
Suicidality in the Light of Schema Therapy Constructs, i.e., Early Maladaptive Schema and Schema Modes: A Longitudinal Study

Abstract
:1. Introduction
1.1. Suicidality and Theoretical Approaches
1.2. Schema Therapy Constructs (EMSs and Schema Modes) and Their Links to Suicidality
1.3. Objectives of the Present Study
2. Methods and Design
2.1. Participants
2.2. Materials
- Young Schema Questionnaire—S3 (YSQ-S3)
- Schema Mode Inventory (SMI)
- Symptom Checklist (SCL-90)
2.3. Procedure
2.4. Statistical Analyses
3. Results
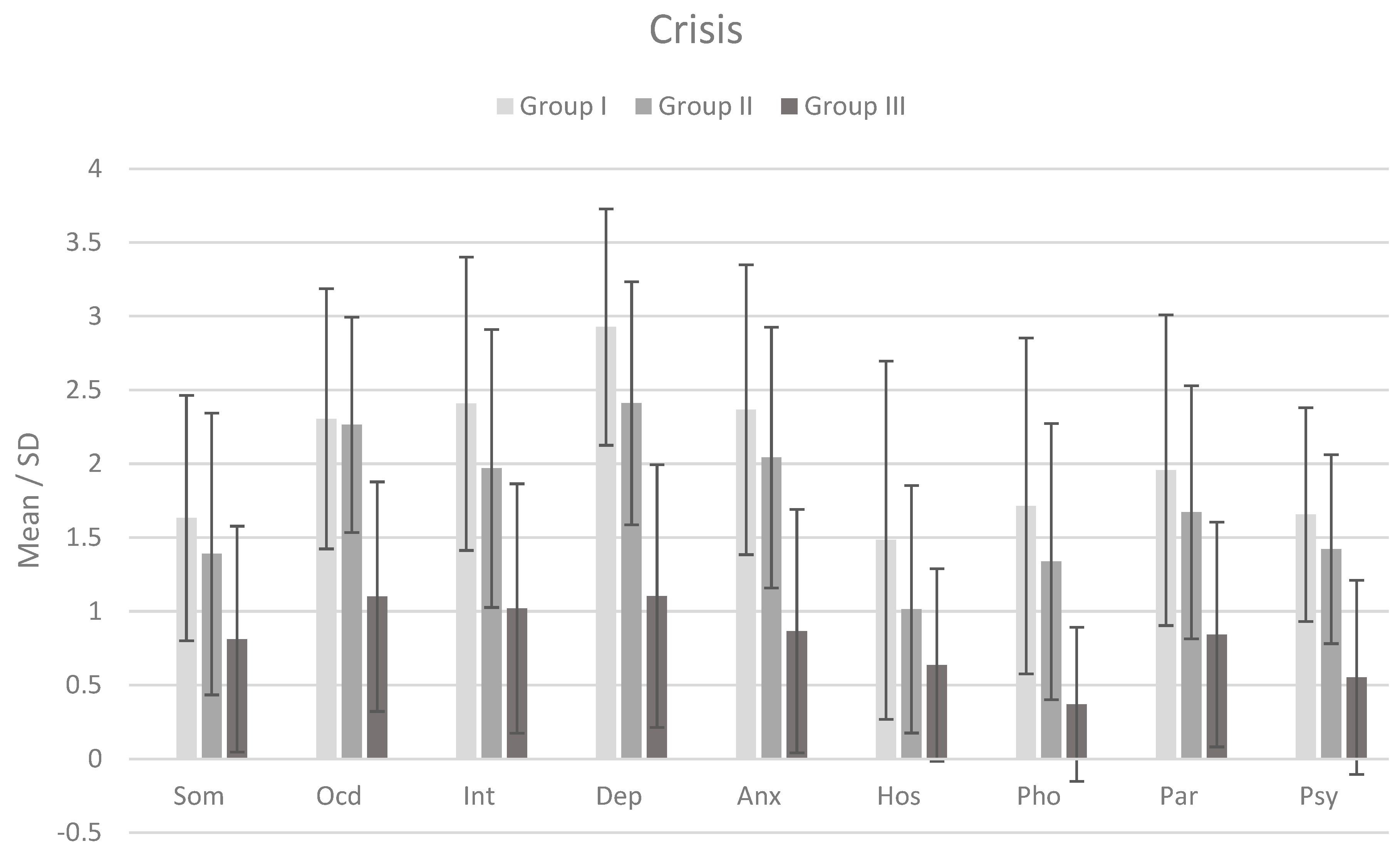
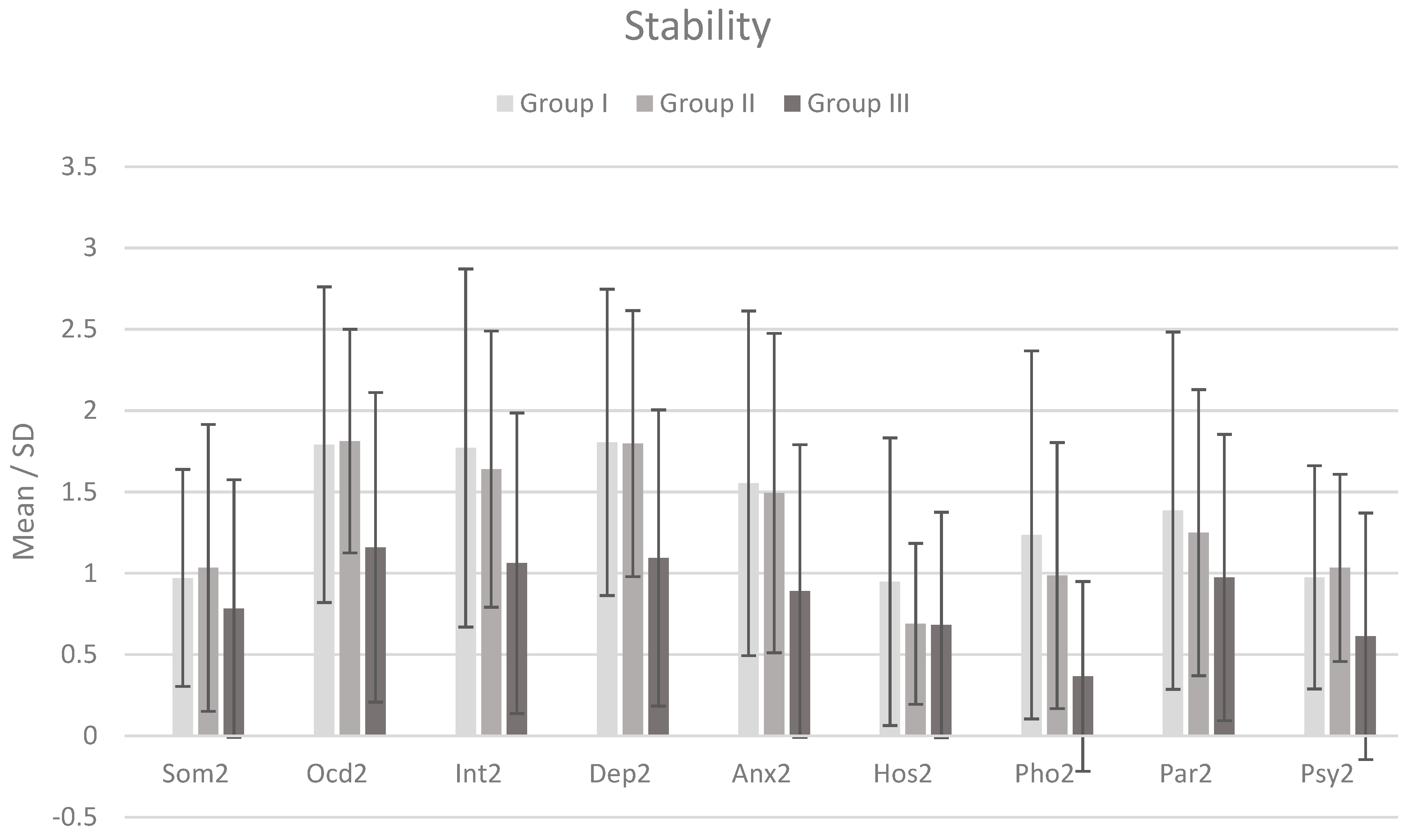
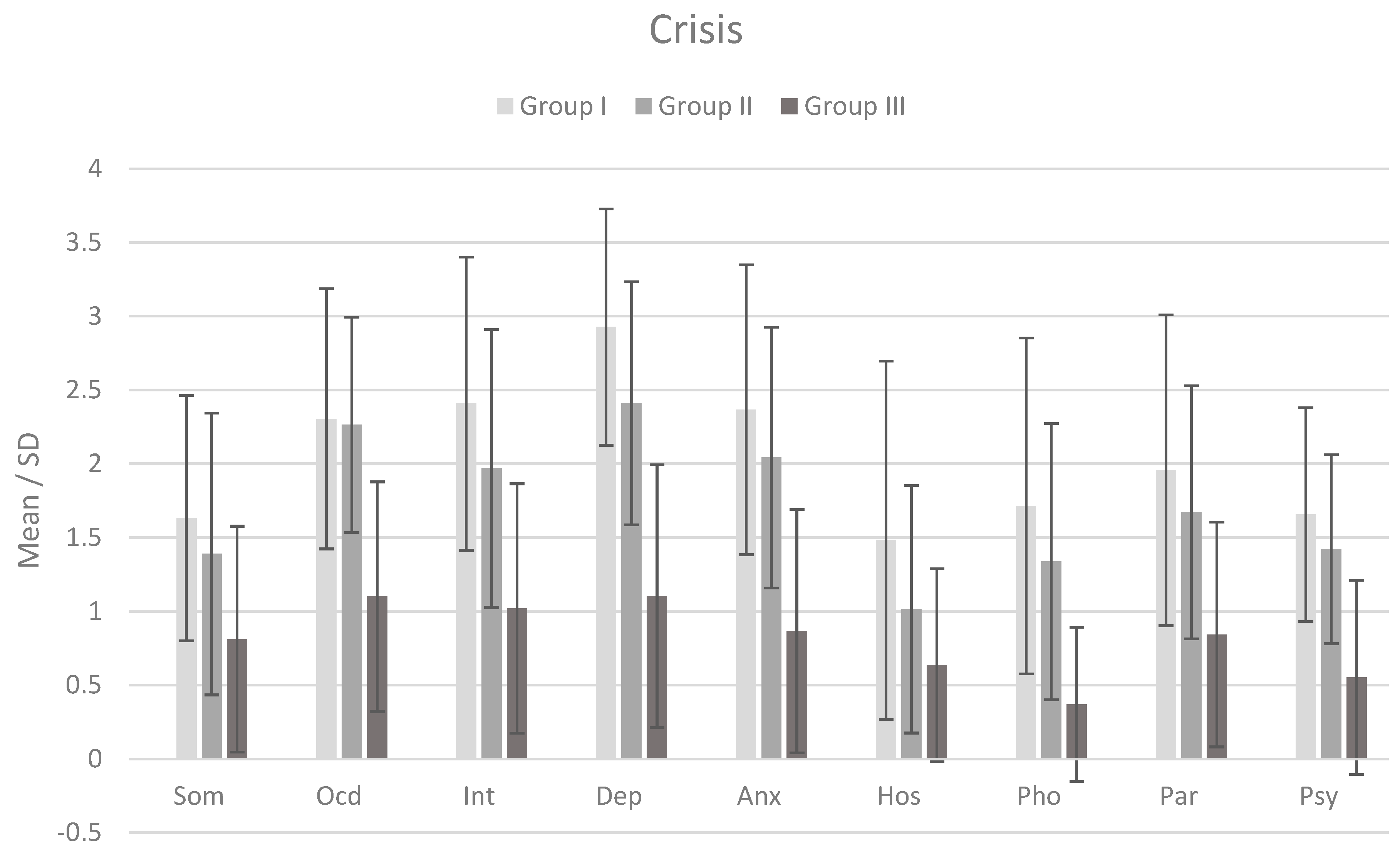
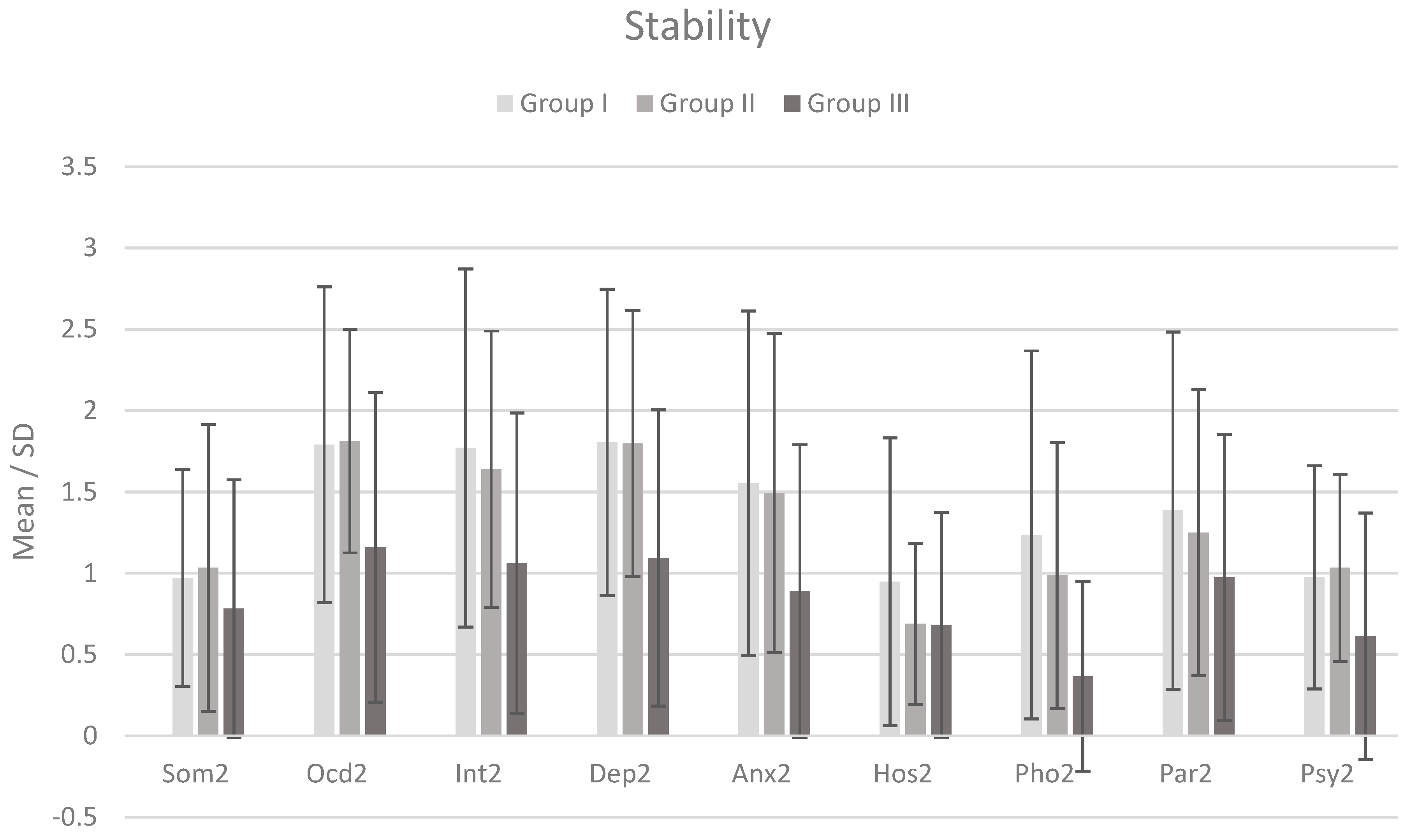
3.1. Characteristics of Participants Considering Severity of Psychopathological Symptoms
3.2. Intra- and Intergroup Differences between EMSs and Schema Modes—General Assessment
3.3. Intergroup Differences in EMSs and Schema Modes—Detailed Assessment
3.4. Differences in ESMs and Schema Modes between Crisis and Stability Times—A Detailed Assessment
4. Discussion
4.1. Main Findings
4.1.1. The Combined Relevance of Schema Therapy Constructs to Suicidality
4.1.2. EMSs and Suicidality
4.1.3. Schema Modes and Suicidality
4.2. Practical Implications
4.3. Limitations
4.4. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Suicide Worldwide in 2019: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2021.
