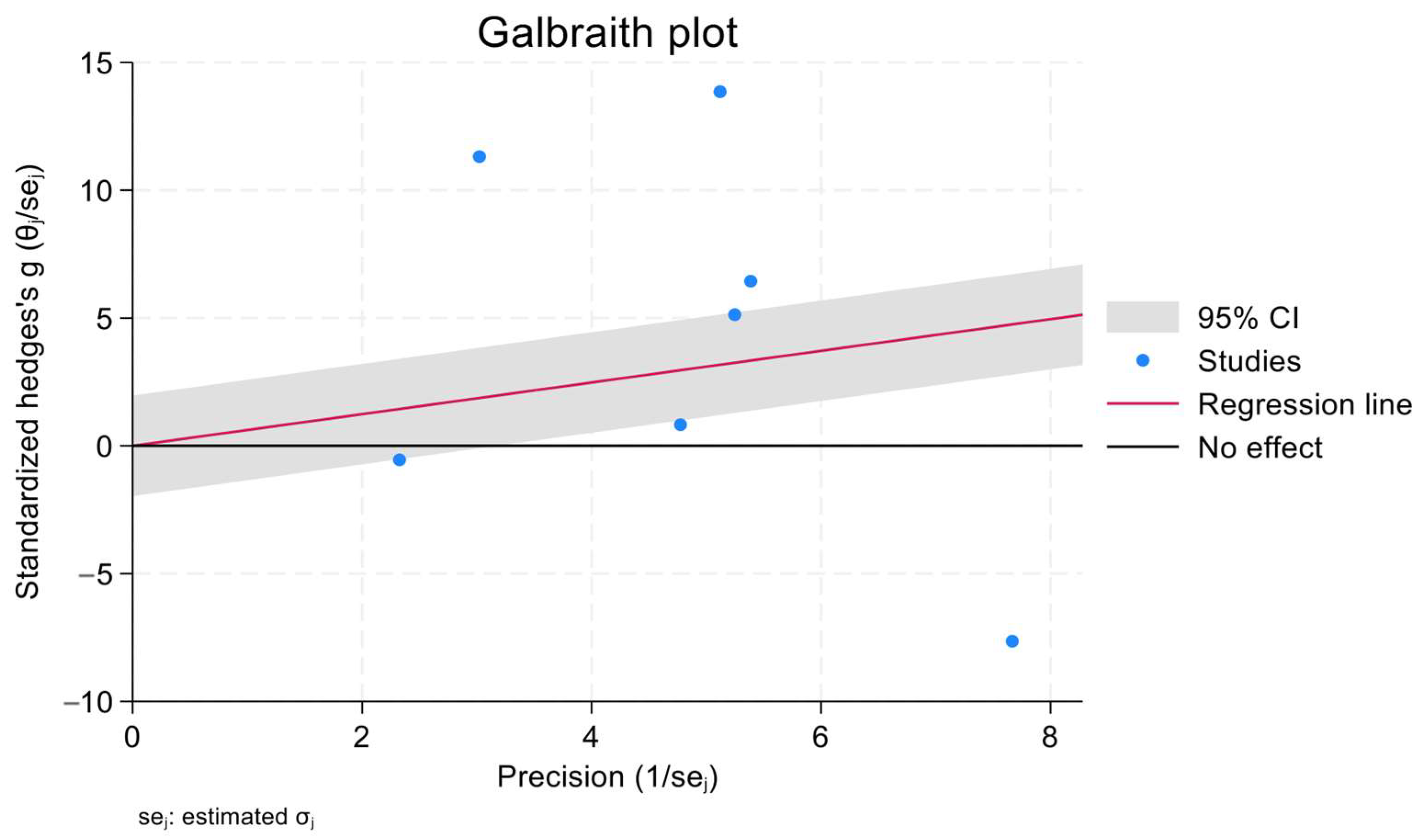
3.6. Meta-Regression Analysis
4. Discussion
4.1. IDA and HbA1c (Clinical Overview and Pathophysiology)
4.2. IRT Effect on HbA1c
5. Conclusions
- Clinicians should not rely only on HbA1c measurements when determining the treatment course for diabetic or nondiabetic patients with IDA, but rather should perform a comprehensive assessment.
