
Asthma Is Associated with Back Pain and Migraine—Results of Population-Based Case–Control Study


 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Study Population and Matching Method
2.3. Study Variables
2.4. Statistical Analysis
2.5. Sensitivity Analysis
2.6. Ethical Considerations
3. Results
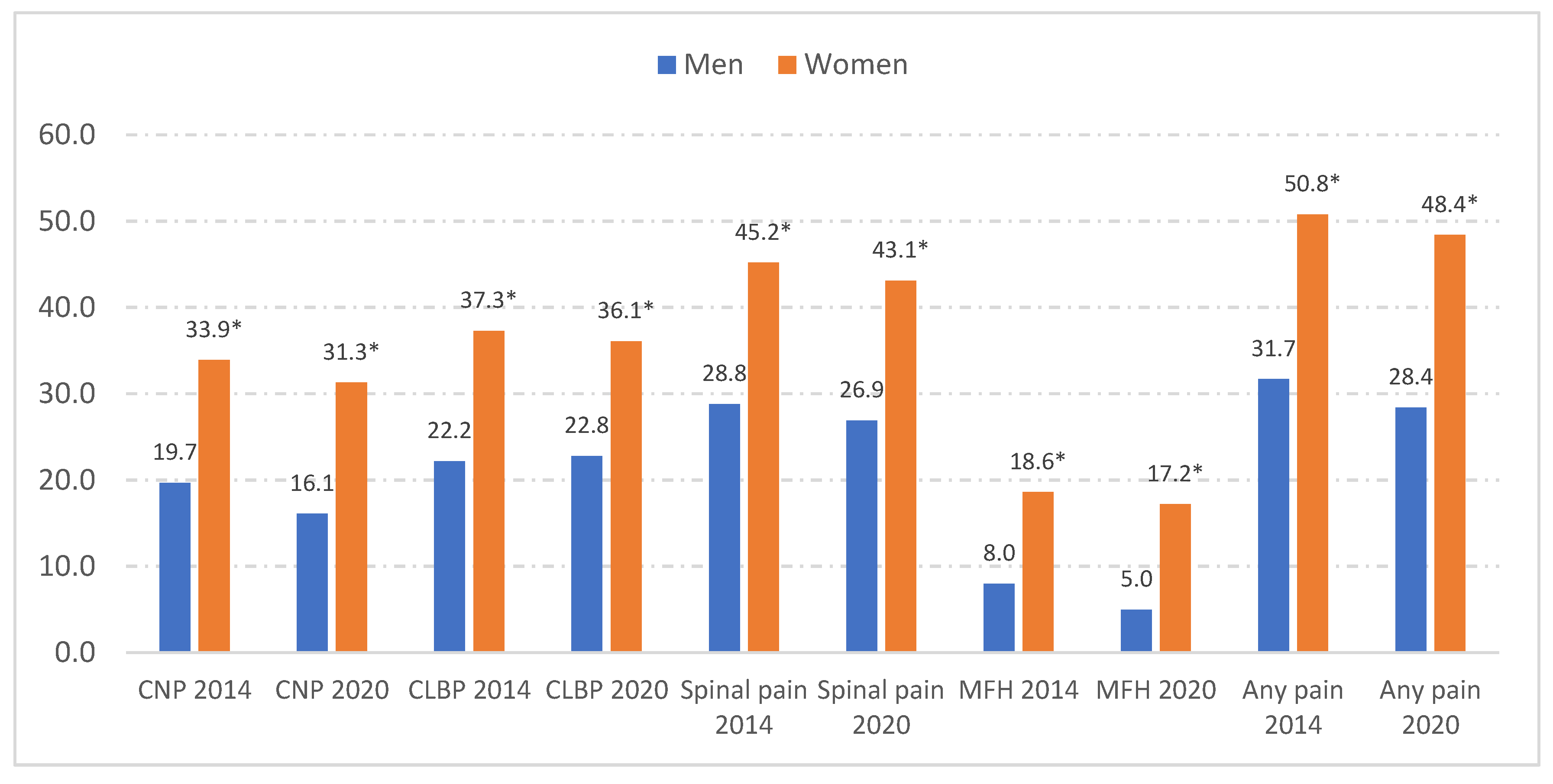
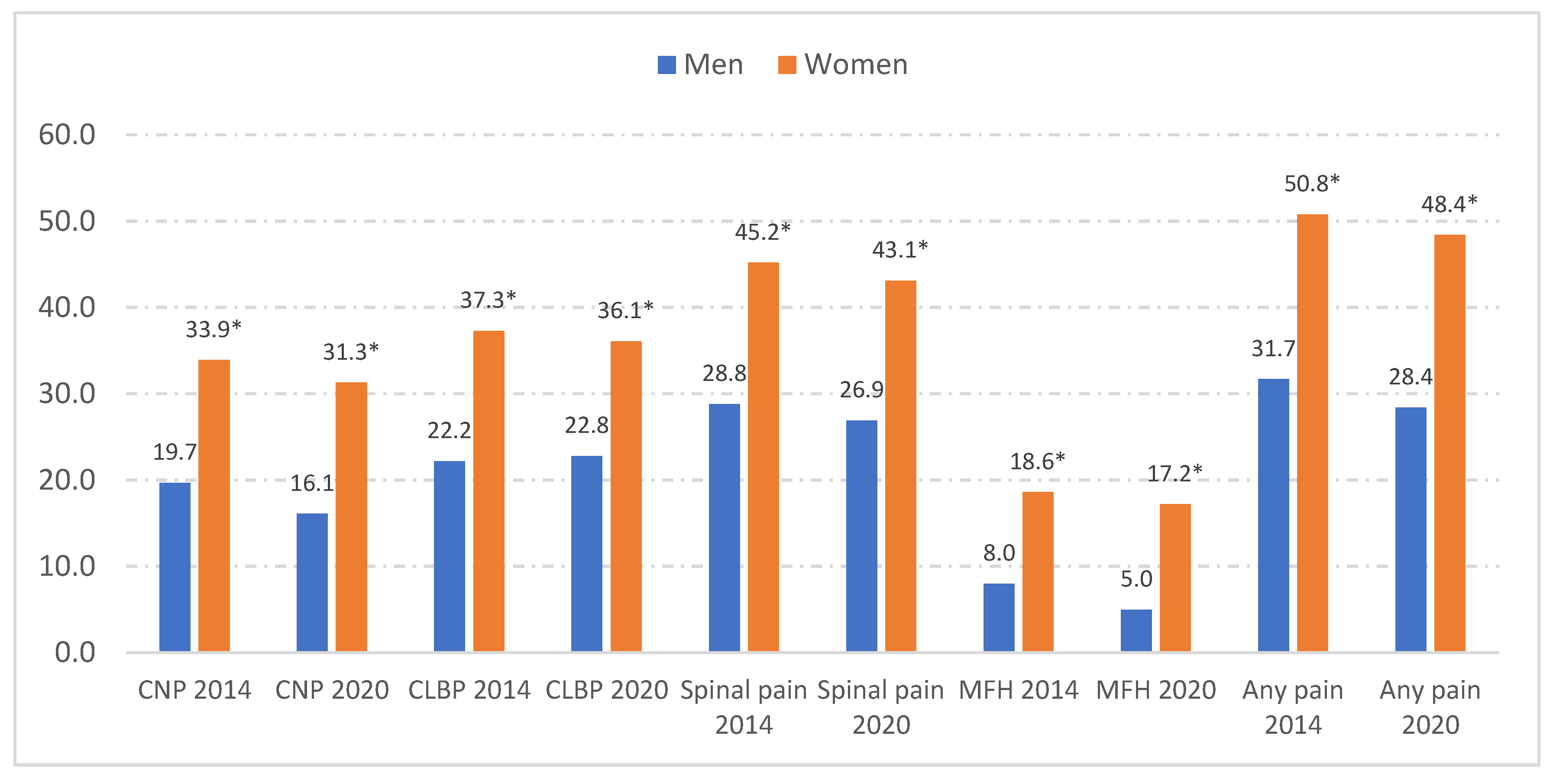
3.1. Sex Differences in Prevalence of Pain among People with Asthma
3.2. Prevalence of Pain among Cases and Matched Controls
3.3. Variables Associated with Self-Reported Presence of CNP, CLBP, and MFH in Asthma Patients
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Quirce, S.; Plaza, V.; Picado, C.; Vennera, M.; Casafont, J. Prevalence of uncontrolled severe persistent asthma in pneumology and allergy hospital units in Spain. J. Investig. Allergol. Clin. Immunol. 2011, 21, 466–471. [Google Scholar] [PubMed]
- Beeckmans, N.; Vermeersch, A.; Lysens, R.; Van Wambeke, P.; Goossens, N.; Thys, T.; Brumagne, S.; Janssens, L. The presence of respiratory disorders in individuals with low back pain: A systematic review. Man. Ther. 2016, 26, 77–86. [Google Scholar] [CrossRef]
- Rasmussen-Barr, E.; Magnusson, C.; Nordin, M.; Skillgate, E. Are respiratory disorders risk factors for troublesome low-back pain? A study of a general population cohort in Sweden. Eur. Spine J. 2019, 28, 2502–2509. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.L.; Chen, P.E.; Tung, T.H.; Chien, C.W. Association Between Asthma and Migraine: A Systematic Review and Meta-Analysis of Observational Studies. Front. Allergy 2021, 2, 741135. [Google Scholar] [CrossRef] [PubMed]
