
Cardiorespiratory Fitness and Risk of Cardiovascular Events and Mortality in Middle Age Patients without Known Cardiovascular Disease


Abstract
:1. Introduction
2. Materials and Methods
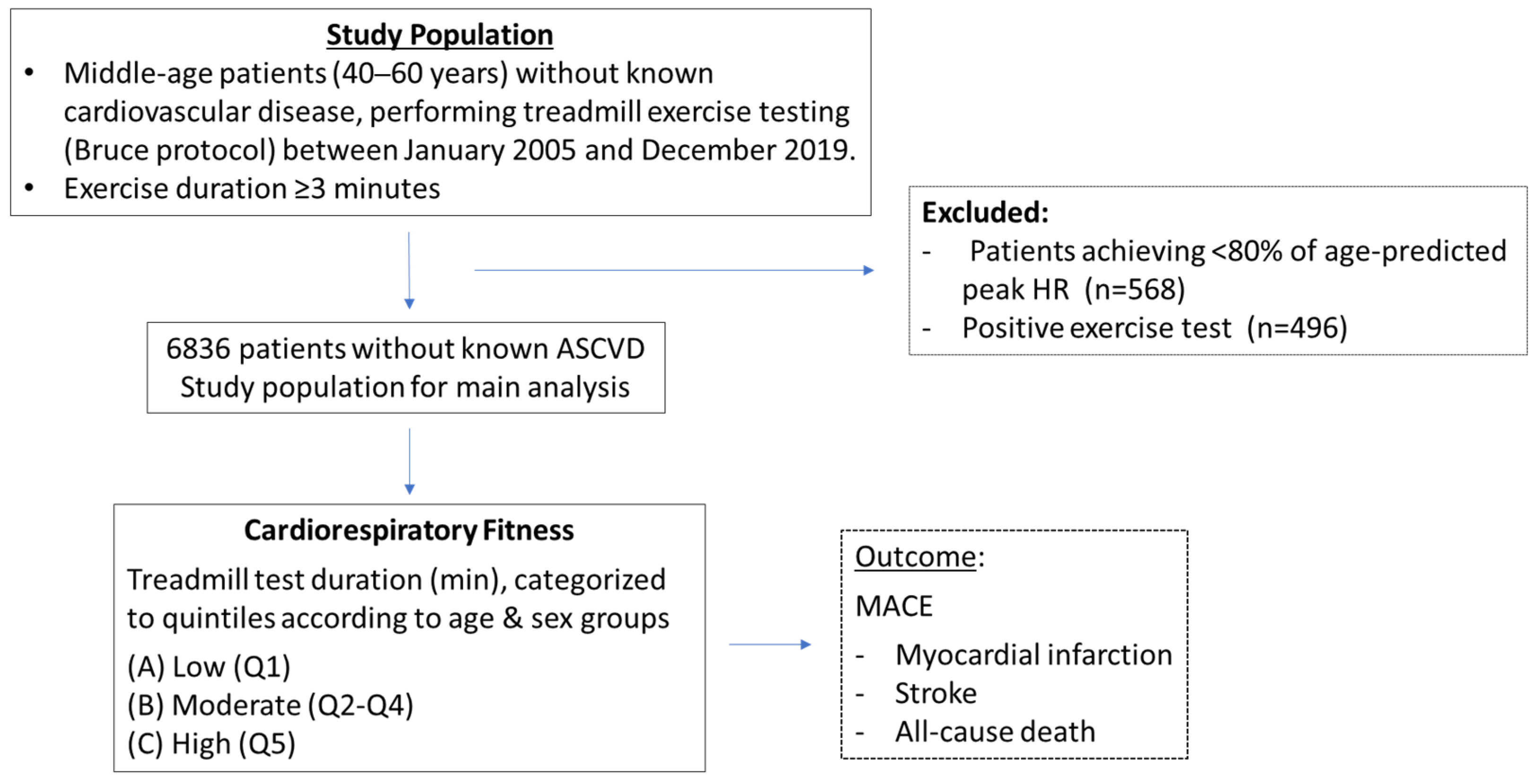
2.1. Study Population
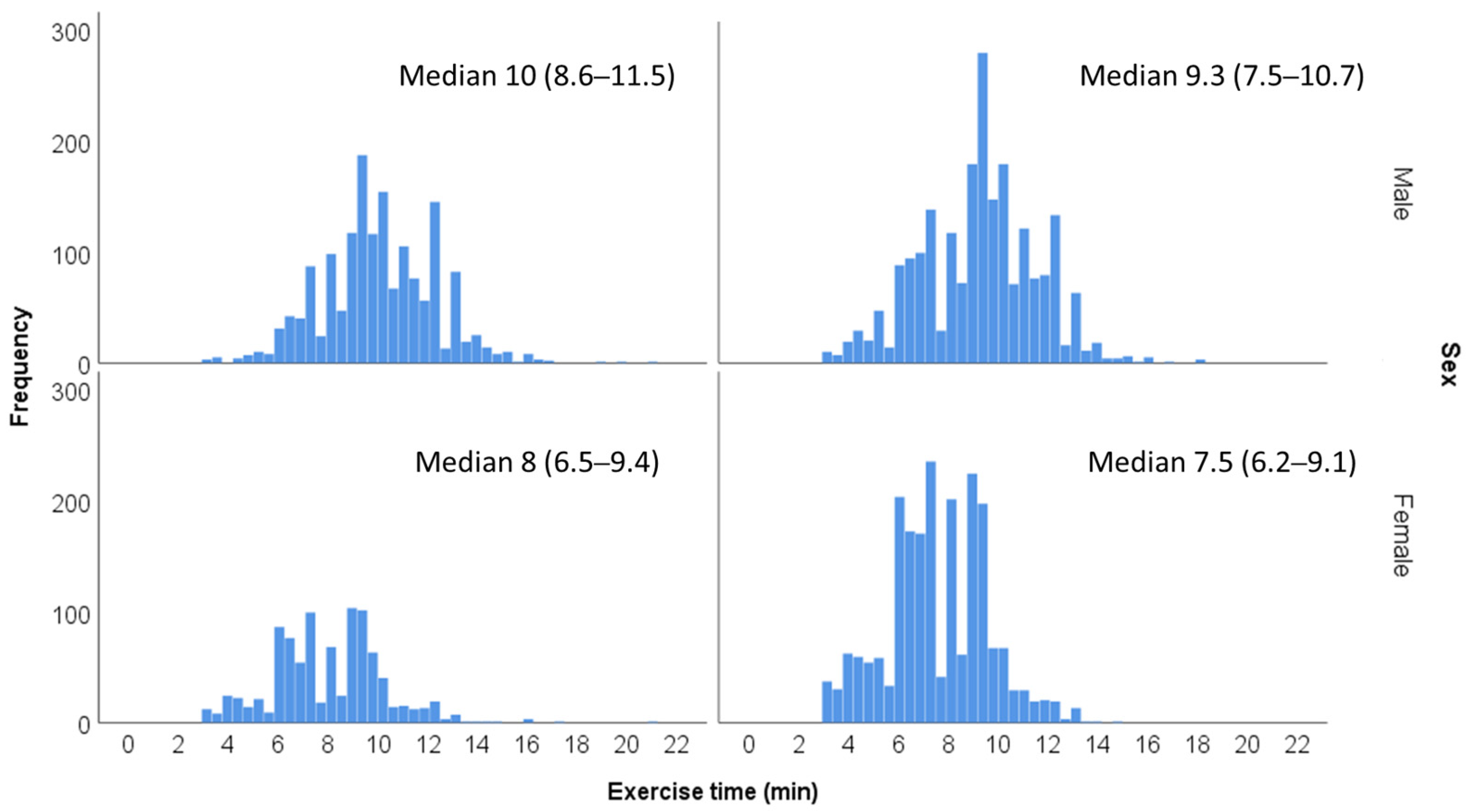
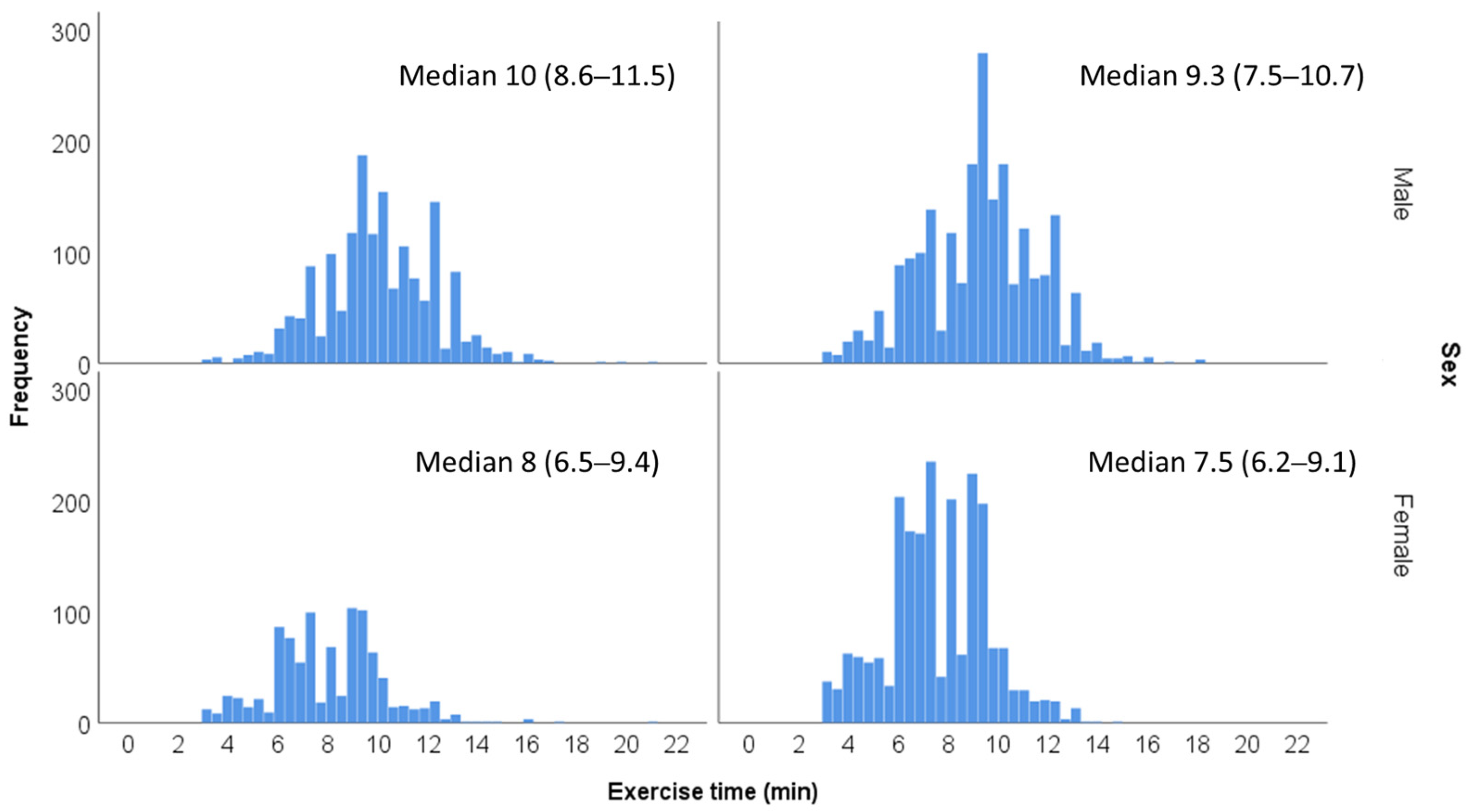
2.2. Exercise Stress Testing and Fitness Level
2.3. Data Analysis
3. Results
3.1. Patients Characteristics
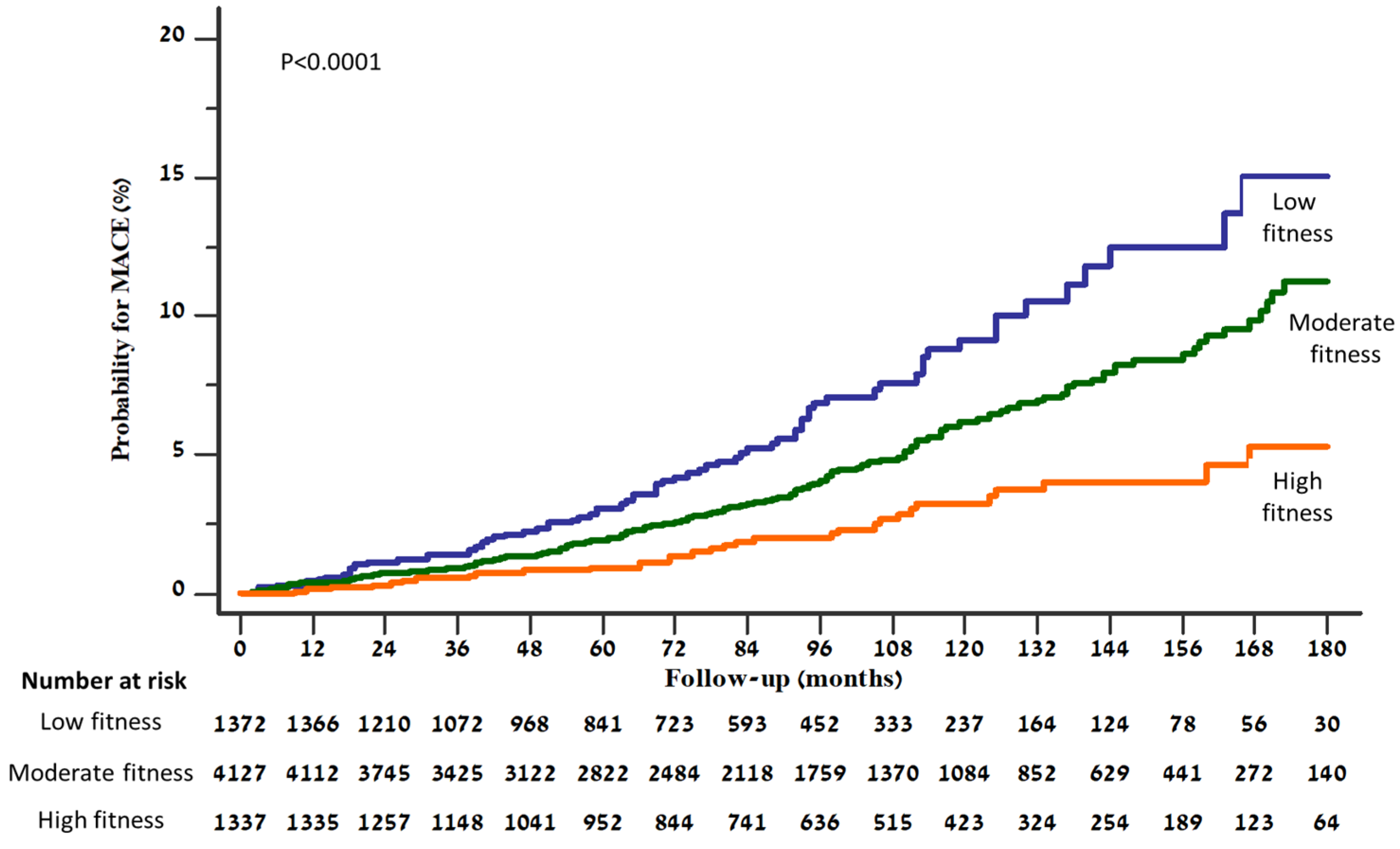
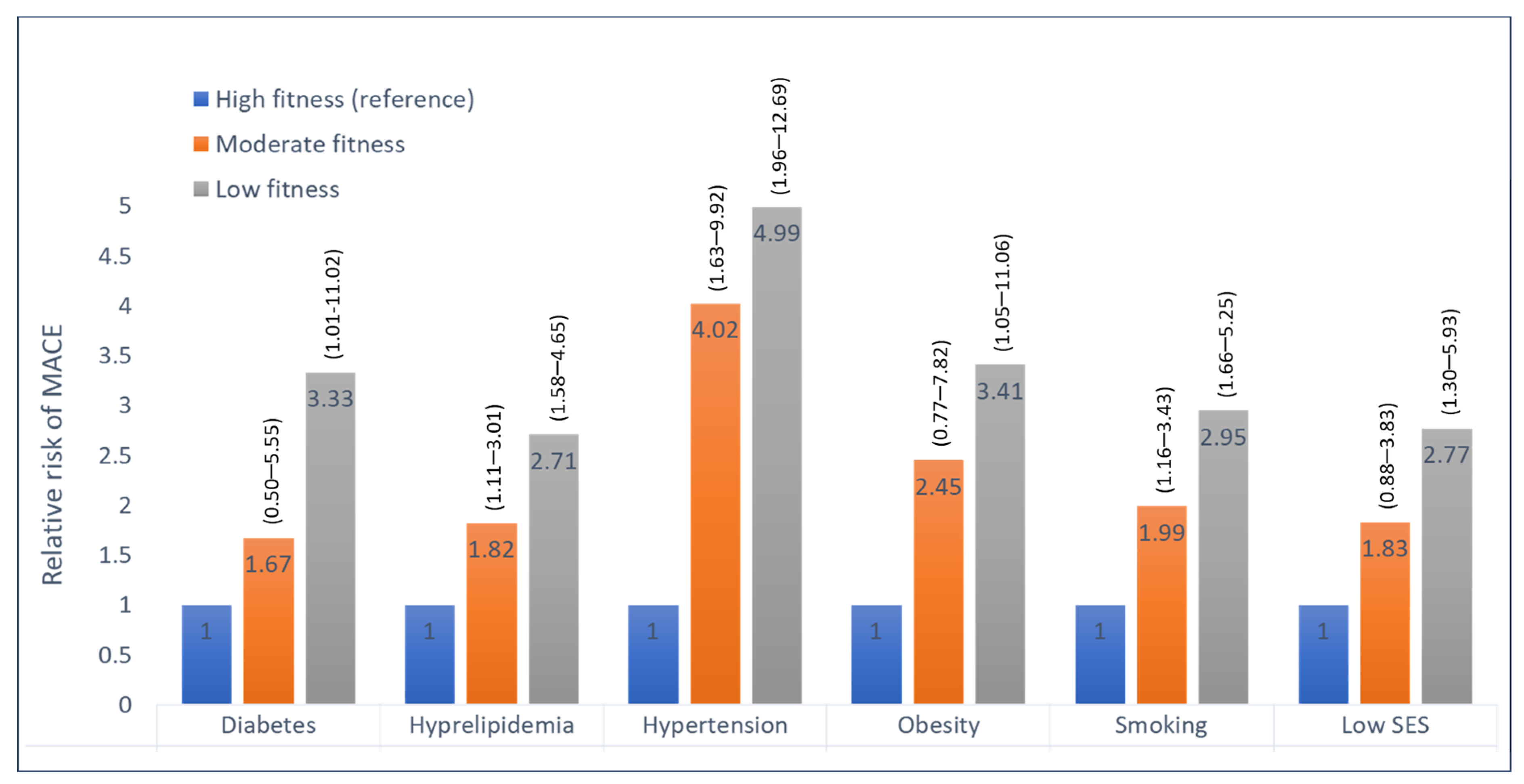
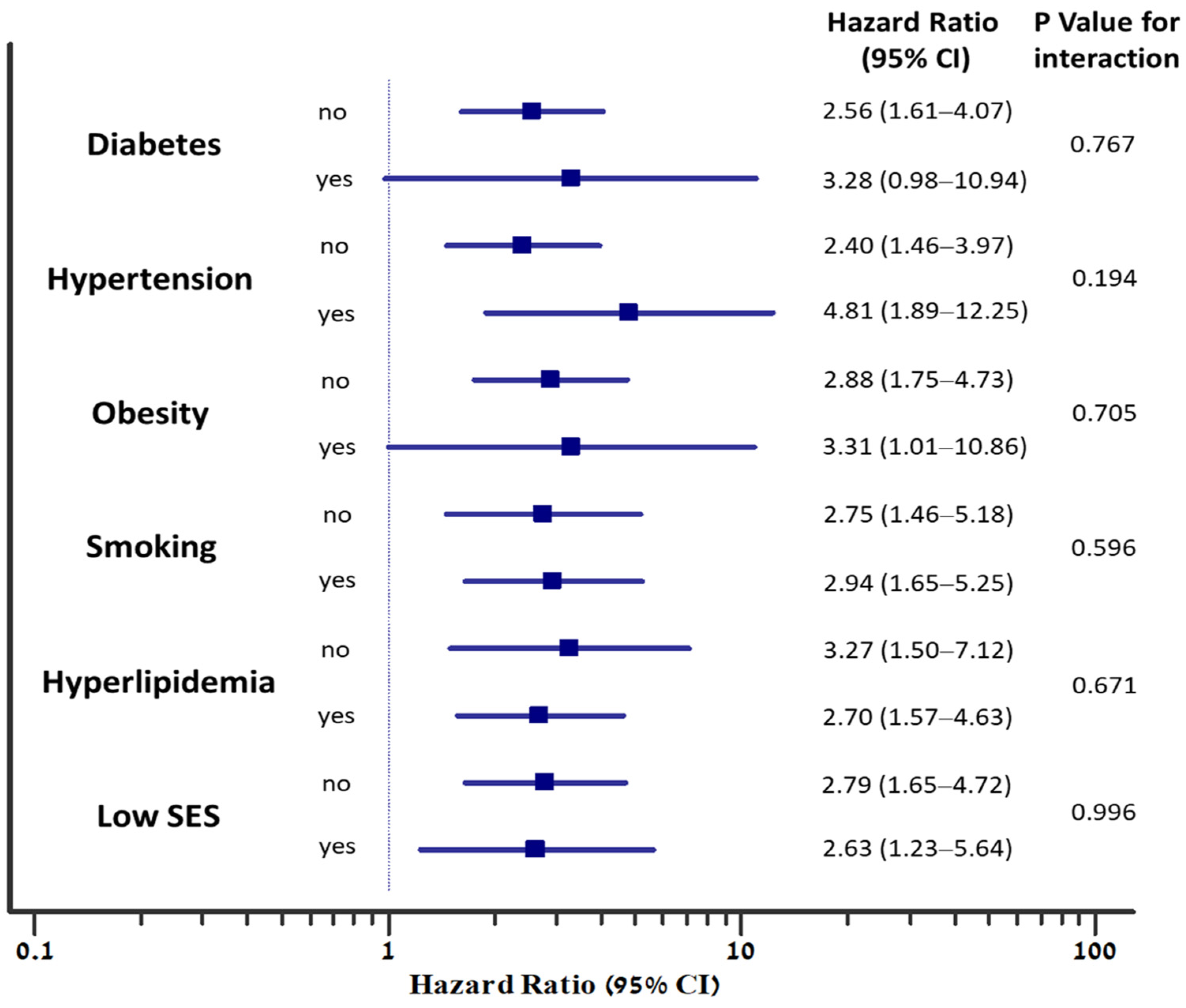
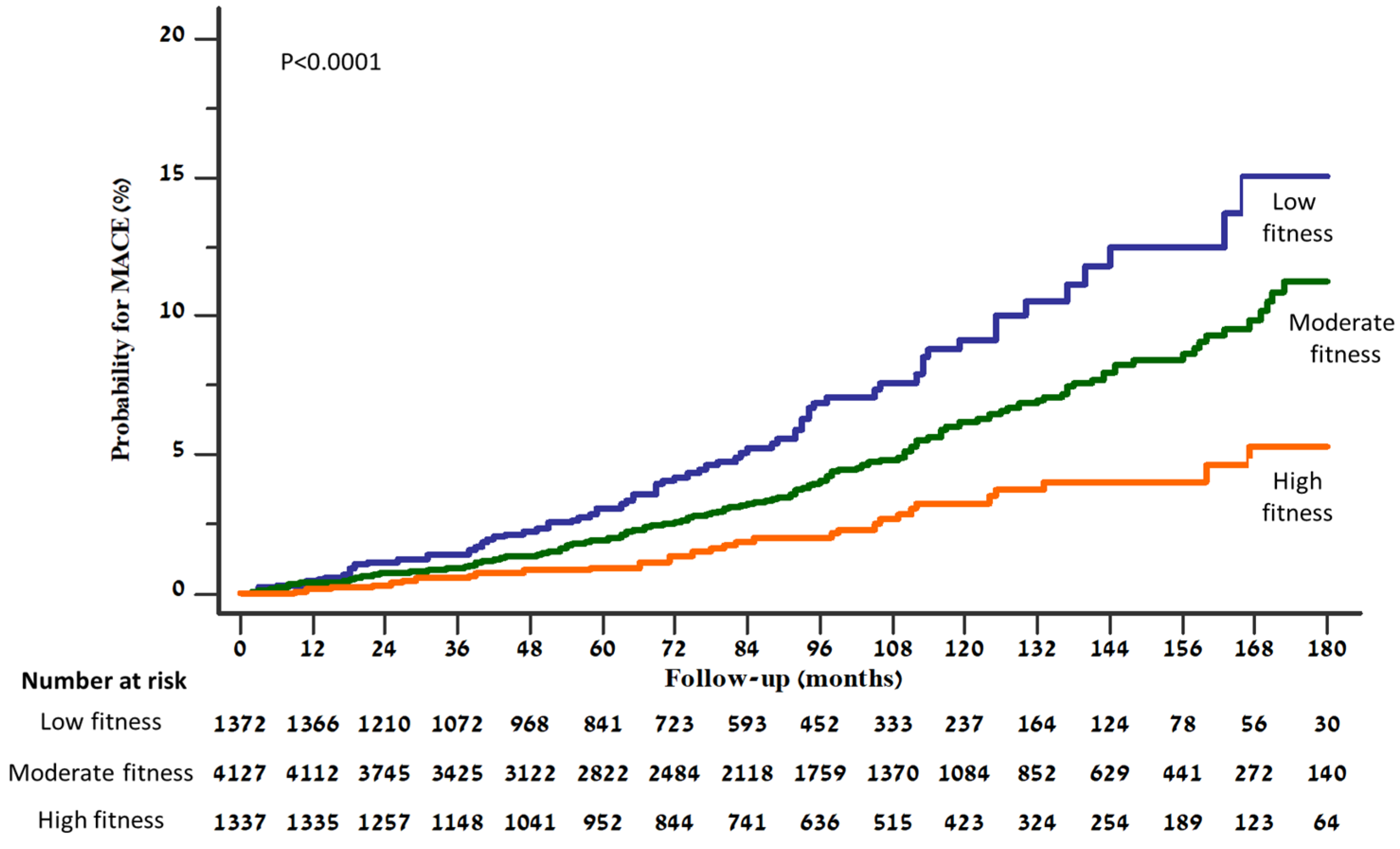
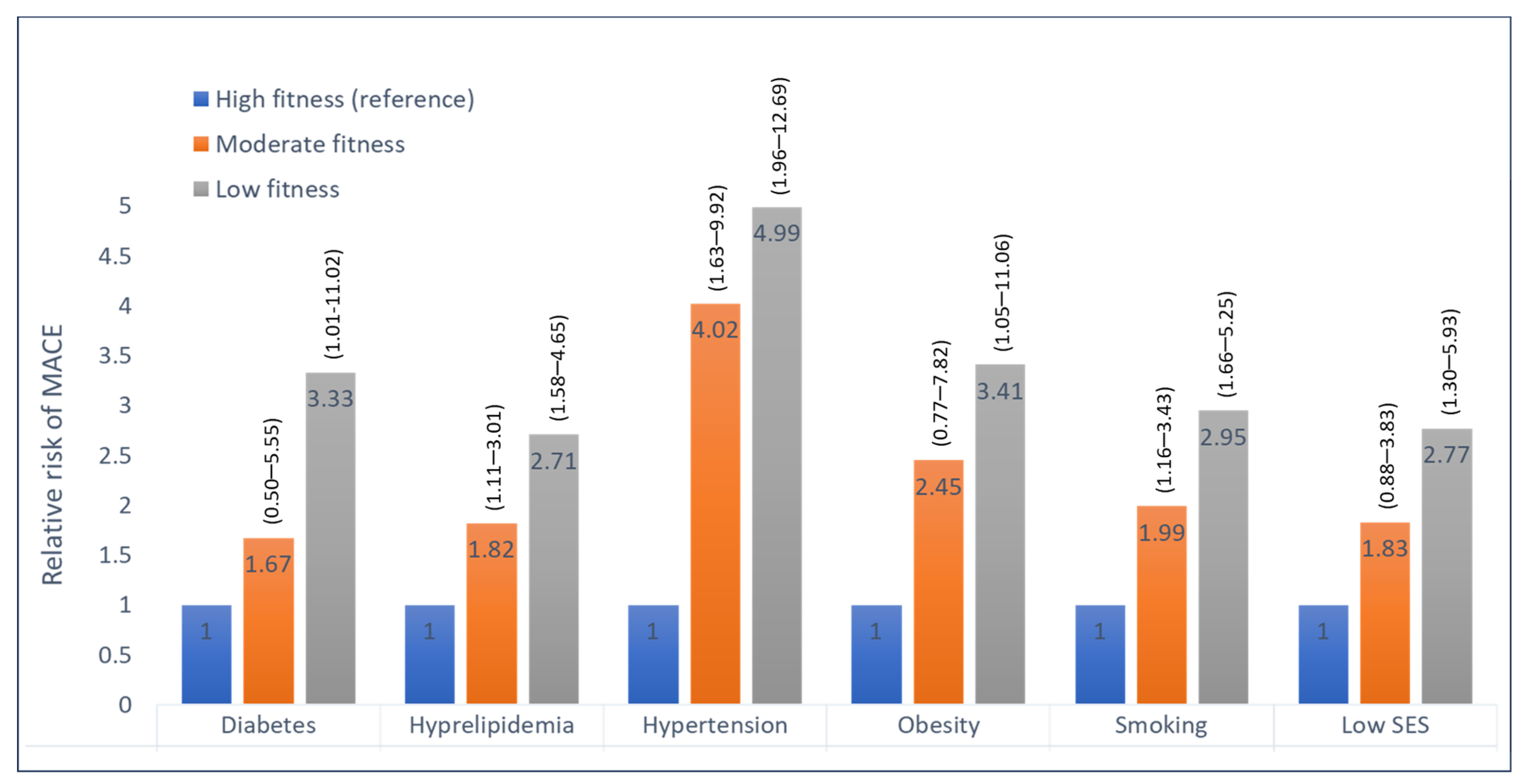
3.2. Fitness Level and Adverse Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fletcher, G.F.; Landolfo, C.; Niebauer, J.; Ozemek, C.; Arena, R.; Lavie, C.J. Promoting physical activity and exercise: JACC health promotion series. J. Am. Coll. Cardiol. 2018, 72, 1622–1639. [Google Scholar] [CrossRef]
- Lear, S.A.; Hu, W.; Rangarajan, S.; Gasevic, D.; Leong, D.; Iqbal, R.; Casanova, A.; Swaminathan, S.; Anjana, R.M.; Kumar, R.; et al. The effect of physical activity on mortality and cardiovascular disease in 130,000 people from 17 high-income, middle-income, and low-income countries: The PURE study. Lancet 2017, 390, 2643–2654. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, G.F.; Ades, P.A.; Kligfield, P.; Arena, R.; Balady, G.J.; Bittner, V.A.; Coke, L.A.; Fleg, J.L.; Forman, D.E.; Gerber, T.C.; et al. Exercise standards for testing and training: A scientific statement from the American Heart Association. Circulation 2013, 128, 873–934. [Google Scholar] [CrossRef] [PubMed]
- Zafrir, B. The prognostic value of exercise testing: Exercise capacity, hemodynamic response, and cardio-metabolic risk factors. Eur. J. Prev. Cardiol. 2017, 24, 1624–1626. [Google Scholar] [CrossRef] [PubMed]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Qie, R.; Shi, X.; Yang, Y.; Lu, J.; Hu, F.; Zhang, M.; Zhang, Z.; Hu, D.; Zhao, Y. Cardiorespiratory fitness and mortality from all causes, cardiovascular disease, and cancer: Dose-response meta-analysis of cohort studies. Br. J. Sports Med. 2022, 56, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, J.A.; Isiozor, N.M.; Kunutsor, S.K. Objectively assessed cardiorespiratory fitness and all-cause mortality risk: An updated meta-analysis of 37 cohort studies involving 2,258,029 participants. Mayo Clin. Proc. 2022, 97, 1054–1073. [Google Scholar] [CrossRef]
- Lavie, C.J.; Arena, R.; Kaminsky, L.A. Making the case to measure and improve cardiorespiratory fitness in routine clinical practice. Mayo Clin. Proc. 2022, 97, 1038–1040. [Google Scholar] [CrossRef]