- HbA1c measurements should be considered when planning a diabetic patient’s glycemic control strategy, and compliance with prescribed medications must be fully encouraged.
- It is necessary to treat IDA in diabetic patients prior to determining their daily doses of antidiabetic medications, as the presence of IDA may result in a premature elevation in the doses of these medications, which could increase the risk of drug-related complications.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andrews, N.C. The iron transporter DMT1. Int. J. Biochem. Cell Biol. 1999, 31, 991–994. [Google Scholar] [CrossRef] [PubMed]
- Adams, P.C.; Reboussin, D.M.; Barton, J.C.; McLaren, C.E.; Eckfeldt, J.H.; McLaren, G.D.; Dawkins, F.W.; Acton, R.T.; Harris, E.L.; Gordeuk, V.R.; et al. Hemochromatosis and iron-overload screening in a racially diverse population. N. Engl. J. Med. 2005, 352, 1769–1778. [Google Scholar] [CrossRef]
- Salonen, J.T.; Tuomainen, T.-P.; Nyyssönen, K.; Lakka, H.-M.; Punnonen, K. Relation between iron stores and non-insulin dependent diabetes in men: Case-control study. BMJ 1998, 317, 727–730. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. Available online: https://pubmed.ncbi.nlm.nih.gov/31082013/ (accessed on 5 August 2023).
- Abbaspour, N.; Hurrell, R.; Kelishadi, R. Review on iron and its importance for human health. J. Res. Med. Sci. 2014, 19, 164–174. [Google Scholar] [PubMed]
- Liu, J.; Li, Q.; Yang, Y.; Ma, L. Iron metabolism and type 2 diabetes mellitus: A meta-analysis and systematic review. J. Diabetes Investig. 2020, 11, 946–955. [Google Scholar] [CrossRef]
- World Health Organization. Use of Glycated Haemoglobin (HbA1c) in Diagnosis of Diabetes Mellitus. Available online: https://www.who.int/publications-detail-redirect/use-of-glycated-haemoglobin-(-hba1c)-in-diagnosis-of-diabetes-mellitus (accessed on 5 August 2023).
- Massi-Benedetti, M. Changing targets in the treatment of type 2 diabetes. Curr. Med. Res. Opin. 2006, 22, S5–S13. [Google Scholar] [CrossRef]
- The International Expert Committee. International Expert Committee Report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009, 32, 1327–1334. [Google Scholar] [CrossRef]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2010, 33, S62–S69. [Google Scholar] [CrossRef]
- Horton, B.F.; Huisman, T.H. Studies on the heterogeneity of haemoglobin. VII. Minor haemoglobin components in haematological diseases. Br. J. Haematol. 1965, 11, 296–304. [Google Scholar] [CrossRef]
- Christy, A.L.; Manjrekar, P.A.; Babu, R.P.; Hegde, A.; Rumkini, M.S. Influence of Iron Deficiency Anemia on Hemoglobin A1C Levels in Diabetic Individuals with Controlled Plasma Glucose Levels. Iran Biomed. J. 2014, 18, 88–93. [Google Scholar] [CrossRef]
