
Effects of a Gait Training Program on Spinal Cord Injury Patients: A Single-Group Prospective Cohort Study

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
- -
- traumatic spinal cord injury older than 19 years;
- -
- onset of more than 1 year;
- -
- upper motor neuron injury with neurological level of injury from T1 to T12;
- -
- and patients with the American Spinal Injury Association (ASIA) Impairment Scale (AIS) A, B, C, or D were included [5].
- -
- joint contracture of the lower extremity;
- -
- fracture risk with severe osteoporosis;
- -
- pressure injuries of the sacrum, ischium, or coccyx;
- -
- cognitive impairment;
- -
- and gait problems prior to spinal cord injury.
2.3. Outcomes Measures
2.3.1. Research Design According to the Gait Training Program Methodology
2.3.2. Initial Evaluation of the Sample
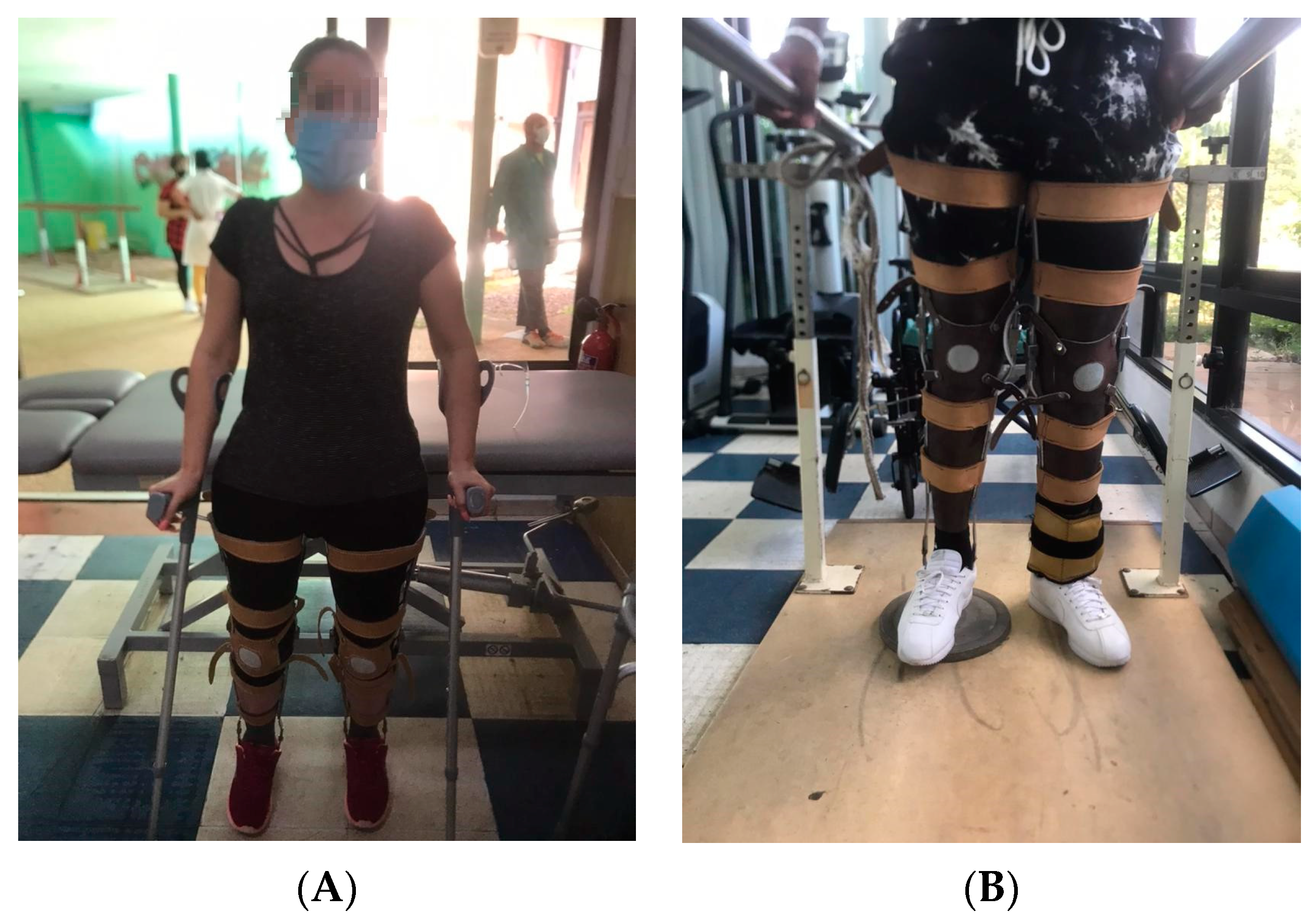
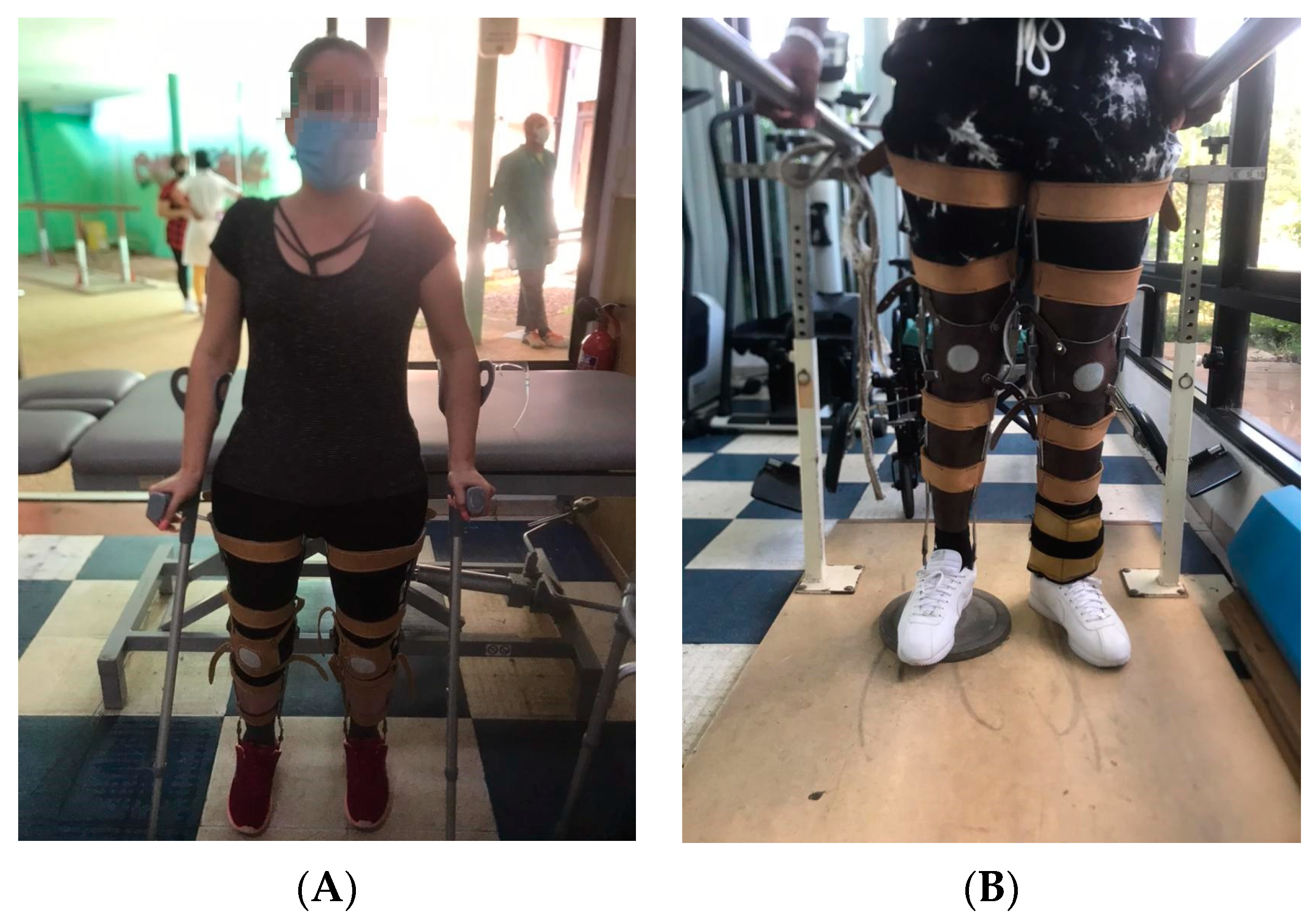
2.3.3. Implementation of the Physical Rehabilitation Program
2.3.4. 1st Stage: General Preparation
2.3.5. 2nd Stage: Special Preparation
2.3.6. 3rd Stage: Functional Preparation
2.4. Final Evaluation of the Sample
2.4.1. Intervention Dosage
2.4.2. Study Evaluations
2.5. Statistical Analysis
3. Sample Size
4. Results
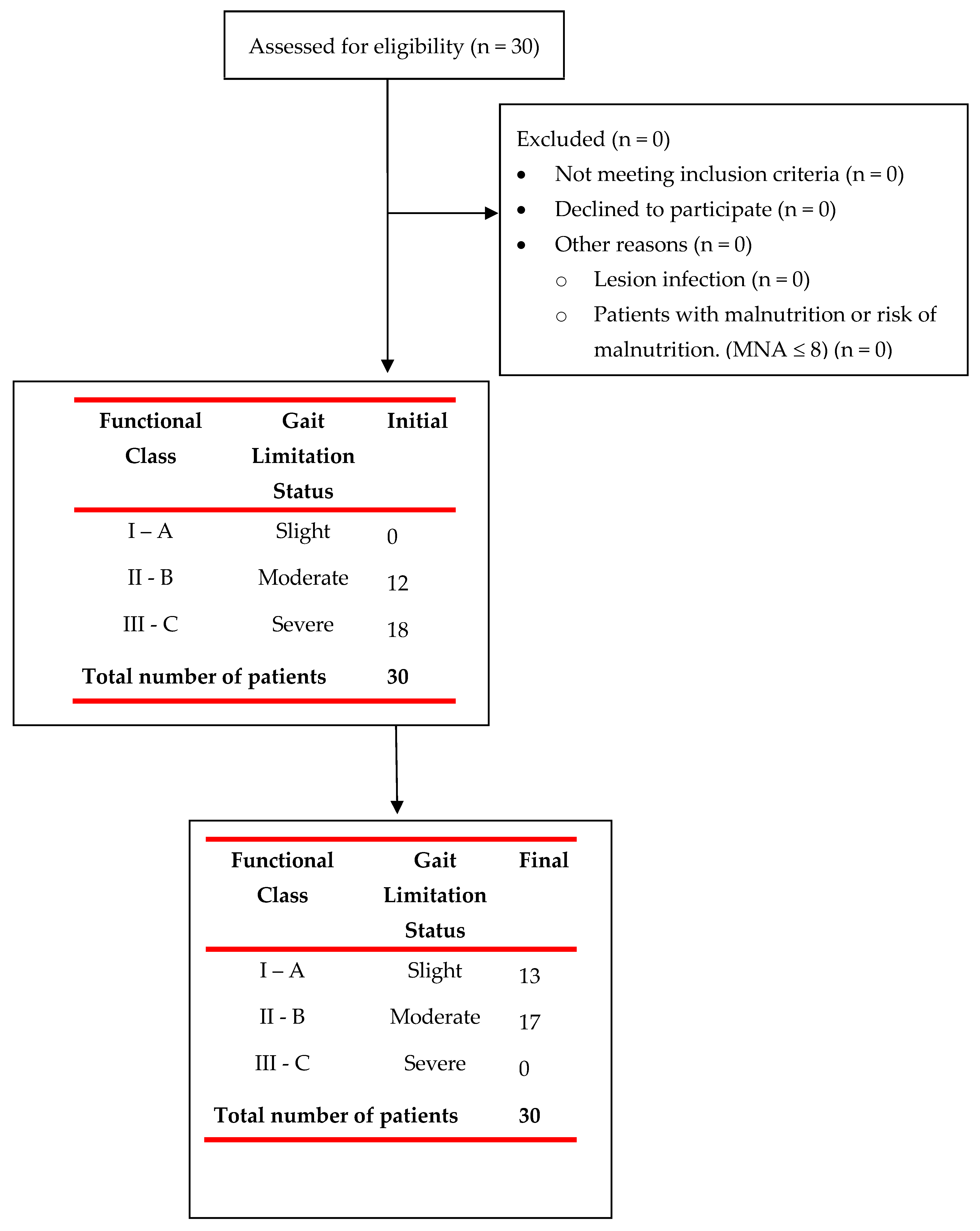
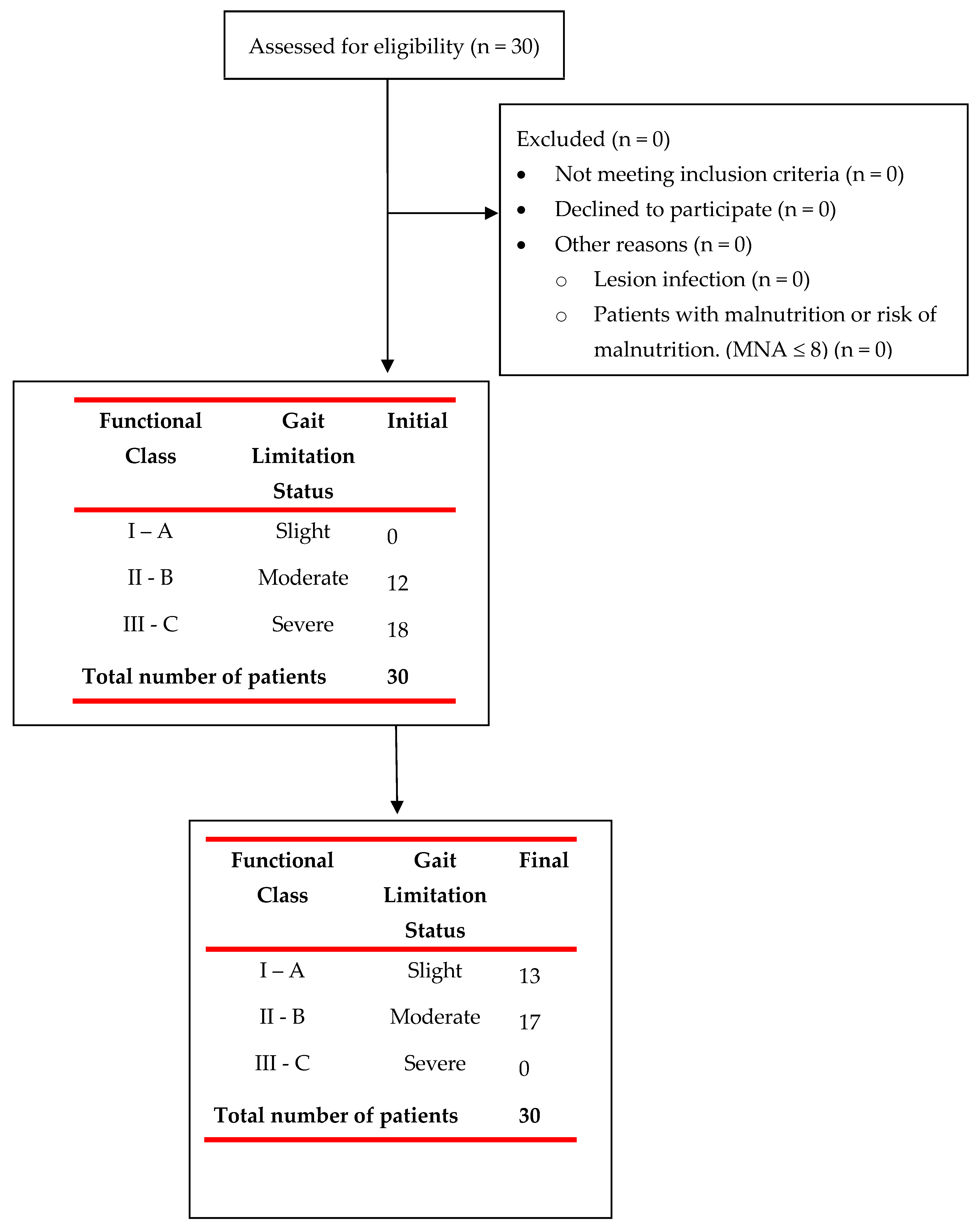
4.1. Patient Flow and Principal Characteristics
4.2. Pre-Post-Treatment Results for All Outcome Variables
5. Discussion
Limitations and Future Directions
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Spinal Cord Injuries Collaborators. Global, regional, and national burden of spinal cord injury, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2023, 22, 1026–1047. [Google Scholar] [CrossRef]
- Crispo, J.A.G.; Kuramoto, L.K.; Cragg, J.J. Global burden of spinal cord injury: Future directions. Lancet Neurol. 2023, 22, 976–978. [Google Scholar] [CrossRef]
- Lema, H.; Pérez, C.; Parra, J. Modelo predictivo del grado de discapacidad en adultos con lesión medular: Resultados desde el Who-Das II. Rev. Cienc. Salud. 2011, 9, 159–172. [Google Scholar]
- Lünenburger, L.; Lam, T.; Riener, R.; Colombo, G. Gait retraining after neurological disorders. In Wiley Encyclopedia of Biomedical Engineering; John & Wiley & Sons: Hoboken, NJ, USA, 2006. [Google Scholar]