- Pollock, M.L.; Bohannon, R.L.; Cooper, K.H.; Ayres, J.J.; Ward, A.; White, S.R.; Linnerud, A.C. A comparative analysis of four protocols for maximal treadmill stress testing. Am. Heart J. 1976, 92, 39–46. [Google Scholar] [CrossRef]
- Imboden, M.T.; Harber, M.P.; Whaley, M.H.; Finch, W.H.; Bishop, D.L.; Kaminsky, L.A. Cardiorespiratory fitness and mortality in healthy men and women. J. Am. Coll. Cardiol. 2018, 72, 2283–2292. [Google Scholar] [CrossRef] [PubMed]
- Erez, A.; Kivity, S.; Berkovitch, A.; Milwidsky, A.; Klempfner, R.; Segev, S.; Goldenberg, I.; Sidi, Y.; Maor, E. The association between cardiorespiratory fitness and cardiovascular risk may be modulated by known cardiovascular risk factors. Am. Heart. J. 2015, 169, 916–923.e1. [Google Scholar] [CrossRef] [PubMed]
- Ladenvall, P.; Persson, C.U.; Mandalenakis, Z.; Wilhelmsen, L.; Grimby, G.; Svärdsudd, K.; Hansson, P.O. Low aerobic capacity in middle-aged men associated with increased mortality rates during 45 years of follow-up. Eur. J. Prev. Cardiol. 2016, 23, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Rohatgi, A.; Ayers, C.R.; Willis, B.L.; Haskell, W.L.; Khera, A.; Drazner, M.H.; de Lemos, J.A.; Berry, J.D. Cardiorespiratory fitness and classification of risk of cardiovascular disease mortality. Circulation 2011, 123, 1377–1383. [Google Scholar] [CrossRef] [PubMed]