- Prasad, K.; Gupte, S. Correlation of Iron Deficiency Anemia on HbA1C Levels: Comparison among Patients living with Diabetic and Non-diabetics. Int. J. Health Clin. Res. 2020, 3, 160–162. [Google Scholar]
- Chaudhari, A.S.; Sontakke, A.N.; Trimbake, S.B. HbA1c status in Type II Diabetes Mellitus with and without Iron Deficiency Anemia. Int. J. Biochem. Res. Rev. 2020, 29, 114–120. [Google Scholar] [CrossRef]
- Madhu, S.V.; Raj, A.; Gupta, S.; Giri, S.; Rusia, U. Effect of iron deficiency anemia and iron supplementation on HbA1c levels—Implications for diagnosis of Prediabetes and diabetes mellitus in Asian Indians. Clin. Chim. Acta 2017, 468, 225–229. [Google Scholar] [CrossRef]
- Urrechaga, E. Influence of iron deficiency on Hb A1C levels in type 2 diabetic patients. Diabetes Metab. Syndr. 2018, 12, 1051–1055. [Google Scholar] [CrossRef]
- Hong, J.W.; Ku, C.R.; Noh, J.H.; Ko, K.S.; Rhee, B.D.; Kim, D.-J. Association between the presence of iron deficiency anemia and hemoglobin A1C in Korean adults. Medicine 2015, 94, e825. [Google Scholar] [CrossRef]
- Sharma, A.; Kalra, H.S.; Arora, R.; Kukreja, S. Is HbA1c a reliable diagnostic marker for diabetes mellitus in patients with iron deficiency anaemia?: A Cross Sectional Study. Int. J. Clin. Biochem. Res. 2020, 7, 12–18. [Google Scholar] [CrossRef]
- Altuntaş, S.Ç.; Evran, M.; Gürkan, E.; Sert, M.; Tetiker, T. HbA1c level decreases in iron deficiency anemia. Wien Klin Wochenschr. 2021, 133, 102–106. [Google Scholar] [CrossRef]
- Puri, S.S.; Gautam, S.; Singhal, P. Correlation of iron deficiency anaemia with haemoglobin A1C at a Tertiary Care Teaching Hospital In Uttar Prades. Int. J. Health Clin. Res. 2021, 4, 234–240. [Google Scholar]
- Kalairajan, S.; K, V.D.; R, M.A. A study on influence of iron deficiency anaemia over HbA1c levels. Int. J. Adv. Med. 2019, 6, 1095–1100. [Google Scholar] [CrossRef]
- Solomon, A.; Hussein, M.; Negash, M.; Ahmed, A.; Bekele, F.; Kahase, D. Effect of iron deficiency anemia on HbA1c in diabetic patients at Tikur Anbessa Specialized Teaching Hospital, Addis Ababa Ethiopia. BMC Hematol. 2019, 19, 2. [Google Scholar] [CrossRef]
- Oğuz, E.; Ercan, M.; Yilmaz, F. Effect of Iron Deficiency Anemia on Hemoglobin A1c Levels in Normoglisemic Individuals. Ank. Med. J. 2014, 14, 15–18. [Google Scholar]
- Mitchell, T.R.; Anderson, D.; Shepperd, J. Iron deficiency, haemochromatosis, and glycosylated haemoglobin. Lancet 1980, 316, 747. [Google Scholar] [CrossRef]
- Silva, J.F.; Pimentel, A.L.; Camargo, J.L. Effect of iron deficiency anaemia on HbA1c levels is dependent on the degree of anaemia. Clin. Biochem. 2016, 49, 117–120. [Google Scholar] [CrossRef]