- Shandilya, S. Suicide and suicide prevention: A historical review. Res. J. Soc. Sci. 2018, 9, 35–40. [Google Scholar]
- Andrews, J. Winslow, Forbes Benignus (1810–1874), physician and specialist in insanity. In Oxford Dictionary of National Biography; Oxford University Press: Oxford, UK, 2004. [Google Scholar] [CrossRef]
- Díaz-Oliván, I.; Porras-Segovia, A.; Barrigón, M.; Jiménez-Muñoz, L.; Baca-García, E. Theoretical models of suicidal behaviour: A systematic review and narrative synthesis. Eur. J. Psychiatry 2021, 35, 181–192. [Google Scholar] [CrossRef]
- Baumeister, R.F. Suicide as escape from self. Psychol. Rev. 1990, 97, 90–113. [Google Scholar] [CrossRef]
- Shneidman, E.S. Commentary: Suicide as Psychache. J. Nerv. Ment. Dis. 1993, 181, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Linehan, M.M. Cognitive Behavioral Treatment of Borderline Personality Disorder; Guilford Publications: New York, NY, USA, 1993. [Google Scholar]
- Beck, A.T.; Brown, G.; Berchick, R.J.; Stewart, B.L.; Steer, R.A. Relationship between hopelessness and ultimate suicide: A replication with psychiatric outpatients. Am. J. Psychiatry 1990, 147, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Klonsky, E.D.; Qiu, T.; Saffer, B.Y. Recent advances in differentiating suicide attempters from suicide ideators. Curr. Opin. Psychiatry 2017, 30, 15–20. [Google Scholar] [CrossRef]
- Rudd, M.D. The suicidal mode: A cognitive-behavioral model of suicidality. Suicide Life Threat. Behav. 2000, 30, 18–30. [Google Scholar] [PubMed]
- Joiner, T.E.; Van Orden, K.A. The Interpersonal–Psychological Theory of Suicidal Behavior Indicates Specific and Crucial Psychotherapeutic Targets. Int. J. Cogn. Ther. 2008, 1, 80–89. [Google Scholar] [CrossRef]
- Klonsky, E.D.; May, A.M. The Three-Step Theory (3ST): A New Theory of Suicide Rooted in the “Ideation-to-Action” Framework. Int. J. Cogn. Ther. 2015, 8, 114–129. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Kirtley, O.J. The integrated motivational–volitional model of suicidal behaviour. Philos. Trans. R. Soc. B Biol. Sci. 2018, 373, 20170268. [Google Scholar] [CrossRef]
- Mann, J.J.; Rizk, M.M. A Brain-Centric Model of Suicidal Behavior. Am. J. Psychiatry 2020, 177, 902–916. [Google Scholar] [CrossRef] [PubMed]
- Favril, L.; Yu, R.; Uyar, A.; Sharpe, M.; Fazel, S. Risk factors for suicide in adults: Systematic review and meta-analysis of psychological autopsy studies. Evid. Based Ment. Health 2022, 25, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Tao, M.; Riley, L.; Kann, L.; Ye, L.; Tian, X.; Tian, B.; Hu, J.; Chen, D. Protective factors relating to decreased risks of adolescent suicidal behaviour. Child Care Heal. Dev. 2009, 35, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Appleby, L. Suicide in Psychiatric Patients: Risk and Prevention. Br. J. Psychiatry 1992, 161, 749–758. [Google Scholar] [CrossRef]
- Pereira, A.S.; Willhelm, A.R.; Koller, S.H.; Almeida, R.M.M.D. Risk and protective factors for suicide attempt in emerging adulthood. Ciênc. Saúde Coletiva 2018, 23, 3767–3777. [Google Scholar] [CrossRef] [PubMed]
- Young, J.E.; Klosko, J.S.; Weishaar, M.E. Schema Therapy: A Practitioner’s Guide; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Lobbestael, J.; van Vreeswijk, M.; Arntz, A. Shedding light on schema modes: A clarification of the mode concept and its current research status. Neth. J. Psychol. 2007, 63, 69–78. [Google Scholar] [CrossRef]
- Lobbestael, J.; van Vreeswijk, M.; Spinhoven, P.; Schouten, E.; Arntz, A. Reliability and Validity of the Short Schema Mode Inventory (SMI). Behav. Cogn. Psychother. 2010, 38, 437–458. [Google Scholar] [CrossRef]
- Beck, A.T.; Kovacs, M.; Weissman, A. Hopelessness and Suicidal Behavior. JAMA 1975, 234, 1146. [Google Scholar] [CrossRef]
- Linehan, M.M.; Goodstein, J.L.; Nielsen, S.L.; Chiles, J.A. Reasons for staying alive when you are thinking of killing yourself: The Reasons for Living Inventory. J. Consult. Clin. Psychol. 1983, 51, 276–286. [Google Scholar] [CrossRef]
- Grażka, A.; Królewiak, K.; Sójta, K.; Strzelecki, D. The Reliability and Validity of the Polish Version of the Schema Mode Inventory (SMI). J. Clin. Med. 2023, 12, 6400. [Google Scholar] [CrossRef]
- Azadi, S.; Khosravani, V.; Naragon-Gainey, K.; Bastan, F.S.; Mohammadzadeh, A.; Ghorbani, F. Early Maladaptive Schemas Are Associated with Increased Suicidal Risk among Individuals with Schizophrenia. Int. J. Cogn. Ther. 2019, 12, 274–291. [Google Scholar] [CrossRef]
- Khosravani, V.; Mohammadzadeh, A.; Bastan, F.S.; Amirinezhad, A.; Amini, M. Early maladaptive schemas and suicidal risk in inpatients with bipolar disorder. Psychiatry Res. 2018, 271, 351–359. [Google Scholar] [CrossRef] [PubMed]
- Ahmadpanah, M.; Astinsadaf, S.; Akhondi, A.; Haghighi, M.; Bahmani, D.S.; Nazaribadie, M.; Jahangard, L.; Holsboer-Trachsler, E.; Brand, S. Early maladaptive schemas of emotional deprivation, social isolation, shame and abandonment are related to a history of suicide attempts among patients with major depressive disorders. Compr. Psychiatry 2017, 77, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Frías, Á.; Navarro, S.; Palma, C.; Farriols, N.; Aliaga, F.; Salvador, A.; Aluco, E.; Martínez, B.; Solves, L. Early maladaptive schemas associated with dimensional and categorical psychopathology in patients with borderline personality disorder. Clin. Psychol. Psychother. 2018, 25, e30–e41. [Google Scholar] [CrossRef]
- Ha, J.; Park, D. Suicidal ideation and suicide attempts among university students in South Korea during the COVID-19 pandemic: The application of interpersonal-psychological theory and early maladaptive schema. PeerJ 2022, 10, e13830. [Google Scholar] [CrossRef]
- Leppänen, V.; Vuorenmaa, E.; Lindeman, S.; Tuulari, J.; Hakko, H. Association of parasuicidal behaviour to early maladaptive schemas and schema modes in patients with BPD: The Oulu BPD study. Pers. Ment. Heal. 2016, 10, 58–71. [Google Scholar] [CrossRef]
- American Psychiatric Association. Desk Reference to the Diagnostic Criteria from DSM-5; American Psychiatric Association Publishing: Arlington, TX, USA, 2016. [Google Scholar]
- Bär, A.; Bär, H.E.; Rijkeboer, M.M.; Lobbestael, J. Early Maladaptive Schemas and Schema Modes in clinical disorders: A systematic review. Psychol. Psychother. Theory Res. Pract. 2023, 96, 716–747. [Google Scholar] [CrossRef]
- Wang, C.E.; Halvorsen, M.; Eisemann, M.; Waterloo, K. Stability of dysfunctional attitudes and early maladaptive schemas: A 9-year follow-up study of clinically depressed subjects. J. Behav. Ther. Exp. Psychiatry 2010, 41, 389–396. [Google Scholar] [CrossRef]
- Riso, L.P.; Froman, S.E.; Raouf, M.; Gable, P.; Maddux, R.E.; Turini-Santorelli, N.; Penna, S.; Blandino, J.A.; Jacobs, C.H.; Cherry, M. The Long-Term Stability of Early Maladaptive Schemas. Cogn. Ther. Res. 2006, 30, 515–529. [Google Scholar] [CrossRef]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia–Suicide Severity Rating Scale: Initial Validity and Internal Consistency Findings from Three Multisite Studies With Adolescents and Adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef]
- Phillips, K.; Brockman, R.; Bailey, P.E.; Kneebone, I.I. Young Schema Questionnaire—Short Form Version 3 (YSQ-S3): Preliminary validation in older adults. Aging Ment. Health 2019, 23, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Oettingen, J.; Chodkiewicz, J.; Mącik, D.; Gruszczyńska, E. Polish adaptation of the Young Schema Questionnaire 3 Short Form (YSQ-S3-PL). Psychiatr. Pol. 2018, 52, 707–718. [Google Scholar] [CrossRef] [PubMed]
- Włodawiec, B. Zastosowanie Kwestionariusza SCL-90 w Badaniach nad Efektywnością Psychoterapii. 2007. Available online: https://psychologia.net.pl/artykul.php?level=298 (accessed on 7 August 2023).
