
Polypill Therapy for Cardiovascular Disease Prevention and Combination Medication Therapy for Hypertension Management


Abstract
1. Introduction
2. Polypill Strategies for the Cardiovascular Disease Prevention
2.1. Polypill Therapy for Secondary Prevention of Cardiovascular Disease
2.2. Polypill Therapy and Medication Adherence
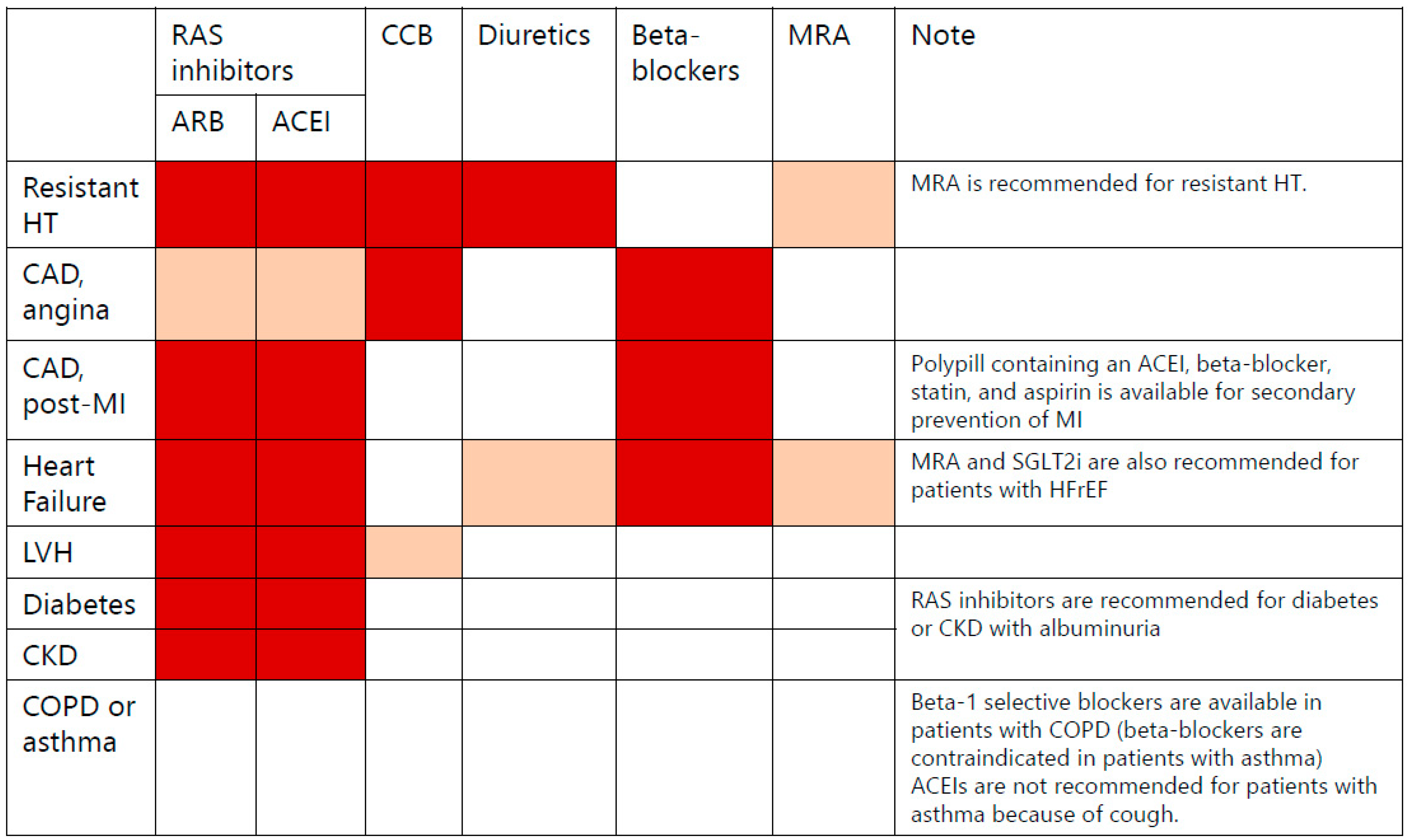
3. Combination Therapy of Antihypertensive Medications in the Management of Hypertension
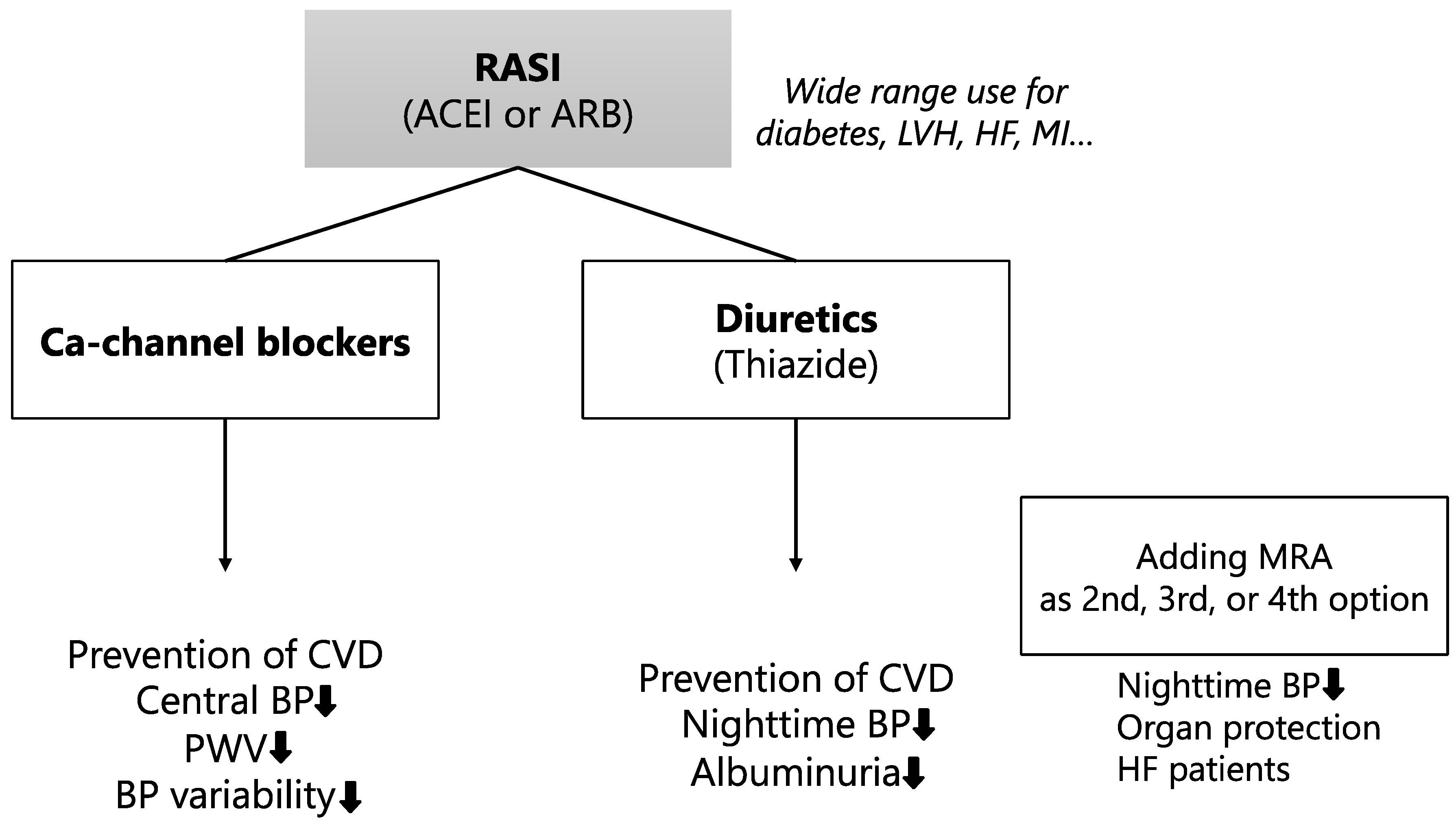
4. Combination Therapy of Renin-Angiotensin System (RAS) Inhibitors and Ca-Channel Blockers or Thiazide Diuretics
5. Novel Medications with Diverse Effects
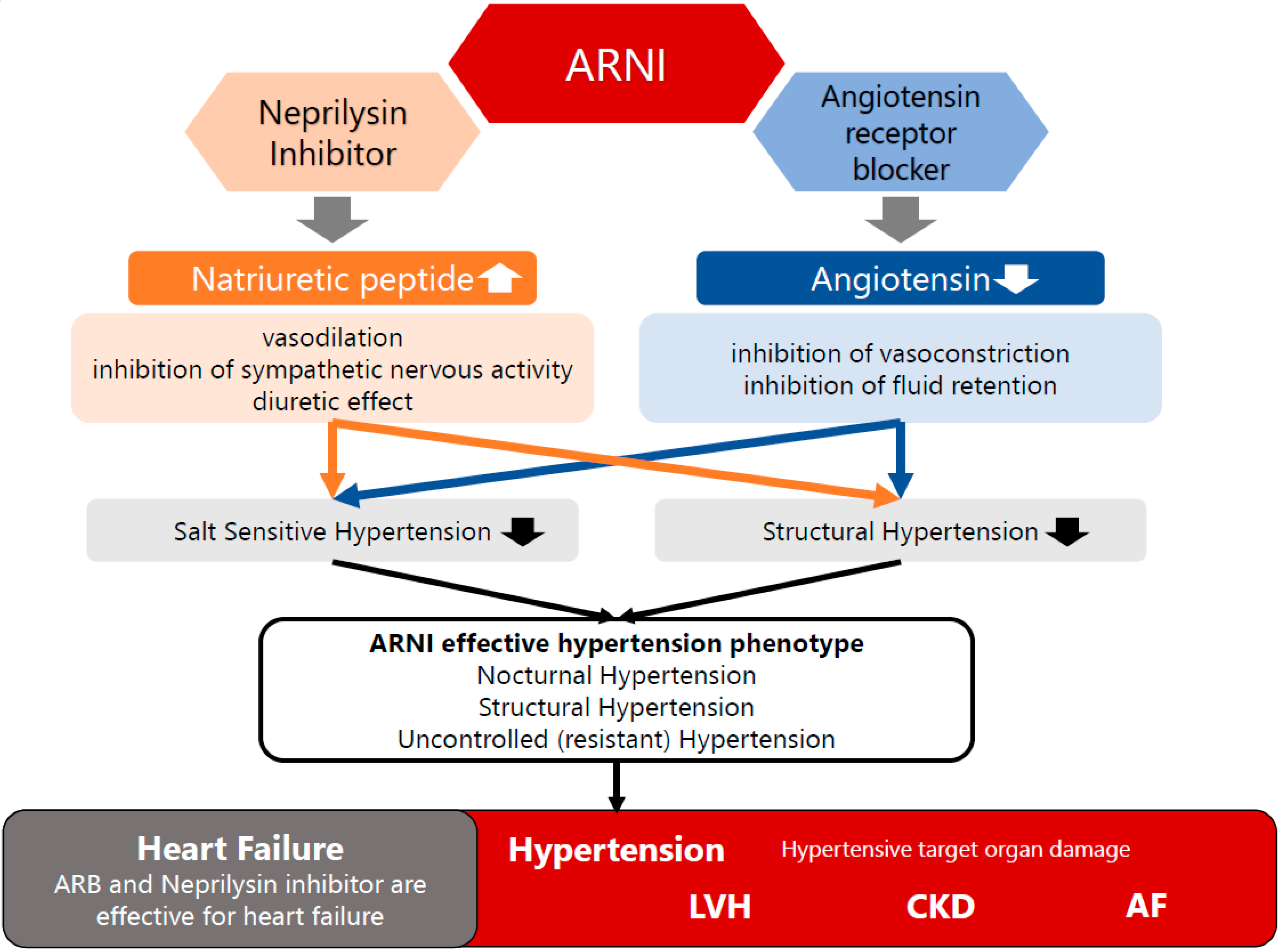
5.1. Angiotensin Receptor Neprilysin Inhibitors (ARNI)
5.2. Sodium Glucose Cotransporter 2 Inhibitor (SGLT2i)
6. Problems and Limitations of Polypill Therapy
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lauder, L.; Mahfoud, F.; Azizi, M.; Bhatt, D.L.; Ewen, S.; Kario, K.; Parati, G.; Rossignol, P.; Schlaich, M.P.; Teo, K.K.; et al. Hypertension management in patients with cardiovascular comorbidities. Eur. Heart J. 2023, 44, 2066–2077. [Google Scholar] [CrossRef]
- Umemura, S.; Arima, H.; Arima, S.; Asayama, K.; Dohi, Y.; Hirooka, Y.; Horio, T.; Hoshide, S.; Ikeda, S.; Ishimitsu, T.; et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens. Res. 2019, 42, 1235–1481. [Google Scholar] [CrossRef]
- Sukonthasarn, A.; Chia, Y.C.; Wang, J.; Nailes, J.G.; Buranakitjaroen, P.; Van Minh, H.; Verma, N.; Hoshide, S.; Shin, J.; Turana, Y.; et al. The feasibility of polypill for cardiovascular disease prevention in Asian Population. J. Clin. Hypertens. 2021, 23, 545–555. [Google Scholar] [CrossRef]
- Kario, K.; Kai, H.; Nanto, S.; Yokoi, H. Anti-hypertensive medication adherence in the REQUIRE trial: Post-hoc exploratory evaluation. Hypertens. Res. 2023, 46, 2044–2047. [Google Scholar] [CrossRef]
