
Latanoprost PF vs. Bimatoprost PF: Which Treats the Ocular Surface Better?

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Population
2.3. Ocular Surface MMP-9 Levels, Schirmer’s Test and TBUT
2.4. Statistical Analysis
3. Results
3.1. Participants’ Demographics
3.2. Ocular MMP-9 Levels
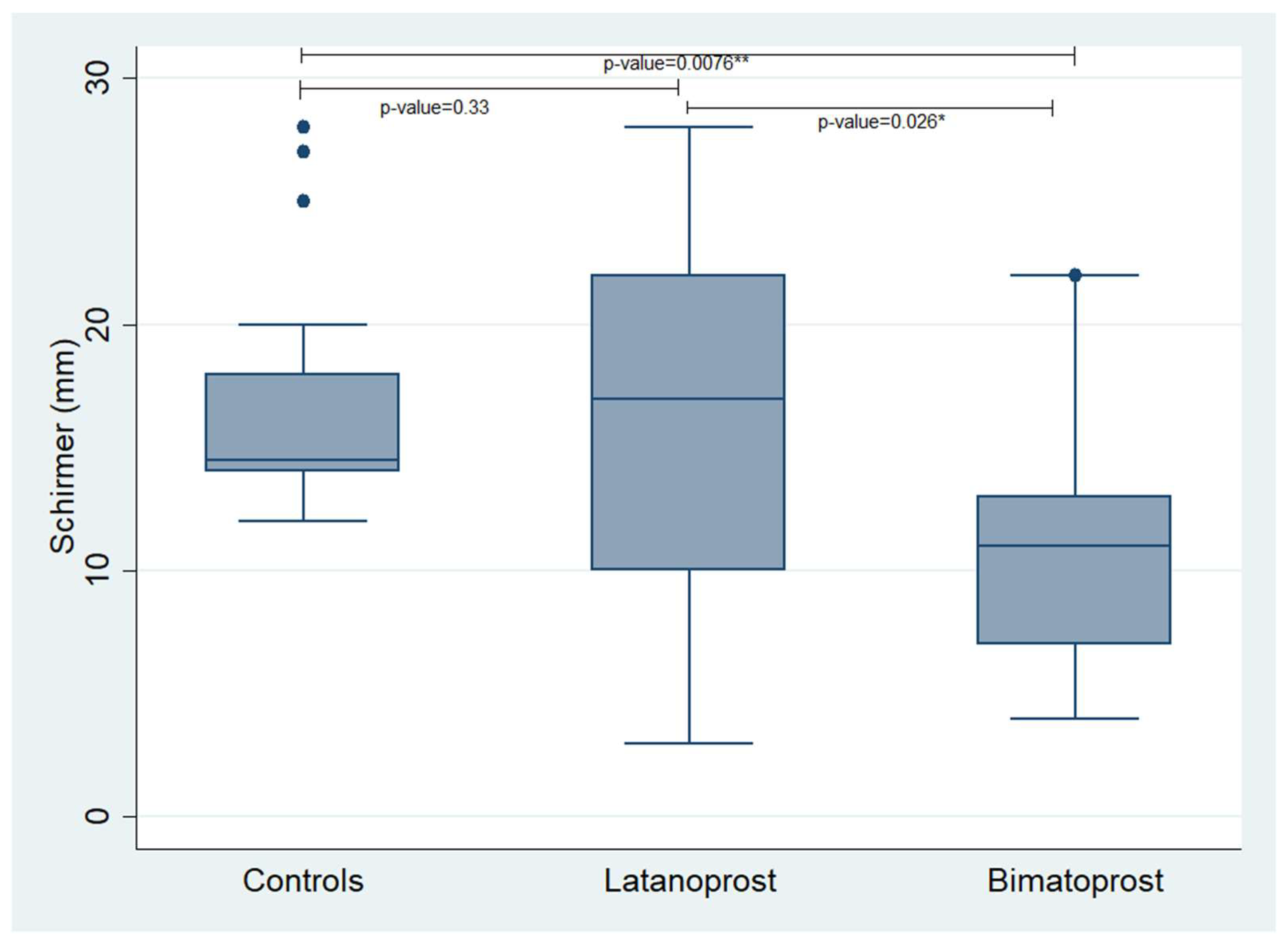
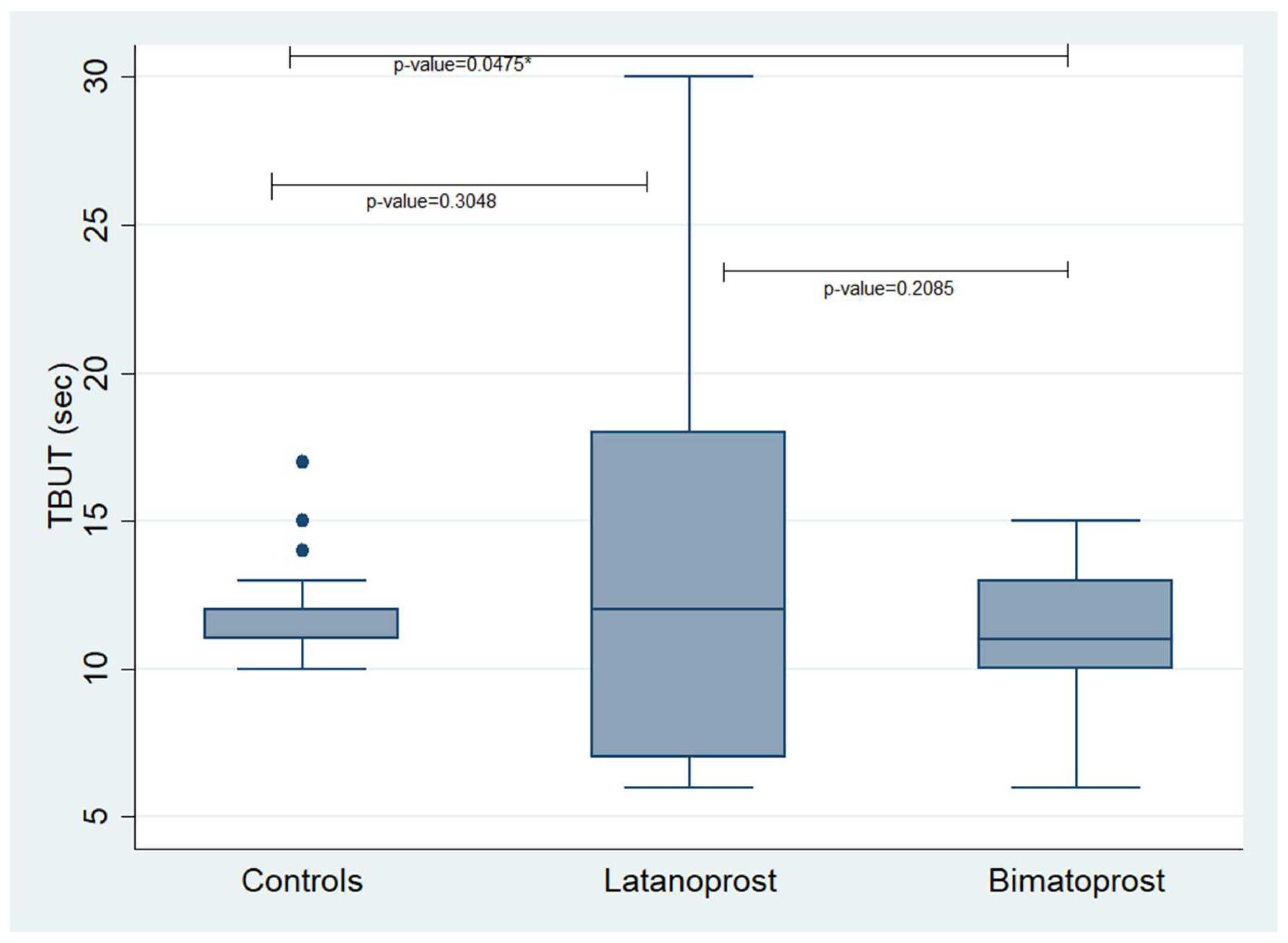
3.3. Schirmer’s Test and TBUT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tham, Y.-C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.-Y. Global Prevalence of Glaucoma and Projections of Glaucoma Burden through 2040: A Systematic Review and Meta-Analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Prum, B.E.; Rosenberg, L.F.; Gedde, S.J.; Mansberger, S.L.; Stein, J.D.; Moroi, S.E.; Herndon, L.W.; Lim, M.C.; Williams, R.D. Primary Open-Angle Glaucoma Preferred Practice Pattern(®) Guidelines. Ophthalmology 2016, 123, P41–P111. [Google Scholar] [CrossRef] [PubMed]
- Toris, C.B.; Gabelt, B.T.; Kaufman, P.L. Update on the Mechanism of Action of Topical Prostaglandins for Intraocular Pressure Reduction. Surv. Ophthalmol. 2008, 53 (Suppl. S1), S107–S120. [Google Scholar] [CrossRef]
- Zaleska-Żmijewska, A.; Strzemecka, E.; Wawrzyniak, Z.M.; Szaflik, J.P. Extracellular MMP-9-Based Assessment of Ocular Surface Inflammation in Patients with Primary Open-Angle Glaucoma. J. Ophthalmol. 2019, 2019, 1240537. [Google Scholar] [CrossRef]