- Kuncewicz, D.; Dragan, M.; Hardt, J. Validation of the Polish Version of the Symptom Checklist-27-plus Questionnaire. Psychiatr. Pol. 2014, 48, 345–358. [Google Scholar]
- Field, A.P. Discovering Statistics Using SPSS: (And Sex and Drugs and Rock ‘n’ Roll); SAGE Publications: New York, NY, USA, 2009. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Grażka, A.; Strzelecki, D. Early Maladaptive Schemas and Schema Modes among People with Histories of Suicidality and the Possibility of a Universal Pattern: A Systematic Review. Brain Sci. 2023, 13, 1216. [Google Scholar] [CrossRef] [PubMed]
- Molina, I.O.L.; Zumalde, E.C. Maladaptive Schemas as An Explanation for Gender Differences in Eating Disorder Symptoms in Adolescents. Rev. De Psicol. Clínica Con Niños Y Adolesc. 2023, 10, 3. [Google Scholar] [CrossRef]
- Brenning, K.; Bosmans, G.; Braet, C.; Theuwis, L. Gender Differences in Cognitive Schema Vulnerability and Depressive Symptoms in Adolescents. Behav. Chang. 2012, 29, 164–182. [Google Scholar] [CrossRef]
- Polewka, A.; Szkolnicka, B.; Targosz, D.; Groszek, B.; Kroch, S.; Maj, J.C.; Zieba, A. Fluctuations and seasonality in suicidal attempts. Prz. Lek. 2004, 61, 269–273. [Google Scholar]

{kind=link}
{kind=link}
| Domain | Early Maladaptive Schema | Description |
|---|---|---|
| Disconnection/Rejection | Abandonment/instability | Beliefs about the instability and unreliability of available relationships. |
| Mistrust/abuse | The expectation that others will intentionally hurt, abuse, humiliate, cheat, lie, manipulate, or gain an advantage. | |
| Emotional deprivation | A belief that the desire to have a usual level of emotional support from others will not be sufficiently fulfilled. | |
| Defectiveness/shame | A sense of incompleteness, of being inadequate, unwanted, or inferior, which makes it impossible to be loved and accepted. | |
| Social isolation/alienation | A feeling that a person is disconnected from the world, different from other people, and not part of society. | |
| Impaired autonomy/performance | Dependence/incompetence | A general perception of being unable to cope with daily duties without having significant help from others. |
| Vulnerability to harm and illness | Experiencing an excessive fear of the possibility of a catastrophe (health, emotional, external) that cannot be avoided. | |
| Enmeshment/undeveloped self | Over-involvement emotionally and closeness to at least one person, leading to impairment of complete individuation or normal social development. | |
| Failure | The individual’s belief that he has completely failed and is incompetent compared to others in fields of achievement. | |
| Impaired limits | Entitlement/grandiosity | An individual’s conviction that he or she is superior to others and entitled to special rights and benefits. |
| Insufficient self-control/self-discipline | The difficulties in developing adequate self-control and tolerance to frustration. | |
| Other directedness | Subjugation | Perception of the need to surrender control of others’ needs and emotions to avoid feelings of anger, revenge, or being abandoned. |
| Self-sacrifice | Focusing on voluntarily fulfilling the needs of others over one’s own. | |
| Approval seeking/recognition seeking | It is an overly excessive desire to gain appreciation, respect, or attention from others or to conform to them at the expense of developing a strong, authentic self. | |
| Hyper vigilance/inhibition | Negativity/pessimism | A constant concentration on the negative aspects of life (e.g., pain, death, loss, conflict, possible mistakes), accompanied by overlooking or underestimating the positive aspects. |
| Emotional inhibition | Excessive inhibition of spontaneous behavior, feelings, and communication with others to avoid disapproval, feelings of embarrassment, or losing control. | |
| Unrelenting standards/hypercriticalness | Feeling the need to meet high internalized behavioral and performance standards to avoid criticism. | |
| Punitiveness | The conviction that people should be heavily punished for their faults. |
| Category | Schema Modes | Description |
|---|---|---|
| Maladaptive Child Modes | Vulnerable Child | The individual experiences a sense of unhappiness, anxiety, sadness, and helplessness. |
| Angry Child | The person experiences intense anger and even rage and feels frustrated and impatient when their needs go unmet. | |
| Enraged Child | The person experiences excessive anger, leading to out-of-control outbursts of aggression in which he or she may hurt others or destroy objects. | |
| Impulsive Child | A person acts on impulse or desires. He does not regard the consequences of his/her behavior and has difficulties deferring gratification. | |
| Undisciplined Child | The individual cannot push himself/herself to complete routine, repetitive tasks as he/she quickly becomes frustrated and gives up. | |
| Dysfunctional Coping Modes | Compliant Surrender | The individual is passive and submissive, requires reassurance and guarantees, and diminishes his/her value because of fear of conflict or rejection. |
| Detached Protector | The person escapes the mental pain of unsatisfied needs by turning off all emotions, breaking ties with others, and rejecting anyone’s help. He/she behaves like a robot. | |
| Detached Self-Soother | The person avoids experiencing emotions by engaging in activities that soothe, stimulate, or distract him or her (such as workaholism, gambling, extreme sports, casual sex, or drug use). | |
