
Increased Serum Levels of Phoenixin-14, Nesfatin-1 and Dopamine Are Associated with Positive Pregnancy Rate after Ovarian Stimulation



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethics
2.3. Study Participants
- Age < 40 years old.
- Infertility diagnosed as the failure to conceive after 6 months (for women < 40 years old) or one year (for women <35 years old) of regular intercourse without contraception.
- PCOS was diagnosed based on the Rotterdam PCOS Diagnostic Criteria (at least two of oligo- or anovulation, clinical and/or biochemical hyperandrogenism, or polycystic ovaries on ultrasound), after the exclusion of related disorders.
- Excluded fallopian tube obstruction by hysterosalpingography.
- Confirmed suitable sperm quality (per WHO 2021 guidelines).
- The exclusion criteria included the following:
- Poor ovarian response (POR): (1) advanced maternal age ≥ 40 years or any other risk factor for POR; (2) an abnormal ovarian reserve test (i.e., antral follicle count; AFC < 5–7 follicles or anti-Müllerian hormone levels; AMH < 0.5–1.1 ng/mL).
- Use of hormonal therapy within 3 months before OS: oral contraceptives or dienogest therapy (due to endometriosis).
- Concomitant diseases: severe hypertension, diabetes mellitus, known malignancy, any chronic inflammatory diseases (e.g., rheumatoid arthritis) or signs of an acute infection, advanced chronic renal disease (estimated glomerular filtration rate (eGFR) < 30 mL/min), or international normalized ratio (INR) more than 1.2 at the day of blood draw.
- Endometriosis stages III or more according to the revised American Society for Reproductive Medicine score (rASRM).
2.4. Ovarian Stimulation
2.5. Blood Sampling and Analyses
2.6. Data Management and Statistical Analyses
3. Results
3.1. Participants’ Characteristics
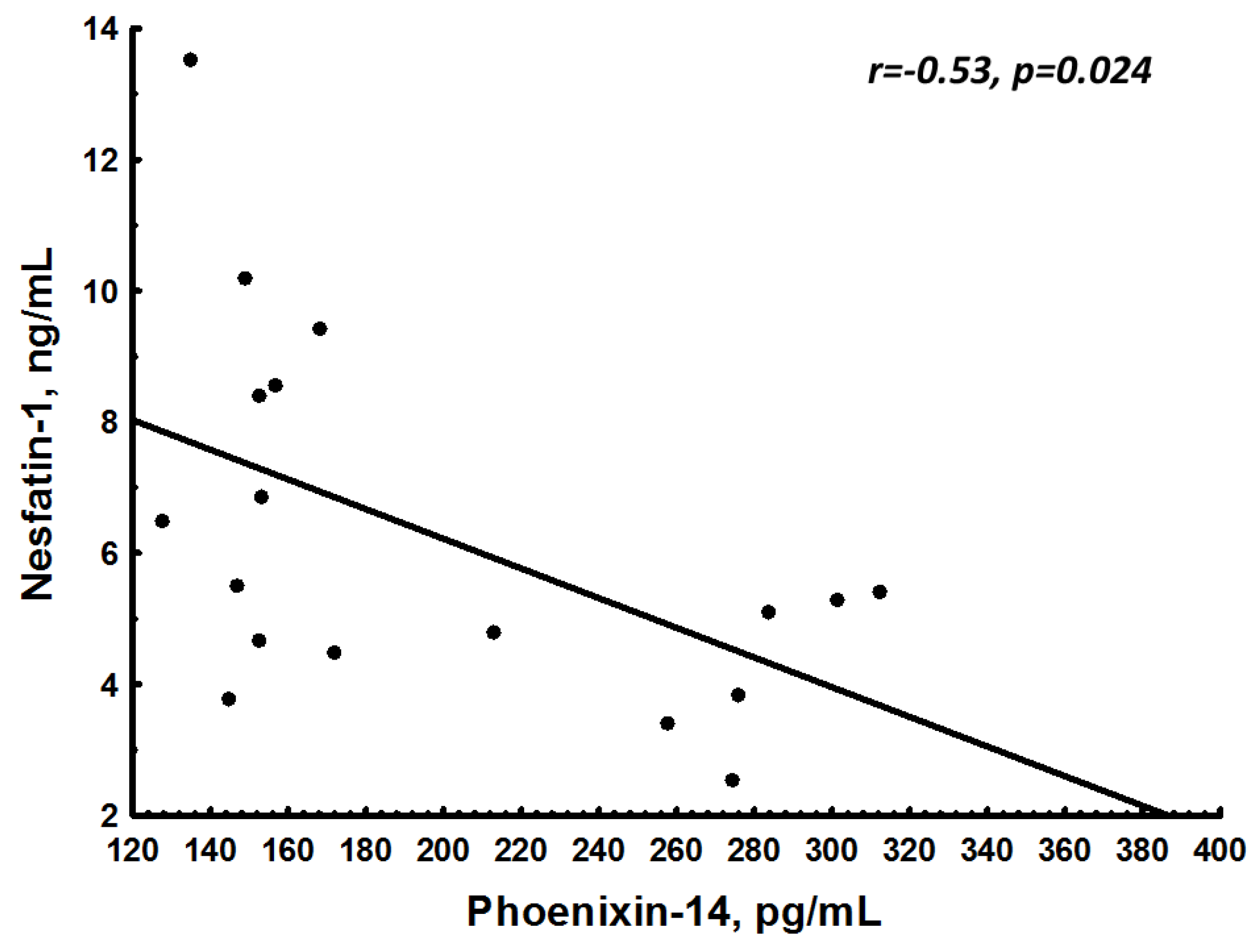
3.2. Neuropeptides before OS
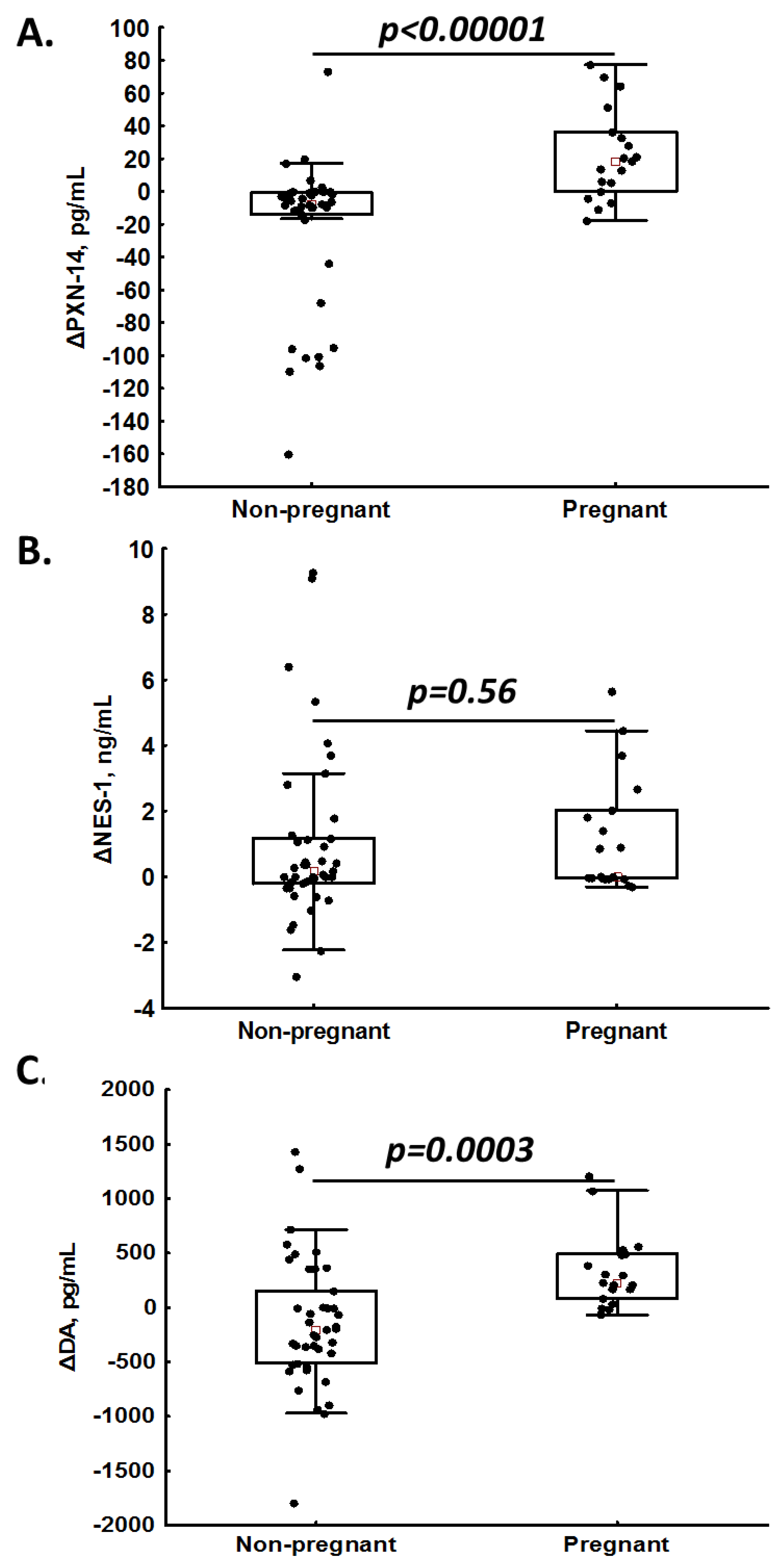
3.3. Post-Stimulation Changes in Neuropeptide Levels
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Inhorn, M.C.; Patrizio, P. Infertility around the globe: New thinking on gender, reproductive technologies and global movements in the 21st century. Hum. Reprod. Update 2015, 21, 411–426. [Google Scholar] [CrossRef]
