

Spontaneous Cultural Conversion Rate of Mycobacterium avium Complex Pulmonary Disease Based on BACES Severity


Abstract
:1. Introduction
2. Methods
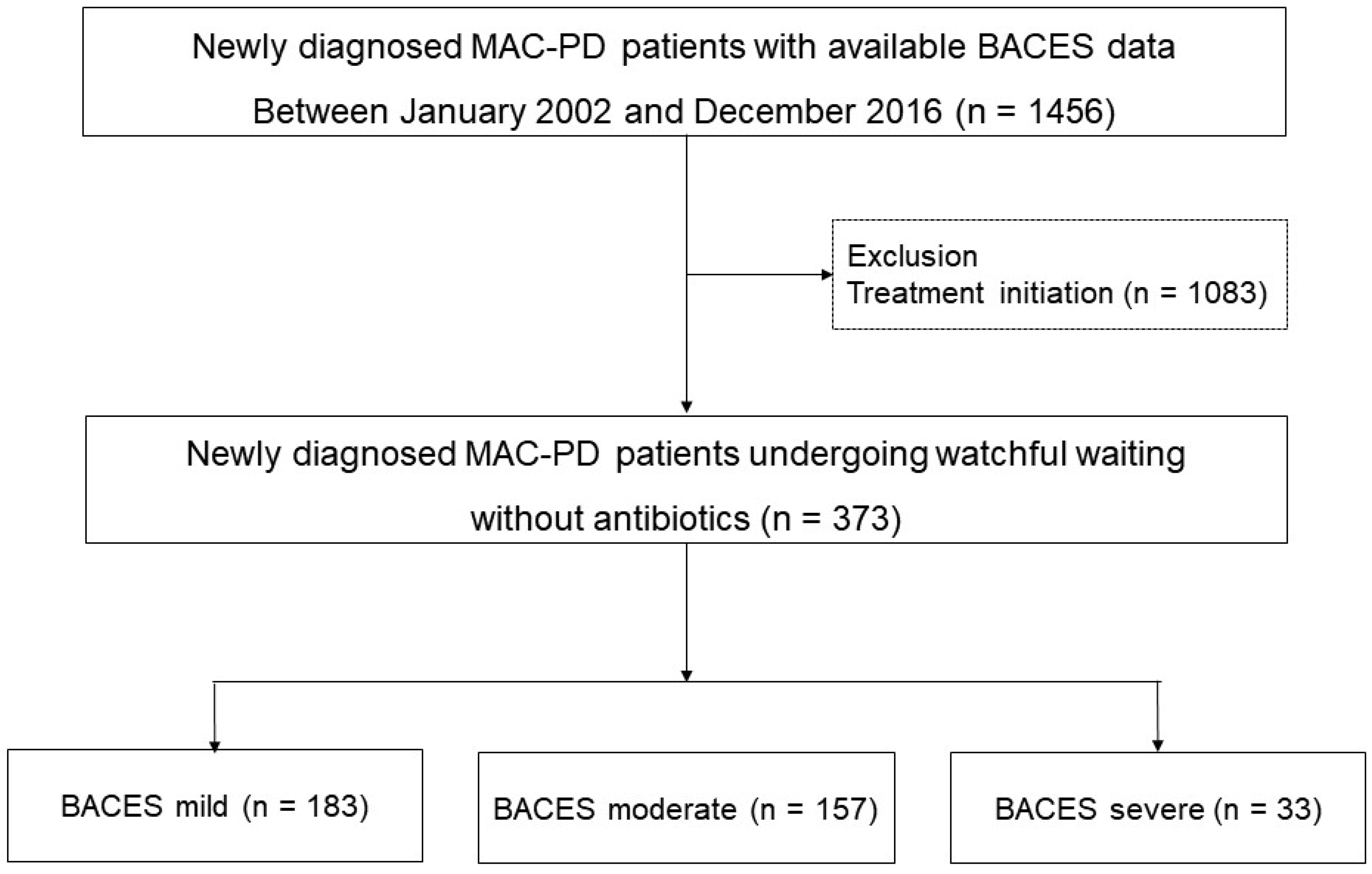
2.1. Study Design and Population
2.2. Evaluation of BACES Severity
2.3. Sputum and Radiological Examinations
2.4. Evaluation of Microbiological Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Study Patients
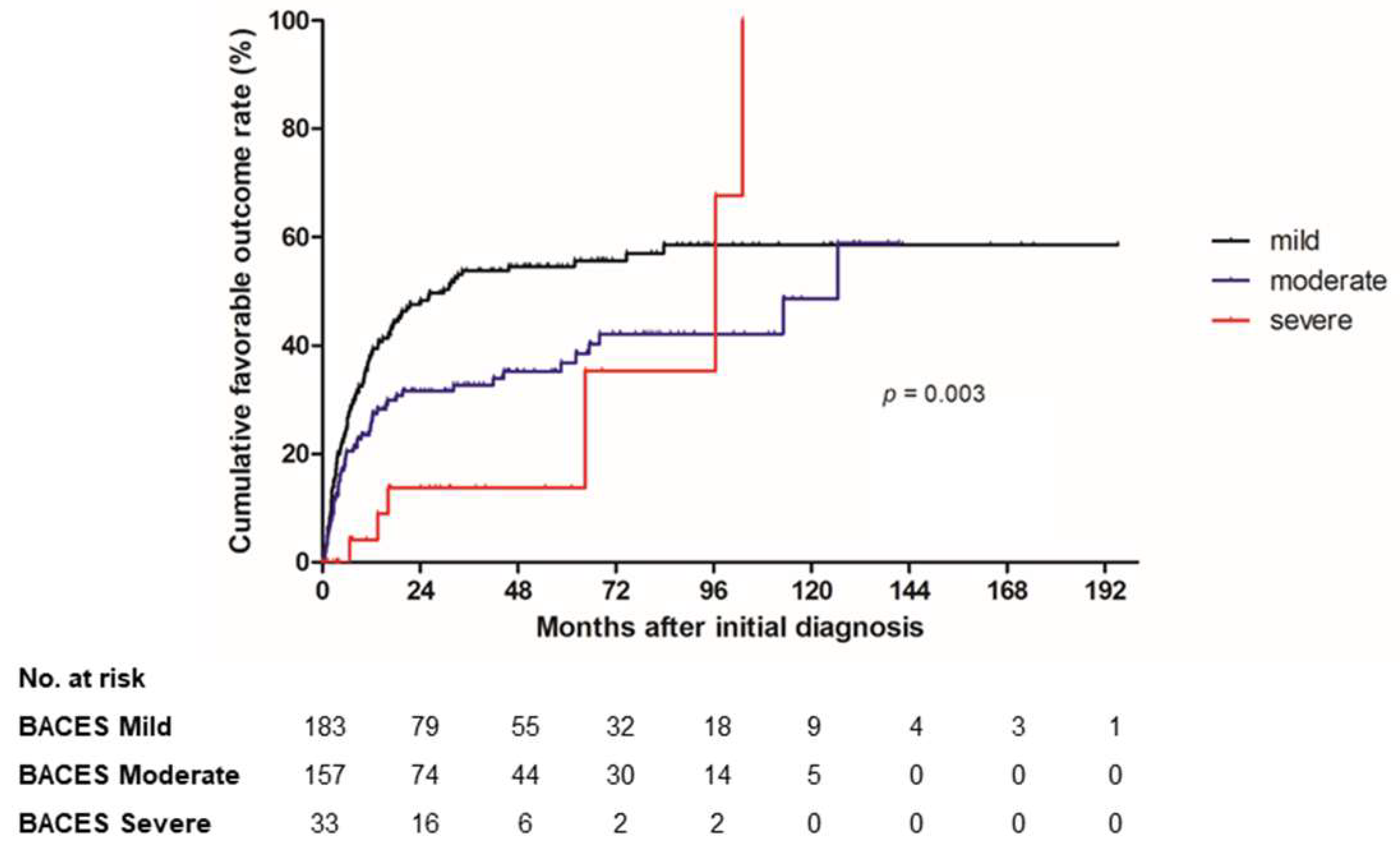
3.2. Microbiological Outcomes in Patients without Antibiotic Treatment
3.3. Factors Associated with the Microbiological Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, H.; Myung, W.; Koh, W.J.; Moon, S.M.; Jhun, B.W. Epidemiology of nontuberculous mycobacterial infection, South Korea, 2007–2016. Emerg. Infect. Dis. 2019, 25, 569–572. [Google Scholar] [CrossRef]
- Griffith, D.E.; Aksamit, T.; Brown-Elliott, B.A.; Catanzaro, A.; Daley, C.; Gordin, F.; Holland, S.M.; Horsburgh, R.; Huitt, G.; Iademarco, M.F.; et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 2007, 175, 367–416. [Google Scholar] [CrossRef]
- Daley, C.L.; Iaccarino, J.M.; Lange, C.; Cambau, E.; Wallace, R.J., Jr.; Andrejak, C.; Böttger, E.C.; Brozek, J.; Griffith, D.E.; Guglielmetti, L.; et al. Treatment of nontuberculous mycobacterial pulmonary disease: An official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur. Respir. J. 2020, 56, 2000535. [Google Scholar] [CrossRef] [PubMed]
- Haworth, C.S.; Banks, J.; Capstick, T.; Fisher, A.J.; Gorsuch, T.; Laurenson, I.F.; Leitch, A.; Loebinger, M.R.; Milburn, H.J.; Nightingale, M.; et al. British Thoracic Society guidelines for the management of non-tuberculous mycobacterial pulmonary disease (NTM-PD). Thorax 2017, 72, ii1–ii64. [Google Scholar] [CrossRef] [PubMed]
- Pasipanodya, J.G.; Ogbonna, D.; Deshpande, D.; Srivastava, S.; Gumbo, T. Meta-analyses and the evidence base for microbial outcomes in the treatment of pulmonary Mycobacterium avium-intracellulare complex disease. J. Antimicrob. Chemother. 2017, 72, i3–i19. [Google Scholar] [CrossRef]