- Wald, N.J.; Law, M.R. A strategy to reduce cardiovascular disease by more than 80%. BMJ 2003, 326, 1419. [Google Scholar] [CrossRef]
- Castellano, J.M.; Sanz, G.; Fuster, V. Evolution of the Polypill Concept and Ongoing Clinical Trials. Can. J. Cardiol. 2014, 30, 520–526. [Google Scholar] [CrossRef]
- Zamorano, J.; Erdine, S.; Pavia, A.; Kim, J.-H.; Al-Khadra, A.; Westergaard, M.; Sutradhar, S.; Yunis, C. Proactive multiple cardiovascular risk factor management compared with usual care in patients with hypertension and additional risk factors: The CRUCIAL trial. Curr. Med Res. Opin. 2011, 27, 821–833. [Google Scholar] [CrossRef]
- Huffman, M.D.; Xavier, D.; Perel, P. Uses of polypills for cardiovascular disease and evidence to date. Lancet 2017, 389, 1055–1065. [Google Scholar] [CrossRef]
- Roshandel, G.; Khoshnia, M.; Poustchi, H.; Hemming, K.; Kamangar, F.; Gharavi, A.; Ostovaneh, M.R.; Nateghi, A.; Majed, M.; Navabakhsh, B.; et al. Effectiveness of polypill for primary and secondary prevention of cardiovascular diseases (PolyIran): A pragmatic, cluster-randomised trial. Lancet 2019, 394, 672–683. [Google Scholar] [CrossRef]
- Castellano, J.M.; Pocock, S.J.; Bhatt, D.L.; Quesada, A.J.; Owen, R.; Fernandez-Ortiz, A.; Sanchez, P.L.; Marin Ortuño, F.; Vazquez Rodriguez, J.M.; Domingo-Fernández, A.; et al. Polypill Strategy in Secondary Cardiovascular Prevention. N. Engl. J. Med. 2022, 387, 967–977. [Google Scholar] [CrossRef]
- Selak, V.; Webster, R.; Stepien, S.; Bullen, C.; Patel, A.; Thom, S.; Arroll, B.; Bots, M.L.; Brown, A.; Crengle, S.; et al. Reaching cardiovascular prevention guideline targets with a polypill-based approach: A meta-analysis of randomised clinical trials. Heart 2019, 105, 42–48. [Google Scholar] [CrossRef]
- Wang, N.; Huffman, M.D.; Sundström, J.; Rodgers, A. Halving cardiovascular risk with combined blood pressure and cholesterol lowering – Why are we not there yet? Int. J. Cardiol. 2021, 341, 96–99. [Google Scholar] [CrossRef]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2018, 73, 3168–3209. [Google Scholar] [CrossRef]
