
Low Energy Intake Diagnosed Using the Harris–Benedict Equation Is Associated with Poor Prognosis in Elderly Heart Failure Patients
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
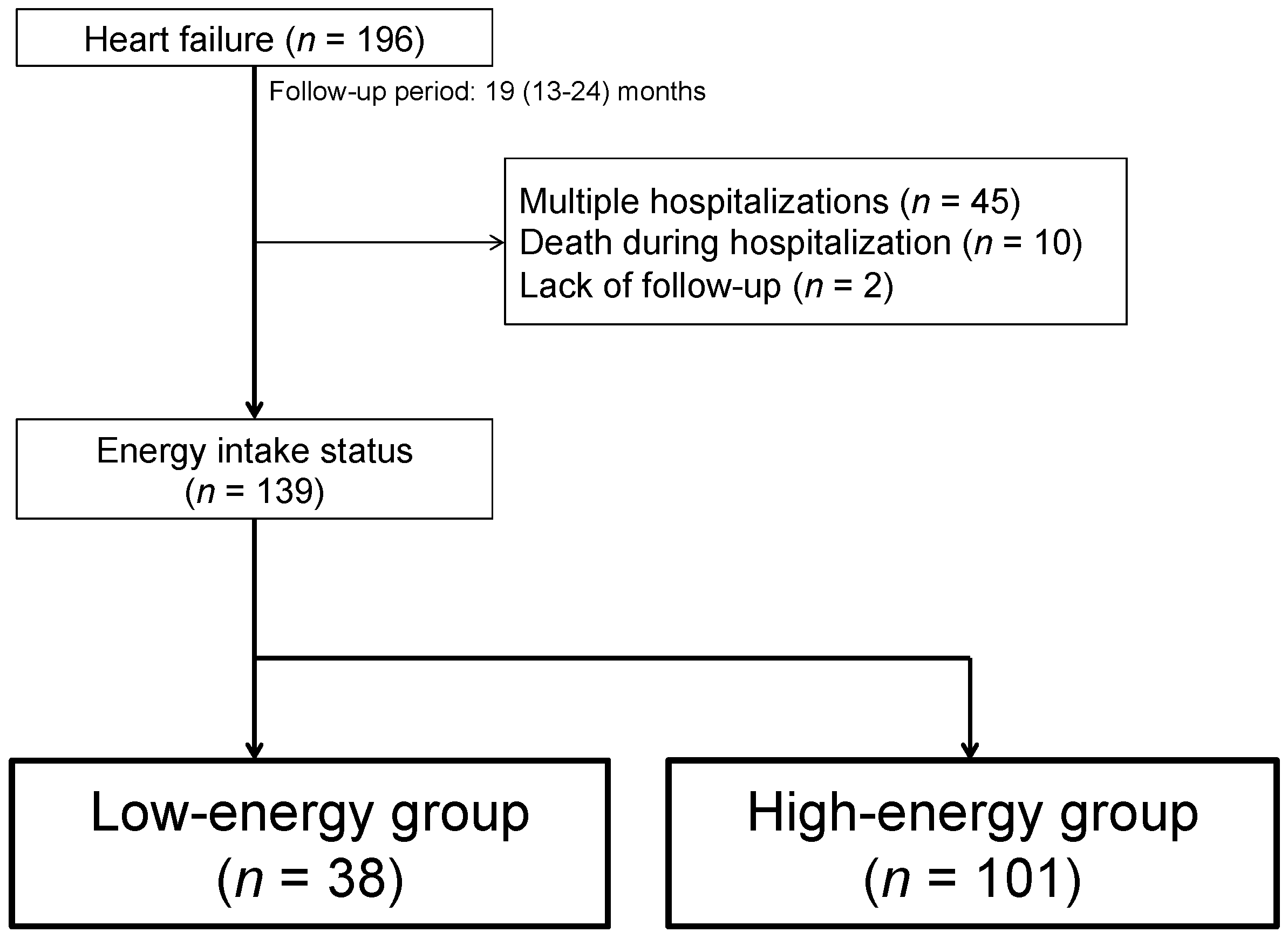
2.1. Subjects
2.2. Patient Characteristics
2.3. Dietary Assessment
2.4. Malnutrition Screening Tools
2.5. MAGGIC Risk Score
2.6. Outcomes and Follow-Up
2.7. Statistical Analyses
3. Results
3.1. General Observations
3.2. Multivariate Analysis of the Determinants of Low Energy Intake
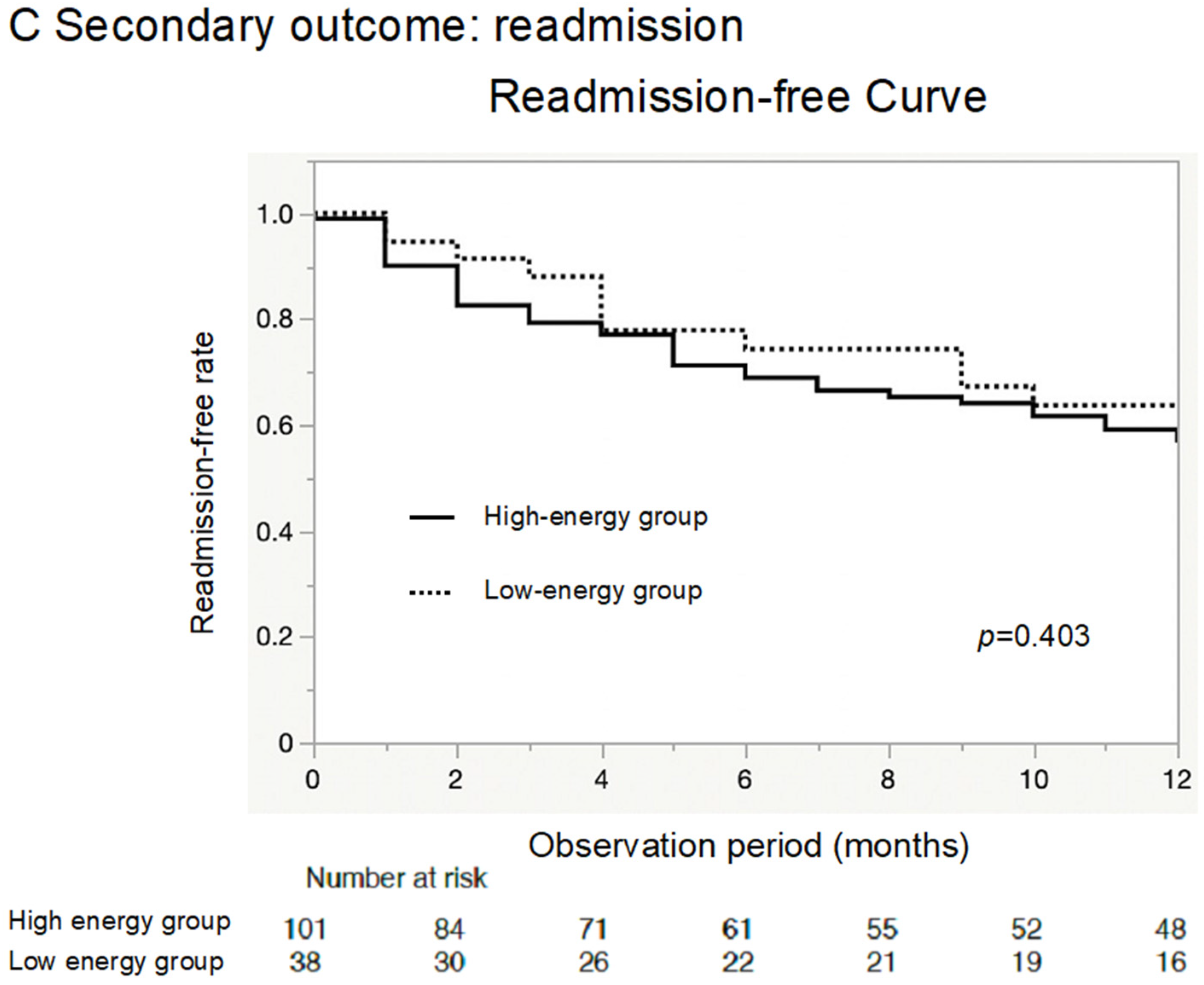
3.3. Prognosis of Patients with Low Energy Intake
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Honda, Y.; Nagai, T.; Iwakami, N.; Sugano, Y.; Honda, S.; Okada, A.; Asaumi, Y.; Aiba, T.; Noguchi, T.; Kusano, K.; et al. Usefulness of Geriatric Nutritional Risk Index for Assessing Nutritional Status and Its Prognostic Impact in Patients Aged >/=65 Years With Acute Heart Failure. Am. J. Cardiol. 2016, 118, 550–555. [Google Scholar] [CrossRef]
- Anker, S.D.; Ponikowski, P.; Varney, S.; Chua, T.P.; Clark, A.L.; Webb-Peploe, K.M.; Harrington, D.; Kox, W.J.; Poole-Wilson, P.A.; Coats, A.J. Wasting as independent risk factor for mortality in chronic heart failure. Lancet 1997, 349, 1050–1053. [Google Scholar] [CrossRef] [PubMed]
- Pocock, S.J.; Ariti, C.A.; McMurray, J.J.; Maggioni, A.; Kober, L.; Squire, I.B.; Swedberg, K.; Dobson, J.; Poppe, K.K.; Whalley, G.A.; et al. Predicting survival in heart failure: A risk score based on 39 372 patients from 30 studies. Eur. Heart J. 2013, 34, 1404–1413. [Google Scholar] [CrossRef]
- Sawano, M.; Shiraishi, Y.; Kohsaka, S.; Nagai, T.; Goda, A.; Mizuno, A.; Sujino, Y.; Nagatomo, Y.; Kohno, T.; Anzai, T.; et al. Performance of the MAGGIC heart failure risk score and its modification with the addition of discharge natriuretic peptides. ESC Heart Fail. 2018, 5, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Khanam, S.S.; Choi, E.; Son, J.W.; Lee, J.W.; Youn, Y.J.; Yoon, J.; Lee, S.H.; Kim, J.Y.; Ahn, S.G.; Ahn, M.S.; et al. Validation of the MAGGIC (Meta-Analysis Global Group in Chronic Heart Failure) heart failure risk score and the effect of adding natriuretic peptide for predicting mortality after discharge in hospitalized patients with heart failure. PLoS ONE 2018, 13, e0206380. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Ignacio de Ulibarri, J.; Gonzalez-Madrono, A.; de Villar, N.G.; Gonzalez, P.; Gonzalez, B.; Mancha, A.; Rodriguez, F.; Fernandez, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Hiesmayr, M.; Schindler, K.; Pernicka, E.; Schuh, C.; Schoeniger-Hekele, A.; Bauer, P.; Laviano, A.; Lovell, A.D.; Mouhieddine, M.; Schuetz, T.; et al. Decreased food intake is a risk factor for mortality in hospitalised patients: The NutritionDay survey 2006. Clin. Nutr. 2009, 28, 484–491. [Google Scholar] [CrossRef]
- Villet, S.; Chiolero, R.L.; Bollmann, M.D.; Revelly, J.P.; Cayeux, R.N.M.; Delarue, J.; Berger, M.M. Negative impact of hypocaloric feeding and energy balance on clinical outcome in ICU patients. Clin. Nutr. 2005, 24, 502–509. [Google Scholar] [CrossRef]
- Harris, J.A.; Benedict, F.G. A Biometric Study of Human Basal Metabolism. Proc. Natl. Acad. Sci. USA 1918, 4, 370–373. [Google Scholar] [CrossRef]
- Jesus, P.; Achamrah, N.; Grigioni, S.; Charles, J.; Rimbert, A.; Folope, V.; Petit, A.; Dechelotte, P.; Coeffier, M. Validity of predictive equations for resting energy expenditure according to the body mass index in a population of 1726 patients followed in a Nutrition Unit. Clin. Nutr. 2015, 34, 529–535. [Google Scholar] [CrossRef]
- Compher, C.; Cato, R.; Bader, J.; Kinosian, B. Harris-Benedict equations do not adequately predict energy requirements in elderly hospitalized African Americans. J. Natl. Med. Assoc. 2004, 96, 209–214. [Google Scholar]
- Anderson, T.; Cascino, T.M.; Koelling, T.M.; Perry, D.; Grafton, G.; Houston, D.K.; Upadhya, B.; Kitzman, D.W.; Hummel, S.L. Measured Versus Estimated Resting Metabolic Rate in Heart Failure With Preserved Ejection Fraction. Circ. Heart Fail. 2021, 14, e007962. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Shoji, S.; Shiraishi, Y.; Kawana, M.; Kohno, T.; Inoue, K.; Fukuda, K.; Heidenreich, P.A.; Kohsaka, S. Hospital meal intake in acute heart failure patients and its association with long-term outcomes. Open Heart 2020, 7, e001248. [Google Scholar] [CrossRef]
- Breslow, R.A.; Sorkin, J.D. Comparison of one-day and three-day calorie counts in hospitalized patients: A pilot study. J. Am. Geriatr. Soc. 1993, 41, 923–927. [Google Scholar] [CrossRef]
- Sze, S.; Pellicori, P.; Kazmi, S.; Rigby, A.; Cleland, J.G.F.; Wong, K.; Clark, A.L. Prevalence and Prognostic Significance of Malnutrition Using 3 Scoring Systems Among Outpatients With Heart Failure: A Comparison With Body Mass Index. JACC. Heart Fail. 2018, 6, 476–486. [Google Scholar] [CrossRef]
