
Sepsis Outcome after Major Abdominal Surgery Does Not Seem to Be Improved by the Use of Pentameric Immunoglobulin IgM: A Single-Center Retrospective Analysis

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Methods
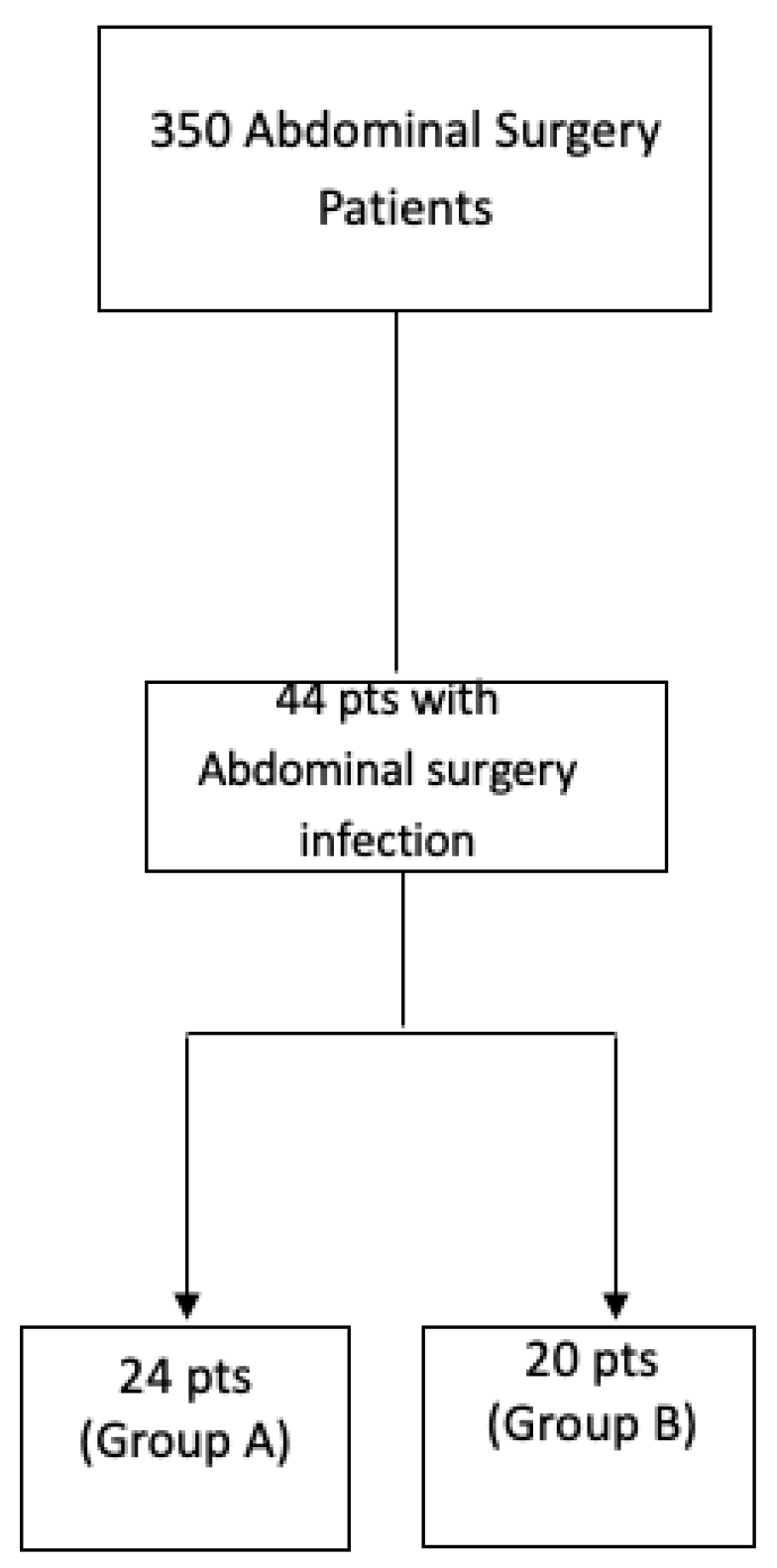
2.1. Study Design
2.2. Study Endpoints
2.3. Ethics Approval
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock:2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef] [PubMed]
- Kyriazopoulou, E.; Leventogiannis, K.; Norrby-Teglund, A.; Dimopoulos, G.; Pantazi, A.; Orfanos, S.E.; Rovina, N.; Tsangaris, I.; Gkavogianni, T.; Botsa, E.; et al. Macrophage activation-like syndrome: An immunological entity associated with rapid progression to death in sepsis. BMC Med. 2017, 15, 172. [Google Scholar] [CrossRef] [PubMed]
- Artenstein, A.W.; Higgins, T.L.; Opal, S.M. Sepsis and scientific revolutions. Crit. Care Med. 2013, 41, 2770–2772. [Google Scholar] [CrossRef] [PubMed]
- Tang, B.M.; Huang, S.J.; McLean, A.S. Genome-wide transcription profiling of human sepsis: A systematic review. Crit. Care 2010, 14, R237. [Google Scholar] [CrossRef] [PubMed]
- Tamayo, E.; Fernandez, A.; Almansa, R.; Carrasco, E.; Heredia, M.; Lajo, C.; Goncalves, L.; Gomez-Herreras, J.I.; de Lejarazu, R.O.; Bermejo-Martin, J.F. Pro- and anti-inflammatory responses are regulated simultaneously from the first moments of septic shock. Eur. Cytokine Netw. 2011, 22, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Alejandria, M.M.; Lansang, M.A.D.; Dans, L.F.; Mantaring, J.B., III. Intravenous immunoglobulin for treating sepsis, severe sepsis and septic shock. Cochrane Database Syst. Rev. 2013, 2018, CD001090. [Google Scholar] [CrossRef] [PubMed]
- Werdan, K.; Pilz, G.; Bujdoso, O.; Fraunberger, P.; Neeser, G.; Schmieder, R.E.; Viell, B.; Marget, W.; Seewald, M.; Walger, P.; et al. Score-based immunoglobulin G therapy of patients with sepsis: The SBITS study. Crit. Care Med. 2007, 35, 2693–2701. [Google Scholar] [PubMed]
- Cavazzuti, I.; Serafni, G.; Busani, S.; Rinaldi, L.; Biagioni, E.; Buoncristiano, M.; Girardis, M. Early therapy with IgM-enriched polyclonal immunoglobulin in patients with septic shock. Intensive Care Med. 2014, 40, 1888–1896. [Google Scholar] [CrossRef] [PubMed]
- Giamarellos-Bourboulis, E.J.; Tziolos, N.; Routsi, C.; Katsenos, C.; Tsangaris, I.; Pneumatikos, I.; Vlachogiannis, G.; Theodorou, V.; Prekates, A.; Antypa, E.; et al. Improving outcomes of severe infections by multidrug-resistant pathogens with polyclonal IgM-enriched immunoglobulins. Clin. Microbiol. Infect. 2016, 22, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, R.P.; Rhodes, A.; Evans, L.; Alhazzani, W.; Beale, R.; Jaeschke, R.; Machado, F.R.; Masur, H.; Osborn, T.; Parker, M.M.; et al. Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.regione.campania.it/assets/documents/linee-indirizzo-terapia-antibiotica.pdf (accessed on 24 August 2023).
