

Morphological Comparison of Residual Ridge in Impression for Removable Partial Denture between Digital and Conventional Techniques: A Preliminary In-Vivo Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Digital Impression Data
2.3. Conventional Impression Data
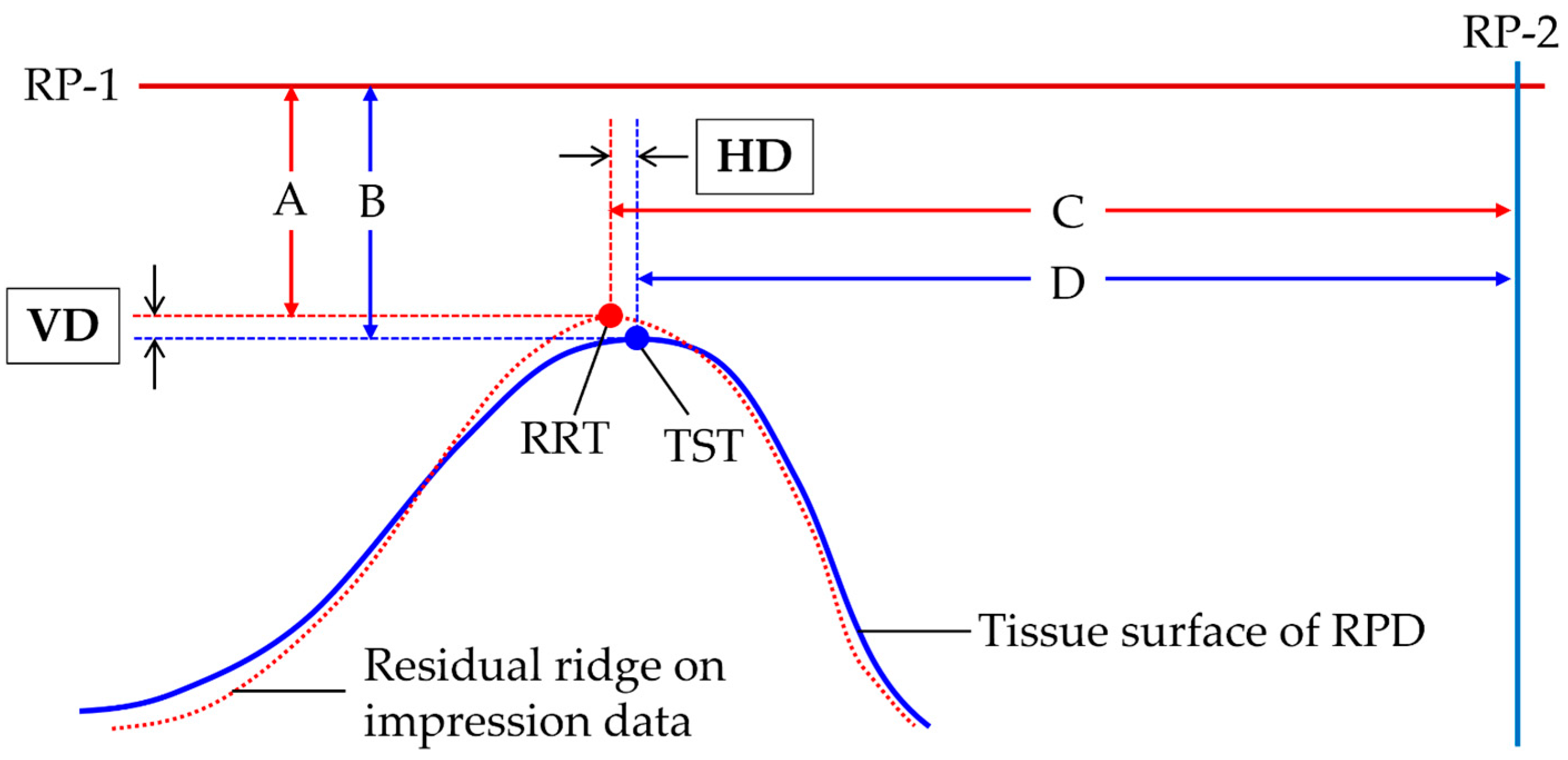
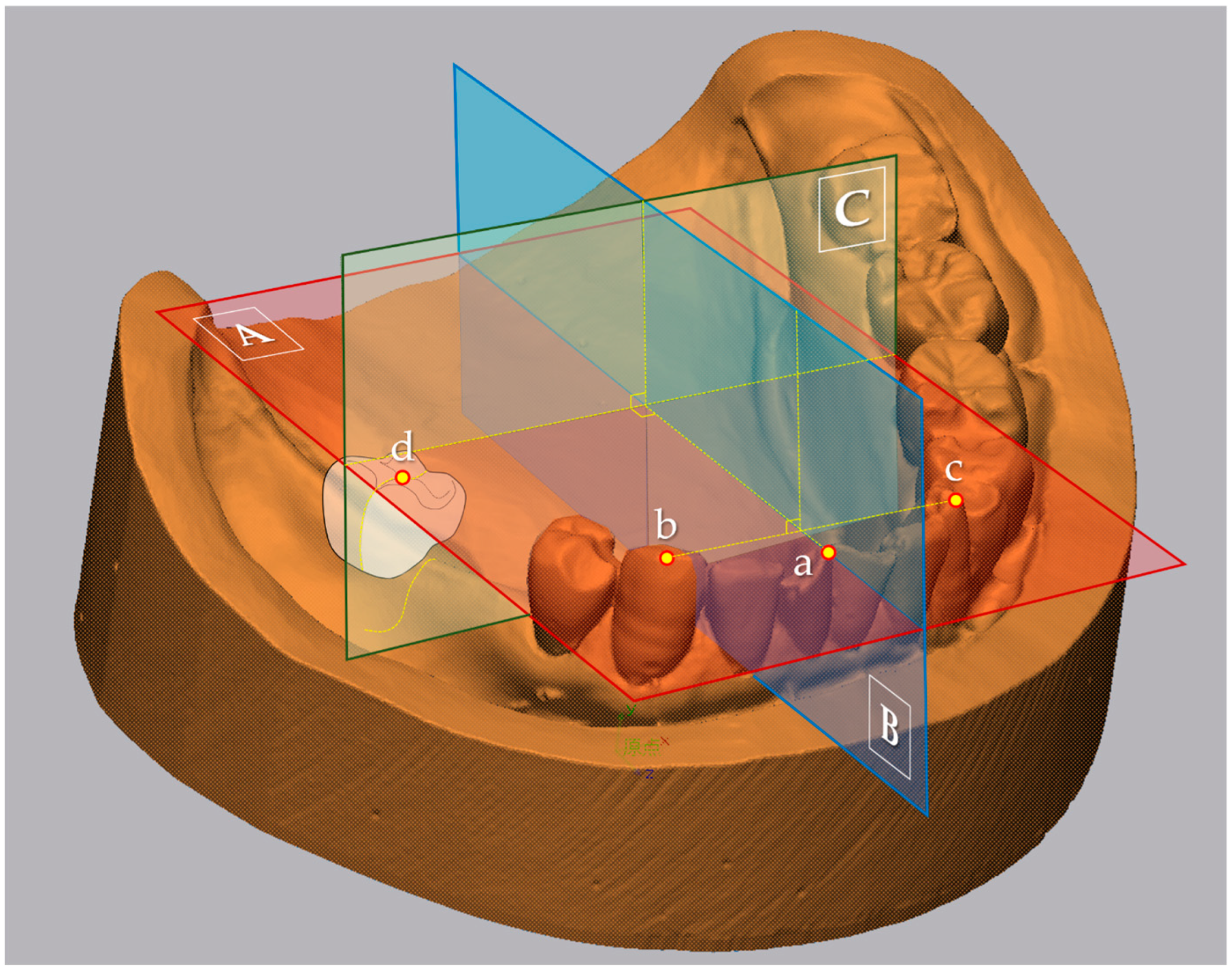
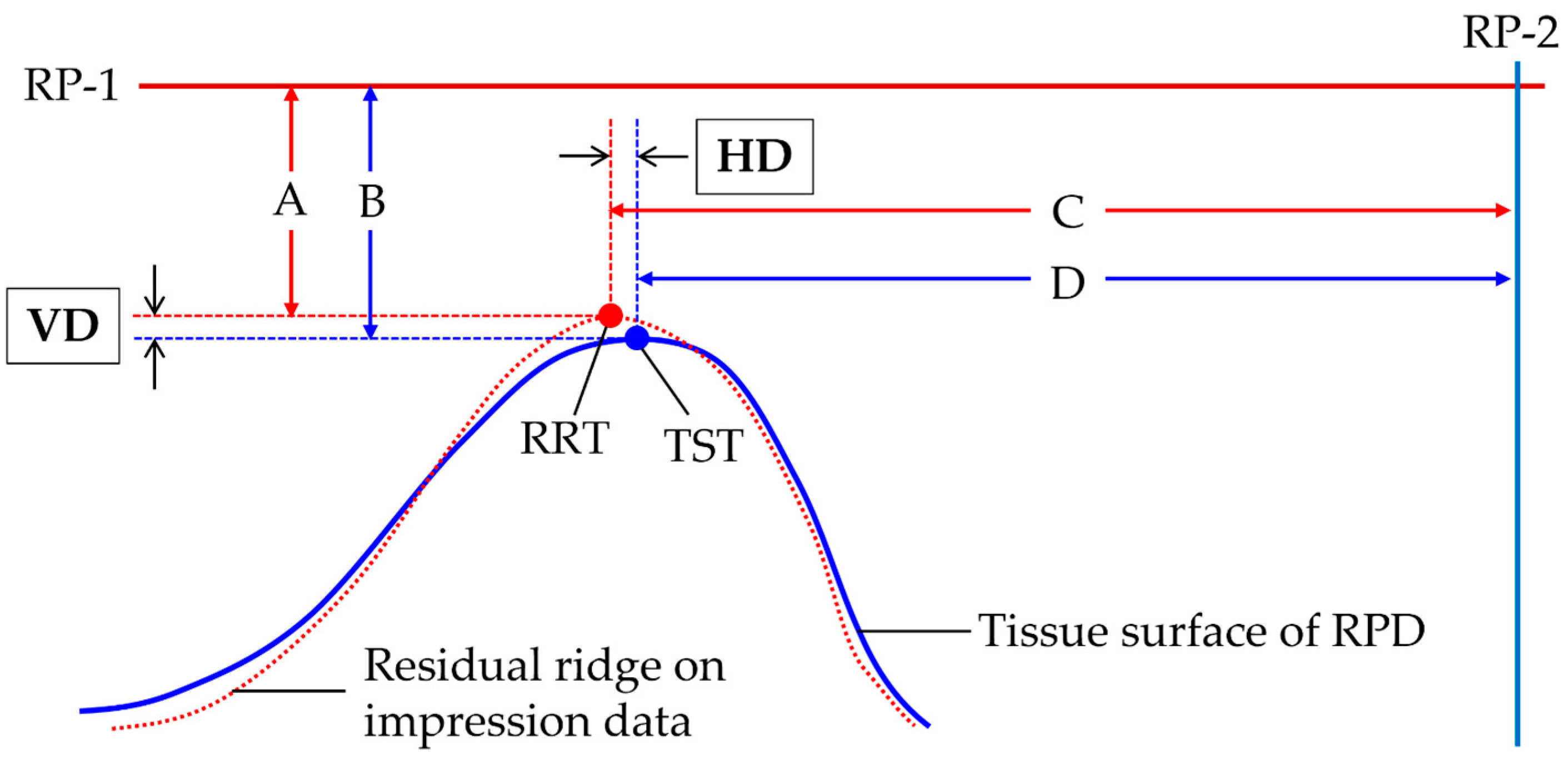
2.4. Calculation of Representative Values for Morphological Comparison
2.5. Mucosal Thickness of Residual Ridge
2.6. Statistical Analysis
3. Results
3.1. Participants and Visual Assessment
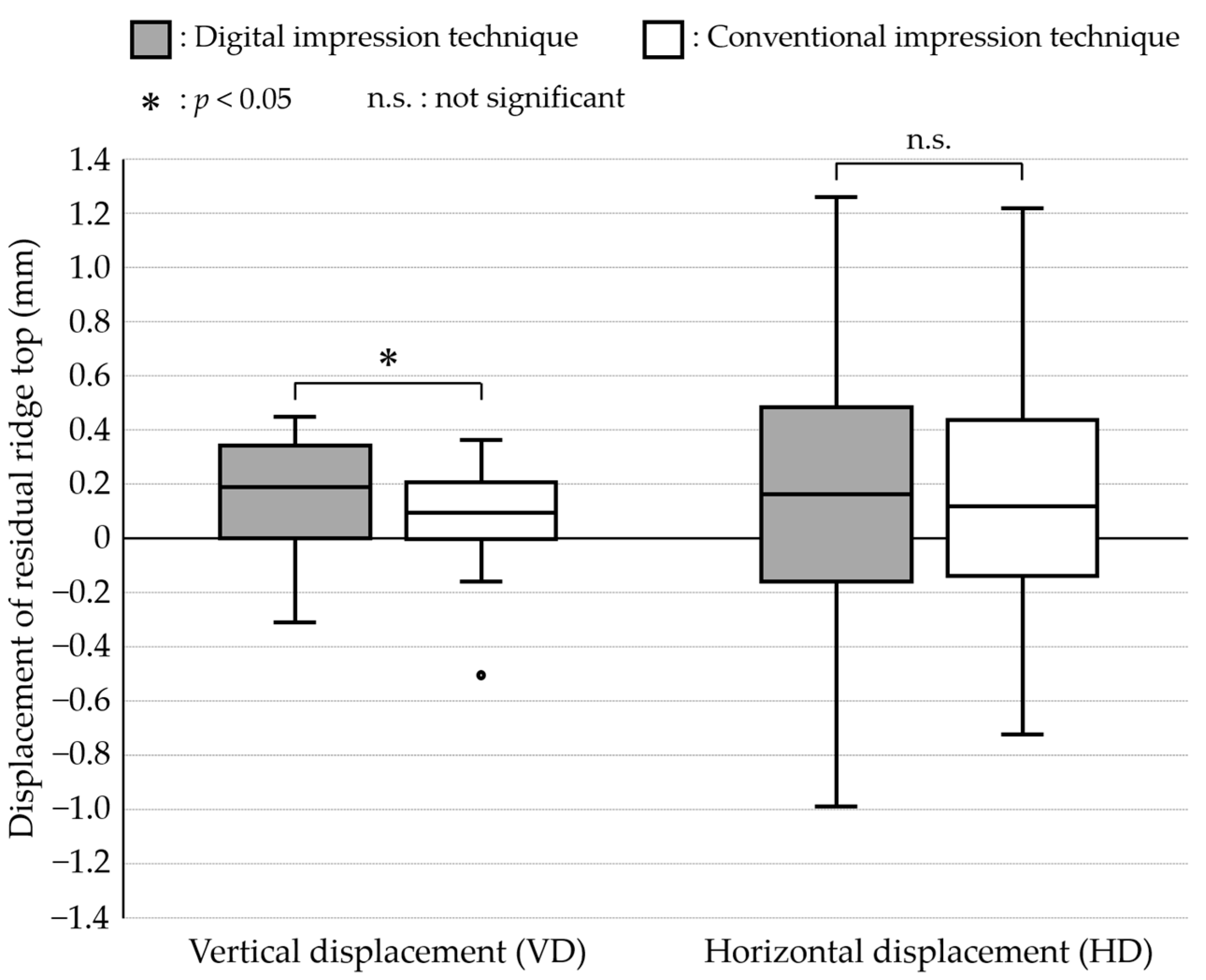
3.2. Comparison between Digital and Conventional Impressions