- Wasilewski, T.; Łukaszewicz-Zając, M.; Wasilewska, J.; Mroczko, B. Biochemistry of infertility. Clin. Chim. Acta 2020, 508, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Pałasz, A.; Rojczyk, E.; Bogus, K.; Worthington, J.J.; Wiaderkiewicz, R. The novel neuropeptide phoenixin is highly co-expressed with nesfatin-1 in the rat hypothalamus, an immunohistochemical study. Neurosci. Lett. 2015, 592, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Szeliga, A.; Rudnicka, E.; Maciejewska-Jeske, M.; Kucharski, M.; Kostrzak, A.; Hajbos, M.; Niwczyk, O.; Smolarczyk, R.; Meczekalski, B. Neuroendocrine Determinants of Polycystic Ovary Syndrome. Int. J. Environ. Res. Public Health 2022, 19, 3089. [Google Scholar] [CrossRef] [PubMed]
- Kalamon, N.; Błaszczyk, K.; Szlaga, A.; Billert, M.; Skrzypski, M.; Pawlicki, P.; Górowska-Wójtowicz, E.; Kotula-Balak, M.; Błasiak, A.; Rak, A. Levels of the neuropeptide phoenixin-14 and its receptor GRP173 in the hypothalamus, ovary and periovarian adipose tissue in rat model of polycystic ovary syndrome. Biochem. Biophys. Res. Commun. 2020, 528, 628–635. [Google Scholar] [CrossRef]
- Ullah, K.; Ur Rahman, T.; Wu, D.D.; Lin, X.H.; Liu, Y.; Guo, X.Y.; Leung, P.C.K.; Zhang, R.J.; Huang, H.F.; Sheng, J.Z. Phoenixin-14 concentrations are increased in association with luteinizing hormone and nesfatin-1 concentrations in women with polycystic ovary syndrome. Clin. Chim. Acta 2017, 471, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Hatef, A.; Unniappan, S. Gonadotropin-releasing hormone, kisspeptin, and gonadal steroids directly modulate nucleobindin-2/nesfatin-1 in murine hypothalamic gonadotropin-releasing hormone neurons and gonadotropes. Biol. Reprod. 2017, 96, 635–651. [Google Scholar] [CrossRef]
- Prinz, P.; Scharner, S.; Friedrich, T.; Schalla, M.; Goebel-Stengel, M.; Rose, M.; Stengel, A. Central and peripheral expression sites of phoenixin-14 immunoreactivity in rats. Biochem. Biophys. Res. Commun. 2017, 493, 195–201. [Google Scholar] [CrossRef]
- Goebel, M.; Stengel, A.; Wang, L.; Lambrecht, N.W.; Taché, Y. Nesfatin-1 immunoreactivity in rat brain and spinal cord autonomic nuclei. Neurosci. Lett. 2009, 452, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Foo, K.S.; Brismar, H.; Broberger, C. Distribution and neuropeptide coexistence of nucleobindin-2 mRNA/nesfatin-like immunoreactivity in the rat CNS. Neuroscience 2008, 156, 563–579. [Google Scholar] [CrossRef] [PubMed]
- Hamed, E.A.; Sayyed, H.G.; Abbas, A.M.; Gaber, M.M.A.; Aleem, H.M.A.E. Nesfatin-1, Dopamine, and NADPH levels in Infertile Women with Polycystic Ovary Syndrome: Is There a Relationship between Their Levels and Metabolic and Hormonal Variables. J. Reprod. Infertil. 2022, 23, 160–168. [Google Scholar] [CrossRef]