- Rajagopal, L.; Arunachalam, S.; Ganapathy, S.; Ramraj, B.; Raja, V. A comparison of effect of Iron Deficiency Anemia on HbA1c levels in controlled diabetics and non-diabetics: A cross sectional analysis of 300 cases. Ann. Pathol. Lab. Med. 2017, 4, 212–218. [Google Scholar] [CrossRef][Green Version]
- Bansal, R.K.; Yadav, Y.R.; Kulkarni, H.S.; Garg, S.; Jain, P.; Sharma, V.K.; Maheshwari, S. Effect of Iron Deficiency Anemia on HbA1c in Non-Diabetics. J. Diabetes Endocrinol. Assoc. Nepal 2020, 4, 10–16. [Google Scholar] [CrossRef]
- Rajagopal, L.; Ganapathy, S.; Arunachalam, S.; Raja, V.; Ramraj, B. Does Iron Deficiency Anaemia and its Severity Influence HbA1C Level in Non Diabetics? An Analysis of 150 Cases. J. Clin. Diagn. Res. 2017, 11, EC13–EC15. [Google Scholar] [CrossRef]
- Jimenez, K.; Kulnigg-Dabsch, S.; Gasche, C. Management of Iron Deficiency Anemia. Gastroenterol. Hepatol. 2015, 11, 241–250. [Google Scholar]
- Brooks, A.P.; Metcalfe, J.; Day, J.L.; Edwards, M.S. Iron deficiency and glycosylated haemoglobin A. Lancet 1980, 2, 141. [Google Scholar] [CrossRef]
- Gram-Hansen, P.; Eriksen, J.; Mourits-Andersen, T.; Olesen, L. Glycosylated haemoglobin (HbA1c) in iron- and vitamin B12 deficiency. J. Intern. Med. 1990, 227, 133–136. [Google Scholar] [CrossRef]
- Coban, E.; Ozdogan, M.; Timuragaoglu, A. Effect of iron deficiency anemia on the levels of hemoglobin A1C in nondiabetic patients. Acta Haematol. 2004, 112, 126–128. [Google Scholar] [CrossRef] [PubMed]
- El-Agouza, I.; Abu Shahla, A.; Sirdah, M. The effect of iron deficiency anaemia on the levels of haemoglobin subtypes: Possible consequences for clinical diagnosis. Clin. Lab. Haematol. 2002, 24, 285–289. [Google Scholar] [CrossRef]
- Hashimoto, K.; Noguchi, S.; Morimoto, Y.; Hamada, S.; Wasada, K.; Imai, S.; Murata, Y.; Kasayama, S.; Koga, M. A1C but Not Serum Glycated Albumin Is Elevated in Late Pregnancy Owing to Iron Deficiency. Diabetes Care 2008, 31, 1945–1948. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K.; Koga, M. Indicators of glycemic control in patients with gestational diabetes mellitus and pregnant women with diabetes mellitus. World J. Diabetes 2015, 6, 1045–1056. [Google Scholar] [CrossRef] [PubMed]
- Tarim, Ö.; Küçükerdogan, A.; Günay, Ü.; Eralp, Ö.; Ercan, İ. Effects of iron deficiency anemia on hemoglobin A1C in type 1 diabetes mellitus. Pediatr. Int. 1999, 41, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Sinha, N.; Mishra, T.K.; Singh, T.; Gupta, N. Effect of iron deficiency anemia on hemoglobin A1C levels. Ann. Lab. Med. 2012, 32, 17–22. [Google Scholar] [CrossRef]
- AlQarni, A.; Alghamdi, A.; Aljubran, H.; Bamalan, O. The Effect of Iron Deficiency Anemia on Glycated Hemoglobin A1c: A Systematic Review and Meta-Analysis, PROSPERO 2022 CRD42022312203. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022312203 (accessed on 28 September 2023).
