
«Digesting Crohn’s Disease»: The Journey of Young Adults since Diagnosis

 , ,
, ,
Abstract
:1. Introduction
1.1. Crohn’s Disease
1.2. Crohn’s Disease Psychosocial Outcomes
1.3. The Specific Case of Young Adults with Crohn’s Disease
1.4. Identity Challenges in Young Adults with Crohn’s Disease
2. Method
2.1. Design, Participants and Procedure
2.2. Data Analysis
2.3. Ethical Considerations
3. Results
3.1. Participant Characteristics
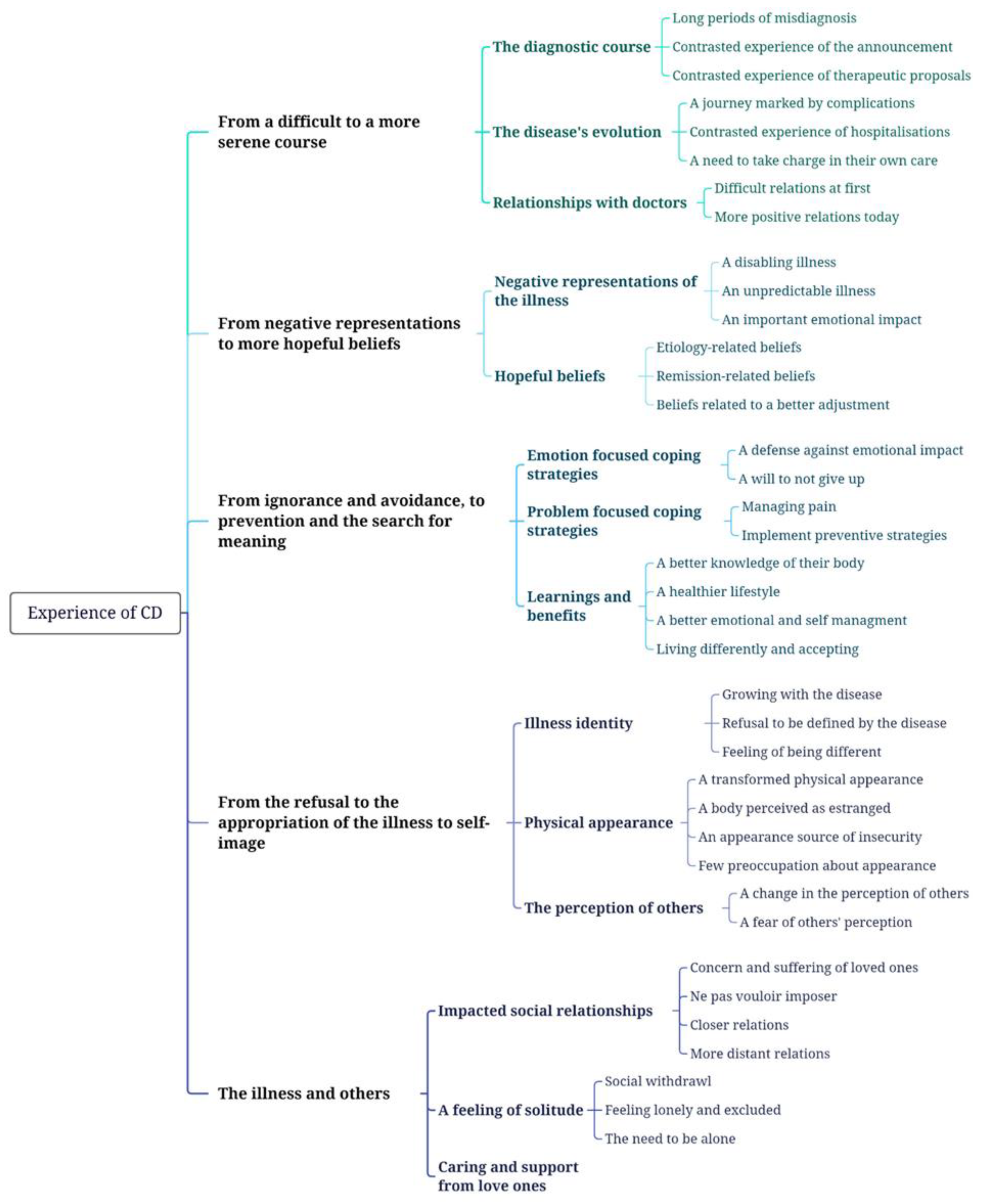
3.2. Thematic Analysis of Major Themes
3.2.1. The Disease Course: From a Difficult Course to a More Serene Pathway
“The first thing I wondered about was the impact it would have later on [...] and whether I was going to die sooner than if I hadn’t had this disease [...] all these worries about death, about the disease getting worse, that was really the first thing that came in mind”(Ms. S, 23 years old)
“It’s the biological, clinical pain of having a complicated disease that alters your quality of life, and it’s also the moral, psychological pain, not to say the trauma, because you are condemned”(Ms. F, 37 years old)
“I was in a state of denial because I was still digesting this disease”(Ms. L, 31 years old)
“It reassured me to know what I had, that it was explainable, that there was a treatment and that I would be OK”(Mr. J, 29 years old)
“I’d been in and out of hospital several times [...] I had to undergo emergency surgery and had 21 cm of intestine removed [...] the intestine was really rotten and sticking to the abdominal wall. After that, I had a lot of problems [...] crisis after crisis, lots of intestinal occlusions. Last year I had maybe 7 intestinal obstructions, and each time I had to stay in hospital for 4–5 days”.(Mr. N, 30 years old)
“The hospital was a gloomy environment, I swear it was very hard because we leave feeling down and completely drained”(Ms. F, 37 years old)
“The doctor who took care of me at the beginning tended to treat me like I was just a “patient file”, I wasn’t a human being”.(Ms. S, 37 years old)
“I have the cell phone number of the Professor, I know I can reach him if I need it […]. I know I can count on the medical staff, so it reassures me”(Ms. J, 28 years old)
3.2.2. Illness Perceptions: From Negative Representations to More Hopeful Beliefs
“I was very tired, even today […]. No matter how much I slept or didn’t sleep, I was tired. So sometimes I don’t want to do anything […]. Fatigue is really like a leitmotif, it’s recurrent. It really bothered me a lot, it’s tiring in fact, it’s something that’s very tiring daily”(Ms. M, 28 years old)
“I couldn’t hold myself, to the point that one day I was about to take the metro and there was a 4–5 min wait and I told myself that I would never make it. So, I got out of the metro and went between two cars. It was very humiliating, even though no one saw me, but I told myself it is not possible I am not capable of holding myself. It lasted for months, it was very complicated to manage personally”(Ms. M, 28 years old)
“The disease changed my relationship with food. I like to drink, I like to eat, I also like to smoke and all the bad good thing in life were taken away from me […]. These were the three things that I would allow myself to escape daily life and to erase this, it was a big constraint”(Ms. S, 37 years old)
“It is heavy when we are young because we want to do a lot of things […] we rather think about having fun, going out, pursuing studies, work and not necessarily live with this disease”(Mr. L, 34 years old)