- Jahromi, B.N.; Dabbaghmanesh, M.H.; Bakhshaie, P.; Parsanezhad, M.E.; Anvar, Z.; Alborzi, M.; Zarei, A.; Bakhshaei, M. Assessment of oxytocin level, glucose metabolism components and cutoff values for oxytocin and anti-mullerian hormone in infertile PCOS women. Taiwan J. Obstet. Gynecol. 2018, 57, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Parillo, F.; Maranesi, M.; Mignini, F.; Marinelli, L.; Di Stefano, A.; Boiti, C.; Zerani, M. Evidence for a dopamine intrinsic direct role in the regulation of the ovary reproductive function: In vitro study on rabbit corpora lutea. PLoS ONE 2014, 9, e104797. [Google Scholar] [CrossRef]
- Hernández, I.; Parra, A.; Méndez, I.; Cabrera, V.; Cravioto, M.C.; Mercado, M.; Díaz-Sánchez, V.; Larrea, F. Hypothalamic dopaminergic tone and prolactin bioactivity in women with polycystic ovary syndrome. Arch. Med. Res. 2000, 31, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Henderson, H.L.; Townsend, J.; Tortonese, D.J. Direct effects of prolactin and dopamine on the gonadotroph response to GnRH. J. Endocrinol. 2008, 197, 343–350. [Google Scholar] [CrossRef]
- Ho, J.M.; Blevins, J.E. Coming full circle: Contributions of central and peripheral oxytocin actions to energy balance. Endocrinology 2013, 154, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Stubbendorff, C.; Stevenson, C.W. Dopamine regulation of contextual fear and associated neural circuit function. Eur. J. Neurosci. 2021, 54, 6933–6947. [Google Scholar] [CrossRef]
- Amer, S.A.; Smith, J.; Mahran, A.; Fox, P.; Fakis, A. Double-blind randomized controlled trial of letrozole versus clomiphene citrate in subfertile women with polycystic ovarian syndrome. Hum. Reprod. 2017, 32, 1631–1638. [Google Scholar] [CrossRef] [PubMed]
- Franik, S.; Eltrop, S.M.; Kremer, J.A.; Kiesel, L.; Farquhar, C. Aromatase inhibitors (letrozole) for subfertile women with polycystic ovary syndrome. Cochrane Database Syst. Rev. 2018, 5, CD010287. [Google Scholar] [CrossRef] [PubMed]
- Quaas, A.M.; Gavrizi, S.Z.; Peck, J.D.; Diamond, M.P.; Legro, R.S.; Robinson, R.D.; Casson, P.; Christman, G.M.; Zhang, H.; Hansen, K.R.; et al. Endometrial thickness after ovarian stimulation with gonadotropin, clomiphene, or letrozole for unexplained infertility, and association with treatment outcomes. Fertil. Steril. 2020, 115, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. (2) Classification and diagnosis of diabetes. Diabetes Care 2015, 38 (Suppl. 1), S8–S16. [Google Scholar] [CrossRef]