- Hwang, J.A.; Kim, S.; Jo, K.W.; Shim, T.S. Natural history of Mycobacterium avium complex lung disease in untreated patients with stable course. Eur. Respir. J. 2017, 49, 1600537. [Google Scholar] [CrossRef]
- Moon, S.M.; Jhun, B.W.; Baek, S.Y.; Kim, S.; Jeon, K.; Ko, R.E.; Shin, S.H.; Lee, H.; Kwon, O.J.; Huh, H.J.; et al. Long-term natural history of non-cavitary nodular bronchiectatic nontuberculous mycobacterial pulmonary disease. Respir. Med. 2019, 151, 1–7. [Google Scholar] [CrossRef]
- Kwon, B.S.; Lee, J.H.; Koh, Y.; Kim, W.S.; Song, J.W.; Oh, Y.M.; Lee, S.D.; Lee, S.W.; Lee, J.S.; Lim, C.M.; et al. The natural history of non-cavitary nodular bronchiectatic Mycobacterium avium complex lung disease. Respir. Med. 2019, 150, 45–50. [Google Scholar] [CrossRef]
- Kim, H.J.; Kwak, N.; Hong, H.; Kang, N.; Im, Y.; Jhun, B.W.; Yim, J.J. BACES score for predicting mortality in nontuberculous mycobacterial pulmonary disease. Am. J. Respir. Crit. Care Med. 2021, 203, 230–236. [Google Scholar] [CrossRef]
- Kim, H.J.; Song, M.J.; Kwon, B.S.; Kim, Y.W.; Lim, S.Y.; Lee, Y.J.; Park, J.S.; Cho, Y.J.; Lee, C.T.; Lee, J.H. Usefulness of the BACES score in nontuberculous mycobacterial pulmonary disease for various clinical outcomes. Sci. Rep. 2023, 13, 7495. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.G.; Jhun, B.W.; Kim, H.; Kwon, O.J. Treatment outcomes of Mycobacterium avium complex pulmonary disease according to disease severity. Sci. Rep. 2022, 12, 1970. [Google Scholar] [CrossRef] [PubMed]
- Jhun, B.W.; Moon, S.M.; Jeon, K.; Kwon, O.J.; Yoo, H.; Carriere, K.C.; Huh, H.J.; Lee, N.Y.; Shin, S.J.; Daley, C.L.; et al. Prognostic factors associated with long-term mortality in 1445 patients with nontuberculous mycobacterial pulmonary disease: A 15-year follow-up study. Eur. Respir. J. 2020, 55, 1900798. [Google Scholar] [CrossRef] [PubMed]