- Sze, S.; Pellicori, P.; Zhang, J.; Clark, A.L. Malnutrition, congestion and mortality in ambulatory patients with heart failure. Heart 2019, 105, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Tsutamoto, T.; Wada, A.; Maeda, K.; Hisanaga, T.; Maeda, Y.; Fukai, D.; Ohnishi, M.; Sugimoto, Y.; Kinoshita, M. Attenuation of compensation of endogenous cardiac natriuretic peptide system in chronic heart failure: Prognostic role of plasma brain natriuretic peptide concentration in patients with chronic symptomatic left ventricular dysfunction. Circulation 1997, 96, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Price, J.F.; Thomas, A.K.; Grenier, M.; Eidem, B.W.; O’Brian Smith, E.; Denfield, S.W.; Towbin, J.A.; Dreyer, W.J. B-type natriuretic peptide predicts adverse cardiovascular events in pediatric outpatients with chronic left ventricular systolic dysfunction. Circulation 2006, 114, 1063–1069. [Google Scholar] [CrossRef]
- Nishii, M.; Inomata, T.; Takehana, H.; Naruke, T.; Yanagisawa, T.; Moriguchi, M.; Takeda, S.; Izumi, T. Prognostic utility of B-type natriuretic peptide assessment in stable low-risk outpatients with nonischemic cardiomyopathy after decompensated heart failure. J. Am. Coll. Cardiol. 2008, 51, 2329–2335. [Google Scholar] [CrossRef]
- Nakamura, T.; Haraguchi, Y.; Matsumoto, M.; Ishida, T.; Momomura, S.I. Prognostic impact of malnutrition in elderly patients with acute myocardial infarction. Heart Vessel. 2022, 37, 385–391. [Google Scholar] [CrossRef]
- Kinugasa, Y.; Kato, M.; Sugihara, S.; Hirai, M.; Yamada, K.; Yanagihara, K.; Yamamoto, K. Geriatric nutritional risk index predicts functional dependency and mortality in patients with heart failure with preserved ejection fraction. Circ. J. Off. J. Jpn. Circ. Soc. 2013, 77, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Yasumura, K.; Abe, H.; Iida, Y.; Kato, T.; Nakamura, M.; Toriyama, C.; Nishida, H.; Idemoto, A.; Shinouchi, K.; Mishima, T.; et al. Prognostic impact of nutritional status and physical capacity in elderly patients with acute decompensated heart failure. ESC Heart Fail. 2020, 7, 1801–1808. [Google Scholar] [CrossRef]