“It is a recurrent anxiety […] when I had my oral or written exams I used to wonder: what if it doesn’t go well? If I am suddenly in pain, what do I do?”(Ms. F, 37 years old)
“I was able to stabilize the disease by doing several things […] note what I eat, favor raw over cooked foods, cook rather than bye processed meals and of course I quit smoking […] and overall pay more attention to my lifestyle”(Ms. L, 31 years old)
“I know that when I am in a negative phase emotionally, after a traumatizing life-event such as a separation or the loss of someone close, I know that the disease will be more present. I also know I will be more in pain when I am upset or angry, I know it is going to make the disease worse”(Mr. L, 34 years old)
3.2.3. Managing the Disease: From Ignorance and Avoidance to Prevention and the Search for Meaning
“When I was in pain, I took it upon myself. It was the beginning, I was fighting”(Mr. J, 28 years old)
“I had two choices, either I condemned myself to not living and let the disease take over my life, or I took control of the disease and lived. So, in the beginning I preferred to restrict myself to everything, but as time goes by you tell yourself that you’re young, that you’ve got your whole life ahead of you and that you’ve got to get on top of it”(Ms. J, 28 years old)
“When pain is intense, I try to take time to breath […] I focus on the pain to try to reduce it”(Mr. N, 30 years old)
“We try to hold on to the positive inside the negative. I think that it plays an important role, I really think a have a mental strength”(Mr. J, 28 years old)
“I planned everything. For example, in my bag I’d pack toilet paper and wipes. If I went to such and such a place, I’d make sure there was a toilet nearby, or a McDonald’s where I could get to the toilet. In fact, everything was planned, every outing was planned”(Ms. J, 28 years old)
“Even if this illness was complicated to manage, it brought me a lot of positive things […]. I am realizing that since this illness I seen life differently […] I live every moment more intensely”(Ms. C, 25 years old)
3.2.4. Illness Identity: From Refusal to the Appropriation of the Disease to Self-Image
“The illness came at a moment when adolescence is taking place, when puberty is taking place, so I had a hard time with that”(Mr. K, 26 years old)
“Many people told me to ask for the disabled status, but psychologically I couldn’t do it. I tell myself I am not disabled. In addition, it is a status you keep for life, you cannot one day no longer be disabled. I tell myself that one day I will no longer have this disease”(Ms. C, 25 years old)
“Before I was a very lively person, but then I felt transformed, I was like a dragon, nobody could talk to me”(Ms. S, 37 years old)
“Yes, I was skeletal, and I was hunched over because of the operation, because of the scar, I had trouble straightening up. So yes, it was weird to see myself like that and it was hard to accept. When I saw myself, I didn’t recognize myself anymore”(Mr. N, 30 years old)
“I was afraid that no one would accept it, that people would think I was sick. I was really afraid it would be repulsive”.(Ms. J, 28 years old)