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Pilla, R.; Palleti, S.K.; Rayala, R.; Skss, S.R.; Abdul Razzack, A.; Kalla, S. Glycated Haemoglobin (HbA1c) Variations in Nondiabetics With Nutritional Anemia. Cureus 2020, 12, e11479. [Google Scholar] [CrossRef]
- Varshney, A.K.; Singhal, S.; Gupta, P.K.; Taneja, R.S.; Chawla, M.P.S.; Tonk, R.S.; Mahto, S.K.; Sharma, L.K. Effect of Iron Supplementation on Glycosylated Haemoglobin in Non-Diabetic Individuals with Iron Deficiency Anaemia. J. Indian Acad. Clin. Med. 2018, 19, 178–182. [Google Scholar]
- Aydın, B.; Özçelik, S.; Kilit, T.P.; Eraslan, S.; Çelik, M.; Onbaşı, K. Relationship between glycosylated hemoglobin and iron deficiency anemia: A common but overlooked problem. Prim. Care Diabetes 2022, 16, 312–317. [Google Scholar] [CrossRef]
- Mustafa, R.; Uthman, M. Effect of Iron Replacement on Mean Decrease of Hba1c in Diabetic Type 2 Patients with Iron Deficiency Anemia. Pak. J. Med. Health Sci. 2021, 15, 764–766. [Google Scholar]
- Nasli-Esfahani, E.; Larijani, B.; Amini, P.; Ghodssi-Ghassemabadi, R.; Razmandeh, R. Effect of treatment of iron deficiency anemia on hemoglobin A1C in type 2 diabetic patients. Turk. J. Med. Sci. 2017, 47, 1441–1446. [Google Scholar] [CrossRef]
- Gallagher, E.J.; Roith, D.L.; Bloomgaren, Z. Review of hemoglobin A1c in the management of diabetes. J. Diabetes 2009, 1, 9–17. [Google Scholar] [CrossRef]
- Kesson, C.M.; Whitelaw, J.W.; Ireland, J.T. Drug-induced haemolysis and fast haemoglobin A1 in diabetes mellitus. Br. Med. J. 1979, 2, 1037–1038. [Google Scholar] [CrossRef][Green Version]
- Tack, C.J.; Wetzels, J.F. Decreased HbA1c levels due to sulfonamide-induced hemolysis in two IDDM patients. Diabetes Care 1996, 19, 775–776. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Robertson, M. Artificially low HbA1c associated with treatment with ribavirin. BMJ 2008, 336, 505. [Google Scholar] [CrossRef] [PubMed]
- Diop, M.-E.; Bastard, J.-P.; Meunier, N.; Thévenet, S.; Maachi, M.; Capeau, J.; Pialoux, G.; Vigouroux, C. Inappropriately low glycated hemoglobin values and hemolysis in HIV-infected patients. AIDS Res. Hum. Retroviruses 2006, 22, 1242–1247. [Google Scholar] [CrossRef]
- Yedla, N.; Kuchay, M.S.; Mithal, A. Hemoglobin E disease and glycosylated hemoglobin. Indian J. Endocrinol. Metab. 2015, 19, 683–685. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Wimbley, T.D.; Graham, D.Y. Diagnosis and management of iron deficiency anemia in the 21st century. Ther. Adv. Gastroenterol. 2011, 4, 177–184. [Google Scholar] [CrossRef]
- Kumar, A.; Sharma, E.; Marley, A.; Samaan, M.A.; Brookes, M.J. Iron deficiency anaemia: Pathophysiology, assessment, practical management. BMJ Open Gastroenterol. 2022, 9, e000759. [Google Scholar] [CrossRef]
- Little, R.R.; Sacks, D.B. HbA1c: How do we measure it and what does it mean? Curr. Opin. Endocrinol. Diabetes Obes. 2009, 16, 113–118. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/health-topics/anaemia (accessed on 1 August 2023).