| Self-Aggrandizer | The individual is inclined toward competition and power, behaves pretentiously, downplays, and uses others to achieve what he/she wants. He shows superiority and demands special treatment. | |
| Bully and Attack | The individual uses threats, bullying, and aggression to achieve what he/she wants or to protect himself/herself from perceived harm. | |
| Dysfunctional Parent Modes | Punitive Parent | It is the internalized voice of significant others who criticize or punish the individual. It results in self-hate, self-denial, self-harm, suicidal fantasies, and self-destructive behavior. |
| Demanding Parent | It is a voice that pressures and pushes the individual to meet excessive standards. It expects perfectionism, maintaining order, tidiness, pursuing high status, high productivity, and not wasting time. | |
| Healthy Modes | Healthy Adult | He/she performs functions specific to adults, such as working, raising children, and taking responsibility. He/she also undertakes activities that are a pleasure, such as sex, pursues intellectual, aesthetic, and cultural interests, takes care of his/her health, and plays sports. |
| Happy Child | The individual experiences inner peace because his/her basic emotional needs are satisfied. He/she feels loved, fulfilled, competent, secure, praised, valuable, understood, resilient, optimistic, and spontaneous. He/she feels connected and cared for by others. Meanwhile, he/she has a sense of autonomy and control. |
| Demographic Characteristics | Subgroup I | Subgroup II | Subgroup III | Whole Sample |
|---|---|---|---|---|
| N | 39 | 36 | 51 | 126 |
| Gender, N (%): | ||||
| Female | 22 (56.4%) | 26 (72.2%) | 41(80.4%) | 89 (70.6%) |
| Male | 17 (43.6%) | 10 (27.8%) | 10 (19.6%) | 37 (29.4%) |
| Age; mean (SD) | 26.08 (10.18) | 34.00 (13.32) | 31.76 (9.17) | 30.64 (11.19) |
| Education; N (%) | ||||
| higher | 6 (15.4%) | 18 (50.0%) | 35 (68.6%) | 59 (46.8%) |
| secondary | 16 (41.0%) | 12 (33.3%) | 14 (27.5%) | 42 (33.3%) |
| basic vocational | 1 (2.6%) | 2 (5.6%) | 0 (0.0%) | 3 (2.4%) |
| elementary | 16 (41.0%) | 4 (11.1%) | 2 (3.9%) | 22 (17.5%) |
| Place of residence | ||||
| village | 7 (17.9%) | 9 (25.0%) | 12 (23.5%) | 28 (22.2%) |
| city under 100,000 inhabitants | 8 (20.5%) | 4 (11.1%) | 11 (21.6%) | 23 (18.3%) |
| city over 100,000 inhabitants | 24 (75.0%) | 23 (63.9%) | 28 (54.9%) | 75 (59.5%) |
| Marital status | ||||
| married | 5 (12.8%) | 10 (27.8%) | 24 (47.1%) | 39 (31.0%) |
| in an informal relationship | 11 (28.2%) | 9 (25.0%) | 18 (35.3%) | 38 (30.2%) |
| single | 23 (59.0%) | 17 (47.2%) | 9 (17.6%) | 49 (38.9%) |
| Employment | ||||
| employed/student | 18 (46.2%) | 28 (77.8%) | 49 (96.1%) | 95 (75.4%) |
| retired | 1 (2.6%) | 0 (0.0%) | 0 (0.0%) | 1 (0.8%) |
| unemployed | 20 (51.3%) | 8 (22.2%) | 2 (3.9%) | 30 (23.8%) |
| SCL-90 Subscales/Crisis vs. Stability | Gr. I | Gr. II | Gr. III | Crisis vs. Stability | |||
|---|---|---|---|---|---|---|---|
| Gr. I | Gr. II | Gr. III | |||||
| m (SD) | m (SD) | m (SD) | t | t | t | ||
| Somatization | c | 1.6 (0.8) | 1.4 (1.0) | 0.8 (0.8) | 0.609 * | 0.311 * | −0.096 |
| s | 1.0 (0.7) ↓ | 1.0 (0.9) ↓ | 0.8 (0.8) | ||||
| Obsessive–compulsive | c | 2.3 (0.9) | 2.3 (0.7) | 1.1 (0.8) | 0.491 * | 0.427 * | −0.062 |
| s | 1.8 (1.0) ↓ | 1.8 (0.7) ↓ | 1.2 (1.0) | ||||
| Interpersonal severity | c | 2.4 (1.0) | 2.0 (0.9) | 1.0 (0.8) | 0.559 * | 0.274 * | −0.069 |
| s | 1.8 (1.1) ↓ | 1.6 (0.8) ↓ | 1.1 (0.9) | ||||
| Depression | c | 2.9 (0.8) | 2.4 (0.8) | 1.1 (0.9) | 1.060 * | 0.569 * | 0.024 |
| s | 1.8 (0.9) ↓ | 1.8 (0.8) ↓ | 1.1 (0.9) | ||||
| Anxiety | c | 2.4 (1.0) | 2.0 (0.9) | 0.9 (0.8) | 0.703 * | 0.530 * | 0.031 |
| s | 1.6 (1.1) ↓ | 1.5 (1.0) ↓ | 0.9 (0.9) | ||||
| Anger and hostility | c | 1.5 (1.2) | 1.0 (0.8) | 0.6 (0.7) | 0.510 * | 0.328 * | −0.068 |
| s | 0.9 (0.9) ↓ | 0.7 (0.5) ↓ | 0.7 (0.7) | ||||
| Phobia | c | 1.7 (1.1) | 1.3 (0.9) | 0.4 (0.5) | 0.411 * | 0.324 * | −0.036 |
| s | 1.2 (1.1) ↓ | 1.0 (0.8) ↓ | 0.4 (0.6) | ||||
| Paranoid ideation | c | 2.0 (1.1) | 1.7 (0.9) | 0.8 (0.8) | 0.536 * | 0.361 * | −0.224 * |
| s | 1.4 (1.1) ↓ | 1.3 (0.9) ↓ | 1.0 (0.9) ↑ | ||||
| Psychoticism | c | 1.7 (0.7) | 1.4 (0.6) | 0.6 (0.7) | 0.625 * | 0.350 * | −0.091 |
| s | 1.0 (0.7) ↓ | 1.0 (0.6) ↓ | 0.6 (0.8) | ||||
| Schema Domains and EMSs | SS | df | MS | F | ηp2 |
|---|---|---|---|---|---|
| Disconnection/rejection | |||||
| Abandonment/instability | 5.799 | 2 | 2.900 | 7.317 *** | 0.139 |
| Mistrust/abuse | 3.493 | 2 | 1.747 | 4.536 * | 0.091 |
| Emotional deprivation | 0.705 | 2 | 0.353 | 0.823 | 0.018 |
| 29.308 | 2 | 14.654 | 5.697 ** | 0.111 |
| 2.266 | 1 | 2.266 | 5.290 * | 0.055 |
| Defectiveness/shame | 5.997 | 2 | 2.999 | 8.202 *** | 0.153 |
| Social isolation/alienation | 4.085 | 2 | 2.043 | 7.977 *** | 0.149 |
| Impaired autonomy/performance | |||||
| Dependence/incompetence | 3.349 | 2 | 1.674 | 7.364 *** | 0.139 |
| Vulnerability to harm and illness | 2.778 | 2 | 1.389 | 4.621 * | 0.092 |
| Enmeshment/undeveloped self | 0.996 | 2 | 0.498 | 1.858 | 0.039 |
| 19.105 | 2 | 9.553 | 5.280 ** | 0.104 |
| 0.347 | 1 | 0.347 | 1.293 | 0.014 |
| Failure | 2.273 | 2 | 1.137 | 2.503 | 0.052 |
| 76.084 | 2 | 38.042 | 10.676 *** | 0.190 |
| 3.300 | 1 | 3.300 | 7.267 ** | 0.074 |
| Impaired limits | |||||
| Entitlement/grandiosity | 0.251 | 2 | 0.126 | 0.566 | 0.012 |
| 0.122 | 2 | 0.061 | 0.046 | 0.001 |