- Esclarin, A.R. Lesion medular. In Un Enfoque Multidisciplinario; Medica Panamericana: Madrid, Spain, 2010; 332p. [Google Scholar]
- Field-Fote, E.C.; Fluet, G.G.; Schafer, S.D.; Schneider, E.M.; Smith, R.; Downey, P.A.; Ruhl, C.D. The Spinal Cord Injury Functional Ambulation Inventory (SCI-FAI). J. Rehabil. Med. 2001, 33, 177–181. [Google Scholar] [CrossRef]
- Nene, A.V.; Hermens, H.J.; Zilvold, G. Paraplegic locomotion: A review. Paraplegia 1996, 34, 507–524. [Google Scholar] [CrossRef]
- Bissolotti, L.; Rota, M.; Calza, S.; Sanchez Romero, E.A.; Battaglino, A.; Villafañe, J.H. Relationship between Lower Limbs Performance and Spinal Alignment in Parkinson’s Disease Patients: An Observational Study with Cross Sectional Design. J. Clin. Med. 2022, 11, 3775. [Google Scholar] [CrossRef]
- Zhang, L.; Lin, F.; Sun, L.; Chen, C. Comparison of Efficacy of Lokomat and Wearable Exoskeleton-Assisted Gait Training in People with Spinal Cord Injury: A Systematic Review and Network Meta-Analysis. Front. Neurol. 2022, 13, 772660. [Google Scholar] [CrossRef]
- Stampacchia, G.; Olivieri, M.; Rustici, A.; D’Avino, C.; Gerini, A.; Mazzoleni, S. Gait rehabilitation in persons with spinal cord injury using innovative technologies: An observational study. Spinal Cord 2020, 58, 988–997. [Google Scholar] [CrossRef]
- Fang, C.Y.; Tsai, J.L.; Li, G.S.; Lien, A.S.; Chang, Y.J. Effects of Robot-Assisted Gait Training in Individuals with Spinal Cord Injury: A Meta-analysis. Biomed. Res. Int. 2020, 2020, 2102785. [Google Scholar] [CrossRef]
- Tan, K.; Koyama, S.; Sakurai, H.; Teranishi, T.; Kanada, Y.; Tanabe, S. Wearable robotic exoskeleton for gait reconstruction in patients with spinal cord injury: A literature review. J. Orthop. Transl. 2021, 28, 55–64. [Google Scholar] [CrossRef]
- Zhang, C.; Li, N.; Xue, X.; Lu, X.; Li, D.; Hong, Q. Effects of lower limb exoskeleton gait orthosis compared to mechanical gait orthosis on rehabilitation of patients with spinal cord injury: A systematic review and future perspectives. Gait. Posture 2023, 102, 64–71. [Google Scholar] [CrossRef]