- Martin, V.T.; Fanning, K.M.; Serrano, D.; Buse, D.C.; Reed, M.L.; Lipton, R.B. Asthma is a risk factor for new onset chronic migraine: Results from the American migraine prevalence and prevention study. Headache 2016, 56, 118–131. [Google Scholar] [CrossRef]
- Kazeminasab, S.; Nejadghaderi, S.A.; Amiri, P.; Pourfathi, H.; Araj-Khodaei, M.; Sullman, M.J.M.; Kolahi, A.A.; Safiri, S. Neck pain: Global epidemiology, trends and risk factors. BMC Musculoskelet. Disord. 2022, 23, 26. [Google Scholar] [CrossRef]
- Steiner, T.J.; Stovner, L.J.; Jensen, R.; Uluduz, D.; Katsarava, Z.; Lifting the Burden: The Global Campaign against Headache. Migraine remains second among the world’s causes of disability, and first among young women: Findings from GBD2019. J. Headache Pain. 2020, 21, 137. [Google Scholar] [CrossRef]
- Stewart, W.F.; Shechter, A.; Rasmussen, B.K. Migraine prevalence. A review of population-based studies. Neurology 1994, 44, S17–S23. [Google Scholar]
- Tucker, G.F., Jr. Pulmonary migraine. Ann. Otol. Rhinol. Laryngol. 1977, 86, 671–676. [Google Scholar] [CrossRef]
- Sayyah, M.; Saki-Malehi, A.; Javanmardi, F.; Forouzan, A.; Shirbandi, K.; Rahim, F. Which came first, the risk of migraine or the risk of asthma? A systematic review. Neurol. Neurochir. Pol. 2018, 52, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen-Barr, E.; Nordin, M.; Skillgate, E. Are respiratory disorders risk factors for troublesome neck/shoulder pain? A study of a general population cohort in Sweden. Eur. Spine J. 2023, 32, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Hellebrandova, L.; Chlumsky, J.; Vostatek, P.; Novak, D.; Ryznarova, Z.; Bunc, V. Airfow limitation is accompanied by diaphragm dysfunction. Physiol. Res. 2006, 65, 469–479. [Google Scholar]