- Yosten, G.L.; Lyu, R.M.; Hsueh, A.J.; Avsian-Kretchmer, O.; Chang, J.K.; Tullock, C.W.; Dun, S.L.; Dun, N.; Samson, W.K. A novel reproductive peptide, phoenixin. J. Neuroendocrinol. 2013, 25, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, T.; Stengel, A. Role of the Novel Peptide Phoenixin in Stress Response and Possible Interactions with Nesfatin-1. Int. J. Mol. Sci. 2021, 22, 9156. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Du, Y.; Han, X.; Wang, H.; Sheng, Y.; Lian, F.; Lian, Q. Efficacy of atosiban for repeated implantation failure in frozen embryo transfer cycles. Sci. Rep. 2023, 13, 9277. [Google Scholar] [CrossRef]
- Chou, P.Y.; Wu, M.H.; Pan, H.A.; Hung, K.H.; Chang, F.M. Use of an oxytocin antagonist in in vitro fertilization-embryo transfer for women with repeated implantation failure: A retrospective study. Taiwan J. Obstet. Gynecol. 2011, 50, 136–140. [Google Scholar] [CrossRef]
- Pierzynski, P. Oxytocin and vasopressin V(1A) receptors as new therapeutic targets in assisted reproduction. Reprod. Biomed. Online 2011, 22, 9–16. [Google Scholar] [CrossRef]
- Xia, T.; Liu, Q.; Ye, Q.; Xing, W.; Wang, D.; Li, J.; Zang, Z.J. Serum oxytocin profiles in patients with repeated implantation failure during IVF cycles. Gynecol. Endocrinol. 2018, 34, 1048–1052. [Google Scholar] [CrossRef]
- Kiss, A.; Mikkelsen, J.D. Oxytocin—Anatomy and functional assignments: A minireview. Endocr. Regul. 2005, 39, 97–105. [Google Scholar] [PubMed]
- Tachibana, A.; Yamamoto, Y.; Noguchi, H.; Takeda, A.; Tamura, K.; Aoki, H.; Minato, S.; Uchishiba, M.; Yamamoto, S.; Kamada, S.; et al. Changes in Serum Oxytocin Levels under Physiological and Supraphysiological Gonadal Steroid Hormone Conditions in Women of Reproductive Age: A Preliminary Study. Nutrients 2022, 14, 5350. [Google Scholar] [CrossRef]
- Liu, X.; Herbison, A.E. Dopamine regulation of gonadotropin-releasing hormone neuron excitability in male and female mice. Endocrinology 2013, 154, 340–350. [Google Scholar] [CrossRef]
- Lee, S.; Jung, J.; An, S.; Lee, K.; Park, J.; Yang, H. Nesfatin-1 level in follicular fluid (FF) is associated with the number of retrieved oocyte in IVF cycle. In Human Reproduction; Oxford University Press: Oxford, UK, 2015; pp. 415–416. [Google Scholar]