- Patathong, T.; Klaewkasikum, K.; Woratanarat, P.; Rattanasiri, S.; Anothaisintawee, T.; Woratanarat, T.; Thakkinstian, A. The efficacy of gait rehabilitations for the treatment of incomplete spinal cord injury: A systematic review and network meta-analysis. J. Orthop. Surg. Res. 2023, 18, 60. [Google Scholar] [CrossRef]
- Fiore, S.; Battaglino, A.; Sinatti, P.; Sánchez-Romero, E.A.; Ruiz-Rodriguez, I.; Manca, M.; Gargano, S.; Villafañe, J.H. The effectiveness of robotic rehabilitation for the functional recovery of the upper limb in post-stroke patients: A systematic review. Retos 2023, 50, 91–101. [Google Scholar] [CrossRef]
- Di Benedetto, S.; Battaglino, A.; Abuín-Porras, V.; Sánchez-Romero, E.A.; Cantero-Tellez, R.; Valdes, K.; Villafañe, J.H. Evaluation of the factors that impact upper limb coordination in children with cerebral palsy: A narrative review. Retos 2023, 48, 470–480. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Ditunno, J.F., Jr.; Ditunno, P.L.; Scivoletto, G.; Patrick, M.; Dijkers, M.; Barbeau, H.; Burns, A.S.; Marino, R.J.; Schmidt-Read, M. The Walking Index for Spinal Cord Injury (WISCI/WISCI II): Nature, metric properties, use and misuse. Spinal Cord 2013, 51, 346–355. [Google Scholar] [CrossRef]
- Esclarín-De Ruz, A.; Alcobendas-Maestro, M.; Casado-López, A.; Muñoz-González, A.; Florido-Sánchez, M.A.; González-Valdizán, E. Sistema robotizado para la reeducación de la marcha en pacientes con lesión medular incompleta. Rev. Neurol. 2009, 49, 617–622. [Google Scholar] [CrossRef]
- Echemendía del Valle, A.; Sentmanat Belisón, A.; Gómez Pérez, R.; Noa Pelier, B.Y. Cambios funcionales en pacientes con lesiones medulares dorsales altas que son sometidos al programa de rehabilitación. OLIMPIA Rev. De La Fac. De Cult. Física De La Univ. De Granma 2018, 15, 110–125. [Google Scholar]
- Echemendía del Valle, A.; Sentmanat Belisón, A.; Ocaña Rodríguez, F.O. Aplicación del World Health Organization-Disability Assessment Schedule II en el Lesionado Medular. Rev. Cuba. De Med. Del Deporte Y La Cult. Física 2020, 15, e189. [Google Scholar]
- Echemendia del Valle, A. Metodología para el entrenamiento de la marcha convencional en pacientes con lesiones medulares. Estudio preliminar. PODIUM-Rev. De Cienc. Y Tecnol. En La Cult. Física 2021, 16, 757–771. [Google Scholar]