- Lunardi, A.C.; Marques da Silva, C.C.; Rodrigues Mendes, F.A.; Marques, A.P.; Stelmach, R.; Fernandes Carvalho, C.R. Musculoskeletal dysfunction and pain in adults with asthma. J. Asthma 2011, 48, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Rajan, J.P.; Wineinger, N.E.; Stevenson, D.D.; White, A.A. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: A meta-analysis of the literature. J. Allergy Clin. Immunol. 2015, 135, 676–681.e1. [Google Scholar] [CrossRef]
- Levy, S.; Volans, G. The use of analgesics in patients with asthma. Drug. Saf. 2001, 24, 829–841. [Google Scholar] [CrossRef]
- Ingram, E.E.; Bocklud, B.E.; Corley, S.C.; Granier, M.A.; Neuchat, E.E.; Ahmadzadeh, S.; Shekoohi, S.; Kaye, A.D. Non-CGRP Antagonist/Non-Triptan Options for Migraine Disease Treatment: Clinical Considerations. Curr. Pain Headache Rep. 2023, 27, 497–502. [Google Scholar] [CrossRef]
- Martínez-Moragón, E.; Serra-Batllés, J.; De Diego, A.; Palop, M.; Casan, P.; Rubio-Terrés, C.; Pellicer, C.; por el Grupo de Investigadores del estudio AsmaCost. Coste económico del paciente asmático en España (estudio AsmaCost) [Economic cost of treating the patient with asthma in Spain: The AsmaCost study]. Arch. Bronconeumol. 2009, 45, 481–486. (In Spanish) [Google Scholar] [CrossRef]
- Sicras-Mainar, A.; Capel, M.; Navarro-Artieda, R.; Nuevo, J.; Orellana, M.; Resler, G. Real-life retrospective observational study to determine the prevalence and economic burden of severe asthma in Spain. J. Med. Econ. 2020, 23, 492–500. [Google Scholar] [CrossRef]
- Consejo General de Colegios Oficiales de Médicos Los Costes de la Cronificación del Dolor Lumbar y Cervical [The Costs of Chronic Lumbar and Cervical and Pain]. Available online: https://pautasdeactuacionyseguimiento.com/static/uploads/files/modulos/dolor-cervical-y-lumbar-agudo.pdf (accessed on 11 November 2023).