- Perrella, A.; Esposito, C.; Amato, G.; Perrella, O.; Migliaccio, C.; Pisaniello, D.; Calise, F.; Cuomo, O.; Santaniello, W. Antifungal prophylaxis with liposomal amphotericin B and caspofungin in high-risk patients after liver transplantation: Impact on fungal infections and immune system. Infect. Dis. 2016, 48, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Prescott, H.C.; Sussman, J.B.; Wiersinga, W.J. Postcritical illness vulnerability. Curr. Opin. Crit. Care 2020, 26, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Kakoullis, L.; Pantzaris, N.D.; Platanaki, C.; Lagadinou, M.; Papachristodoulou, E.; Velissaris, D. The use of IgM-enriched immunoglobulin in adult patients with sepsis. J. Crit. Care 2018, 47, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Barratt-Due, A.; Sokolov, A.; Gustavsen, A.; Hellerud, B.C.; Egge, K.; Pischke, S.E.; Lindstad, J.K.; Pharo, A.; Castellheim, A.; Thorgersen, E.B.; et al. Polyvalent immunoglobulin signifcantly attenuated the formation of IL-1β in Escherichia coli-induced sepsis in pigs. Immunobiology 2013, 218, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Hofman, J.N.; Fertmann, J.M.; Vollmar, B.; Laschke, M.W.; Jauch, K.W.; Menger, M.D. Immunoglobulin M-enriched human intravenous immunoglobulins reduce leukocyte-endothelial cell interactions and attenuate microvascular perfusion failure in normotensive endotoxemia. Shock 2008, 29, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Vaschetto, R.; Clemente, N.; Pagni, A.; Esposito, T.; Longhini, F.; Mercalli, F.; Boggio, E.; Boldorini, R.; Chicchetti, A.; Dianzani, U.; et al. A double blind randomized experimental study on the use of IgM-enriched polyclonal immunoglobulins in an animal model of pneumonia developing shock. Immunobiology 2017, 222, 1074–1080. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, A.; Rello, J.; Neira, J.; Maskin, B.; Ceraso, D.; Vasta, L.; Palizas, F. Effects of high-dose of intravenous immunoglobulin and antibiotics on survival for severe sepsis undergoin surgery. Shock 2005, 23, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Wei, X.; Lv, H.; Li, Y.; Li, P.; Chen, Z.; Liu, G. The clinical efficacy of intravenous IgM-enriched immunoglobulin (pentaglobin) in sepsis or septic shock: A meta-analysis with trial sequential analysis. Ann. Intensive Care 2019, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Perrella, A.; Carannante, N.; Capoluongo, N.; Mascolo, A.; Capuano, A. Endotoxin: Structure Source and Effects. In Endotoxin Induced-Shock: A Multidisciplinary Approach in Critical Care; Springer: Berlin/Heidelberg, Germany, 2023; pp. 1–11. [Google Scholar]