- Yang, J.; Gong, Y.; Yu, L.; Peng, L.; Cui, Y.; Huang, H. Effect of exoskeleton robot-assisted training on gait function in chronic stroke survivors: A systematic review of randomised controlled trials. BMJ Open 2023, 13, e074481. [Google Scholar] [CrossRef]
- De Vitis, A.; Battaglino, A.; Sinatti, P.; Romero, E.A.S.; Bissolotti, L.; Cotella, D.; Villafañe, J.H. Effects of Telemedicine for Postural Instability in Independent Patients with Parkinson’s Disease: A Literature Review. Top. Geriatr. Rehabil. 2023, 39, 294–306. [Google Scholar] [CrossRef]
- Hou, J.; Nelson, R.; Mohammad, N.; Mustafa, G.; Plant, D.; Thompson, F.J.; Bose, P. Effect of Simultaneous Combined Treadmill Training and Magnetic Stimulation on Spasticity and Gait Impairments after Cervical Spinal Cord Injury. J. Neurotrauma 2020, 37, 1999–2013. [Google Scholar] [CrossRef]
- La Rosa, G.; Avola, M.; Di Gregorio, T.; Calabro, R.S.; Onesta, M.P. Gait Recovery in Spinal Cord Injury: A Systematic Review with Metanalysis Involving New Rehabilitative Technologies. Brain Sci. 2023, 13, 703. [Google Scholar] [CrossRef]
- Bin, L.; Wang, X.; Jiatong, H.; Donghua, F.; Qiang, W.; Yingchao, S.; Yiming, M.; Yong, M. The effect of robot-assisted gait training for patients with spinal cord injury: A systematic review and meta-analysis. Front. Neurosci. 2023, 17, 1252651. [Google Scholar] [CrossRef]
- Aguirre-Güemez, A.V.; Pérez-Sanpablo, A.I.; Quinzaños-Fresnedo, J.; Pérez-Zavala, R.; Barrera-Ortiz, A. Walking speed is not the best outcome to evaluate the effect of robotic assisted gait training in people with motor incomplete spinal cord injury: A systematic review with meta-analysis. J. Spinal Cord Med. 2019, 42, 142–154. [Google Scholar] [CrossRef]
- Santos, L.V.; Pereira, E.T.; Reguera-Garcia, M.M.; Oliveira, C.E.P.; Moreira, O.C. Resistance Training and Muscle Strength in people with Spinal cord injury: A systematic review and meta-analysis. J. Bodyw. Mov. Ther. 2022, 29, 154–160. [Google Scholar] [CrossRef]
- Gollie, J.M.; Guccione, A.A.; Keyser, R.E.; Chin, L.M.K.; Panza, G.S.; Herrick, J.E. Walking endurance, muscle oxygen extraction, and perceived fatigability after overground locomotor training in incomplete spinal cord injury: A pilot study. J. Spinal Cord Med. 2022, 45, 381–389. [Google Scholar] [CrossRef]