- Shepard, J.G.; Airee, A.; Dake, A.W.; McFarland, M.S.; Vora, A. Limitations of A1c Interpretation. South Med. J. 2015, 108, 724–729. [Google Scholar] [CrossRef]
- Maheshwari, V.D.; Capoor, S.; Chaturvedi, S.; Manglunia, A.; Singla, A. Impact of Iron and Vitamin B12 Anaemia at Glycosylated Hemoglobin Level: A Case Control Study. IOSR J. Dent. Med. Sci. 2017, 16, 01–04. [Google Scholar] [CrossRef]
- Bry, L.; Chen, P.C.; Sacks, D.B. Effects of Hemoglobin Variants and Chemically Modified Derivatives on Assays for Glycohemoglobin. Clin. Chem. 2001, 47, 153–163. [Google Scholar] [CrossRef]
- Albright, E.S.; Ovalle, F.; Bell, D.S.H. Artificially low hemoglobin A1c caused by use of dapsone. Endocr. Pract. 2002, 8, 370–372. [Google Scholar] [CrossRef]
- Bernstein, R.M.; Freedman, D.B.; Liyanage, S.P.; Dandona, P. Glycosylated haemoglobin in rheumatoid arthritis. Ann. Rheum. Dis. 1982, 41, 604–606. [Google Scholar] [CrossRef] [PubMed]
- Weykamp, C. HbA1c: A Review of Analytical and Clinical Aspects. Ann. Lab. Med. 2013, 33, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Hellman, R. When are HBA1C Values Misleading? AACE Clin. Case Rep. 2016, 2, 377–379. [Google Scholar] [CrossRef]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 2. classification and diagnosis of diabetes: Standards of care in Diabetes-2023. Diabetes Care 2023, 46, 19–40. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Author | Country | Study Design | Sample Size: (Control; Cases) | Median Age in Years | Female (%) | |
|---|---|---|---|---|---|---|---|
| Cases | Control | ||||||
| 1 | Altuntaş, et al. (2021) [19] | Turkey | Prospective case—control study | (132; 131) | 39 ± 10 | 41 ± 9 | 89 |
| 2 | Pilla, et al. (2020) [41] | India | Prospective case—control study | (100; 100) | 38 | 40 | - |
| 3 | Varshney, et al. (2018) [42] | India | Prospective case—control study | (50; 100) | 32.14 ± 3.11 | 35.60 ± 4.57 | 54 |
| 4 | Madhu, et al. (2016) [15] | India | Prospective case—control study | (60; 62) | 31.4 ± 11.3 | 32.5 ± 10.1 | Case = 87.1 Control = 85 |
| 5 | Coban, et al. (2004) [32] | Turkey | Prospective case—control study | (50; 50) | 35.7 ± 11.9 | 60 | |
| 6 | Gram-Hansen, et al. (1990) [31] | Denmark | Prospective case—control study | (10; 10) | 52 ± 13.5 | 60 ± 5.5 | - |
| 7 | Aydın, et al. (2022) [43] | Turkey | Prospective cohort study | (0; 146) | 45 ± 2.5 | 82.1 | |
| 8 | El-agouza, et al. (2002) [33] | Egypt | Prospective cohort study | (0; 51) | University school age | - | |
| 9 | Mustafa, et al. (2021) [44] | Pakistan | Quasi-experimental trial | (0; 182) | 54.84 ± 8.69 | 45 | |
| 10 | Nasli-Esfahani, et al. (2017) [45] | Iran | Randomized clinical trial | (45; 45) | 51.47 ± 7.07 | 52 ± 7.35 | 70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlQarni, A.M.; Alghamdi, A.A.; Aljubran, H.J.; Bamalan, O.A.; Abuzaid, A.H.; AlYahya, M.A. The Effect of Iron Replacement Therapy on HbA1c Levels in Diabetic and Nondiabetic Patients: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 7287. https://doi.org/10.3390/jcm12237287
AlQarni AM, Alghamdi AA, Aljubran HJ, Bamalan OA, Abuzaid AH, AlYahya MA. The Effect of Iron Replacement Therapy on HbA1c Levels in Diabetic and Nondiabetic Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(23):7287. https://doi.org/10.3390/jcm12237287
Chicago/Turabian StyleAlQarni, Amani M., Amal A. Alghamdi, Hussain J. Aljubran, Omar A. Bamalan, Abdullah H. Abuzaid, and Mohammed A. AlYahya. 2023. "The Effect of Iron Replacement Therapy on HbA1c Levels in Diabetic and Nondiabetic Patients: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 23: 7287. https://doi.org/10.3390/jcm12237287
APA StyleAlQarni, A. M., Alghamdi, A. A., Aljubran, H. J., Bamalan, O. A., Abuzaid, A. H., & AlYahya, M. A. (2023). The Effect of Iron Replacement Therapy on HbA1c Levels in Diabetic and Nondiabetic Patients: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(23), 7287. https://doi.org/10.3390/jcm12237287