- Laukkanen, J.A.; Kunutsor, S.K.; Yates, T.; Willeit, P.; Kujala, U.M.; Khan, H.; Zaccardi, F. Prognostic Relevance of Cardiorespiratory Fitness as Assessed by Submaximal Exercise Testing for All-Cause Mortality: A UK Biobank Prospective Study. Mayo Clin. Proc. 2020, 95, 867–878. [Google Scholar] [CrossRef]
- Zafrir, B.; Azaiza, M.; Gaspar, T.; Dobrecky-Mery, I.; Azencot, M.; Lewis, B.S.; Rubinshtein, R.; Halon, D.A. Low cardiorespiratory fitness and coronary artery calcification: Complementary cardiovascular risk predictors in asymptomatic type 2 diabetics. Atherosclerosis 2015, 241, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Israel, A.; Kivity, S.; Sidi, Y.; Segev, S.; Berkovitch, A.; Klempfner, R.; Lavi, B.; Goldenberg, I.; Maor, E. Use of exercise capacity to improve SCORE risk prediction model in asymptomatic adults. Eur. Heart J. 2016, 37, 2300–2306. [Google Scholar] [CrossRef]
- Wilson, M.G.; Ellison, G.M.; Cable, N.T. Basic science behind the cardiovascular benefits of exercise. Heart 2015, 101, 758–765. [Google Scholar] [CrossRef]
- Joyner, M.J.; Green, D.J. Exercise protects the cardiovascular system: Effects beyond traditional risk factors. J. Physiol. 2009, 587, 5551–5558. [Google Scholar] [CrossRef]