- Jhun, B.W.; Kim, S.Y.; Moon, S.M.; Jeon, K.; Kwon, O.J.; Huh, H.J.; Ki, C.S.; Lee, N.Y.; Shin, S.J.; Daley, C.L.; et al. Development of macrolide resistance and reinfection in refractory Mycobacterium avium complex lung disease. Am. J. Respir. Crit. Care Med. 2018, 198, 1322–1330. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Jhun, B.W.; Kim, J.; Huh, H.J.; Lee, N.Y. Clinical characteristics and outcomes of surgically resected solitary pulmonary nodules due to nontuberculous mycobacterial Infections. J. Clin. Med. 2019, 8, 1898. [Google Scholar] [CrossRef]
- van Ingen, J.; Aksamit, T.; Andrejak, C.; Böttger, E.C.; Cambau, E.; Daley, C.L.; Griffith, D.E.; Guglielmetti, L.; Holland, S.M.; Huitt, G.A.; et al. Treatment outcome definitions in nontuberculous mycobacterial pulmonary disease: An NTM-NET consensus statement. Eur. Respir. J. 2018, 51, 1800170. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.W.; Shu, C.C.; Feng, J.Y.; Wang, J.Y.; Chan, Y.J.; Yu, C.J.; Su, W.J. Microbiological persistence in patients with Mycobacterium avium complex lung disease: The predictors and the impact on radiographic progression. Clin. Infect. Dis. 2017, 65, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Prieto, M.D.; Jang, J.; Franciosi, A.N.; Av-Gay, Y.; Bach, H.; Tebbutt, S.J.; Quon, B.S. Whole blood RNA-seq demonstrates an increased host immune response in individuals with cystic fibrosis who develop nontuberculous mycobacterial pulmonary disease. PLoS ONE 2022, 17, e0278296. [Google Scholar] [CrossRef]
- Hull, R.C.; Huang, J.T.J.; Barton, A.K.; Keir, H.R.; Ellis, H.; Cookson, W.O.C.; Moffatt, M.F.; Loebinger, M.R.; Chalmers, J.D. Sputum proteomics in nontuberculous mycobacterial lung disease. Chest 2022, 161, 1180–1191. [Google Scholar] [CrossRef]
- Pan, S.W.; Su, W.J.; Chan, Y.J.; Ho, M.L.; Feng, J.Y.; Shu, C.C.; Wang, J.Y.; Wang, H.C.; Yu, C.J.; Chen, Y.M. Disease progression in patients with nontuberculous mycobacterial lung disease of nodular bronchiectatic (NB) pattern: The roles of cavitary NB and soluble programmed death protein-1. Clin. Infect. Dis. 2022, 75, 239–247. [Google Scholar] [CrossRef]
- Jeon, D. Infection source and epidemiology of nontuberculous mycobacterial lung disease. Tuberc. Respir. Dis. 2019, 82, 94–101. [Google Scholar] [CrossRef]