{kind=link}
| Parameter | |
|---|---|
| Age (yrs), median [IQR] | 53.5 [45.2–59.7] |
| Sex, n (%) | |
| Male | 29 (65.9) |
| Female | 15 (34.1) |
| BMI, median [IQR] | 23.5 [22–25] |
| Smoke, n (%) | 22 (50) |
| Potus, n (%) | 12 (27.3) |
| Diabetes, n (%) | 8 (18.2) |
| Metabolic syndrome, n (%) | 7 (15.9) |
| Lactates at EAB, median [IQR] | 2.15 [1.73–3] |
| SOFA score, median [IQR] | 8 [7–8] |
| Leukocytosis, median [IQR] | |
| Baseline | 20.5 [18–22.3] |
| 72 h | 18 [16–20] |
| 96 h | 16 [13.2–18] |
| PCT, median [IQR] | |
| Baseline | 4.5 [2–8] |
| 48 h | 5 [3–6] |
| EAA, median [IQR] | |
| Baseline | 0.6 [0.5–0.7] |
| 72 h | 0.51 [0.5–0.6] |
| PCR, median [IQR] | |
| Baseline | 183.5 [147–254] |
| 48 h | 124 [109–181] |
| Therapy, n (%) | |
| Pentaglobin + antibiotic | 24 (54.5) |
| Only antibiotic | 20 (45.5) |
| Major abdominal surgery, n (%) | 34 (77.3) |
| Inotropes, n (%) | 17 (38.6) |
| Inotrope drugs, n (%) | 21 (47.7) |
| Acidosis at EGA, n (%) | 23 (52.3) |
| ICU stay over 15 days, n (%) | 21 (47.7) |
| Response at 48 h, n (%) | 23 (52.3) |
| Exitus, n (%) | 11 (25) |
| Infected devices, n (%) | 15 (34.1) |
| Fungal infections, n (%) | 4 (9.1) |
| Bacteria, n (%) | |
| Gram-negative | 35 (79.5) |
| Gram-positive | 9 (20.5) |
| Univariate Analysis | |||
|---|---|---|---|
| Parameter | Pentaglobin + Antibiotic (n = 24) | Antibiotic (n = 20) | p |
| Age (yrs), median [IQR] | 48.5 [45.2–57] | 57.5 [47–61.7] | 0.125 |
| Sex, n (%) | 0.210 | ||
| Male | 18 (75) | 11 (65) | |
| Female | 6 (25) | 9 (35) | |
| BMI, median [IQR] | 23 [22–25] | 24 [23–26] | 0.204 |
| Smoke, n (%) | 14 (58.3) | 8 (40) | 0.364 |
| Potus, n (%) | 5 (20.8) | 7 (35) | 0.329 |
| Diabetes, n (%) | 3 (12.5) | 5 (25) | 0.436 |
| Metabolic syndrome, n (%) | 2 (8.3) | 5 (25) | 0.217 |
| SOFA score, median [IQR] | 8 [7–9] | 8 [7–8] | 0.360 |
| Lactates at EAB, median [IQR] | 2.3 [1.85–3] | 2 [1.55–3.75] | 0.849 |
| Leukocytosis, median [IQR] | |||
| Baseline | 19.5 [17.2–22.3] | 21 [19–22.8] | 0.293 |
| 72 h | 18 [16–20.7] | 18 [16–20] | 0.785 |
| 96 h | 15.3 [12.2–18] | 16 [15.2–18] | 0.414 |
| PCT, median [IQR] | |||
| Baseline | 3.5 [2–7.5] | 5 [3.13–8.75] | 0.129 |
| 48 h | 5 [2–7] | 5 [4–6] | 0.403 |
| EAA, median [IQR] | |||