- Lobelo, F.; Rohm Young, D.; Sallis, R.; Garber, M.D.; Billinger, S.A.; Duperly, J.; Hutber, A.; Pate, R.R.; Thomas, R.J.; Widlansky, M.E.; et al. Routine assessment and promotion of physical activity in healthcare settings: A scientific statement from the American Heart Association. Circulation 2018, 137, e495–e522. [Google Scholar] [CrossRef]
- Holtermann, A.; Marott, J.L.; Gyntelberg, F.; Søgaard, K.; Mortensen, O.S.; Prescott, E.; Schnohr, P. Self-reported cardiorespiratory fitness: Prediction and classification of risk of cardiovascular disease mortality and longevity–a prospective investigation in the Copenhagen City Heart Study. J. Am. Heart Assoc. 2015, 4, e001495. [Google Scholar] [CrossRef]
- Lodi, E.; Rodighiero, E.; Donati, F.; Pergreffi, M.; D’Antonio, L.; Guicciardi, C.; Morales, J.R.; Lodi, G.; Modena, M.G. Sex and physical exercise: One only size does not fit all. Differences between men and women in regulation and adaptations in response to exercise. Ital. J. Gender-Specific Med. 2022, 8, 163–171. [Google Scholar]
- Loef, M.; Walach, H. The combined effects of healthy lifestyle behaviors on all-cause mortality: A systematic review and meta-analysis. Prev. Med. 2012, 55, 163–170. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 6836) | Low Fitness (n = 1372) | Moderate Fitness (n = 4127) | High Fitness (n = 1337) | p Value |
|---|---|---|---|---|---|
| Age (years) | 51.9 ± 5.9 | 52.3 ± 5.9 | 51.9 ± 5.9 | 51.4 ± 5.9 | 0.001 |