- Eurostat. European Health Interview Survey (EHIS). Available online: https://ec.europa.eu/eurostat/web/microdata/european-health-interview-survey (accessed on 28 May 2023).
- Instituto Nacional de Estadística. Encuesta Europea de Salud en España. [European Health Interview Surveys for Spain]. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176784&menu=metodologia&idp=1254735573175 (accessed on 28 May 2023).
- Ministerio de Sanidad. European Health Survey in Spain 2020 [Encuesta Europea de Salud en España 2020]. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/EncuestaEuropea/Enc_Eur_Salud_en_Esp_2020.htm (accessed on 28 May 2023).
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression, 3rd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013. [Google Scholar]
- Ministerio de Sanidad. Encuesta Europea de Salud en España. Available online: https://www.sanidad.gob.es/estadisticas/microdatos.do (accessed on 28 May 2023).
- GBD 2021 Low Back Pain Collaborators. Global, Regional, and National Burden of Low Back Pain, 1990–2020, Its Attributable Risk Factors, and Projections to 2050: A Systematic Analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023, 5, e316–e329. [Google Scholar] [CrossRef]
- Matías-Guiu, J.; Porta-Etessam, J.; Mateos, V.; Díaz-Insa, S.; López-Gil, A.; Fernández, C.; Scientific Committee of the PALM Program. One-year prevalence of migraine in Spain: A nationwide population-based survey. Cephalalgia 2011, 31, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Bento, T.P.F.; Genebra, C.V.D.S.; Maciel, N.M.; Cornelio, G.P.; Simeão, S.F.A.P.; Vitta, A. Low back pain and some associated factors: Is there any difference between genders? Braz. J. Phys. Ther. 2020, 24, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Pérez, M.P.; Marín-Gracia, M.; Bellosta-Diago, E.; Santos-Lasaosa, S. Epidemiología de la migraña en España y Latinoamérica [Epidemiology of migraine in Spain and Latin America]. Rev. Neurol. 2020, 71, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Palacios-Ceña, D.; Albaladejo-Vicente, R.; Hernández-Barrera, V.; Lima-Florencio, L.; Fernández-de-Las-Peñas, C.; Jimenez-Garcia, R.; López-de-Andrés, A.; de Miguel-Diez, J.; Perez-Farinos, N. Female Gender Is Associated with a Higher Prevalence of Chronic Neck Pain, Chronic Low Back Pain, and Migraine: Results of the Spanish National Health Survey, 2017. Pain Med. 2021, 22, 382–395. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, N.U.; Guntur, V.P.; Newcomb, D.C.; Wechsler, M.E. Sex and gender in asthma. Eur. Respir. Rev. 2021, 30, 210067. [Google Scholar] [CrossRef] [PubMed]
- Triebner, K.; Johannessen, A.; Puggini, L.; Benediktsdóttir, B.; Bertelsen, R.J.; Bifulco, E.; Dharmage, S.C.; Dratva, J.; Franklin, K.A.; Gíslason, T.; et al. Menopause as a predictor of new-onset asthma: A longitudinal Northern European population study. J. Allergy Clin. Immunol. 2016, 137, 50–57.e6. [Google Scholar] [CrossRef] [PubMed]