- Faulkner, J.; Martinelli, L.; Cook, K.; Stoner, L.; Ryan-Stewart, H.; Paine, E.; Hobbs, H.; Lambrick, D. Effects of robotic-assisted gait training on the central vascular health of individuals with spinal cord injury: A pilot study. J. Spinal Cord Med. 2021, 44, 299–305. [Google Scholar] [CrossRef]
- Hu, X.; Lu, J.; Wang, Y.; Pang, R.; Liu, J.; Gou, X.; Bai, X.; Zhang, A.; Cheng, H.; Wang, Q.; et al. Effects of a lower limb walking exoskeleton on quality of life and activities of daily living in patients with complete spinal cord injury: A randomized controlled trial. Technol. Health Care 2023. online ahead of print. [Google Scholar] [CrossRef]
- Lozano-Berrio, V.; Alcobendas-Maestro, M.; Polonio-Lopez, B.; Gil-Agudo, A.; de la Pena-Gonzalez, A.; de Los Reyes-Guzman, A. The Impact of Robotic Therapy on the Self-Perception of Upper Limb Function in Cervical Spinal Cord Injury: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 6321. [Google Scholar] [CrossRef]
- Baunsgaard, C.B.; Nissen, U.V.; Brust, A.K.; Frotzler, A.; Ribeill, C.; Kalke, Y.B.; León, N.; Gómez, B.; Samuelsson, K.; Antepohl, W.; et al. Exoskeleton gait training after spinal cord injury: An exploratory study on secondary health conditions. J. Rehabil. Med. 2018, 50, 806–813. [Google Scholar] [CrossRef]
- Yıldırım, M.A.; Öneş, K.; Gökşenoğlu, G. Early term effects of robotic assisted gait training on ambulation and functional capacity in patients with spinal cord injury. Turk. J. Med. Sci. 2019, 49, 838–843. [Google Scholar] [CrossRef]
- Alajam, R.A.; Alqahtanti, A.S.; Frederick, J.; Liu, W. The feasibility of an 8-Week walking training program using a novel assistive gait training device in individuals with spinal cord injury. Disabil. Rehabil. Assist Technol. 2022, 17, 658–667. [Google Scholar] [CrossRef]
- Gupta, A.; Prakash, N.B.; Honavar, P.R. Gait Training with Robotic Exoskeleton Assisted Rehabilitation System in Patients with Incomplete Traumatic and Non-Traumatic Spinal Cord Injury: A Pilot Study and Review of Literature. Ann. Indian Acad. Neurol. 2023, 26 (Suppl. S1), S26–S31. [Google Scholar] [CrossRef]