| Sex (Female) | 3040 (44.5%) | 610 (44.5%) | 1828 (44.3%) | 602 (45%) | 0.896 |
| Socioeconomic status (Low) | 2372 (34.7%) | 655 (47.7%) | 1429 (34. 6%) | 288 (21.5%) | <0.001 |
| Body Mass Index (BMI) | 27.9 ± 4.9 | 30.4 ± 5.6 | 27.9 ± 4.6 | 25.2 ± 3.4 | <0.001 |
| Obesity | 1905 (27.9%) | 661 (48.2%) | 1147 (27.8%) | 97 (7.3%) | <0.001 |
| Current smoking | 2973 (43.5%) | 688 (50.1%) | 1787 (43.3%) | 498 (37.2%) | <0.001 |
| Hyperlipidemia | 3506 (51.3%) | 805 (58.7%) | 2104 (51%) | 597 (44.7%) | <0.001 |
| Hypertension | 1947 (28.5%) | 543 (39.6%) | 1177 (28.5%) | 227 (17%) | <0.001 |
| Diabetes mellitus | 860 (12.6%) | 311 (22.7%) | 482 (11.7%) | 67 (5%) | <0.001 |
| Chronic Kidney Disease | 79 (1.2%) | 23 (1.7%) | 44 (1.1%) | 12 (0.9%) | 0.115 |
| COPD | 100 (1.5%) | 37 (2.7%) | 53 (1.3%) | 10 (0.7%) | <0.001 |
| Beta blockers | 915 (13.4%) | 267 (19.5%) | 535 (13%) | 113 (8.5%) | <0.001 |
| Anti-hypertensive drugs | 2086 (30.5%) | 584 (42.6%) | 1245 (30.2%) | 257 (19.2%) | <0.001 |
| Statins | 2176 (31.8%) | 516 (37.6%) | 1314 (31.8%) | 346 (25.9%) | <0.001 |
| Exercise testing parameters | |||||
| Exercise duration (min) | 8.8 ± 2.4 | 5.7 ± 1.3 | 8.8 ± 1.4 | 11.8 ± 1.7 | <0.001 |
| Resting heart rate (BPM) | 81 ± 13 | 87 ± 14 | 81 ± 13 | 75 ± 12 | <0.001 |
| Peak heart rate (bpm) | 159 ± 13 | 154 ± 13 | 158 ± 13 | 163 ± 12 | <0.001 |