- Larsson, U.; Taft, C.; Karlsson, J.; Sullivan, M. Gender and age differences in the relative burden of rhinitis and asthma on health-related quality of life—A Swedish population study. Respir. Med. 2007, 101, 1291–1298. [Google Scholar] [CrossRef]
- Mills, S.E.E.; Nicolson, K.P.; Smith, B.H. Chronic pain: A review of its epidemiology and associated factors in population-based studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- de Miguel-Díez, J.; López-de-Andrés, A.; Hernandez-Barrera, V.; Jimenez-Trujillo, I.; Del Barrio, J.L.; Puente-Maestu, L.; Martinez-Huedo, M.A.; Jimenez-García, R. Prevalence of Pain in COPD Patients and Associated Factors: Report from a Population-based Study. Clin. J. Pain. 2018, 34, 787–794. [Google Scholar] [CrossRef]
- Bentsen, S.B.; Holm, A.M.; Christensen, V.L.; Henriksen, A.H.; Småstuen, M.C.; Rustøen, T. Changes in and predictors of pain and mortality in patients with chronic obstructive pulmonary disease. Respir. Med. 2020, 171, 106116. [Google Scholar] [CrossRef]
- Bordoni, B.; Marelli, F.; Morabito, B.; Sacconi, B.; Caiazzo, P.; Castagna, R. Low back pain and gastroesophageal reflux in patients with COPD: The disease in the breath. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 325–334. [Google Scholar] [CrossRef] [PubMed]
- Almeida, V.P.; Guimarães, F.S.; Moço, V.J.; Menezes, S.L.; Mafort, T.T.; Lopes, A.J. Correlação entre função pulmonar, postura e composição corporal em pacientes com asma [Correlation between pulmonary function, posture, and body composition in patients with asthma]. Rev. Port. Pneumol. 2013, 19, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Boulay, C.; Tardieu, C.; Hecquet, J.; Benaim, C.; Mouilleseaux, B.; Marty, C.; Prat-Pradal, D.; Legaye, J.; Duval-Beaupère, G.; Pélissier, J. Sagittal alignment of spine and pelvis regulated by pelvic incidence: Standard values and prediction of lordosis. Eur. Spine J. 2006, 15, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad. Spanish National Health Survey in [Encuesta Nacional de Salud]. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736176783&menu=metodologia&idp=1254735573175 (accessed on 11 November 2023).

{kind=link}
| Variable | Categories | EHISS 2014 | EHISS 2020 | |||
|---|---|---|---|---|---|---|
| n | % | n | % | p | ||
| Sex | Women | 785 | 59.8 | 668 | 58.0 | 0.366 |
| Age, Mean (SD) | 52.6 | (18.9) | 54.1 | (18.8) | 0.165 | |
| Age groups (Years) | 18–49 | 610 | 47.8 | 496 | 44.5 | 0.251 |
| 50–69 | 370 | 29.0 | 340 | 30.5 | ||
| 70 or over | 295 | 23.1 | 279 | 25.0 | ||
| Educational level | No studies/primary | 745 | 56.8 | 629 | 54.6 | 0.210 |
| Secondary | 211 | 16.1 | 216 | 18.8 | ||
| High education | 356 | 27.1 | 306 | 26.6 | ||
| Living with a partner | Yes | 699 | 53.6 | 556 | 48.6 | 0.012 |
| Chronic neck pain | Yes | 370 | 28.2 | 287 | 24.9 | 0.067 |
| Chronic low back pain | Yes | 410 | 31.3 | 351 | 30.5 | 0.686 |
| Spinal pain | Yes | 507 | 38.6 | 418 | 36.3 | 0.234 |
| Migraine or frequent headache | Yes | 188 | 14.3 | 139 | 12.1 | 0.100 |
| Any pain | Yes | 566 | 43.1 | 460 | 40.0 | 0.111 |