- Merat, S.; Jafari, E.; Radmard, A.R.; Khoshnia, M.; Sharafkhah, M.; Baygi, A.N.; Marshall, T.; Khuzani, A.S.; Cheng, K.K.; Poustchi, H.; et al. Polypill for prevention of cardiovascular diseases with focus on non-alcoholic steatohepatitis: The PolyIran-Liver trial. Eur. Heart J. 2022, 43, 2023–2033. [Google Scholar] [CrossRef]
- Yusuf, S.; Joseph, P.; Dans, A.; Gao, P.; Teo, K.; Xavier, D.; López-Jaramillo, P.; Yusoff, K.; Santoso, A.; Gamra, H.; et al. Polypill with or without Aspirin in Persons without Cardiovascular Disease. N. Engl. J. Med. 2021, 384, 216–228. [Google Scholar] [CrossRef]
- Joseph, P.; Roshandel, G.; Gao, P.; Pais, P.; Lonn, E.; Xavier, D.; Avezum, A.; Zhu, J.; Liu, L.; Sliwa, K.; et al. Fixed-dose combination therapies with and without aspirin for primary prevention of cardiovascular disease: An individual participant data meta-analysis. Lancet 2021, 398, 1133–1146. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2017, 39, 119–177. [Google Scholar] [CrossRef]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: The Task Force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 42, 1289–1367. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Chow, C.K.; Atkins, E.R.; Hillis, G.S.; Nelson, M.R.; Reid, C.M.; Schlaich, M.P.; Hay, P.; Rogers, K.; Billot, L.; Burke, M.; et al. Initial treatment with a single pill containing quadruple combination of quarter doses of blood pressure medicines versus standard dose monotherapy in patients with hypertension (QUARTET): A phase 3, randomised, double-blind, active-controlled trial. Lancet 2021, 398, 1043–1052. [Google Scholar] [CrossRef]
- Birla, S.; Angural, A.; Madathumchalil, A.; Shende, R.V.; Shastry, S.V.; Mahadevappa, M.; Shambhu, S.K.; Vishwanath, P.; Prashant, A. Redefining the polypill: Pros and cons in cardiovascular precision medicine. Front. Pharmacol. 2023, 14, 1268119. [Google Scholar] [CrossRef]