“Illness is not our whole life, it’s a painful part of it, but it’s not our whole life at all”.(Ms. S, 23 years old)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Observatoire National des MICI. Les MICI en 2019 Dans l’ALD24 (Infographie). 2019. Available online: http://www.observatoire-crohn-rch.fr/les-mici-en-france/ (accessed on 1 October 2023).
- Hart, A.; Ng, S. Crohn’s Disease. Inflamm. Bowel Dis. 2015, 43, 282–290. [Google Scholar] [CrossRef]
- Torres, J.; Mehandru, S.; Colombel, J.-F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Peyrin-Biroulet, L. Histoire naturelle de la maladie de Crohn. In Post’U FMC-HGE; Springer: Paris, France, 2011. [Google Scholar] [CrossRef]
- Aoun, N. Maladie de Crohn: Compréhension de la Pathologie et Présentation des Différents Aspects de sa Prise en Charge à L’officine. Ph.D. Thesis, Université de Bordeaux, Bordeaux, France, 2019. Available online: https://dumas.ccsd.cnrs.fr/dumas-02100360/document (accessed on 1 October 2023).
- Pamart-Bera, C. La Maladie de Crohn Pédiatrique: Spécificités et Prise en Charge. Ph.D. Thesis, Université de Lille, Lille, France, 2017. Available online: https://pepite-depot.univ-lille.fr/LIBRE/Th_Pharma/2017/2017LIL2E067.pdf (accessed on 1 October 2023).
- Reenaers, C. Maladie de Crohn minime à modérée: Comment la définir, quelles stratégies? In Proceedings of the Journées Francophones D’HEPATO-Gastroentérologie & D’oncologie Digestives, Paris, France, 19–22 March 2015; Available online: https://www.fmcgastro.org/wp-content/uploads/file//ppt-2015/c-reenaers.pdf (accessed on 1 October 2023).
- Brandi, M.T.; Ribeiro, M.S.; Chebli, L.A.; Franco, M.B.; Pinto, A.L.; Gaburri, P.D.; Zanini, A.; Chebli, J.M. Psychological distress in Brazilian Crohn’s disease patients: Screening, prevalence, and risk factors. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2009, 15, PH101–PH108. [Google Scholar]
- Iglesias, M.; Barreiro de Acosta, M.; Vázquez, I.; Figueiras, A.; Nieto, L.; Lorenzo, A.; Domínguez-Muñoz, J.E. Impacto psicológico de la enfermedad de Crohn en pacientes en remisión: Riesgo de ansiedad y depresión. Rev. Española Enfermedades Dig. 2009, 101, 249–257. [Google Scholar] [CrossRef]
- Larussa, T.; Flauti, D.; Abenavoli, L.; Boccuto, L.; Suraci, E.; Marasco, R.; Imeneo, M.; Luzza, F. The Reality of Patient-Reported Outcomes of Health-Related Quality of Life in an Italian Cohort of Patients with Inflammatory Bowel Disease: Results from a Cross-Sectional Study. J. Clin. Med. 2020, 9, 2416. [Google Scholar] [CrossRef]
- Luo, X.; Mao, R.; Chen, B.; Qiu, Y.; Zhang, S.; He, Y.; Chen, J.; Zeng, Z.; Ben-Horin, S.; Chen, M. Over-reaching beyond disease activity: The influence of anxiety and medical economic burden on health-related quality of life in patients with inflammatory bowel disease. Patient Prefer. Adherence 2016, 11, 23–31. [Google Scholar] [CrossRef]
- Mikocka-Walus, A.; Massuger, W.; Knowles, S.R.; Moore, G.T.; Buckton, S.; Connell, W.; Pavli, P.; Raven, L.; Andrews, J.M. Psychological distress is highly prevalent in inflammatory bowel disease: A survey of psychological needs and attitudes. JGH Open 2020, 4, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Garcia Calvo, E.; Dura Gil, M.; Velayos Jimenez, B.; Fernández Salazar, L. Prevalence and factors associated with poor sleep quality in inflammatory bowel disease outpatients. Rev. Española Enfermedades Dig. 2020, 113, 512–518. [Google Scholar] [CrossRef]