- Zimmerman, T.J.; Hahn, S.R.; Gelb, L.; Tan, H.; Kim, E.E. The Impact of Ocular Adverse Effects in Patients Treated with Topical Prostaglandin Analogs: Changes in Prescription Patterns and Patient Persistence. J. Ocul. Pharmacol. Ther. 2009, 25, 145–152. [Google Scholar] [CrossRef]
- Rossi, G.C.M.; Pasinetti, G.M.; Scudeller, L.; Bianchi, P.E. Ocular Surface Disease and Glaucoma: How to Evaluate Impact on Quality of Life. J. Ocul. Pharmacol. Ther. 2013, 29, 390–394. [Google Scholar] [CrossRef] [PubMed]
- Lemij, H.G.; Hoevenaars, J.G.; van der Windt, C.; Baudouin, C. Patient Satisfaction with Glaucoma Therapy: Reality or Myth? Clin. Ophthalmol. 2015, 9, 785–793. [Google Scholar] [CrossRef]
- Lucca, J.A.; Nunez, J.N.; Farris, R.L. A Comparison of Diagnostic Tests for Keratoconjunctivitis Sicca: Lactoplate, Schirmer, and Tear Osmolarity. CLAO J. 1990, 16, 109–112. [Google Scholar]
- Sambursky, R.; Davitt, W.F.; Friedberg, M.; Tauber, S. Prospective, Multicenter, Clinical Evaluation of Point-of-Care Matrix Metalloproteinase-9 Test for Confirming Dry Eye Disease. Cornea 2014, 33, 812–818. [Google Scholar] [CrossRef]
- Nichols, K.K.; Mitchell, G.L.; Zadnik, K. The Repeatability of Clinical Measurements of Dry Eye. Cornea 2004, 23, 272–285. [Google Scholar] [CrossRef]