- Horwich, T.B.; Fonarow, G.C.; Hamilton, M.A.; MacLellan, W.R.; Woo, M.A.; Tillisch, J.H. The relationship between obesity and mortality in patients with heart failure. J. Am. Coll. Cardiol. 2001, 38, 789–795. [Google Scholar] [CrossRef]
- Anker, S.D.; Negassa, A.; Coats, A.J.; Afzal, R.; Poole-Wilson, P.A.; Cohn, J.N.; Yusuf, S. Prognostic importance of weight loss in chronic heart failure and the effect of treatment with angiotensin-converting-enzyme inhibitors: An observational study. Lancet 2003, 361, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Kenchaiah, S.; Pocock, S.J.; Wang, D.; Finn, P.V.; Zornoff, L.A.; Skali, H.; Pfeffer, M.A.; Yusuf, S.; Swedberg, K.; Michelson, E.L.; et al. Body mass index and prognosis in patients with chronic heart failure: Insights from the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) program. Circulation 2007, 116, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Vest, A.R.; Chan, M.; Deswal, A.; Givertz, M.M.; Lekavich, C.; Lennie, T.; Litwin, S.E.; Parsly, L.; Rodgers, J.E.; Rich, M.W.; et al. Nutrition, Obesity, and Cachexia in Patients With Heart Failure: A Consensus Statement from the Heart Failure Society of America Scientific Statements Committee. J. Card. Fail. 2019, 25, 380–400. [Google Scholar] [CrossRef]
- Hodin, C.M.; Lenaerts, K.; Grootjans, J.; de Haan, J.J.; Hadfoune, M.; Verheyen, F.K.; Kiyama, H.; Heineman, E.; Buurman, W.A. Starvation compromises Paneth cells. Am. J. Pathol. 2011, 179, 2885–2893. [Google Scholar] [CrossRef]
- Genton, L.; Cani, P.D.; Schrenzel, J. Alterations of gut barrier and gut microbiota in food restriction, food deprivation and protein-energy wasting. Clin. Nutr. 2015, 34, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Elia, M.; Behrens, R.; Northrop, C.; Wraight, P.; Neale, G. Evaluation of mannitol, lactulose and 51Cr-labelled ethylenediaminetetra-acetate as markers of intestinal permeability in man. Clin. Sci. 1987, 73, 197–204. [Google Scholar] [CrossRef]
- Kane, A.V.; Dinh, D.M.; Ward, H.D. Childhood malnutrition and the intestinal microbiome. Pediatr. Res. 2015, 77, 256–262. [Google Scholar] [CrossRef]
- Schroeder, B.O.; Backhed, F. Signals from the gut microbiota to distant organs in physiology and disease. Nat. Med. 2016, 22, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- McMurray, D.N.; Mintzer, C.L.; Bartow, R.A.; Parr, R.L. Dietary protein deficiency and Mycobacterium bovis BCG affect interleukin-2 activity in experimental pulmonary tuberculosis. Infect. Immun. 1989, 57, 2606–2611. [Google Scholar] [CrossRef] [PubMed]