- Magro, F.; Portela, F.; Lago, P.; Deus, J.; Cotter, J.; Cremers, I.; Vieira, A.; Peixe, P.; Caldeira, P.; Lopes, H.; et al. Inflammatory Bowel Disease: A Patient’s and Caregiver’s Perspective. Dig. Dis. Sci. 2009, 54, 2671–2679. [Google Scholar] [CrossRef]
- Parra, R.S.; Chebli, J.M.; Amarante, H.M.; Flores, C.; Parente, J.M.; Ramos, O.; Fernandes, M.; Rocha, J.J.; Feitosa, M.R.; Feres, O.; et al. Quality of life, work productivity impairment and healthcare resources in inflammatory bowel diseases in Brazil. World J. Gastroenterol. 2019, 25, 5862–5882. [Google Scholar] [CrossRef]
- Devlen, J.; Beusterien, K.; Yen, L.; Ahmed, A.; Cheifetz, A.S.; Moss, A.C. The Burden of Inflammatory Bowel Disease: A Patient-Reported Qualitative Analysis and Development of a Conceptual Model. Inflamm. Bowel Dis. 2014, 20, 545–552. [Google Scholar] [CrossRef]
- Purc-Stephenson, R.; Bowlby, D.; Qaqish, S.T. “A gift wrapped in barbed wire” Positive and negative life changes after being diagnosed with inflammatory bowel disease. Qual. Life Res. 2015, 24, 1197–1205. [Google Scholar] [CrossRef] [PubMed]
- Williams-Hall, R.; Trennery, C.; Sully, K.; Wratten, S.; Francis, A.; Chandler, D.; Flynn, J.; Turner, M.; Marks, D.J.B.; Sackeyfio, A.; et al. A qualitative study to explore the symptoms and impacts of Crohn’s disease and to develop the Crohn’s Disease Diary. Qual. Life Res. 2022, 32, 209–223. [Google Scholar] [CrossRef]
- Matini, L.; Ogden, J. A qualitative study of patients’ experience of living with inflammatory bowel disease: A preliminary focus on the notion of adaptation. J. Health Psychol. 2016, 21, 2493–2502. [Google Scholar] [CrossRef]
- Mikocka-Walus, A.; Hanlon, I.; Dober, M.; Emerson, C.; Beswick, L.; Selinger, C.; Taylor, J.; Olive, L.; Evans, S.; Hewitt, C. Lived experience in people with inflammatory bowel disease and comorbid anxiety and depression in the United Kingdom and Australia. J. Health Psychol. 2021, 26, 2290–2303. [Google Scholar] [CrossRef] [PubMed]
- Robertson, N.; Gunn, S.; Piper, R. The Experience of Self-Conscious Emotions in Inflammatory Bowel Disease: A Thematic Analysis. J. Clin. Psychol. Med. Settings 2022, 29, 344–356. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, B.J.; Sirois, F.M. Beyond standard quality of life measures: The subjective experiences of living with inflammatory bowel disease. Qual. Life Res. 2008, 17, 877–886. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Arnett, J.J. Emerging Adulthood: The Winding Road from the Late Teens through the Twenties, 2nd ed.; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- Kunnen, S.-E.; Bosma, H.-A. Le développement de l’identité: Un processus relationnel et dynamique. L’orientation Sc. Prof. 2006, 35, 183–203. [Google Scholar] [CrossRef]
- Acciari, A.S.; Leal, R.F.; Coy, C.S.R.; Dias, C.C.; Ayrizono, M.D.L.S. Relationship among psychological well-being, resilience and coping with social and clinical features in Crohn’s disease patients. Arq. Gastroenterol. 2019, 56, 131–140. [Google Scholar] [CrossRef]
- Freitas, T.H.; Hyphantis, T.N.; Andreoulakis, E.; Quevedo, J.; Miranda, H.L.; Alves, G.S.; Souza, M.H.; Braga, L.L.; Pargament, K.I.; Soczynska, J.K.; et al. Religious coping and its influence on psychological distress, medication adherence, and quality of life in inflammatory bowel disease. Braz. J. Psychiatry 2015, 37, 219–227. [Google Scholar] [CrossRef]