- Varlı, B.; Şükür, Y.E.; Özmen, B.; Ergüder, B.; Sönmezer, M.; Berker, B.; Atabekoğlu, C.; Aytaç, R. Anorexigenic peptide (leptin, obestatin, nesfatin-1) levels and their impact on assisted reproductive technology treatment outcomes in patients with polycystic ovary syndrome. Clin. Exp. Reprod. Med. 2021, 48, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Ademoglu, E.N.; Gorar, S.; Carlıoglu, A.; Yazıcı, H.; Dellal, F.D.; Berberoglu, Z.; Akdeniz, D.; Uysal, S.; Karakurt, F. Plasma nesfatin-1 levels are increased in patients with polycystic ovary syndrome. J. Endocrinol. Investig. 2014, 37, 715–719. [Google Scholar] [CrossRef] [PubMed]
- Sahin, F.K.; Sahin, S.B.; Ural, U.M.; Cure, M.C.; Senturk, S.; Tekin, Y.B.; Balik, G.; Cure, E.; Yuce, S.; Kirbas, A. Nesfatin-1 and Vitamin D levels may be associated with systolic and diastolic blood pressure values and hearth rate in polycystic ovary syndrome. Bosn. J. Basic Med. Sci. 2015, 15, 57–63. [Google Scholar] [CrossRef]
- Deniz, R.; Gurates, B.; Aydin, S.; Celik, H.; Sahin, I.; Baykus, Y.; Catak, Z.; Aksoy, A.; Citil, C.; Gungor, S. Nesfatin-1 and other hormone alterations in polycystic ovary syndrome. Endocrine 2012, 42, 694–699. [Google Scholar] [CrossRef]
- Li, Q.C.; Wang, H.Y.; Chen, X.; Guan, H.Z.; Jiang, Z.Y. Fasting plasma levels of nesfatin-1 in patients with type 1 and type 2 diabetes mellitus and the nutrient-related fluctuation of nesfatin-1 level in normal humans. Regul. Pept. 2010, 159, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Demir Çaltekin, M.; Caniklioğlu, A.; Eris Yalçın, S.; Aydoğan Kırmızı, D.; Baser, E.; Yalvaç, E.S. DLK1 and Nesfatin-1 levels and the relationship with metabolic parameters in polycystic ovary syndrome: Prospective, controlled study. Turk. J. Obstet. Gynecol. 2021, 18, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhang, H.; Li, Q.; Lao, K.; Wang, Y. The role of nesfatin-1 expression in letrozole-induced polycystic ovaries in the rat. Gynecol. Endocrinol. 2017, 33, 438–441. [Google Scholar] [CrossRef]
- Gonzalez, R.; Perry, R.L.; Gao, X.; Gaidhu, M.P.; Tsushima, R.G.; Ceddia, R.B.; Unniappan, S. Nutrient responsive nesfatin-1 regulates energy balance and induces glucose-stimulated insulin secretion in rats. Endocrinology 2011, 152, 3628–3637. [Google Scholar] [CrossRef]
- Catak, Z.; Yavuzkir, S.; Kocdemir, E.; Ugur, K.; Yardim, M.; Sahin, İ.; Agirbas, E.P.; Aydin, S. NUCB2/Nesfatin-1 in the Blood and Follicular Fluid in Patients with Polycystic Ovary Syndrome and Poor Ovarian Response. J. Reprod. Infertil. 2019, 20, 225–230. [Google Scholar]