- Maldonado Galdeano, C.; Novotny Nunez, I.; de Moreno de LeBlanc, A.; Carmuega, E.; Weill, R.; Perdigon, G. Impact of a probiotic fermented milk in the gut ecosystem and in the systemic immunity using a non-severe protein-energy-malnutrition model in mice. BMC Gastroenterol. 2011, 11, 64. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.C.; Wang, J.T.; Wei, S.C.; Ni, Y.H. Host-microbial interactions and regulation of intestinal epithelial barrier function: From physiology to pathology. World J. Gastrointest. Pathophysiol. 2012, 3, 27–43. [Google Scholar] [CrossRef] [PubMed]
- Compher, C.; Kim, J.N.; Bader, J.G. Nutritional requirements of an aging population with emphasis on subacute care patients. AACN Clin. Issues 1998, 9, 441–450. [Google Scholar] [CrossRef]
- Hersberger, L.; Dietz, A.; Burgler, H.; Bargetzi, A.; Bargetzi, L.; Kagi-Braun, N.; Tribolet, P.; Gomes, F.; Hoess, C.; Pavlicek, V.; et al. Individualized Nutritional Support for Hospitalized Patients With Chronic Heart Failure. J. Am. Coll. Cardiol. 2021, 77, 2307–2319. [Google Scholar] [CrossRef] [PubMed]
- Ammar, K.A.; Jacobsen, S.J.; Mahoney, D.W.; Kors, J.A.; Redfield, M.M.; Burnett, J.C., Jr.; Rodeheffer, R.J. Prevalence and prognostic significance of heart failure stages: Application of the American College of Cardiology/American Heart Association heart failure staging criteria in the community. Circulation 2007, 115, 1563–1570. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Low-Energy Group | High-Energy Group | p Value | |
|---|---|---|---|
| (n = 38) | (n = 101) | ||
| Baseline Clinical Characteristics | |||
| Age, years | 81.2 ± 13.7 | 79.1 ± 10.3 | 0.336 |
| Female | 35 (92) | 24 (24) | <0.0001 |
| Hospital stay, days | 22 [17, 30] | 20 [15, 30] | 0.755 |
| Number of previous hospitalizations | 1.8 ± 1.8 | 2.0 ± 2.2 | 0.472 |
| Family living together | 24 (63) | 71 (70) | 0.422 |
| Hypertension | 29 (76) | 75 (74) | 1.000 |
| Diabetes mellitus | 14 (37) | 36 (36) | 0.333 |
| Dyslipidemia | 13 (34) | 39 (39) | 0.697 |
| Smoking (current/past/never) | 2/6/30 | 10/42/49 | 0.005 |
| Atrial fibrillation | 18 (47) | 42 (42) | 0.569 |
| Ischemic heart disease | 3 (8) | 33 (33) | 0.002 |
| Left ventricular ejection fraction, % | 44.6 ± 16.4 | 38.3 ± 15.6 | 0.041 |