| 0.008 | 1 | 0.008 | 0.035 | 0.000 |
| Insufficient self-control/self-discipline | 0.879 | 2 | 0.440 | 1.424 | 0.030 |
| 19.433 | 2 | 9.717 | 3.946 * | 0.080 |
| 3.371 | 1 | 3.371 | 10.914 *** | 0.107 |
| Other-directedness | |||||
| Subjugation | 1.266 | 2 | 0.633 | 2.393 | 0.050 |
| 27.851 | 2 | 13.925 | 7.675 *** | 0.144 |
| 2.270 | 1 | 2.270 | 8.579 ** | 0.086 |
| Self-sacrifice | 1.764 | 2 | 0.882 | 3.400 * | 0.070 |
| Approval seeking/recognition seeking | 0.128 | 2 | 0.064 | 0.216 | 0.005 |
| 3.186 | 2 | 1.593 | 0.640 | 0.014 |
| 1.989 | 1 | 1.989 | 6.747 * | 0.069 |
| Hyper vigilance/inhibition | |||||
| Negativity/Pessimism | 2.270 | 2 | 1.135 | 2.936 | 0.061 |
| 50.138 | 2 | 25.069 | 8.395 *** | 0.156 |
| 3.605 | 1 | 3.605 | 9.327 ** | 0.093 |
| Emotional inhibition | 2.158 | 2 | 1.079 | 5.366 ** | 0.105 |
| Unrelenting standards/hypercriticalness | 0.738 | 2 | 0.369 | 1.601 | 0.034 |
| 0.087 | 2 | 0.043 | 0.021 | 0.000 |
| 2.129 | 1 | 2.129 | 9.233 ** | 0.092 |
| Punitiveness | 4.710 | 2 | 2.355 | 6.081 ** | 0.118 |
| Schema Modes | SS | df | MS | F | ηp2 |
|---|---|---|---|---|---|
| Child modes | |||||
| Vulnerable Child | 8.223 | 2 | 4.112 | 10.451 *** | 0.187 |
| Angry Child | 1.411 | 2 | 0.705 | 3.714 * | 0.075 |
| Enraged Child | 1.065 | 2 | 0.532 | 2.479 | 0.052 |
| 18.854 | 2 | 9.427 | 7.612 *** | 0.143 |
| 2.973 | 1 | 2.973 | 13.844 *** | 0.132 |
| Impulsive Child | 2.202 | 2 | 1.101 | 4.349 * | 0.087 |
| Undisciplined Child | 2.062 | 2 | 1.031 | 2.847 | 0.059 |
| 9.701 | 2 | 4.850 | 2.151 | 0.045 |
| 5.292 | 1 | 5.292 | 14.615 *** | 0.138 |
| Dysfunctional coping modes | |||||
| Compliant Surrender | 2.758 | 2 | 1.379 | 5.552 ** | 0.109 |
| Detached Protector | 7.706 | 2 | 3.853 | 11.229 *** | 0.198 |
| Detached Self-Soother | 0.269 | 2 | 0.135 | 0.439 | 0.010 |
| 11.846 | 2 | 5.923 | 2.897 | 0.060 |
| 4.560 | 1 | 4.560 | 14.866 *** | 0.140 |
| Self-Aggrandizer | 0.187 | 2 | 0.094 | 0.737 | 0.016 |
| 2.856 | 2 | 1.428 | 1.106 | 0.024 |
| 0.120 | 1 | 0.120 | 0.947 | 0.010 |
| Bully and Attack | 0.660 | 2 | 0.330 | 1.680 | 0.036 |
| 7.799 | 2 | 3.899 | 4.067 * | 0.082 |
| 1.504 | 1 | 1.504 | 7.659 ** | 0.078 |
| Dysfunctional parent modes | |||||
| Punitive Parent | 4.926 | 2 | 2.463 | 8.384 *** | 0.156 |
| Demanding Parent | 0.329 | 2 | 0.164 | 0.686 | 0.015 |
| 0.463 | 2 | 0.231 | 0.173 | 0.004 |
| 2.271 | 1 | 2.271 | 9.470 ** | 0.094 |
| Healthy modes | |||||
| Healthy Adult | 1.754 | 2 | 0.877 | 3.431 * | 0.070 |
| Happy Child | 2.358 | 2 | 1.179 | 3.700 * | 0.075 |
| EMSs/Crisis vs. Stability | Gr. I | Gr. II | Gr. III | Gr. I vs. Gr. II | Gr. I vs. Gr. III | |||
|---|---|---|---|---|---|---|---|---|
| m (SD) | m (SD) | m (SD) | t | r | t | r | ||
| Disconnection/rejection | ||||||||
| Abandonment/instability | c | 4.8 (1.1) | 3.5 (1.2) ↓ | 2.8 (1.3) ↓ | 4.473 *** | 0.425 | 7.660 *** | 0.626 |
| s | 4.1 (1.2) | 3.6 (1.2) | 2.8 (1.3) ↓ | 1.721 | 0.178 | 4.437 *** | 0.422 | |
| Mistrust/abuse | c | 4.2 (1.5) | 3.2 (1.2) ↓ | 2.3 (1.1) ↓ | 3.484 *** | 0.343 | 6.399 *** | 0.557 |
| s | 3.5 (1.5) | 2.9 (1.2) | 2.1 (1.1) ↓ | 1.810 | 0.186 | 4.452 *** | 0.423 | |
| Emotional deprivation | c | 3.2 (1.4) | 3.0 (1.3) | 2.1 (1.2) ↓ | 0.985 | 0.103 | 3.503 *** | 0.345 |
| s | 2.9 (1.3) | 2.5 (1.3) | 2.1 (1.1) ↓ | 1.142 | 0.119 | 2.674 ** | 0.270 | |
| Defectiveness/shame | c | 4.1 (1.4) | 2.9 (1.1) ↓ | 1.7 (1.0) ↓ | 3.795 *** | 0.370 | 7.715 *** | 0.629 |
| s | 3.1 (1.6) | 2.6 (1.2) | 1.7 (1.0) ↓ | 1.536 | 0.159 | 4.458 *** | 0.423 | |
| Social isolation/alienation | c | 4.4 (1.4) | 3.7 (1.3) ↓ | 2.3 (1.2) ↓ | 2.918 ** | 0.292 | 7.042 *** | 0.594 |
| s | 3.9 (1.5) | 3.5 (1.5) | 2.4 (1.1) ↓ | 1.295 | 0.134 | 4.401 *** | 0.419 | |
| Impaired autonomy/performance | ||||||||
| Dependence/ incompetence | c | 3.6 (1.4) | 3.1 (1.1) | 1.8 (0.8) ↓ | 0.765 | 0.080 | 5.384 *** | 0.492 |
| s | 2.7 (1.3) | 3.0 (1.0) | 1.8 (1.0) ↓ | −1.118 | 0.116 | 3.314 *** | 0.328 | |
| Vulnerability to harm and illness | c | 3.7 (1.4) | 3.3 (1.2) | 2.3 (1.2) ↓ | 1.107 | 0.115 | 4.409 *** | 0.420 |
| s | 3.0 (1.3) | 3.1 (1.1) | 2.2 (1.3) ↓ | −0.238 | 0.025 | 2.556 * | 0.259 | |
| Enmeshment/ undeveloped self | c | 2.5 (1.1) | 2.6 (0.9) | 1.7 (0.7) ↓ | −0.342 | 0.036 | 3.007 ** | 0.301 |
| s | 2.1 (0.9) | 2.5 (1.2) | 1.8 (1.2) | −1.278 | 0.133 | 1.372 | 0.142 | |
| Failure | c | 4.3 (1.4) | 3.7 (1.3) | 2.3 (1.3) ↓ | 1.024 | 0.107 | 5.012 *** | 0.465 |
| s | 3.5 (1.7) | 3.4 (1.3) | 2.3 (1.4) ↓ | 0.125 | 0.013 | 3.142 ** | 0.313 | |
| Impaired limits | ||||||||
| Entitlement/grandiosity | c | 2.8 (1.0) | 2.8 (2.8) | 2.7 (0.9) | 0.692 | 0.072 | 0.346 | 0.036 |
| s | 2.7 (0.9) | 2.7 (0.8) | 2.7 (1.0) | −0.121 | 0.013 | −0.028 | 0.003 | |
| Insufficient self-control/ self-discipline | c | 3.9 (1.4) | 3.7 (1.1) | 2.8 (1.2) ↓ | 0.468 | 0.049 | 2.891 ** | 0.290 |
| s | 3.3 (1.1) | 3.4 (1.1) | 2.8 (1.2) | −0.118 | 0.012 | 1.867 | 0.192 | |
| Other-directedness | ||||||||
| Subjugation | c | 3.5 (1.2) | 3.0 (1.0) | 2.3 (1.1) ↓ | 1.459 | 0.151 | 4.425 *** | 0.421 |
| s | 2.9 (1.2) | 2.7 (0.9) | 2.2 (1.0) ↓ | 0.862 | 0.090 | 2.782 ** | 0.280 | |
| Self-sacrifice | c | 4.0 (1.3) | 3.1 (1.0) ↓ | 3.3 (1.0) ↓ | 3.333 *** | 0.330 | 2.926 ** | 0.293 |
| s | 3.7 (1.3) | 3.0 (1.1) ↓ | 3.3 (1.0) | 2.204 * | 0.225 | 1.213 | 0.126 | |
| Approval seeking/ recognition seeking | c | 3.7 (1.2) | 3.9 (1.1) | 3.3 (1.2) | −0.281 | 0.029 | 0.889 | 0.093 |
| s | 3.5 (1.2) | 3.4 (1.0) | 3.2 (1.3) | 0.114 | 0.012 | 0.891 | 0.093 | |