| Pain intensity | No pain | 498 | 38.0 | 482 | 41.9 | 0.048 |
| Light | 329 | 25.1 | 261 | 22.7 | ||
| Moderate | 265 | 20.2 | 249 | 21.6 | ||
| Severe/extreme | 220 | 16.8 | 159 | 13.8 | ||
| Use of pain medication | Yes | 509 | 44.8 | 464 | 48.7 | 0.076 |
| Self-rated health | Very good/good | 624 | 47.6 | 555 | 48.2 | 0.744 |
| Fair/poor/very poor | 688 | 52.4 | 596 | 51.8 | ||
| Diabetes | Yes | 153 | 11.7 | 135 | 11.7 | 0.959 |
| COPD | Yes | 334 | 25.5 | 260 | 22.6 | 0.097 |
| Heart diseases | Yes | 170 | 13.0 | 165 | 14.3 | 0.320 |
| Stroke | Yes | 37 | 2.8 | 38 | 3.3 | 0.488 |
| Cancer | Yes | 67 | 5.1 | 70 | 6.1 | 0.292 |
| High blood pressure | Yes | 402 | 30.6 | 376 | 32.7 | 0.280 |
| Mental disease | Yes | 306 | 23.3 | 276 | 24.0 | 0.702 |
| Physical activity in leisure time | No | 557 | 42.6 | 507 | 44.1 | 0.443 |
| Alcohol consumption | Yes | 697 | 53.2 | 573 | 49.8 | 0.094 |
| Active smoking | Yes | 287 | 21.9 | 212 | 18.5 | 0.034 |
| Body mass index | <25 | 545 | 41.6 | 456 | 39.8 | 0.392 |
| 25–29.9 | 469 | 35.8 | 405 | 35.3 | ||
| ≥30 | 297 | 22.7 | 286 | 24.9 | ||
| CNP | CLBP | MFH | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No Asthma n% | Asthma n% | No Asthma n% | Asthma n% | No Asthma n% | Asthma n% | ||||||||
| Sex d,e,f,g,h,i | Men a,b,c | 85 | 8.4 | 182 | 18.0 | 125 | 12.4 | 227 | 22.5 | 30 | 3.0 | 66 | 6.5 |
| Women a,b,c | 288 | 19.8 | 475 | 32.7 | 307 | 21.1 | 534 | 36.8 | 171 | 11.8 | 261 | 18.0 | |
| Age groups d,e,f,g,h | 18–49 years a,b,c | 94 | 8.5 | 170 | 15.4 | 102 | 9.2 | 197 | 17.8 | 101 | 9.1 | 142 | 12.8 |
| 50–69 years a,b,c | 140 | 19.7 | 244 | 34.4 | 164 | 23.1 | 287 | 40.4 | 65 | 9.2 | 110 | 15.5 | |
| 70 years or over a,b,c | 138 | 24.0 | 241 | 42.0 | 166 | 28.9 | 273 | 47.6 | 33 | 5.7 | 68 | 11.8 | |
| Educational level d,e,g,h,i | No studies/primary a,b,c | 253 | 19.1 | 486 | 35.4 | 305 | 23.1 | 551 | 40.1 | 104 | 7.9 | 205 | 14.9 |
| Secondary a,b,c | 59 | 12.3 | 72 | 16.9 | 57 | 11.9 | 90 | 21.1 | 38 | 7.9 | 57 | 13.3 | |
| High education a,b,c | 61 | 9.2 | 99 | 15.0 | 70 | 10.6 | 120 | 18.1 | 59 | 8.9 | 65 | 9.8 | |
| Living with a partner f | No a,b,c | 192 | 15.9 | 305 | 25.6 | 213 | 17.6 | 350 | 29.3 | 81 | 6.7 | 167 | 14.0 |
| Yes a,b,c | 180 | 14.5 | 349 | 27.8 | 219 | 17.6 | 409 | 32.6 | 119 | 9.6 | 158 | 12.6 | |
| Pain intensity d,e,f,g,h,i | No pain a,b,c | 56 | 4.2 | 82 | 8.4 | 73 | 5.5 | 92 | 9.4 | 45 | 3.4 | 42 | 4.3 |
| Light a,b,c | 92 | 16.6 | 141 | 23.9 | 109 | 19.7 | 174 | 29.5 | 44 | 8.0 | 67 | 11.4 | |
| Moderate a,b,c | 117 | 32.5 | 219 | 42.6 | 127 | 35.3 | 240 | 46.7 | 60 | 16.7 | 104 | 20.2 | |
| Severe/extreme a,c | 108 | 51.7 | 215 | 56.7 | 123 | 58.9 | 255 | 67.3 | 52 | 24.9 | 114 | 30.1 | |
| Use of pain medication d,e,f,g,h,i | No a,b,c | 92 | 9.7 | 196 | 17.6 | 112 | 11.8 | 205 | 18.4 | 53 | 5.6 | 88 | 7.9 |
| Yes a,b,c | 233 | 34.7 | 434 | 44.6 | 279 | 41.6 | 510 | 52.4 | 121 | 18.0 | 223 | 22.9 | |
| Concomitant CNP e,f,h,i | No b,c | NA | NA | NA | NA | 157 | 12.1 | 239 | 16.4 | 111 | 8.6 | 133 | 9.1 |