- Park, Y.; Kwak, S.H.; Yong, S.H.; Lee, S.H.; Leem, A.Y.; Kim, S.Y.; Lee, S.H.; Chung, K.; Kim, E.Y.; Jung, J.Y.; et al. The association between behavioral risk factors and nontuberculous mycobacterial pulmonary disease. Yonsei Med. J. 2021, 62, 702–707. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Goeminne, P.; Aliberti, S.; McDonnell, M.J.; Lonni, S.; Davidson, J.; Poppelwell, L.; Salih, W.; Pesci, A.; Dupont, L.J.; et al. The bronchiectasis severity index. An international derivation and validation study. Am. J. Respir. Crit. Care Med. 2014, 189, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Martínez-García, M.; de Gracia, J.; Vendrell Relat, M.; Girón, R.M.; Máiz Carro, L.; de la Rosa Carrillo, D.; Olveira, C. Multidimensional approach to non-cystic fibrosis bronchiectasis: The FACED score. Eur. Respir. J. 2014, 43, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Garcia, M.A.; Athanazio, R.A.; Girón, R.; Máiz-Carro, L.; de la Rosa, D.; Olveira, C.; de Gracia, J.; Vendrell, M.; Prados-Sánchez, C.; Gramblicka, G.; et al. Predicting high risk of exacerbations in bronchiectasis: The E-FACED score. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Henriette Zweijpfenning, S.M.; Chiron, R.; Essink, S.; Schildkraut, J.; Akkerman, O.W.; Aliberti, S.; Altenburg, J.; Arets, B.; Van Braeckel, E.; Delaere, B.; et al. Safety and outcomes of amikacin liposome inhalation suspension for Mycobacterium abscessus pulmonary disease: A NTM-NET. Chest 2022, 162, 76–81. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total (n = 373) | Spontaneous Negative Culture Conversion (n = 153) | No Culture Conversion (n = 220) | p-Value |
|---|---|---|---|---|
| BACES items | ||||
| BMI < 18.5 kg/m2 | 73 (20) | 30 (20) | 43 (20) | 0.988 |
| Age ≥ 65 years | 153 (41) | 47 (31) | 106 (48) | 0.001 |
| Cavity | 36 (10) | 9 (6) | 27 (12) | 0.040 |
| Elevated ESR * | 234 (63) | 96 (63) | 138 (63) | 0.997 |
| Sex, male | 145 (39) | 56 (37) | 89 (41) | 0.453 |
| Ex- or current smoker | 98 (26) | 113 (74) | 161 (73) | 0.885 |
| Underlying condition | ||||
| Previous tuberculosis | 103 (28) | 43 (28) | 60 (27) | 0.860 |