- Thom, S.; Poulter, N.; Field, J.; Patel, A.; Prabhakaran, D.; Stanton, A.; Grobbee, D.E.; Bots, M.L.; Reddy, K.S.; Cidambi, R.; et al. Effects of a Fixed-Dose Combination Strategy on Adherence and Risk Factors in Patients with or at High Risk of CVD: The UMPIRE Randomized Clinical Trial. JAMA 2013, 310, 918–929. [Google Scholar] [CrossRef]
- Selak, V.; Elley, C.R.; Bullen, C.; Crengle, S.; Wadham, A.; Rafter, N.; Parag, V.; Harwood, M.; Doughty, R.N.; Arroll, B.; et al. Effect of fixed dose combination treatment on adherence and risk factor control among patients at high risk of cardiovascular disease: Randomised controlled trial in primary care. BMJ 2014, 348, g3318. [Google Scholar] [CrossRef]
- Castellano, J.M.; Sanz, G.; Peñalvo, J.L.; Bansilal, S.; Fernández-Ortiz, A.; Alvarez, L.; Guzmán, L.; Linares, J.C.; García, F.; D’aniello, F.; et al. A Polypill Strategy to Improve Adherence: Results from the FOCUS project. J. Am. Coll. Cardiol. 2014, 64, 2071–2082. [Google Scholar] [CrossRef]
- Fuster, V.; Gambús, F.; Patriciello, A.; Hamrin, M.; Grobbee, D.E. The polypill approach – An innovative strategy to improve cardiovascular health in Europe. BMC Pharmacol. Toxicol. 2017, 18, 10. [Google Scholar] [CrossRef]
- Castellano, J.M.; Sanz, G.; Ortiz, A.F.; Garrido, E.; Bansilal, S.; Fuster, V. A Polypill Strategy to Improve Global Secondary Cardiovascular Prevention: From concept to reality. J. Am. Coll. Cardiol. 2014, 64, 613–621. [Google Scholar] [CrossRef]
- Webster, R.; Patel, A.; Selak, V.; Billot, L.; Bots, M.L.; Brown, A.; Bullen, C.; Cass, A.; Crengle, S.; Elley, C.R.; et al. Effectiveness of fixed dose combination medication (‘polypills’) compared with usual care in patients with cardiovascular disease or at high risk: A prospective, individual patient data meta-analysis of 3140 patients in six countries. Int. J. Cardiol. 2016, 205, 147–156. [Google Scholar] [CrossRef]