3.3. Correlation of Mucosal Thickness with the Morphological Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virard, F.; Venet, L.; Richert, R.; Pfeffer, D.; Viguié, G.; Bienfait, A.; Farges, J.C.; Ducret, M. Manufacturing of an immediate removable partial denture with an intraoral scanner and CAD-CAM technology: A case report. BMC Oral Health 2018, 18, 120. [Google Scholar] [CrossRef] [PubMed]
- Nishiyama, H.; Taniguchi, A.; Tanaka, S.; Baba, K. Novel fully digital workflow for removable partial denture fabrication. J. Prosthodont. Res. 2020, 64, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Phoenix, R.D.; Cagna, D.R.; DeFreest, C.F. Stewart’s Clinical Removable Partial Prosthodontics, 4th ed.; Quintessence Publishing Co.: Chicago, IL, USA, 2008; p. 24. [Google Scholar]
- Dental Impression Materials. Available online: https://www.ncbi.nlm.nih.gov/books/NBK574496/ (accessed on 9 November 2023).
- Fueki, K.; Inamochi, Y.; Wada, J.; Arai, Y.; Takaichi, A.; Murakami, N.; Ueno, T.; Wakabayashi, N. A systematic review of digital removable partial dentures. Part I: Clinical evidence, digital impression, and maxillomandibular relationship record. J. Prosthodont. Res. 2020, 66, 40–52. [Google Scholar] [CrossRef]
- Harb, I.E.; Abdel-Khalek, E.A.; Hegazy, S.A. CAD/CAM Constructed Poly(etheretherketone) (PEEK) Framework of Kennedy Class I Removable Partial Denture: A Clinical Report. J. Prosthodont. 2019, 28, e595–e598. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Cheng, Y.; Gao, B.; Yu, H. A novel digital altered cast impression technique for fabricating a removable partial denture with a distal extension. J. Am. Dent. Assoc. 2020, 151, 297–302. [Google Scholar] [CrossRef]
- Cameron, A.B.; Evans, J.L.; Robb, N.D. A technical and clinical digital approach to the altered cast technique with an intraoral scanner and polyvinyl siloxane impression material. J. Prosthet. Dent. 2022, 15. [Google Scholar] [CrossRef] [PubMed]
- Thompson, W.D.; Kratochvil, F.J.; Caputo, A.A. Evaluation of photoelastic stress patterns produced by various designs of bilateral distal-extension removable partial dentures. J. Prosthet. Dent. 1977, 38, 261–273. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, E. Partial Denture Construction; Dental Items of Interest: Brooklyn, NY, USA, 1928; pp. 231–247. [Google Scholar]
- Kim, E.Y.; Wada, J.; Sakamoto, K.; Ishioka, Y.; Arai, Y.; Murakami, N.; Yamazaki, T.; Hayama, H.; Utsumi, M.; Inukai, S.; et al. Effect of Scanning Origin Location on Data Accuracy of Abutment Teeth Region in Digital Impression Acquired Using Intraoral Scanner for Removable Partial Denture: A Preliminary In Vitro Study. J. Clin. Med. 2022, 11, 7392. [Google Scholar] [CrossRef] [PubMed]
- ISO 12836:2015; Dentistry, Digitizing devices for CAD/CAM systems for Indirect Dental Restorations, Test Methods for Assessing Accuracy. ISO: Geneva, Switzerland, 2015. Available online: https://www.iso.org/standard/68414.html (accessed on 9 November 2023).