| Chronic obstructive pulmonary disease | 24 (6) | 16 (11) | 8 (4) | 0.008 |
| Chronic pulmonary aspergillosis | 2 (1) | - | - | 0.515 |
| Lung cancer | 18 (5) | 6 (4) | 12 (6) | 0.497 |
| Symptoms | ||||
| Cough | 230 (62) | 99 (65) | 131 (60) | 0.313 |
| Sputum | 227 (61) | 94 (61) | 133 (61) | 0.848 |
| Hemoptysis | 63 (17) | 28 (18) | 35 (16) | 0.544 |
| Weight loss | 17 (5) | 4 (3) | 13 (6) | |
| Positive sputum AFB smear | 122 (33) | 40 (26) | 82 (37) | 0.024 |
| Etiology | 0.081 | |||
| M. avium | 229 (61) | 102 (67) | 127 (58) | |
| M. intracellulare | 144 (39) | 51 (33) | 93 (42) | |
| Radiological phenotype | 0.096 | |||
| Nodular bronchiectatic form | 353 (94) | 147 (96) | 206 (94) | |
| Fibrocavitary form | 20 (5) | 6 (4) | 14 (6) |
| Watchful Waiting | Total (n = 373) | Mild (n = 183) | Moderate (n = 157) | Severe (n = 33) | p-Value | p-Trend † |
|---|---|---|---|---|---|---|
| Spontaneous negative culture conversion | 153 (41) | 87/183 (48) | 58/157 (37) | 8/33 (24) | 0.017 ac | 0.005 |
| Time to culture conversion, months | 6.2 (2.7–17.7) | 6.0 (2.2–16.1) | 5.4 (2.8–17.2) | 22.1 (14.2–88.5) | 0.008 bc | 0.037 |
| Favorable outcome * | 157 (42) | 97/183 (53) | 54/157 (34) | 6/33 (18) | <0.001 ac | <0.001 |
| Time to favorable outcome, months | 6.2 (2.5–15.8) | 6.2 (2.3–14.3) | 5.4 (2.5–14.0) | 40.3 (11.8–98.2) | 0.022 bc | 0.346 |
| Variables | Univariable Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| Unadjusted HR (95% CI) | p-Value | Adjusted HR (95% CI) | p-Value | |
| Spontaneous negative culture conversion | ||||
| Ex- or current smoker | 0.85 (0.59–1.22) | 0.388 | 0.99 (0.66–1.49) | 0.971 |
| Underlying condition | ||||
| Previous pulmonary tuberculosis | 1.02 (0.72–1.46) | 0.901 | 1.12 (0.77–1.62) | 0.556 |
| Chronic obstructive pulmonary disease | 1.54 (0.91–2.58) | 0.106 | 1.76 (1.02–3.05) | 0.043 |
| Lung cancer | 0.92 (0.40–2.07) | 0.915 | 0.89 (0.38–2.08) | 0.792 |
| Etiology | ||||
| M. avium | Reference | Reference | ||
| M. intracellulare | 0.83 (0.60–1.17) | 0.287 | 0.83 (0.59–1.17) | 0.295 |