- Tarnacka, B.; Korczyński, B.; Frasuńska, J. Impact of Robotic-Assisted Gait Training in Subacute Spinal Cord Injury Patients on Outcome Measure. Diagnostics 2023, 13, 1966. [Google Scholar] [CrossRef]
- Mıdık, M.; Paker, N.; Buğdaycı, D.; Mıdık, A.C. Effects of robot-assisted gait training on lower extremity strength, functional independence, and walking function in men with incomplete traumatic spinal cord injury. Turk. J. Phys. Med. Rehabil. 2020, 66, 54–59. [Google Scholar] [CrossRef]
- Tamburella, F.; Tagliamonte, N.L.; Masciullo, M.; Pisotta, I.; Arquilla, M.; van Asseldonk, E.H.F.; van der Kooij, H.; Wu, A.R.; Dzeladini, F.; Ijspeert, A.J.; et al. Gait training with Achilles ankle exoskeleton in chronic incomplete spinal cord injury subjects. J. Biol. Regul. Homeost. Agents 2020, 34 (Suppl. S3), 147–164. [Google Scholar]
- Lucareli, P.R.G.; Lim, C.; Garbelotti, J.S.A.; Gimenes, R.O.; Almeida, J.G.; Greve, J.M.D. Análisis de la marcha y evaluación de la calidad de vida después del entrenamiento de la marcha en pacientes con lesión medular. Rev. Neurol. 2008, 46, 406–410. [Google Scholar] [CrossRef]
- Alashram, A.R.; Annino, G.; Padua, E. Robot-assisted gait training in individuals with spinal cord injury: A systematic review for the clinical effectiveness of Lokomat. J. Clin. Neurosci. 2021, 91, 260–269. [Google Scholar] [CrossRef]
- Zarco-Perinan, M.J.; Barrera-Chacon, M.J.; Garcia-Obrero, I.; Mendez-Ferrer, J.B.; Alarcon, L.E.; Echevarria-Ruiz de Vargas, C. Development of the Spanish version of the Spinal Cord Independence Measure version III: Cross-cultural adaptation and reliability and validity study. Disabil. Rehabil. 2014, 36, 1644–1651. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Functional Class | WISCI-II | SCIM III (Mobility) | Gait Limitation Status |
|---|---|---|---|
| I—A | 10 & > | 29 & > | Slight |
| II—B | 6–9 | 18–28 | Moderate |
| III—C | 0–5 | 0–17 | Severe |
| n | 30 | |
|---|---|---|
| Age | 35.33 ± 6.25 | |
| Gender, n (%) | Female | 11 (36.7) |
| Male | 19 (63.3) | |
| Time of evolution (years) | 3.03 ± 1.13 | |
| Topographic level, n (%) | T1 | 2 (6.7) |
| T10 | 6 (20.0) | |
| T11 | 1 (3.3) | |
| T12 | 4 (13.3) | |
| T4 | 3 (10.0) | |