- Alp, E.; Görmüş, U.; Güdücü, N.; Bozkurt, S. Nesfatin-1 levels and metabolic markers in polycystic ovary syndrome. Gynecol. Endocrinol. 2015, 31, 543–547. [Google Scholar] [CrossRef]
- García-Galiano, D.; Navarro, V.M.; Roa, J.; Ruiz-Pino, F.; Sánchez-Garrido, M.A.; Pineda, R.; Castellano, J.M.; Romero, M.; Aguilar, E.; Gaytán, F.; et al. The anorexigenic neuropeptide, nesfatin-1, is indispensable for normal puberty onset in the female rat. J. Neurosci. 2010, 30, 7783–7792. [Google Scholar] [CrossRef] [PubMed]
- Chung, Y.; Kim, H.; Im, E.; Kim, P.; Yang, H. Th 17 Cells and Nesfatin-1 are associated with Spontaneous Abortion in the CBA/j × DBA/2 Mouse Model. Dev. Reprod. 2015, 19, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Sun, S.; Lee, D.; Youk, H.; Yang, H. Gonadotropin regulates NUCB2/nesfatin-1 expression in the mouse ovary and uterus. Biochem. Biophys. Res. Commun. 2019, 513, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Dong, J.; Jiao, Q.; Du, X.; Bi, M.; Jiang, H. “Sibling” battle or harmony: Crosstalk between nesfatin-1 and ghrelin. Cell Mol. Life Sci. 2022, 79, 169. [Google Scholar] [CrossRef] [PubMed]
- Salmeri, N.; Viganò, P.; Cavoretto, P.; Marci, R.; Candiani, M. The kisspeptin system in and beyond reproduction: Exploring intricate pathways and potential links between endometriosis and polycystic ovary syndrome. Rev. Endocr. Metab. Disord. 2023. ahead of print. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Whole Cohort (n = 56) | Pregnant (n = 18) | Non-Pregnant (n = 38) | p | |
|---|---|---|---|---|
| Basic characteristic | ||||
| Age (years) [mean (SD)] | 31.89 (4.59) | 32.9 (5.1) | 31.1 (4.3) | 0.07 |
| BMI (kg/m2) [mean (SD)] | 24.53 (4.83) | 25.63 (4.7) | 24.04 (4.23) | 0.09 |
| Time of infertility (mo) [mean (SD)] | 17.11 (4.34) | 17.0 (4.23) | 17.3 (4.7) | 0.13 |
| AMH (ng/mL) [mean (SD)] | 4.9 (5.52) | 4.32 (4.02) | 5.16 (6.1) | 0.02 |
| Pre-stimulation | ||||
| Estradiol (pmol) [mean (SD)] | 156.67 (88.92) | 162.25 (86.68) | 144.2 (95.25) | 0.04 |
| LH (IU/L) [mean (SD)] | 8.99 (4.29) | 7.59 (4.38) | 9.61 (4.16) | 0.03 |
| FSH (IU/L) [mean (SD)] | 5.4 (1.43) | 5.31 (1.37) | 5.43 (1.47) | 0.06 |
| Prolactin (ng/mL) [mean (SD)] | 284.71 (120.65) | 280.41 (94.0) | 286.64 (131.96) | 0.21 |
| TSH (uIU/mL) [mean (SD)] | 1.63 (0.65) | 1.66 (0.64) | 1.61 (0.66) | 0.09 |
| Post-stimulation | ||||
| Estradiol (pmol) [mean (SD)] | 865.64 (602.29) | 898.29 (653.27) | 790.14 (473.92) | 0.03 |