- Liu, H.; Massi, L.; Laba, T.-L.; Peiris, D.; Usherwood, T.; Patel, A.; Cass, A.; Eades, A.-M.; Redfern, J.; Hayman, N.; et al. Patients’ and Providers’ Perspectives of a Polypill Strategy to Improve Cardiovascular Prevention in Australian Primary Health Care: A qualitative study set within a pragmatic randomized, controlled trial. Circ. Cardiovasc. Qual. Outcomes 2015, 8, 301–308. [Google Scholar] [CrossRef]
- Patel, A.; Cass, A.; Peiris, D.; Usherwood, T.; Brown, A.; Jan, S.; Neal, B.; Hillis, G.S.; Rafter, N.; Tonkin, A.; et al. A pragmatic randomized trial of a polypill-based strategy to improve use of indicated preventive treatments in people at high cardiovascular disease risk. Eur. J. Prev. Cardiol. 2015, 22, 920–930. [Google Scholar] [CrossRef]
- López-Jaramillo, P.; González-Gómez, S.; Zarate-Bernal, D.; Serrano, A.; Atuesta, L.; Clausen, C.; Castro-Valencia, C.; Camacho-Lopez, P.; Otero, J. Polypill: An affordable strategy for cardiovascular disease prevention in low–medium-income countries. Ther. Adv. Cardiovasc. Dis. 2018, 12, 169–174. [Google Scholar] [CrossRef]
- Muñoz, D.; Uzoije, P.; Reynolds, C.; Miller, R.; Walkley, D.; Pappalardo, S.; Tousey, P.; Munro, H.; Gonzales, H.; Song, W.; et al. Polypill for Cardiovascular Disease Prevention in an Underserved Population. N. Engl. J. Med. 2019, 381, 1114–1123. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Himmelfarb, C.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, e13–e115. [Google Scholar] [CrossRef]
- Mancia Chairperson, G.; Kreutz Co-Chair, R.; Brunström, M.; Burnier, M.; Grassi, G.; Januszewicz, A.; Muiesan, M.L.; Tsioufis, K.; Agabiti-Rosei, E.; Algharably, E.A.E.; et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH). J. Hypertens. 2023, 41, 1874–2071. [Google Scholar] [CrossRef]
- World Health Organization. WHO Guideline for the Pharmacological Treatment of Hypertension in Adults. June 14, 2022. Available online: https://iris.who.int/bitstream/handle/10665/344424/9789240033986-eng.pdf?sequence=9789240033981 (accessed on 30 September 2023).