| T5 | 2 (6.7) | |
| T6 | 5 (16.7) | |
| T7 | 2 (6.7) | |
| T8 | 5 (16.7) | |
| Injury level, n (%) | High (T1–T6) | 12 (40.0) |
| Low (T7–T12) | 18 (60.0) | |
| ASIA, n (%) | A | 16 (53.3) |
| B | 14 (46.7) |
| Post-Treatment | Pre-Treatment | Average Difference (95%CI) | Measurement Time a | Measurement Time: Injury Level a | Measurement Time: Gender a | Effect Size (95%CI) | ||
|---|---|---|---|---|---|---|---|---|
| WISCI | 10.43 ± 1.74 | 4.30 ± 3.02 | 6.133 (4.854, 7.413) | F(1, 27) = 145.805, p < 0.001 | F(1, 27) = 0.527, p = 0.474 | F(1, 27) = 1.087, p = 0.306 | 2.102 (0.823, 5.839) * | |
| WISCI functional group, n (%) | I | 13 (43.3) | 0 (0.0) | X2(1) = 28, p < 0.001 | M2(2) = 0.044, p = 0.978 | M2(2) = 0.239, p = 0.887 | 0.933 ↑ | |
| II | 17 (56.7) | 12 (40.0) | ||||||
| III | 0 (0.0) | 18 (60.0) | ||||||
| Mobility in bed | 5.93 ± 0.37 | 4.40 ± 1.22 | 1.533 (1.061, 2.006) | F(1, 27) = 44.992, p < 0.001 | F(1, 27) = 2.034, p = 0.165 | F(1, 27) = 0.028, p = 0.868 | 1.048 (0.394, 3.61) * | |
| Bed chair transfer | 2.00 ± 0.00 | 1.87 ± 0.35 | 0.133 (0.004, 0.262) | F(1, 53.989) = 2.605, p = 0.112 | F(1, 53.989) = 2.969, p = 0.091 | F(1, 53.989) = 0.14, p = 0.71 | 0.062 * | |
| Transfer chair toilet bath | 2.00 ± 0.00 | 1.77 ± 0.43 | 0.233 (0.073, 0.394) | F(1, 54) = 7.449, p = 0.009 | F(1, 54) = 0.505, p = 0.48 | F(1, 54) = 0.186, p = 0.668 | 0.354 (0, 1.238) * | |
| Indoor mobility | 4.43 ± 0.50 | 2.80 ± 1.00 | 1.633 (1.222, 2.045) | F(1, 27) = 112.461, p < 0.001 | F(1, 27) = 0.06, p = 0.808 | F(1, 27) = 0.195, p = 0.662 | 2.019 (0.759, 4.01) * | |
| Mobility over moderate distances | 4.43 ± 0.50 | 2.73 ± 0.98 | 1.7 (1.294, 2.106) | F(1, 27) = 206.136, p < 0.001 | F(1, 27) = 0.614, p = 0.44 | F(1, 27) = 1.013, p = 0.323 | 2.562 (0.854, 5.461) * | |
| Outdoor mobility | 4.23 ± 0.43 | 2.27 ± 0.69 | 1.967 (1.668, 2.266) | F(1, 27) = 222.924, p < 0.001 | F(1, 27) = 3.691, p = 0.065 | F(1, 27) = 1.118, p = 0.3 | 3.203 (1.575, 6.817) * | |
| Handling on stairs | 0.97 ± 0.93 | 0.07 ± 0.25 | 0.9 (0.543, 1.257) | F(1, 27) = 28.535, p < 0.001 | F(1, 27) = 0.206, p = 0.653 | F(1, 27) = 0.175, p = 0.679 | 1.26 (0.392, 2.843) * | |