| Peak METs | 10.7 ± 2.4 | 7.7 ± 1.3 | 10.7 ± 1.4 | 13.7 ± 1.7 | <0.001 |
| Systolic BP—rest | 118 ± 15 | 125 ± 15 | 118 ± 15 | 112 ± 14 | <0.001 |
| Systolic BP—peak | 162 ± 22 | 167 ± 24 | 162 ± 21 | 156 ± 21 | <0.001 |
| Fitness Level | Proportion with Event | Rate Per 1000 Person-Years | Age- and Gender- Adjusted HR | Multivariable * Adjusted HR |
|---|---|---|---|---|
| MACE | ||||
| High Fitness | 32/1337 (2.4%) | 3.02 | Ref. | Ref. |
| Moderate Fitness | 181/4127 (4.4%) | 5.91 | 1.98 (1.36–2.88) p < 0.001 | 1.65 (1.12–2.44) p = 0.011 |
| Low Fitness | 76/1372 (5.5%) | 8.45 | 3.04 (2.01–4.61) p < 0.001 | 2.17 (1.40–3.38) p < 0.001 |
| For each decrease in 1-MET | 1.21 (1.15–1.28) p < 0.001 | 1.18 (1.12–1.25) p < 0.001 | ||
| All-cause Death | ||||
| High Fitness | 10/1337 (0.7%) | 0.94 | Ref. | Ref. |
| Moderate Fitness | 71/4127 (1.7%) | 2.28 | 2.47 (1.27–4.79) p = 0.007 | 2.32 (1.15–4.67) p = 0.019 |
| Low Fitness | 37/1372 (2.7%) | 4.06 | 4.75 (2.36–9.57) p < 0.001 | 4.45 (2.13–9.33) p < 0.001 |
| For each decrease in 1-MET | 1.30 (1.19–1.42) p < 0.001 | 1.29 (1.18–1.41) p < 0.001 | ||
| Myocardial Infarction or Stroke | ||||
| High Fitness | 23/1337 (1.7%) | 2.17 | Ref. | Ref. |
| Moderate Fitness | 113/4127 (2.7%) | 3.69 | 1.72 (1.10–2.69) p = 0.018 | 1.63 (1.03–2.57) p = 0.037 |