- Lonn, E.M.; Bosch, J.; López-Jaramillo, P.; Zhu, J.; Liu, L.; Pais, P.; Diaz, R.; Xavier, D.; Sliwa, K.; Dans, A.; et al. Blood-Pressure Lowering in Intermediate-Risk Persons without Cardiovascular Disease. N. Engl. J. Med. 2016, 374, 2009–2020. [Google Scholar] [CrossRef]
- Patel, A.; MacMahon, S.; Chalmers, J.; Neal, B.; Woodward, M.; Billot, L.; Harrap, S.; Poulter, N.; Marre, M.; Cooper, M.; et al. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): A randomised controlled trial. Lancet 2007, 370, 829–840. [Google Scholar] [CrossRef]
- Staessen, J.A.; Fagard, R.; Thijs, L.; Celis, H.; Arabidze, G.G.; Birkenhäger, W.H.; Bulpitt, C.J.; de Leeuw, P.W.; Dollery, C.T.; Fletcher, A.E.; et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997, 350, 757–764. [Google Scholar] [CrossRef]
- Wang, J.-G.; Staessen, J.A.; Gong, L.; Liu, L. Chinese Trial on Isolated Systolic Hypertension in the Elderly. Systolic Hypertension in China (Syst-China) Collaborative Group. Arch. Intern. Med. 2000, 160, 211–220. [Google Scholar] [CrossRef]
- Ogawa, H.; Kim-Mitsuyama, S.; Matsui, K.; Jinnouchi, T.; Jinnouchi, H.; Arakawa, K. Angiotensin II Receptor Blocker-based Therapy in Japanese Elderly, High-risk, Hypertensive Patients. Am. J. Med. 2012, 125, 981–990. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Report on Hypertension: The Race against a Silent Killer. September 19, 2023. Available online: https://www.who.int/publications/i/item/9789240081062 (accessed on 30 September 2023).
- Weir, M.R.; Bakris, G.L. Combination Therapy With Renin-Angiotensin-Aldosterone Receptor Blockers for Hypertension: How Far Have We Come? J. Clin. Hypertens. 2008, 10, 146–152. [Google Scholar] [CrossRef]
- Narita, K.; Hoshide, S.; Kario, K. The role of blood pressure management in stroke prevention: Current status and future prospects. Expert Rev. Cardiovasc. Ther. 2022, 20, 829–838. [Google Scholar] [CrossRef]
- He, T.; Liu, X.; Li, Y.; Liu, X.Y.; Wu, Q.Y.; Liu, M.L.; Yuan, H. High-dose calcium channel blocker (CCB) monotherapy vs combination therapy of standard-dose CCBs and angiotensin receptor blockers for hypertension: A meta-analysis. J. Hum. Hypertens. 2017, 31, 79–88. [Google Scholar] [CrossRef]
- Filipova, E.; Dineva, S.; Uzunova, K.; Pavlova, V.; Kalinov, K.; Vekov, T. Combining angiotensin receptor blockers with chlorthalidone or hydrochlorothiazide–which is the better alternative? A meta-analysis. Syst. Rev. 2020, 9, 195. [Google Scholar] [CrossRef]
- Matsui, Y.; Eguchi, K.; O’Rourke, M.F.; Ishikawa, J.; Miyashita, H.; Shimada, K.; Kario, K. Differential Effects Between a Calcium Channel Blocker and a Diuretic When Used in Combination With Angiotensin II Receptor Blocker on Central Aortic Pressure in Hypertensive Patients. Hypertension 2009, 54, 716–723. [Google Scholar] [CrossRef]
- Matsui, Y.; Eguchi, K.; Ishikawa, J.; Shimada, K.; Kario, K. Urinary Albumin Excretion During Angiotensin II Receptor Blockade: Comparison of Combination Treatment With a Diuretic or a Calcium-Channel Blocker. Am. J. Hypertens. 2011, 24, 466–473. [Google Scholar] [CrossRef][Green Version]
- Staplin, N.; de la Sierra, A.; Ruilope, L.M.; Emberson, J.R.; Vinyoles, E.; Gorostidi, M.; Ruiz-Hurtado, G.; Segura, J.; Baigent, C.; Williams, B. Relationship between clinic and ambulatory blood pressure and mortality: An observational cohort study in 59 124 patients. Lancet 2023, 401, 2041–2050. [Google Scholar] [CrossRef]
- Yano, Y.; Hoshide, S.; Tamaki, N.; Nagata, M.; Sasaki, K.; Kanemaru, Y.; Shimada, K.; Kario, K. Efficacy of eplerenone added to renin-angiotensin blockade in elderly hypertensive patients: The Jichi-Eplerenone Treatment (JET) study. J. Renin-Angiotensin-Aldosterone Syst. 2011, 12, 340–347. [Google Scholar] [CrossRef]
- Lu, Z.; Chen, Y.; Li, L.; Wang, G.; Xue, H.; Tang, W. Combination therapy of renin–angiotensin system inhibitors plus calcium channel blockers versus other two-drug combinations for hypertension: A systematic review and meta-analysis. J. Hum. Hypertens. 2017, 31, 1–13. [Google Scholar] [CrossRef]