- Luthardt, R.G.; Koch, R.; Rudolph, H.; Walter, M.H. Qualitative computer aided evaluation of dental impressions in vivo. Dent. Mater. 2006, 22, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Rehm, H. Biophysikalischer Beitrag zur Problematik starr abgestützter Freiend-prothesen. Dtsch. Zahnärztl Z. 1962, 17, 963–975. [Google Scholar]
- Steffel, V.L. Fundamental principles involved in partial denture design. J. Am. Dent. Assoc. 1951, 42, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Hayama, H.; Fueki, K.; Wadachi, J.; Wakabayashi, N. Trueness and precision of digital impressions obtained using an intraoral scanner with different head size in the partially edentulous mandible. J. Prosthodont. Res. 2018, 62, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Amelya, A.; Shin, Y.; Shim, J.S. Accuracy of intraoral digital impressions using an artificial landmark. J. Prosthet. Dent. 2017, 117, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Tasaka, A.; Wadachi, J.; Yamashita, S. A new proposal for improving the accuracy of intraoral scanning for partially edentulous residual ridge. J. Prosthodont. Res. 2023, 67, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Uchida, H.; Kobayashi, K.; Nagao, M. Measurement in vivo of masticatory mucosal thickness with 20 MHz B-mode ultrasonic diagnostic equipment. J. Dent. Res. 1989, 68, 95–100. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | |||
|---|---|---|---|
| Age (SD) | 78.2 (9.7) | ||
| Participant number (%) | Sex | Female | 15 (68.2%) |
| Male | 7 (31.8%) | ||
| Missing teeth number of target mucosal area (%) | 2 | 4 (18.2%) | |
| 3 | 8 (36.4%) | ||
| 4 | 10 (45.4%) | ||
| Mucosal thickness (mm) (SD) | 1.87 (0.30) |
| Displacement | Impression Technique | ρ | p-Value |
|---|---|---|---|
| VD | Digital | −0.332 | 0.132 |
| Conventional | −0.327 | 0.138 | |
| HD | Digital | −0.100 | 0.659 |
| Conventional | −0.036 | 0.873 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishioka, Y.; Wada, J.; Kim, E.-Y.; Sakamoto, K.; Arai, Y.; Murakami, N.; Yamazaki, T.; Takakusaki, K.; Hayama, H.; Utsumi, M.; et al. Morphological Comparison of Residual Ridge in Impression for Removable Partial Denture between Digital and Conventional Techniques: A Preliminary In-Vivo Study. J. Clin. Med. 2023, 12, 7103. https://doi.org/10.3390/jcm12227103
Ishioka Y, Wada J, Kim E-Y, Sakamoto K, Arai Y, Murakami N, Yamazaki T, Takakusaki K, Hayama H, Utsumi M, et al. Morphological Comparison of Residual Ridge in Impression for Removable Partial Denture between Digital and Conventional Techniques: A Preliminary In-Vivo Study. Journal of Clinical Medicine. 2023; 12(22):7103. https://doi.org/10.3390/jcm12227103
Chicago/Turabian StyleIshioka, Yurika, Junichiro Wada, Eung-Yeol Kim, Kazuki Sakamoto, Yuki Arai, Natsuko Murakami, Toshiki Yamazaki, Kensuke Takakusaki, Hironari Hayama, Miona Utsumi, and et al. 2023. "Morphological Comparison of Residual Ridge in Impression for Removable Partial Denture between Digital and Conventional Techniques: A Preliminary In-Vivo Study" Journal of Clinical Medicine 12, no. 22: 7103. https://doi.org/10.3390/jcm12227103
APA StyleIshioka, Y., Wada, J., Kim, E.-Y., Sakamoto, K., Arai, Y., Murakami, N., Yamazaki, T., Takakusaki, K., Hayama, H., Utsumi, M., Inukai, S., & Wakabayashi, N. (2023). Morphological Comparison of Residual Ridge in Impression for Removable Partial Denture between Digital and Conventional Techniques: A Preliminary In-Vivo Study. Journal of Clinical Medicine, 12(22), 7103. https://doi.org/10.3390/jcm12227103