
Anomalous Origin of Left Circumflex Artery from the Right Sinus of Valsalva in Cardiac Computed Tomography in a Group of 16,680 Patients—Radiologic and Clinical Characteristics

Abstract
:1. Introduction
2. Methods
3. Results
3.1. Clinical
3.2. Radiologic
3.3. Echocardiographic
4. Discussion
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Basso, C.; Maron, B.J.; Corrado, D.; Thiene, G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J. Am. Coll. Cardiol. 2000, 35, 1493–1501. [Google Scholar] [CrossRef] [PubMed]
- Knuuti, J.; Wijns, W.; Saraste, A.; Capodanno, D.; Barbato, E.; Funck-Brentano, C.; Prescott, E.; Storey, R.F.; Deaton, C.; Cuisset, T.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagno-sis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Newby, L.K.; Arnold, S.V.; Bittner, V.; Brewer, L.C.; Demeter, S.H.; Dixon, D.L.; Fearon, W.F.; Hess, B.; Johnson, H.M.; et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients with Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2023, 148, e9–e119. [Google Scholar] [CrossRef] [PubMed]
- Andreini, D.; Mushtaq, S.; Pontone, G.; Cortinovis, S.; Annoni, A.; Formenti, A.; Agostoni, P.; Bartorelli, A.L.; Fiorentini, C.; Ballerini, G.; et al. Additional clinical role of 64-slice multidetector computed tomography in the evaluation of coronary artery variants and anomalies. Int. J. Cardiol. 2010, 145, 388–390. [Google Scholar] [CrossRef] [PubMed]
- Ghadri, J.R.; Kazakauskaite, E.; Braunschweig, S.; Burger, I.A.; Frank, M.; Fiechter, M.; Gebhard, C.; Fuchs, T.A.; Templin, C.; Gaemperli, O.; et al. Congenital coronary anomalies detected by coronary computed tomography compared to invasive coronary angiography. BMC Cardiovasc. Disord. 2014, 14, 81. [Google Scholar] [CrossRef] [PubMed]
- Eckart, R.E.; Scoville, S.L.; Campbell, C.L.; Shry, E.A.; Stajduhar, K.C.; Potter, R.N.; Pearse, L.A.; Virmani, R. Sudden death in young adults: A 25-year review of autopsies in military recruits. Ann. Intern. Med. 2004, 141, 829–834. [Google Scholar] [CrossRef]
- Krupiński, M.; Urbańczyk-Zawadzka, M.; Laskowicz, B.; Irzyk, M.; Banyś, R.; Klimeczek, P.; Gruszczyńska, K.; Baron, J. Anomalous origin of the coronary artery from the wrong coronary sinus evaluated with computed tomography: “high-risk” anatomy and its clinical relevance. Eur. Radiol. 2014, 24, 2353–2359. [Google Scholar] [CrossRef]
- Opolski, M.P.; Pregowski, J.; Kruk, M.; Witkowski, A.; Kwiecinska, S.; Lubienska, E.; Demkow, M.; Hryniewiecki, T.; Michalek, P.; Ruzyllo, W.; et al. Prevalence and characteristics of coronary anomalies originating from the opposite sinus of Valsalva in 8522 patients referred for coronary computed tomography angiography. Am. J. Cardiol. 2013, 111, 1361–1367. [Google Scholar] [CrossRef]
- Antopol, W.; Kugel, M. Anomalous origin of the left circumflex coronary artery. Am. Heart J. 1933, 8, 802–806. [Google Scholar] [CrossRef]
- Molossi, S.; Agrawal, H.; Mery, C.M.; Krishnamurthy, R.; Masand, P.; Tejtel, S.K.S.; Noel, C.V.; Qureshi, A.M.; Jadhav, S.P.; McKenzie, E.D.; et al. Outcomes in Anomalous Aortic Origin of a Coronary Artery Following a Prospective Standardized Approach. Circ. Cardiovasc. Interv. 2020, 13, e008445. [Google Scholar] [CrossRef]
- Rissam, H.K.; Garg, L.; Mittal, U.K.; Singh, S. Uncommon variants of left circumflex coronary artery (LCX): Evaluation with 256-slice dual source CT coronary angiography. BMJ Case Rep. 2015, 2015. [Google Scholar] [CrossRef]
- Page, H.L.; Engel, H.J.; Campbell, W.B.; Thomasjr, C.S. Anomalous Origin of the Left Circumflex Coronary Artery. Circulation 1974, 50, 768–773. [Google Scholar] [CrossRef]