| Yes b,c | NA | NA | NA | NA | 234 | 72.0 | 476 | 75.6 | 63 | 19.4 | 178 | 28.3 | |
| Concomitant CLBP d,f,g,i | No a,c | 91 | 7.4 | 154 | 11.2 | NA | NA | NA | NA | 100 | 8.1 | 128 | 9.3 |
| Yes c | 234 | 59.8 | 476 | 66.6 | NA | NA | NA | NA | 74 | 18.9 | 183 | 25.6 | |
| Concomitant MFH d,e,g,h | No a,b | 262 | 18.1 | 452 | 25.5 | 317 | 22 | 532 | 30.0 | NA | NA | NA | NA |
| Yes a,b | 63 | 36.2 | 178 | 57.2 | 74 | 42.5 | 183 | 58.8 | NA | NA | NA | NA | |
| CNP | CLBP | MFH | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No Asthma, n% | Asthma, n% | No Asthma, n% | Asthma, n% | No Asthma, n% | Asthma, n% | ||||||||
| Self-rated health d,e,f,g,h,i | Fair/poor/very poor a,b,c | 241 | 33.3 | 510 | 43.3 | 288 | 39.8 | 582 | 49.4 | 104 | 14.4 | 230 | 19.5 |
| Very good/good a,b,c | 132 | 7.6 | 147 | 11.4 | 144 | 8.3 | 179 | 13.9 | 97 | 5.6 | 97 | 7.6 | |
| Diabetes d,e,g,h | No a,b,c | 321 | 14.2 | 543 | 25.0 | 366 | 16.2 | 616 | 28.3 | 185 | 8.2 | 284 | 13.1 |
| Yes a,b,c | 52 | 25.1 | 114 | 39.6 | 66 | 31.9 | 145 | 50.3 | 16 | 7.7 | 43 | 14.9 | |
| COPD d,e,f,g,h,i | No a,b,c | 339 | 14.2 | 403 | 21.6 | 394 | 16.6 | 474 | 25.4 | 185 | 7.8 | 218 | 11.7 |
| Yes a,b,c | 34 | 40.5 | 254 | 42.8 | 38 | 45.2 | 287 | 48.3 | 16 | 19.0 | 109 | 18.4 | |
| Heart diseases d,e,g,h,i | No a,b,c | 293 | 13.2 | 502 | 23.6 | 340 | 15.3 | 586 | 27.5 | 179 | 8.1 | 269 | 12.6 |
| Yes a,b,c | 80 | 32.4 | 155 | 46.3 | 92 | 37.2 | 175 | 52.2 | 22 | 8.9 | 58 | 17.3 | |
| Stroke d,e,g,h,i | No a,b,c | 356 | 14.8 | 620 | 26.0 | 413 | 17.1 | 718 | 30.1 | 197 | 8.2 | 308 | 12.9 |
| Yes a,c | 17 | 33.3 | 37 | 49.3 | 19 | 37.3 | 43 | 57.3 | 4 | 7.8 | 19 | 25.3 | |
| Cancer e,g,h,i | No a,b,c | 352 | 14.9 | 592 | 25.5 | 406 | 17.1 | 692 | 29.8 | 192 | 8.1 | 295 | 12.7 |
| Yes a,b,c | 21 | 22.1 | 65 | 47.4 | 26 | 27.4 | 69 | 50.4 | 9 | 9.5 | 32 | 23.4 | |
| High blood pressure d,e,g,h,i | No a,b,c | 228 | 12.3 | 342 | 20.3 | 249 | 13.4 | 394 | 23.4 | 143 | 7.7 | 190 | 11.3 |
| Yes a,b,c | 145 | 23.9 | 315 | 40.5 | 183 | 30.1 | 367 | 47.2 | 58 | 9.6 | 137 | 17.6 | |
| Mental disease d,e,f,g,h,i | No a,b,c | 253 | 11.9 | 369 | 19.6 | 289 | 13.6 | 449 | 23.9 | 132 | 6.2 | 158 | 8.4 |
| Yes a,b,c | 120 | 35.7 | 288 | 49.5 | 143 | 42.6 | 312 | 53.6 | 69 | 20.5 | 169 | 29.0 | |
| Physical activity in leisure time d,e,f,g,h,i | Never a,b,c | 195 | 20.9 | 383 | 36.0 | 222 | 23.8 | 433 | 40.7 | 104 | 11.2 | 171 | 16.1 |
| Occasionally or frequent a,b,c | 178 | 11.6 | 272 | 19.5 | 210 | 13.7 | 327 | 23.4 | 97 | 6.3 | 156 | 11.2 | |
| Alcohol consumption d,e,f,g,h,i | No a,b,c | 219 | 18.4 | 394 | 33.1 | 253 | 21.2 | 448 | 37.6 | 111 | 9.3 | 210 | 17.6 |
| Yes a,b,c | 153 | 12.1 | 262 | 20.6 | 177 | 14 | 312 | 24.6 | 90 | 7.1 | 117 | 9.2 | |
| Active smoking d,e,g,h | No a,b,c | 301 | 15.8 | 546 | 27.8 | 353 | 18.5 | 647 | 33.0 | 150 | 7.9 | 259 | 13.2 |
| Yes a,b,c | 72 | 13.1 | 110 | 22 | 79 | 14.3 | 113 | 22.6 | 51 | 9.3 | 68 | 13.6 | |