| Hyper vigilance/inhibition | ||||||||
| Negativity/pessimism | c | 4.4 (1.2) | 3.9 (1.3) | 2.9 (1.4) ↓ | 1.346 | 0.140 | 4.643 *** | 0.438 |
| s | 3.8 (1.3) | 3.5 (1.1) | 2.8 (1.5) ↓ | 0.603 | 0.063 | 2.847 ** | 0.286 | |
| Emotional inhibition | c | 3.6 (1.3) | 3.5 (1.2) | 2.6 (1.1) ↓ | 0.743 | 0.078 | 3.368 *** | 0.333 |
| s | 3.0 (1.1) | 3.1 (1.3) | 2.5 (1.1) | −0.357 | 0.037 | 1.701 | 0.176 | |
| Unrelenting standards/ hypercriticalness | c | 3.5 (1.1) | 3.8 (0.9) | 3.5 (1.1) | −0.421 | 0.044 | 0.357 | 0.037 |
| s | 3.5 (1.0) | 3.4 (1.0) | 3.5 (1.2) | 0.248 | 0.026 | −0.113 | 0.012 | |
| Punitiveness | c | 3.7 (1.5) | 3.3 (1.1) | 2.5 (1.2) ↓ | 1.336 | 0.139 | 4.339 *** | 0.414 |
| s | 3.1 (1.4) | 2.8 (1.0) | 2.4 (1.1) ↓ | 0.891 | 0.093 | 2.168 * | 0.222 | |
| Schema Modes/ Crisis vs. Stability | Gr. I | Gr. II | Gr. III | Gr.I vs. Gr.II | Gr.I vs. Gr.III | |||
|---|---|---|---|---|---|---|---|---|
| m (SD) | m (SD) | m (SD) | t | r | t | r | ||
| Child modes | ||||||||
| Vulnerable Child | c | 4.8 (0.9) | 4.0 (1.1) ↓ | 2.5 (1.1) ↓ | 3.619 *** | 0.355 | 8.218 *** | 0.653 |
| s | 3.4 (1.1) | 3.2 (1.1) | 2.3 (1.1) ↓ | 0.854 | 0.089 | 4.075 *** | 0.393 | |
| Angry Child | c | 3.8 (0.9) | 3.2 (0.8) ↓ | 2.9 (0.9) ↓ | 2.928 ** | 0.293 | 4.393 *** | 0.418 |
| s | 3.3 (1.0) | 3.0 (0.9) | 2.6 (0.7) ↓ | 1.125 | 0.117 | 2.808 ** | 0.282 | |
| Enraged Child | c | 2.5 (1.3) | 1.9 (0.8) ↓ | 1.6 (0.6) ↓ | 2.542 * | 0.257 | 3.958 *** | 0.383 |
| s | 2.0 (1.0) | 1.6 (0.5) ↓ | 1.5 (0.6) ↓ | 2.186 * | 0.223 | 3.037 ** | 0.303 | |
| Impulsive Child | c | 3.5 (1.2) | 2.8 (1.0) ↓ | 2.2 (0.9) ↓ | 2.902 ** | 0.291 | 5.330 *** | 0.488 |
| s | 2.7 (1.0) | 2.3 (0.8) | 1.9 (0.8) ↓ | 1.719 | 0.177 | 3.636 *** | 0.356 | |
| Undisciplined Child | c | 4.0 (1.2) | 3.8 (1.0) | 3.0 (1.2) ↓ | 0.579 | 0.061 | 2.615 * | 0.264 |
| s | 3.3 (1.3) | 3.4 (0.9) | 3.1 (1.2) | −0.408 | 0.043 | 0.826 | 0.086 | |
| Dysfunctional coping modes | ||||||||
| Compliant Surrender | c | 3.7 (1.1) | 3.1 (0.8) ↓ | 2.8 (1.0) ↓ | 2.044 * | 0.210 | 3.385 ** | 0.334 |
| s | 2.9 (0.9) | 2.9 (0.8) | 2.7 (0.9) | 0.201 | 0.021 | 0.978 | 0.102 | |
| Detached Protector | c | 3.7 (0.9) | 3.1 (1.2) ↓ | 2.1 (1.1) ↓ | 2.585 * | 0.262 | 5.761 *** | 0.517 |
| s | 2.7 (0.9) | 2.6 (1.2) | 2.2 (1.2) | 0.353 | 0.037 | 1.868 | 0.192 | |
| Detached Self-Soother | c | 3.9 (1.0) | 3.4 (1.2) | 3.1 (1.1) ↓ | 1.679 | 0.173 | 2.417 * | 0.246 |
| s | 3.4 (1.0) | 3.1 (1.2) | 2.8 (1.2) ↓ | 0.930 | 0.097 | 2.065 * | 0.212 | |
| Self-Aggrandizer | c | 2.6 (0.8) | 2.8 (0.9) | 2.9 (0.9) | −0.214 | 0.022 | −1.449 | 0.150 |
| s | 2.7 (0.8) | 2.6 (0.8) | 2.9 (0.8) | 0.423 | 0.044 | −0.908 | 0.095 | |
| Bully and Attack | c | 2.3 (0.8) | 2.2 (0.9) | 1.8 (0.7) ↓ | 0.904 | 0.094 | 3.095 ** | 0.309 |
| s | 2.0 (0.9) | 2.0 (0.7) | 1.7 (0.6) | 0.071 | 0.007 | 1.790 | 0.184 | |
| Dysfunctional parent modes | ||||||||
| Punitive Parent | c | 3.8 (1.2) | 3.0 (0.8) ↓ | 2.0 (0.9) ↓ | 2.698 ** | 0.272 | 6.477 *** | 0.562 |
| s | 2.7 (1.0) | 2.4 (0.9) | 1.8 (0.8) ↓ | 1.211 | 0.126 | 3.723 *** | 0.364 | |
| Demanding Parent | c | 3.8 (0.8) | 3.7 (0.8) | 3.7 (0.9) | 0.586 | 0.061 | 0.607 | 0.064 |
| s | 3.5 (0.8) | 3.4 (0.9) | 3.6 (1.0) | 0.482 | 0.050 | −0.233 | 0.024 | |
| Healthy modes | ||||||||
| Healthy Adult | c | 3.0 (0.8) | 3.3 (0.8) | 4.4 (0.8) ↑ | −1.013 | 0.106 | −6.801 *** | 0.581 |
| s | 3.6 (0.8) | 3.7 (0.8) | 4.5 (0.7) ↑ | −0.215 | 0.023 | −4.589 *** | 0.434 | |
| Happy Child | c | 2.1 (0.7) | 2.5 (0.9) | 3.9 (1.1) ↑ | −1.844 | 0.190 | −7.496 *** | 0.618 |
| s | 2.9 (1.0) | 3.0 (1.2) | 4.0 (0.9) ↑ | −0.079 | 0.008 | −4.397 *** | 0.419 | |
| EMSs/Crisis vs. Stability | Gr. I | Gr. II | Gr. III | Crisis vs. Stability | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Gr. I | Gr. II | Gr. III | ||||||||
| m (SD) | m (SD) | m (SD) | t | r | t | r | t | r | ||
| Disconnection/rejection | ||||||||||
| Abandonment/instability | c | 4.8 (1.1) | 3.5 (1.2) | 2.8 (1.3) | 3.614 *** | 0.354 | −0.957 | 0.100 | −1.191 | 0.124 |
| s | 4.1 (1.2) ↓ | 3.6 (1.2) | 2.8 (1.3) | |||||||
| Mistrust/abuse | c | 4.2 (1.5) | 3.2 (1.2) | 2.3 (1.1) | 3.868 *** | 0.376 | 0.401 | 0.042 | −0.040 | 0.004 |
| s | 3.5 (1.5) ↓ | 2.9 (1.2) | 2.1 (1.1) | |||||||
| Emotional deprivation | c | 3.2 (1.4) | 3.0 (1.3) | 2.1 (1.2) | 1.681 | 0.174 | 1.976 | 0.203 | 0.306 | 0.032 |
| s | 2.9 (1.3) | 2.5 (1.3) | 2.1 (1.1) | |||||||
| Defectiveness/shame | c | 4.1 (1.4) | 2.9 (1.1) | 1.7 (1.0) | 5.954 *** | 0.529 | 1.730 | 0.178 | 0.455 | 0.048 |
| s | 3.1 (1.6) ↓ | 2.6 (1.2) | 1.7 (1.0) | |||||||
| Social isolation/alienation | c | 4.4 (1.4) | 3.7 (1.3) | 2.3 (1.2) | 4.595 *** | 0.434 | 0.796 | 0.083 | −0.939 | 0.098 |
| s | 3.9 (1.5) ↓ | 3.5 (1.5) | 2.4 (1.1) | |||||||
| Impaired autonomy/performance | ||||||||||
| Dependence/ incompetence | c | 3.6 (1.4) | 3.1 (1.1) | 1.8 (0.8) | 4.666 *** | 0.439 | 0.259 | 0.027 | −0.315 | 0.033 |
| s | 2.7 (1.3) ↓ | 3.0 (1.0) | 1.8 (1.0) | |||||||
| Vulnerability to harm and illness | c | 3.7 (1.4) | 3.3 (1.2) | 2.3 (1.2) | 3.922 *** | 0.380 | 0.824 | 0.086 | −0.228 | 0.024 |
| s | 3.0 (1.3) ↓ | 3.1 (1.1) | 2.2 (1.3) | |||||||
| Enmeshment/ undeveloped self | c | 2.5 (1.1) | 2.6 (0.9) | 1.7 (0.7) | 2.221 * | 0.227 | 0.105 | 0.011 | −0.338 | 0.035 |
| s | 2.1 (0.9) ↓ | 2.5 (1.2) | 1.8 (1.2) | |||||||
| Failure | c | 4.3 (1.4) | 3.7 (1.3) | 2.3 (1.3) | 3.228 ** | 0.320 | 1.374 | 0.143 | 0.074 | 0.008 |
| s | 3.5 (1.7) ↓ | 3.4 (1.3) | 2.3 (1.4) | |||||||
| Impaired limits | ||||||||||