- Sarid, O.; Slonim-Nevo, V.; Pereg, A.; Friger, M.; Sergienko, R.; Schwartz, D.; Greenberg, D.; Shahar, I.; Chernin, E.; Vardi, H.; et al. Coping strategies, satisfaction with life, and quality of life in Crohn’s disease: A gender perspective using structural equation modeling analysis. PLoS ONE 2017, 12, e0172779. [Google Scholar] [CrossRef]
- Muse, K.; Johnson, E.; David, A.L. A feeling of otherness: A qualitative research synthesis exploring the lived experiences of stigma in individuals with inflammatory bowel disease. Int. J. Environ. Res. Public Health 2021, 18, 8038. [Google Scholar] [CrossRef]
- Wu, Q.; Zhu, P.; Liu, X.; Ji, Q.; Qian, M. Nirvana: A Qualitative Study of Posttraumatic Growth in Adolescents and Young Adults with Inflammatory Bowel Disease. Children 2022, 9, 879. [Google Scholar] [CrossRef] [PubMed]
- Paillé, P.; Mucchielli, A. L’analyse Qualitative en Sciences Humaines et Sociales; Armand Colin: Pays de la Loire, France, 2021. [Google Scholar]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide [eBook Version]; SAGE: Thousand Oaks, CA, USA, 2021. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef] [PubMed]
- Leventhal, H.; Diefenbach, M.; Leventhal, E.A. Illness cognition: Using common sense to understand treatment adherence and affect cognition interactions. Cogn. Ther. Res. 1992, 16, 143–163. [Google Scholar] [CrossRef]
- Fischer, G.; Tarquinio, C.; Dodeler, V. Chapitre 4. Adaptation et coping. In Dans Les Bases de la Psychologie de la Santé: Concepts, Applications et Perspectives; Fischer, G., Tarquinio, C., Dodeler (Dir), V., Eds.; Dunod: Paris, France, 2020; pp. 103–141. [Google Scholar] [CrossRef]
- Lechner, S.; Stoelb, B.; et Antonin, M. Group based therapies for benefit finding in cancer. In Trauma, Recovery, and Growth: Positive Psychological Perspectives on Post-Traumatic Stress; Jospeh, S., Linley, A., Eds.; Wiley: Hoboken, NJ, USA, 2008. [Google Scholar]
- Bungener, C. Les troubles psychopathologiques et les mécanismes adaptatifs dans la sclérose latérale amyotrophique. Prat. Psychol. 2005, 11, 319–328. [Google Scholar] [CrossRef]
- Untas, A., II. L’ajustement à la maladie. In Dans Psychologie de la Santé; Sultan, S., Ed.; Presses Universitaires de France: Paris, France, 2012; pp. 41–66. [Google Scholar] [CrossRef]
- Oris, L.; Rassart, J.; Prikken, S.; Verschueren, M.; Goubert, L.; Moons, P.; Berg, C.A.; Weets, I.; Luyckx, K. Illness Identity in Adolescents and Emerging Adults with Type 1 Diabetes: Introducing the Illness Identity Questionnaire. Diabetes Care 2016, 39, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Oris, L.; Luyckx, K.; Rassart, J.; Goubert, L.; Goossens, E.; Apers, S.; Arat, S.; Vandenberghe, J.; Westhovens, R.; Moons, P. Illness Identity in Adults with a Chronic Illness. J. Clin. Psychol. Med. Settings 2018, 25, 429–440. [Google Scholar] [CrossRef]
- Kamp, K.J.; West, P.; Holmstrom, A.; Luo, Z.; Wyatt, G.; Given, B. Systematic Review of Social Support on Psychological Symptoms and Self-Management Behaviors among Adults with Inflammatory Bowel Disease. J. Nurs. Scholarsh. 2019, 51, 380–389. [Google Scholar] [CrossRef]
- Lainé, A. Vécu Subjectif de la Maladie de Crohn et Facteurs Psychosociaux Prédictifs de la Rechute: Vers une Approche Intégrative. Ph.D. Thesis, Université Bourgogne Franche-Compté, Besançon, France, 2017. [Google Scholar]
- McCombie, A.M.; Mulder, R.T.; Gearry, R.B. How IBD patients cope with IBD: A systematic review. J. Crohn’s Colitis 2013, 7, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Polak, E.-J.; O’Callaghan, F.; Oaten, M. Perceptions of IBD within patient and community samples: A systematic review. Psychol. Health 2020, 35, 425–448. [Google Scholar] [CrossRef] [PubMed]