- Kario, K.; Williams, B. Angiotensin receptor–neprilysin inhibitors for hypertension—hemodynamic effects and relevance to hypertensive heart disease. Hypertens. Res. 2022, 45, 1097–1110. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, W.; Yan, J.; Ge, Q.; Lu, X.-H.; Chen, S.-X.; Xu, W.-J.; Li, Y.; Li, J.-F.; He, S.-Y.; et al. Efficacy and safety of sacubitril/allisartan for the treatment of primary hypertension: A phase 2 randomized, double-blind study. Hypertens. Res. 2023, 46, 2024–2032. [Google Scholar] [CrossRef]
- Jackson, A.M.; Jhund, P.S.; Anand, I.S.; Düngen, H.-D.; Lam, C.S.P.; Lefkowitz, M.P.; Linssen, G.; Lund, L.H.; Maggioni, A.P.; Pfeffer, M.A.; et al. Sacubitril–valsartan as a treatment for apparent resistant hypertension in patients with heart failure and preserved ejection fraction. Eur. Heart J. 2021, 42, 3741–3752. [Google Scholar] [CrossRef]
- Kario, K.; Okada, K.; Kato, M.; Nishizawa, M.; Yoshida, T.; Asano, T.; Uchiyama, K.; Niijima, Y.; Katsuya, T.; Urata, H.; et al. 24-Hour Blood Pressure-Lowering Effect of an SGLT-2 Inhibitor in Patients with Diabetes and Uncontrolled Nocturnal Hypertension: Results from the Randomized, Placebo-Controlled SACRA Study. Circulation 2018, 139, 2089–2097. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Fitchett, D.; Inzucchi, S.E.; Cannon, C.P.; McGuire, D.K.; Scirica, B.M.; Johansen, O.E.; Sambevski, S.; Kaspers, S.; Pfarr, E.; George, J.T.; et al. Empagliflozin Reduced Mortality and Hospitalization for Heart Failure Across the Spectrum of Cardiovascular Risk in the EMPA-REG OUTCOME Trial. Circulation 2019, 139, 1384–1395. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- Anker, S.D.; Butler, J.; Filippatos, G.; Ferreira, J.P.; Bocchi, E.; Böhm, M.; Brunner–La Rocca, H.-P.; Choi, D.-J.; Chopra, V.; Chuquiure-Valenzuela, E.; et al. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N. Engl. J. Med. 2021, 385, 1451–1461. [Google Scholar] [CrossRef]
- Masuda, T.; Nagata, D. Fluid homeostasis induced by sodium-glucose cotransporter 2 inhibitors: Novel insight for better cardio-renal outcomes in chronic kidney disease. Hypertens. Res. 2023, 46, 1195–1201. [Google Scholar] [CrossRef]
- Ye, N.; Jardine, M.J.; Oshima, M.; Hockham, C.; Heerspink, H.J.L.; Agarwal, R.; Bakris, G.; Schutte, A.E.; Arnott, C.; Chang, T.I.; et al. Blood Pressure Effects of Canagliflozin and Clinical Outcomes in Type 2 Diabetes and Chronic Kidney Disease: Insights From the CREDENCE Trial. Circulation 2021, 143, 1735–1749. [Google Scholar] [CrossRef]
- Georgianos, P.I.; Agarwal, R. Ambulatory Blood Pressure Reduction With SGLT-2 Inhibitors: Dose-Response Meta-analysis and Comparative Evaluation With Low-Dose Hydrochlorothiazide. Diabetes Care 2019, 42, 693–700. [Google Scholar] [CrossRef]
- Roy, A.; Naik, N.; Reddy, K.S. Strengths and Limitations of Using the Polypill in Cardiovascular Prevention. Curr. Cardiol. Rep. 2017, 19, 45. [Google Scholar] [CrossRef]
- Yusuf, S.; Pinto, F.J. The polypill: From concept and evidence to implementation. Lancet 2022, 400, 1661–1663. [Google Scholar] [CrossRef]
- Rodgers, A.; Smith, R. The polypill and medicines access: Two decades and counting. BMJ 2023, 382, p1847. [Google Scholar] [CrossRef]
- Melville, S.; Byrd, J.B. Personalized Medicine and the Treatment of Hypertension. Curr. Hypertens. Rep. 2019, 21, 13. [Google Scholar] [CrossRef]
- Hu, Y.; Huerta, J.; Cordella, N.; Mishuris, R.G.; Paschalidis, I.C. Personalized hypertension treatment recommendations by a data-driven model. BMC Med Informatics Decis. Mak. 2023, 23, 44. [Google Scholar] [CrossRef]
- Visco, V.; Izzo, C.; Mancusi, C.; Rispoli, A.; Tedeschi, M.; Virtuoso, N.; Giano, A.; Gioia, R.; Melfi, A.; Serio, B.; et al. Artificial Intelligence in Hypertension Management: An Ace up Your Sleeve. J. Cardiovasc. Dev. Dis. 2023, 10, 74. [Google Scholar] [CrossRef]
- Kario, K.; Hoshide, S.; Mogi, M. Digital Hypertension 2023: Concept, hypothesis, and new technology. Hypertens. Res. 2022, 45, 1529–1530. [Google Scholar] [CrossRef]
- Narita, K.; Hoshide, S.; Ae, R.; Kario, K. Simple predictive score for nocturnal hypertension and masked nocturnal hypertension using home blood pressure monitoring in clinical practice. J. Hypertens. 2022, 40, 1513–1521. [Google Scholar] [CrossRef]