| EF category (pEF/mrEF/rEF) | 18/3/17 | 30/17/56 | 0.097 |
| Vital, physical, laboratory, echocardiological, and nutritional data at admission | |||
| Body weight, kg | 54.5 ± 13.3 | 57.2 ± 11.9 | 0.306 |
| Heart rate, beats/min | 102.5 ± 29.1 | 90.9 ± 23.8 | 0.017 |
| Systolic blood pressure, mmHg | 140.4 ± 30.9 | 133.4 ± 25.8 | 0.180 |
| Diastolic blood pressure, mmHg | 76.2 ± 19.8 | 76.3 ± 18.3 | 0.987 |
| Body mass index, kg/m2 | 23.2 ± 3.9 | 23.0 ± 3.9 | 0.865 |
| NYHA classification (1/2/3/4) | 0/5/22/11 | 0/31/54/18 | 0.080 |
| Hemoglobin, g/dL | 11.4 ± 2.0 | 11.9 ± 1.9 | 0.232 |
| Creatinine, mg/dL | 1.1 ± 0.5 | 1.4 ± 0.8 | 0.111 |
| BUN, mg/dL | 27.0 ± 13.2 | 26.3 ± 14.5 | 0.809 |
| eGFR, mL/min/1.73 m2 | 40.0 [28.2, 54.8] | 47.6 [32.6, 59.1] | 0.247 |
| BNP (pg/mL) | 651.7 [447.0, 893.8] | 756.0 [504.9, 1203.4] | 0.525 |
| CRP (mg/dL) | 0.8 ± 1.4 | 1.1 ± 2.1 | 0.446 |
| Troponin I (pg/mL) | 51.1 [21.0, 230.0] | 109.8 [35.9, 465.9] | 0.216 |
| Albumin (mg/dL) | 3.6 ± 0.4 | 3.6 ± 0.4 | 0.886 |
| GNRI | 99.3 ± 9,8 | 98.0 ± 9.8 | 0.572 |
| CONUT | 2.0 ± 1.7 | 2.1 ± 1.7 | 0.737 |
| Vital, physical, laboratory, echocardiological, and nutritional data at discharge | |||
| Body weight, kg | 48.6 ± 13.1 | 52.8 ± 10.5 | 0.056 |
| Heart rate, beats/min | 74.4 ± 14.3 | 72.3 ± 11.1 | 0.354 |
| Systolic blood pressure, mmHg | 119.4 ± 16.7 | 113.6 ± 15.8 | 0.060 |
| Diastolic blood pressure, mmHg | 63.9 ± 10.1 | 62.6 ± 10.6 | 0.513 |
| Body mass index, kg/m2 | 21.0 ± 4.3 | 21.1 ± 3.5 | 0.862 |
| NYHA classification (1/2/3/4) | 6/28/4/0 | 33/65/3/0 | 0.101 |
| Hemoglobin, g/dL | 12.0 ± 2.0 | 12.0 ± 1.8 | 0.899 |
| Creatinine, mg/dL | 1.2 ± 0.5 | 1.5 ± 1.1 | 0.118 |
| BUN, mg/dL | 31.2 ± 18.7 | 31.4 ± 19.7 | 0.951 |
| eGFR, mL/min/1.73m2 | 40.1 [28.4, 52.2] | 43.2 [34.6, 52.9] | 0.502 |
| BNP, pg/mL | 261.0 [124.7, 460.0] | 259.7 [138.0, 520.0] | 0.677 |
| Albumin, mg/dl | 3.6 ± 0.3 | 3.6 ± 0.4 | 0.835 |
| GNRI | 91.8 ± 11.4 | 93.1 ± 7.6 | 0.548 |
| CONUT | 1.3 ± 1.5 | 1.2 ± 1.4 | 0.793 |
| MAGGIC risk score | 24.8 ± 6.4 | 26.7 ± 6.6 | 0.139 |
| Low-Energy Group | High-Energy Group | p Value | |
|---|---|---|---|
| (n = 38) | (n = 101) | ||
| At admission | |||
| GNRI (normal/mild/moderate/severe) | 27/5/4/2 | 63/16/22/0 | 0.054 |
| CONUT (normal/mild/moderate/severe) | 15/20/3/0 | 41/48/12/0 | 0.755 |
| At discharge | |||