- Mohsen, G.; Klein, A.J.; Miller, E.; Forsberg, M.; Taniuchi, M. Anomalous left circumflex artery from the right coronary cusp: A benign variant? J. Invasive Cardiol. 2011, 12, e14. [Google Scholar] [CrossRef]
- Bonapace, S.; Lanzoni, L.; Rossi, A.; Cicciò, C.; Cicoira, M.; Dugo, C.; Maffeis, C.; Valbusa, F.; Canali, G.; Guerriero, M.; et al. Sensitivity and Specificity of Transthoracic Echocardiography in Diagnosing the Presence of the Anomalous Origin of Left Circumflex Coronary Artery from the Right Sinus of Valsalva in an Adult Population. J. Am. Heart Assoc. 2023, 12, e030173. [Google Scholar] [CrossRef] [PubMed]
- Witt, C.M.; Elvert, L.A.; Konik, E.A.; Ammash, N.M.; Foley, D.A.; Foley, T.A. The RAC Sign: Retroaortic Anomalous Coronary Artery Visualization by Transthoracic Echocardiography. JACC Cardiovasc. Imaging 2018, 11, 648–649. [Google Scholar] [CrossRef]
- Bianco, F.; Colaneri, M.; Bucciarelli, V.; Surace, F.C.; Iezzi, F.V.; Primavera, M.; Biasi, A.; Giusti, G.; Berton, E.; Baldoni, M.; et al. Echocardiographic screening for the anomalous aortic origin of coronary arteries Congenital heart disease. Heart 2021, 8, e001495. [Google Scholar] [CrossRef]
- Kornej, J.; Henger, S.; Seewöster, T.; Teren, A.; Burkhardt, R.; Thiele, H.; Thiery, J.; Scholz, M. Prevalence of atrial fibrillation dependent on coronary artery status: Insights from the LIFE-Heart Study. Clin. Cardiol. 2020, 43, 1616–1623. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.C.; Hobbs, F.R.; Kenkre, J.E.; Roalfe, A.K.; Iles, R.; Lip, G.Y.; Davies, M.K. Prevalence of atrial fibrillation in the general population and in high-risk groups: The ECHOES study. EP Eurospace 2012, 14, 1553–1559. [Google Scholar] [CrossRef]
- Kalarus, Z.; Średniawa, B.; Mitręga, K.; Wierucki, Ł.; Sokal, A.; Lip, G.; Bandosz, P.; Stokwiszewski, J.; Boidol, J.; Zieleniewicz, P.; et al. Prevalence of atrial fibrillation in the 65 or over Polish population. Report of cross-sectional NOMED-AF study. Kardiol. Pol. 2023, 81, 14–21. [Google Scholar] [CrossRef]
- Ratti, A.; Prestini, B.; Conte, E.; Marchetti, D.; Schillaci, M.; Melotti, E.; Belmonte, M.; Mushtaq, S.; Dessani, M.A.; Pizzamiglio, F.; et al. Anomalous origin of left circumflex artery from the right sinus of Valsalva: Clinical outcomes in a consecutive series of master athletes. Clin. Cardiol. 2023, 46, 1097–1105. [Google Scholar] [CrossRef]
- Bartoli, C.R.; Wead, W.B.; Giridharan, G.A.; Prabhu, S.D.; Koenig, S.C.; Dowling, R.D. Mechanism of myocardial ischemia with an anomalous left coronary artery from the right sinus of Valsalva. J. Thorac. Cardiovasc. Surg. 2012, 144, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Rozenman, Y.; Schechter, D.; Gilon, D.; Gotsman, M.S. Anomalous origin of the circumflex coronary artery from the right sinus of valsalva as a cause of ischemia at old age. Clin. Cardiol. 1993, 16, 900–901. [Google Scholar] [CrossRef] [PubMed]
- Del Torto, A.; Baggiano, A.; Guglielmo, M.; Muscogiuri, G.; Pontone, G. Anomalous origin of the left circumflex artery from the right coronary sinus with retro-aortic course: A potential malign variant. J. Cardiovasc. Comput. Tomogr. 2020, 14, e54–e55. [Google Scholar] [CrossRef] [PubMed]