| LH (IU/L) [mean (SD)] | 17.87 (15.7) | 16.96 (12.83) | 18.26 (16.94) | 0.17 |
| FSH (IU/L) [mean (SD)] | 6.55 (2.99) | 7.2 (3.48) | 6.26 (2.76) | 0.21 |
| Prolactin (ng/mL) [mean (SD)] | 303.4 (142.47) | 265.06 (101.16) | 319.97 (155.3) | 0.06 |
| TSH (uIU/mL) [mean (SD)] | 1.6 (0.62) | 1.56 (0.58) | 1.61 (0.64) | 0.5 |
| Whole Cohort (n = 56) | Pregnant (n = 18) | Non-Pregnant (n = 38) | p * | |
|---|---|---|---|---|
| Pre-stimulation | ||||
| PNX-14 (pg/mL) [median (Q1–Q3)] | 141.7 (122.5–218.5) | 141.4 (131.3–237.95) | 142.01 (121.64–200.78) | 0.46 |
| NES-1 (ng/mL) [median (Q1–Q3)] | 4.21 (2.74–5.17) | 4.64 (3.86–5.69) | 3.59 (2.56–4.86) | 0.04 |
| DA (pg/mL) [median (Q1–Q3)] | 1918 (1037–2674) | 1835.5 (1079.4–2463.7) | 1916.15 (902.21–2338.8) | 0.46 |
| OT (pg/mL) [median (Q1–Q3)] | 284 (105–399) | 368.66 (197.04–491.96) | 256.08 (70.66–387.12) | 0.01 |
| Post-stimulation | ||||
| PNX-14 (pg/mL) [median (Q1–Q3)] | 146.3 (125.4–179.7) | 162.3 (148.7–274.2) | 138.2 (118.2–170.2) | <0.001 |
| NES-1 (ng/mL) [median (Q1–Q3)] | 4.86 (3.41–6.87) | 5.37 (4.51–8.42) | 4.26 (3.21–5.98) | 0.01 |
| DA (pg/mL) [median (Q1–Q3)] | 1873 (949–2545) | 2253.85 (1529.7–3024.5) | 1548.7 (825.22–2345.1) | 0.02 |
| OT (pg/mL) [median (Q1–Q3)] | 227 (92–412) | 99.22 (65.33–270.18) | 263.33 (165.26–415.34) | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piróg, M.; Jach, R.; Ząbczyk, M.; Natorska, J. Increased Serum Levels of Phoenixin-14, Nesfatin-1 and Dopamine Are Associated with Positive Pregnancy Rate after Ovarian Stimulation. J. Clin. Med. 2023, 12, 6991. https://doi.org/10.3390/jcm12226991
Piróg M, Jach R, Ząbczyk M, Natorska J. Increased Serum Levels of Phoenixin-14, Nesfatin-1 and Dopamine Are Associated with Positive Pregnancy Rate after Ovarian Stimulation. Journal of Clinical Medicine. 2023; 12(22):6991. https://doi.org/10.3390/jcm12226991
Chicago/Turabian StylePiróg, Magdalena, Robert Jach, Michał Ząbczyk, and Joanna Natorska. 2023. "Increased Serum Levels of Phoenixin-14, Nesfatin-1 and Dopamine Are Associated with Positive Pregnancy Rate after Ovarian Stimulation" Journal of Clinical Medicine 12, no. 22: 6991. https://doi.org/10.3390/jcm12226991
APA StylePiróg, M., Jach, R., Ząbczyk, M., & Natorska, J. (2023). Increased Serum Levels of Phoenixin-14, Nesfatin-1 and Dopamine Are Associated with Positive Pregnancy Rate after Ovarian Stimulation. Journal of Clinical Medicine, 12(22), 6991. https://doi.org/10.3390/jcm12226991