| Entitlement/grandiosity | c | 2.8 (1.0) | 2.8 (2.8) | 2.7 (0.9) | 0.849 | 0.089 | −0.658 | 0.069 | 0.159 | 0.017 |
| s | 2.7 (0.9) | 2.7 (0.8) | 2.7 (1.0) | |||||||
| Insufficient self-control/ self-discipline | c | 3.9 (1.4) | 3.7 (1.1) | 2.8 (1.2) | 3.149 ** | 0.313 | 1.812 | 0.187 | 0.765 | 0.080 |
| s | 3.3 (1.1) ↓ | 3.4 (1.1) | 2.8 (1.2) | |||||||
| Other-directedness | ||||||||||
| Subjugation | c | 3.5 (1.2) | 3.0 (1.0) | 2.3 (1.1) | 3.111 ** | 0.310 | 1.907 | 0.196 | 0.049 | 0.005 |
| s | 2.9 (1.2) ↓ | 2.7 (0.9) | 2.2 (1.0) | |||||||
| Self-sacrifice | c | 4.0 (1.3) | 3.1 (1.0) | 3.3 (1.0) | 2.553 * | 0.258 | 0.167 | 0.018 | −1080 | 0.112 |
| s | 3.7 (1.3) ↓ | 3.0 (1.1) | 3.3 (1.0) | |||||||
| Approval seeking/ recognition seeking | c | 3.7 (1.2) | 3.9 (1.1) | 3.3 (1.2) | 1.197 | 0.125 | 1.997 * | 0.205 | 1.289 | 0.134 |
| s | 3.5 (1.2) | 3.4 (1.0) ↓ | 3.2 (1.3) | |||||||
| Hyper vigilance/inhibition | ||||||||||
| Negativity/pessimism | c | 4.4 (1.2) | 3.9 (1.3) | 2.9 (1.4) | 3.418 *** | 0.337 | 1.869 | 0.192 | 0.101 | 0.011 |
| s | 3.8 (1.3) ↓ | 3.5 (1.1) | 2.8 (1.5) | |||||||
| Emotional inhibition | c | 3.6 (1.3) | 3.5 (1.2) | 2.6 (1.1) | 6.188 *** | 0.544 | 3.134 ** | 0.312 | 1.617 | 0.167 |
| s | 3.0 (1.1) ↓ | 3.1 (1.3) ↓ | 2.5 (1.1) | |||||||
| Unrelenting standards/ hypercriticalness | c | 3.5 (1.1) | 3.8 (0.9) | 3.5 (1.1) | 1.614 | 0.167 | 3.035 ** | 0.303 | 0573 | 0.060 |
| s | 3.5 (1.0) | 3.4 (1.0) ↓ | 3.5 (1.2) | |||||||
| Punitiveness | c | 3.7 (1.5) | 3.3 (1.1) | 2.5 (1.2) | 3.857 *** | 0.375 | 2.738 ** | 0.276 | −0.844 | 0.088 |
| s | 3.1 (1.4) ↓ | 2.8 (1.0) ↓ | 2.4 (1.1) | |||||||
| Schema Modes/Crisis vs. Stability | Gr. I | Gr. II | Gr. III | Crisis vs. Stability | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Gr. I | Gr. II | Gr. III | ||||||||
| m (SD) | m (SD) | m (SD) | t | r | t | r | t | r | ||
| Child modes | ||||||||||
| Vulnerable Child | c | 4.8 (0.9) | 4.0 (1.1) | 2.5 (1.1) | 8.250 *** | 0.654 | 3.684 *** | 0.360 | 1.953 | 0.201 |
| s | 3.4 (1.1) ↓ | 3.2 (1.1) ↓ | 2.3 (1.1) | |||||||
| Angry Child | c | 3.8 (0.9) | 3.2 (0.8) | 2.9 (0.9) | 4.761 *** | 0.447 | 1.126 | 0.117 | 1.692 | 0.175 |
| s | 3.3 (1.0) ↓ | 3.0 (0.9) | 2.6 (0.7) | |||||||
| Enraged Child | c | 2.5 (1.3) | 1.9 (0.8) | 1.6 (0.6) | 3.776 *** | 0.368 | 2.043 * | 0.209 | 0.629 | 0.066 |
| s | 2.0 (1.0) ↓ | 1.6 (0.5) ↓ | 1.5 (0.6) | |||||||
| Impulsive Child | c | 3.5 (1.2) | 2.8 (1.0) | 2.2 (0.9) | 5.217 *** | 0.480 | 2.405 * | 0.244 | 1.118 | 0.116 |
| s | 2.7 (1.0) ↓ | 2.3 (0.8) ↓ | 1.9 (0.8) | |||||||
| Undisciplined Child | c | 4.0 (1.2) | 3.8 (1.0) | 3.0 (1.2) | 3.989 *** | 0.386 | 2.017 * | 0.207 | 0.623 | 0.065 |
| s | 3.3 (1.3) ↓ | 3.4 (0.9) ↓ | 3.1 (1.2) | |||||||
| Dysfunctional coping modes | ||||||||||
| Compliant Surrender | c | 3.7 (1.1) | 3.1 (0.8) | 2.8 (1.0) | 5.518 *** | 0.501 | 1.998 * | 0.205 | 1.003 | 0.105 |
| s | 2.9 (0.9) ↓ | 2.9 (0.8) ↓ | 2.7 (0.9) | |||||||
| Detached Protector | c | 3.7 (0.9) | 3.1 (1.2) | 2.1 (1.1) | 6.426 *** | 0.559 | 2.375 * | 0.242 | −0.237 | 0.025 |
| s | 2.7 (0.9) ↓ | 2.6 (1.2) ↓ | 2.2 (1.2) | |||||||
| Detached Self-Soother | c | 3.9 (1.0) | 3.4 (1.2) | 3.1 (1.1) | 2.821 ** | 0.284 | 1.457 | 0.151 | 2.426 * | 0.246 |
| s | 3.4 (1.0) ↓ | 3.1 (1.2) | 2.8 (1.2) ↓ | |||||||
| Self-Aggrandizer | c | 2.6 (0.8) | 2.8 (0.9) | 2.9 (0.9) | −0.429 | 0.045 | 1.046 | 0.109 | 1.052 | 0.110 |
| s | 2.7 (0.8) | 2.6 (0.8) | 2.9 (0.8) | |||||||
| Bully and Attack | c | 2.3 (0.8) | 2.2 (0.9) | 1.8 (0.7) | 2.982 ** | 0.298 | 1.415 | 0.147 | 0.403 | 0.042 |
| s | 2.0 (0.9) ↓ | 2.0 (0.7) | 1.7 (0.6) | |||||||
| Dysfunctional parent modes | ||||||||||
| Punitive Parent | c | 3.8 (1.2) | 3.0 (0.8) | 2.0 (0.9) | 7.265 *** | 0.606 | 4.097 *** | 0.395 | 1.476 | 0.153 |
| s | 2.7 (1.0) ↓ | 2.4 (0.9) ↓ | 1.8 (0.8) | |||||||
| Demanding Parent | c | 3.8 (0.8) | 3.7 (0.8) | 3.7 (0.9) | 2.333 * | 0.238 | 2.146 * | 0.220 | 0.839 | 0.088 |
| s | 3.5 (0.8) ↓ | 3.4 (0.9) ↓ | 3.6 (1.0) | |||||||
| Healthy modes | ||||||||||
| Healthy Adult | c | 3.0 (0.8) | 3.3 (0.8) | 4.4 (0.8) | −4.451 *** | 0.423 | −3.064 ** | 0.306 | −0.797 | 0.083 |
| s | 3.6 (0.8) ↑ | 3.7 (0.8) ↑ | 4.5 (0.7) | |||||||
| Happy Child | c | 2.1 (0.7) | 2.5 (0.9) | 3.9 (1.1) | −5.592 *** | 0.506 | −2.745 ** | 0.276 | −1.882 | 0.194 |
| s | 2.9 (1.0) ↑ | 3.0 (1.2) ↑ | 4.0 (0.9) | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grażka, A.; Królewiak, K.; Sójta, K.; Strzelecki, D. Suicidality in the Light of Schema Therapy Constructs, i.e., Early Maladaptive Schema and Schema Modes: A Longitudinal Study. J. Clin. Med. 2023, 12, 6755. https://doi.org/10.3390/jcm12216755
Grażka A, Królewiak K, Sójta K, Strzelecki D. Suicidality in the Light of Schema Therapy Constructs, i.e., Early Maladaptive Schema and Schema Modes: A Longitudinal Study. Journal of Clinical Medicine. 2023; 12(21):6755. https://doi.org/10.3390/jcm12216755
Chicago/Turabian StyleGrażka, Anna, Klara Królewiak, Klaudia Sójta, and Dominik Strzelecki. 2023. "Suicidality in the Light of Schema Therapy Constructs, i.e., Early Maladaptive Schema and Schema Modes: A Longitudinal Study" Journal of Clinical Medicine 12, no. 21: 6755. https://doi.org/10.3390/jcm12216755
APA StyleGrażka, A., Królewiak, K., Sójta, K., & Strzelecki, D. (2023). Suicidality in the Light of Schema Therapy Constructs, i.e., Early Maladaptive Schema and Schema Modes: A Longitudinal Study. Journal of Clinical Medicine, 12(21), 6755. https://doi.org/10.3390/jcm12216755