- Byrd, J.B. Personalized medicine and treatment approaches in hypertension: Current perspectives. Integr. Blood Press. Control. 2016, 9, 59–67. [Google Scholar] [CrossRef]
- Rey-García, J.; Townsend, R.R. Renal Denervation: A Review. Am. J. Kidney Dis. 2022, 80, 527–535. [Google Scholar] [CrossRef]
- Barbato, E.; Azizi, M.; Schmieder, R.E.; Lauder, L.; Böhm, M.; Brouwers, S.; Bruno, R.M.; Dudek, D.; Kahan, T.; Kandzari, D.E.; et al. Renal denervation in the management of hypertension in adults. A clinical consensus statement of the ESC Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 2023, 44, 1313–1330. [Google Scholar] [CrossRef]
- Kario, K.; Nomura, A.; Harada, N.; Okura, A.; Nakagawa, K.; Tanigawa, T.; Hida, E. Efficacy of a digital therapeutics system in the management of essential hypertension: The HERB-DH1 pivotal trial. Eur. Heart J. 2021, 42, 4111–4122. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Trial | Year | Confirmation of Polypill | Primary or Secondary Prevention | Number of Patients | Findings |
|---|---|---|---|---|---|
| CRUCIAL | 2011 | amlodipine, atorvastatin | - | 1461 | Lower BP and cholesterol with polypill than usual care (UC). Framingham 10-year CHD risk 13% with polypill vs. 16% in usual care. |
| UMPIRE | 2013 | aspirin, simvastatin, lisinopril, atenolol or hydrochlorothiazide | Primary and secondary | 2004 | Lower BP and cholesterol with polypill than UC. There is no difference in major CVD events at median 15 mo. follow-up: 50 (5%) with polypill vs. 35 (3.5%) in UC, RR 1.45, 95%CI 0.94–2.29, p = 0.09 (NS) |
| IMPACT | 2014 | aspirin, simvastatin, lisinopril, atenolol or hydrochlorothiazide | Primary and secondary | 513 | Improved adherence with polypill. No difference in BP and LDL-cholesterol between polypill and UC. There is no difference major CVD events at 12 mo. follow-up: 16 with polypill vs. 18 in UC, p = 0.73 (NS) |
| Kanyini GAP | 2014 | aspirin, simvastatin, lisinopril, atenolol or hydrochlorothiazide | Primary and secondary | 623 | Improved adherence with polypill. No difference in BP and LDL-cholesterol between polypill and UC. |
| FOCUS | 2014 | aspirin, simvastatin. ramipril | Secondary | 2118 | Improved adherence with polypill. No difference in BP and LDL-cholesterol between polypill and UC |
| SPACE | 2016 | aspirin, simvastatin, lisinopril, atenolol or hydrochlorothiazide | Primary and secondary | 3140 | Combination of three trials (UMPIRE, Kyayini GAP, and IMPACT) for polypill. Improved adherence with polypill. Lower BP and cholesterol with polypill than UC. |
| PolyIran | 2022 | aspirin, atorvastatin, hydrochlorothiazide, enalapril or valsartan | Primary and secondary | 6838 | Polypill is associated with reduced major CVD events at 60 mo. follow-up: 202 (5.9%) with polypill vs. 301 (8.8%) in UC, HR 0.66, 95%CI 0.55–0.80. Improved adherence with polypill. |
| SECURE | 2022 | aspirin, ramipril, atorvastatin | Secondary | 2499 | Polypill is associated with reduced major CVD events at 36 mo. follow-up: 118 (9.5%) with polypill vs. 156 (12.7%) in UC, HR 0.76, 95%CI 0.60–0.96, p = 0.02. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Narita, K.; Hoshide, S.; Kario, K. Polypill Therapy for Cardiovascular Disease Prevention and Combination Medication Therapy for Hypertension Management. J. Clin. Med. 2023, 12, 7226. https://doi.org/10.3390/jcm12237226
Narita K, Hoshide S, Kario K. Polypill Therapy for Cardiovascular Disease Prevention and Combination Medication Therapy for Hypertension Management. Journal of Clinical Medicine. 2023; 12(23):7226. https://doi.org/10.3390/jcm12237226
Chicago/Turabian StyleNarita, Keisuke, Satoshi Hoshide, and Kazuomi Kario. 2023. "Polypill Therapy for Cardiovascular Disease Prevention and Combination Medication Therapy for Hypertension Management" Journal of Clinical Medicine 12, no. 23: 7226. https://doi.org/10.3390/jcm12237226
APA StyleNarita, K., Hoshide, S., & Kario, K. (2023). Polypill Therapy for Cardiovascular Disease Prevention and Combination Medication Therapy for Hypertension Management. Journal of Clinical Medicine, 12(23), 7226. https://doi.org/10.3390/jcm12237226