| GNRI (normal/mild/moderate/severe) | 10/11/12/5 | 26/32/38/3 | 0.402 |
| CONUT (normal/mild/moderate/severe) | 25/0/13/0 | 61/38/2/0 | 0.616 |
| Low-Energy Group | High-Energy Group | p Value | |
|---|---|---|---|
| (n = 38) | (n = 101) | ||
| ACEi/ARB | 21 (55) | 67 (66) | 0.242 |
| β blocker | 24 (68) | 67 (66) | 0.816 |
| MRA | 7 (18) | 36 (36) | 0.0502 |
| Loop diuretic | 33 (87) | 92 (91) | 0.529 |
| Tolvaptan | 12 (32) | 32 (32) | 1.000 |
| Calcium blocker | 10 (26) | 30 (30) | 0.834 |
| Digitalis | 2 (5) | 1 (1) | 0.181 |
| Oral inotropic drug | 2 (5) | 12 (12) | 0.350 |
| Statin | 11 (29) | 32 (32) | 0.839 |
| Odds Ratio | 95% CI | p Value | |
|---|---|---|---|
| Female | 82.760 | 8.967–872.729 | <0.001 |
| Smoking habit (y/n) | 4.937 | 0.505–41.945 | 0.092 |
| Ischemic heart disease | 0.439 | 0.095–2.115 | 0.283 |
| HR at admission | 1.017 | 0.996–1.038 | 0.097 |
| sBP at discharge | 1.022 | 0.989–1.053 | 0.172 |
| MRA at discharge | 0.797 | 0.225–2.871 | 0.725 |
| LVEF | 1.389 | 0.973–1.065 | 0.755 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taruya, A.; Nishiguchi, T.; Ota, S.; Taniguchi, M.; Kashiwagi, M.; Shiono, Y.; Wan, K.; Ino, Y.; Tanaka, A. Low Energy Intake Diagnosed Using the Harris–Benedict Equation Is Associated with Poor Prognosis in Elderly Heart Failure Patients. J. Clin. Med. 2023, 12, 7191. https://doi.org/10.3390/jcm12227191
Taruya A, Nishiguchi T, Ota S, Taniguchi M, Kashiwagi M, Shiono Y, Wan K, Ino Y, Tanaka A. Low Energy Intake Diagnosed Using the Harris–Benedict Equation Is Associated with Poor Prognosis in Elderly Heart Failure Patients. Journal of Clinical Medicine. 2023; 12(22):7191. https://doi.org/10.3390/jcm12227191
Chicago/Turabian StyleTaruya, Akira, Tsuyoshi Nishiguchi, Shingo Ota, Motoki Taniguchi, Manabu Kashiwagi, Yasutsugu Shiono, Ke Wan, Yasushi Ino, and Atsushi Tanaka. 2023. "Low Energy Intake Diagnosed Using the Harris–Benedict Equation Is Associated with Poor Prognosis in Elderly Heart Failure Patients" Journal of Clinical Medicine 12, no. 22: 7191. https://doi.org/10.3390/jcm12227191
APA StyleTaruya, A., Nishiguchi, T., Ota, S., Taniguchi, M., Kashiwagi, M., Shiono, Y., Wan, K., Ino, Y., & Tanaka, A. (2023). Low Energy Intake Diagnosed Using the Harris–Benedict Equation Is Associated with Poor Prognosis in Elderly Heart Failure Patients. Journal of Clinical Medicine, 12(22), 7191. https://doi.org/10.3390/jcm12227191