- Ewais, T.; Begun, J.; Kenny, M.; Rickett, K.; Hay, K.; Ajilchi, B.; Kisely, S. A systematic review and meta-analysis of mindfulness based interventions and yoga in inflammatory bowel disease. J. Psychosom. Res. 2019, 116, 44–53. [Google Scholar] [CrossRef]
- Lavelle, J.; Storan, D.; Eswara Murthy, V.; De Dominicis, N.; Mulcahy, H.E.; McHugh, L. Brief and Telehealth Acceptance and Commitment Therapy (ACT) Interventions for Stress in Inflammatory Bowel Disease (IBD): A Series of Single Case Experimental Design (SCED) Studies. J. Clin. Med. 2022, 11, 2757. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| General Question |
| Can you tell me about your experience of being diagnosed with Crohn’s disease as a young person? |
| Addressed topics |
| What the disease has changed Difficulties or concerns caused by the disease Strategies for coping with illness/symptoms Body/self-image Family relations Friendships Couple/sexual relationships Academic/professional sphere |
| ID | Age | Sex | Marital Status | Latest Degree | Professional Status | Age at 1st Symptoms | Age at Diagnostic | Reported Disease State | Interview Duration |
|---|---|---|---|---|---|---|---|---|---|
| P1 | 31 | F | Single | BTEC | Self-employed | 25 | 26 | Remission | 60 |
| P2 | 29 | M | Single | Bachelor | Employee | 14 | 15 | Stabilized | 46 |
| P3 | 28 | M | Relationship | Master’s | Employee | 16 | 16 | Stabilized | 49 |
| P4 | 28 | F | Married | Master’s | Employee | 17 | 17 | Stabilized | 47 |
| P5 | 26 | M | Single | Master’s | Employee | 15 | 17 | Stabilized | 75 |
| P6 | 30 | M | Married | BTEC | Employee | 11 | 14 | Stabilized | 60 |
| P7 | 28 | F | Married | Bachelor | Employee | 18 | 18 | Stabilized | 43 |
| P9 | 20 | F | Single | A levels | Student | 18 | 18 | Stabilized | 59 |
| P11 | 25 | F | Relationship | Master’s | Unemployed | 18 | 18 | Stabilized | 41 |
| P15 | 37 | F | Relationship | BTEC | Self-employed | 16 | 24 | Stabilized | 47 |
| P16 | 37 | F | Relationship | PhD | Self-employed | 18 | 19 | Remission | 66 |
| P18 | 24 | F | Relationship | Master’s | Employee | 17 | 17 | Stabilized | 63 |
| P22 | 25 | F | Relationship | A levels | Self-employed | 20 | 21 | Stabilized | 61 |
| P24 | 34 | M | Relationship | A levels | Self-employed | 32 | 33 | Stabilized | 23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Touma, N.; Zanni, L.; Blanc, P.; Savoye, G.; Baeza-Velasco, C. «Digesting Crohn’s Disease»: The Journey of Young Adults since Diagnosis. J. Clin. Med. 2023, 12, 7128. https://doi.org/10.3390/jcm12227128
Touma N, Zanni L, Blanc P, Savoye G, Baeza-Velasco C. «Digesting Crohn’s Disease»: The Journey of Young Adults since Diagnosis. Journal of Clinical Medicine. 2023; 12(22):7128. https://doi.org/10.3390/jcm12227128
Chicago/Turabian StyleTouma, Nathalie, Louise Zanni, Pierre Blanc, Guillaume Savoye, and Carolina Baeza-Velasco. 2023. "«Digesting Crohn’s Disease»: The Journey of Young Adults since Diagnosis" Journal of Clinical Medicine 12, no. 22: 7128. https://doi.org/10.3390/jcm12227128
APA StyleTouma, N., Zanni, L., Blanc, P., Savoye, G., & Baeza-Velasco, C. (2023). «Digesting Crohn’s Disease»: The Journey of Young Adults since Diagnosis. Journal of Clinical Medicine, 12(22), 7128. https://doi.org/10.3390/jcm12227128