| BACES severity | ||||
| Mild | Reference | Reference | ||
| Moderate | 0.75 (0.54–1.05) | 0.093 | 0.74 (0.52–1.07) | 0.106 |
| Severe | 0.53 (0.26–1.10) | 0.089 | 0.49 (0.22–1.08) | 0.076 |
| Positive sputum AFB smear at diagnosis | 0.68 (0.47–0.97) | 0.034 | 0.70 (0.48–1.01) | 0.057 |
| Favorable outcome * | ||||
| Ex- or current smoker | 0.77 (0.53–1.12) | 0.167 | 1.04 (0.69–1.57) | 0.861 |
| Underlying condition | ||||
| Previous pulmonary tuberculosis | 0.83 (0.58–1.19) | 0.313 | 0.95 (0.65–1.38) | 0.767 |
| Chronic obstructive pulmonary disease | 1.11 (0.63–1.95) | 0.728 | 1.35 (0.75–2.44) | 0.317 |
| Lung cancer | 0.89 (0.40–2.02) | 0.785 | 1.01 (0.44–2.33) | 0.982 |
| Etiology | ||||
| M. avium | Reference | Reference | ||
| M. intracellulare | 0.67 (0.48–0.94) | 0.021 | 0.67 (0.47–0.94) | 0.020 |
| BACES severity | ||||
| Mild | Reference | Reference | ||
| Moderate | 0.63 (0.45–0.88) | 0.007 | 0.63 (0.44–0.91) | 0.013 |
| Severe | 0.37 (0.16–0.84) | 0.017 | 0.37 (0.16–0.90) | 0.028 |
| Positive sputum AFB smear | 0.79 (0.55–1.12) | 0.787 | 0.84 (0.59–1.20) | 0.333 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.-G.; Yu, J.Y.; Jhun, B.W. Spontaneous Cultural Conversion Rate of Mycobacterium avium Complex Pulmonary Disease Based on BACES Severity. J. Clin. Med. 2023, 12, 7125. https://doi.org/10.3390/jcm12227125
Kim B-G, Yu JY, Jhun BW. Spontaneous Cultural Conversion Rate of Mycobacterium avium Complex Pulmonary Disease Based on BACES Severity. Journal of Clinical Medicine. 2023; 12(22):7125. https://doi.org/10.3390/jcm12227125
Chicago/Turabian StyleKim, Bo-Guen, Jin Young Yu, and Byung Woo Jhun. 2023. "Spontaneous Cultural Conversion Rate of Mycobacterium avium Complex Pulmonary Disease Based on BACES Severity" Journal of Clinical Medicine 12, no. 22: 7125. https://doi.org/10.3390/jcm12227125
APA StyleKim, B.-G., Yu, J. Y., & Jhun, B. W. (2023). Spontaneous Cultural Conversion Rate of Mycobacterium avium Complex Pulmonary Disease Based on BACES Severity. Journal of Clinical Medicine, 12(22), 7125. https://doi.org/10.3390/jcm12227125