| Baseline | 0.6 [0.5–0.7] | 0.55 [0.4–0.7] | 0.457 |
| 72 h | 0.56 [0.5–0.6] | 0.5 [0.5–0.67] | 0.772 |
| PCR, median [IQR] | |||
| Baseline | 202 [153–242.2] | 163.5 [135.2–258.2] | 0.548 |
| 48 h | 123 [108.2–174.7] | 146 [110–191.2] | 0.333 |
| Major abdominal surgery, n (%) | 24 (70.8) | 20 (85) | 0.402 |
| Inotrope, n (%) | 11 (45.8) | 6 (30) | 0.359 |
| Inotrope drugs, n (%) | 14 (58.3) | 7 (35) | 0.143 |
| Acidosis at EGA, n (%) | 12 (50) | 11 (55) | 0.771 |
| ICU stay over 14 days, n (%) | 17 (70.8) | 4 (20) | 0.001 |
| Response at 48 h, n (%) | 6 (25) | 17 (85) | 0.000 |
| Exitus, n (%) | 6 (25) | 5 (25) | 1.000 |
| Infected devices, n (%) | 11 (45.8) | 4 (20) | 0.111 |
| Fungal infections, n (%) | 2 (8.3) | 2 (10) | 1.000 |
| Bacteria, n (%) | |||
| Gram-negative | 20 (83.3) | 15 (75) | 0.710 |
| MDR ^ | 4 (16.6) | 3(15) | n.s. |
| Gram-positive | 4 (16.7) | 5 (25) | 0.710 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perrella, A.; Rinaldi, L.; Guarino, I.; Bernardi, F.F.; Castriconi, M.; Antropoli, C.; Pafundi, P.C.; Di Micco, P.; Sarno, M.; Capoluongo, N.; et al. Sepsis Outcome after Major Abdominal Surgery Does Not Seem to Be Improved by the Use of Pentameric Immunoglobulin IgM: A Single-Center Retrospective Analysis. J. Clin. Med. 2023, 12, 6887. https://doi.org/10.3390/jcm12216887
Perrella A, Rinaldi L, Guarino I, Bernardi FF, Castriconi M, Antropoli C, Pafundi PC, Di Micco P, Sarno M, Capoluongo N, et al. Sepsis Outcome after Major Abdominal Surgery Does Not Seem to Be Improved by the Use of Pentameric Immunoglobulin IgM: A Single-Center Retrospective Analysis. Journal of Clinical Medicine. 2023; 12(21):6887. https://doi.org/10.3390/jcm12216887
Chicago/Turabian StylePerrella, Alessandro, Luca Rinaldi, Ilaria Guarino, Francesca Futura Bernardi, Maurizio Castriconi, Carmine Antropoli, Pia Clara Pafundi, Pierpaolo Di Micco, Marina Sarno, Nicolina Capoluongo, and et al. 2023. "Sepsis Outcome after Major Abdominal Surgery Does Not Seem to Be Improved by the Use of Pentameric Immunoglobulin IgM: A Single-Center Retrospective Analysis" Journal of Clinical Medicine 12, no. 21: 6887. https://doi.org/10.3390/jcm12216887
APA StylePerrella, A., Rinaldi, L., Guarino, I., Bernardi, F. F., Castriconi, M., Antropoli, C., Pafundi, P. C., Di Micco, P., Sarno, M., Capoluongo, N., Minei, G., Perrella, M., Frangiosa, A., & Capuano, A. (2023). Sepsis Outcome after Major Abdominal Surgery Does Not Seem to Be Improved by the Use of Pentameric Immunoglobulin IgM: A Single-Center Retrospective Analysis. Journal of Clinical Medicine, 12(21), 6887. https://doi.org/10.3390/jcm12216887