| Low Fitness | 43/1372 (3.1%) | 4.78 | 2.38 (1.43–3.96) p < 0.001 | 1.96 (1.16–3.31) p = 0.012 |
| For each decrease in 1 MET | 1.16 (1.09–1.24) p < 0.001 | 1.13 (1.06–1.21) p = 0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aker, A.; Saliba, W.; Bahouth, F.; Naoum, I.; Zafrir, B. Cardiorespiratory Fitness and Risk of Cardiovascular Events and Mortality in Middle Age Patients without Known Cardiovascular Disease. J. Clin. Med. 2023, 12, 7011. https://doi.org/10.3390/jcm12227011
Aker A, Saliba W, Bahouth F, Naoum I, Zafrir B. Cardiorespiratory Fitness and Risk of Cardiovascular Events and Mortality in Middle Age Patients without Known Cardiovascular Disease. Journal of Clinical Medicine. 2023; 12(22):7011. https://doi.org/10.3390/jcm12227011
Chicago/Turabian StyleAker, Amir, Walid Saliba, Fadel Bahouth, Ibrahim Naoum, and Barak Zafrir. 2023. "Cardiorespiratory Fitness and Risk of Cardiovascular Events and Mortality in Middle Age Patients without Known Cardiovascular Disease" Journal of Clinical Medicine 12, no. 22: 7011. https://doi.org/10.3390/jcm12227011
APA StyleAker, A., Saliba, W., Bahouth, F., Naoum, I., & Zafrir, B. (2023). Cardiorespiratory Fitness and Risk of Cardiovascular Events and Mortality in Middle Age Patients without Known Cardiovascular Disease. Journal of Clinical Medicine, 12(22), 7011. https://doi.org/10.3390/jcm12227011