- Mahowald, J.M.; Mlieden, L.C.; Coe, J.I.; Edwards, J.E. Ectopic origin of a coronary artery from the aorta. Sudden death in 3 of 23 patients. Chest 1986, 89, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Samarendra, P.; Kumari, S.; Hafeez, M.; Vasavada, B.C.; Sacchi, T.J. Anomalous circumflex coronary artery: Benign or predisposed to selective atherosclerosis. Angiology 2001, 52, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Mohsen, G.A.; Mohsin, K.G.; Forsberg, M.; Miller, E.; Taniuchi, M.; Klein, A.J. Anomalous left circumflex artery from the right coronary cusp: A benign variant. J. Invasive Cardiol. 2013, 25, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Corrado, D.; Pennelli, T.; Piovesana, P.; Thiene, G. Anomalous origin of the left circumflex coronary artery from the right aortic sinus of valsalva and sudden death. Cardiovasc. Pathol. 1994, 3, 269–271. [Google Scholar] [CrossRef]
- Singh, J.P.; Evans, J.C.; Levy, D.; Larson, M.G.; A Freed, L.; Fuller, D.L.; Lehman, B.; Benjamin, E.J. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (The Framingham Heart Study). Am. J. Cardiol. 1999, 83, 897–902. [Google Scholar] [CrossRef]
- Pastore, M.C.; Mandoli, G.E.; Contorni, F.; Cavigli, L.; Focardi, M.; D’ascenzi, F.; Patti, G.; Mondillo, S.; Cameli, M. Speckle Tracking Echocardiography: Early Predictor of Diagnosis and Prognosis in Coronary Artery Disease. BioMed Res. Int. 2021, 2021, 6685378. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 56 | 100% |
|---|---|---|
| Male | 30 | 54 |
| Female | 26 | 46 |
| Heart failure | 8 | 14 |
| CAD | 13 | 23 |
| AF | 7 | 13 |
| DM t. 2 | 7 | 13 |
| Obesity | 6 | 11 |
| Dyslipidemia | 17 | 30 |
| Smoking | 5 | 9 |
| Type | Diagram | CT Image |
|---|---|---|
| Normal | 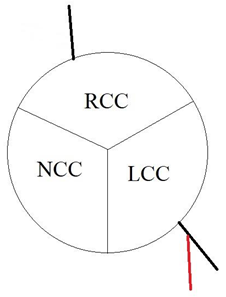 | 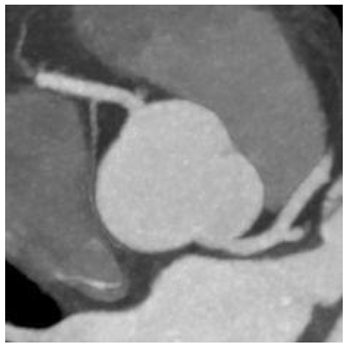 |
| I | 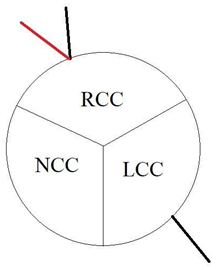 |  |
| II |  |  |
| III | 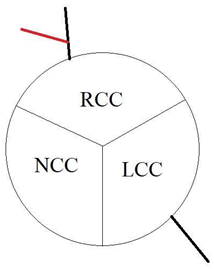 | 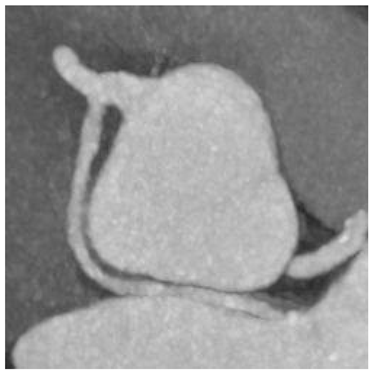 |
| Radiologic Feature | Types | Number of Patients | % |
|---|---|---|---|
| Origin | I | 27 | 48 |
| II | 14 | 25 | |
| III | 15 | 27 | |
| Course | Between aorta and pulmonary trunk “malignant” | 0 | 0 |
| Between aorta and left atrium “benign” | 56 | 100 | |
| Ostia | Round (normal) | 42 | 75 |
| Oval | 14 | 25 | |
| Slit | 0 | 0 | |
| Angle | ≤45 | 39 | 70 |
| >45 | 17 | 30 | |
| Intramural course | 29 | 52 |
| Echocardiographic Feature | Number of Patients | % |
|---|---|---|
| Enlarged LA | 11 | 30 |
| MR | 14 | 38 |
| MS | 0 | 0 |
| AR | 3 | 8 |
| AS | 3 | 8 |
| TR | 8 | 22 |
| TS | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suchodolski, A.; Głowacki, J.; Szulik, M. Anomalous Origin of Left Circumflex Artery from the Right Sinus of Valsalva in Cardiac Computed Tomography in a Group of 16,680 Patients—Radiologic and Clinical Characteristics. J. Clin. Med. 2023, 12, 7240. https://doi.org/10.3390/jcm12237240
Suchodolski A, Głowacki J, Szulik M. Anomalous Origin of Left Circumflex Artery from the Right Sinus of Valsalva in Cardiac Computed Tomography in a Group of 16,680 Patients—Radiologic and Clinical Characteristics. Journal of Clinical Medicine. 2023; 12(23):7240. https://doi.org/10.3390/jcm12237240
Chicago/Turabian StyleSuchodolski, Alexander, Jan Głowacki, and Mariola Szulik. 2023. "Anomalous Origin of Left Circumflex Artery from the Right Sinus of Valsalva in Cardiac Computed Tomography in a Group of 16,680 Patients—Radiologic and Clinical Characteristics" Journal of Clinical Medicine 12, no. 23: 7240. https://doi.org/10.3390/jcm12237240
APA StyleSuchodolski, A., Głowacki, J., & Szulik, M. (2023). Anomalous Origin of Left Circumflex Artery from the Right Sinus of Valsalva in Cardiac Computed Tomography in a Group of 16,680 Patients—Radiologic and Clinical Characteristics. Journal of Clinical Medicine, 12(23), 7240. https://doi.org/10.3390/jcm12237240