| Body mass index d,e,f,g,h,i | <25 a,b,c | 145 | 12 | 212 | 21.2 | 163 | 13.5 | 241 | 24.1 | 102 | 8.5 | 125 | 12.5 |
| 25–29.9 a,b,c | 137 | 16.1 | 236 | 27 | 166 | 19.5 | 280 | 32.0 | 54 | 6.3 | 114 | 13.0 | |
| ≥30 a,b,c | 90 | 22.4 | 208 | 35.7 | 103 | 25.6 | 238 | 40.8 | 44 | 10.9 | 87 | 14.9 | |
| CNP | CLBP | MFH | ||
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | ||
| Sex | Men | 1 | 1 | 1 |
| Women | 1.37 (1.07–1.76) | 1.25 (1.02–1.58) | 2.00 (1.44–2.77) | |
| Age groups | 18–49 years | 1 | 1 | 1 |
| 50–69 years | 1.41 (1.05–1.88) | 1.76 (1.31–2.35) | 0.41 (0.29–0.58) | |
| 70 years or over | 1.64 (1.20–2.23) | 1.52 (1.11–2.09) | 0.21 (0.14–0.32) | |
| Self-rated health | Very good/good | 1 | 1 | 1 |
| Fair/poor/very poor | 0.50 (0.38–0.65) | 0.47 (0.36–0.61) | 0.74 (0.0.51–0.97) | |
| Diabetes | No | NSDM | 1 | NSDM |
| Yes | NSDM | 1.39 (1.00–1.93) | NSDM | |
| COPD | No | 1 | NSDM | NSDM |
| Yes | 1.31 (1.01–1.70) | NSDM | NSDM | |
| Mental disorder | No | 1 | NSDM | 1 |
| Yes | 1.55 (1.19–2.02) | NSDM | 2.73 (2.05–3.63) | |
| Use of pain medication | No | NSDM | 1 | 1 |
| Yes | NSDM | 2.46 (1.91–3.16) | 2.19 (1.61–2.98) | |
| Concomitant CNP | No | NA | 1 | 1 |
| Yes | NA | 9.81 (7.67–12.54) | 2.44 (1.76–3.37) | |
| Concomitant CLBP | No | 1 | NA | 1 |
| Yes | 10.06 (7.95–12.73) | NA | 1.65 (1.19–2.30) | |
| MFH | No | 1 | 1 | NA |
| Yes | 2.39 (1.74–3.28) | 1.67 (1.20–2.32) | NA | |
| YEAR | 2020 | 0.81 (0.65–1.02) | 1.05 (0.83–1.33) | 0.81 (0.62–1.06) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Albaladejo, N.; López-de-Andrés, A.; Cuadrado-Corrales, N.; Albaladejo-Vicente, R.; Villanueva-Orbaiz, R.; Carricondo, F.; Romero-Gomez, B.; Jiménez-García, R.; Perez-Farinos, N. Asthma Is Associated with Back Pain and Migraine—Results of Population-Based Case–Control Study. J. Clin. Med. 2023, 12, 7107. https://doi.org/10.3390/jcm12227107
Gutiérrez-Albaladejo N, López-de-Andrés A, Cuadrado-Corrales N, Albaladejo-Vicente R, Villanueva-Orbaiz R, Carricondo F, Romero-Gomez B, Jiménez-García R, Perez-Farinos N. Asthma Is Associated with Back Pain and Migraine—Results of Population-Based Case–Control Study. Journal of Clinical Medicine. 2023; 12(22):7107. https://doi.org/10.3390/jcm12227107
Chicago/Turabian StyleGutiérrez-Albaladejo, Natalia, Ana López-de-Andrés, Natividad Cuadrado-Corrales, Romana Albaladejo-Vicente, Rosa Villanueva-Orbaiz, Francisco Carricondo, Barbara Romero-Gomez, Rodrigo Jiménez-García, and Napoleon Perez-Farinos. 2023. "Asthma Is Associated with Back Pain and Migraine—Results of Population-Based Case–Control Study" Journal of Clinical Medicine 12, no. 22: 7107. https://doi.org/10.3390/jcm12227107
APA StyleGutiérrez-Albaladejo, N., López-de-Andrés, A., Cuadrado-Corrales, N., Albaladejo-Vicente, R., Villanueva-Orbaiz, R., Carricondo, F., Romero-Gomez, B., Jiménez-García, R., & Perez-Farinos, N. (2023). Asthma Is Associated with Back Pain and Migraine—Results of Population-Based Case–Control Study. Journal of Clinical Medicine, 12(22), 7107. https://doi.org/10.3390/jcm12227107