| Chair car transfer | 2.00 ± 0.00 | 1.30 ± 0.60 | 0.7 (0.477, 0.923) | F(1, 32.33) = 38.912, p < 0.001 | F(1, 32.33) = 0.09, p = 0.766 | F(1, 32.33) = 0.608, p = 0.441 | 1.356 (0.193, 3.645) * | |
| Floor chair transfer | 0.73 ± 0.91 | 0.03 ± 0.18 | 0.7 (0.356, 1.044) | F(1, 27) = 15.305, p = 0.001 | F(1, 27) = 0.02, p = 0.89 | F(1, 27) = 0.078, p = 0.782 | 0.712 (0.024, 1.798) * | |
| Subtotal | 26.73 ± 3.14 | 17.23 ± 3.93 | 9.5 (7.66, 11.34) | F(1, 27) = 397.559, p < 0.001 | F(1, 27) = 0.319, p = 0.577 | F(1, 27) = 0.242, p = 0.627 | 3.843 (1.717, 11.425) * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Echemendía del Valle, A.; Bender del Busto, J.E.; Sentmanat Belisón, A.; Cuenca-Zaldívar, J.N.; Martínez-Pozas, O.; Martínez-Lozano, P.; Fernández-Carnero, S.; Valcárcel Izquierdo, N.; Sánchez-Romero, E.A. Effects of a Gait Training Program on Spinal Cord Injury Patients: A Single-Group Prospective Cohort Study. J. Clin. Med. 2023, 12, 7208. https://doi.org/10.3390/jcm12237208
Echemendía del Valle A, Bender del Busto JE, Sentmanat Belisón A, Cuenca-Zaldívar JN, Martínez-Pozas O, Martínez-Lozano P, Fernández-Carnero S, Valcárcel Izquierdo N, Sánchez-Romero EA. Effects of a Gait Training Program on Spinal Cord Injury Patients: A Single-Group Prospective Cohort Study. Journal of Clinical Medicine. 2023; 12(23):7208. https://doi.org/10.3390/jcm12237208
Chicago/Turabian StyleEchemendía del Valle, Alexander, Juan Enrique Bender del Busto, Armando Sentmanat Belisón, Juan Nicolás Cuenca-Zaldívar, Oliver Martínez-Pozas, Pedro Martínez-Lozano, Samuel Fernández-Carnero, Norberto Valcárcel Izquierdo, and Eleuterio A. Sánchez-Romero. 2023. "Effects of a Gait Training Program on Spinal Cord Injury Patients: A Single-Group Prospective Cohort Study" Journal of Clinical Medicine 12, no. 23: 7208. https://doi.org/10.3390/jcm12237208
APA StyleEchemendía del Valle, A., Bender del Busto, J. E., Sentmanat Belisón, A., Cuenca-Zaldívar, J. N., Martínez-Pozas, O., Martínez-Lozano, P., Fernández-Carnero, S., Valcárcel Izquierdo, N., & Sánchez-Romero, E. A. (2023). Effects of a Gait Training Program on Spinal Cord Injury Patients: A Single-Group Prospective Cohort Study. Journal of Clinical Medicine, 12(23), 7208. https://doi.org/10.3390/jcm12237208