- Chotikavanich, S.; de Paiva, C.S.; Li, D.Q.; Chen, J.J.; Bian, F.; Farley, W.J.; Pflugfelder, S.C. Production and Activity of Matrix Metalloproteinase-9 on the Ocular Surface Increase in Dysfunctional Tear Syndrome. Investig. Ophthalmol. Vis. Sci. 2009, 50, 3203–3209. [Google Scholar] [CrossRef]
- Ollivier, F.J.; Gilger, B.C.; Barrie, K.P.; Kallberg, M.E.; Plummer, C.E.; O’Reilly, S.; Gelatt, K.N.; Brooks, D.E. Proteinases of the Cornea and Preocular Tear Film. Vet. Ophthalmol. 2007, 10, 199–206. [Google Scholar] [CrossRef]
- Li, D.-Q.; Pflugfelder, S.C. Matrix Metalloproteinases in Corneal Inflammation. Ocul. Surf. 2005, 3, S198–S202. [Google Scholar] [CrossRef]
- Asahi, M.; Wang, X.; Mori, T.; Sumii, T.; Jung, J.C.; Moskowitz, M.A.; Fini, M.E.; Lo, E.H. Effects of Matrix Metalloproteinase-9 Gene Knock-out on the Proteolysis of Blood-Brain Barrier and White Matter Components after Cerebral Ischemia. J. Neurosci. 2001, 21, 7724–7732. [Google Scholar] [CrossRef] [PubMed]
- Sternlicht, M.D.; Werb, Z. How Matrix Metalloproteinases Regulate Cell Behavior. Annu. Rev. Cell Dev. Biol. 2001, 17, 463–516. [Google Scholar] [CrossRef] [PubMed]
- Behzadian, M.A.; Wang, X.-L.; Windsor, L.J.; Ghaly, N.; Caldwell, R.B. TGF-β Increases Retinal Endothelial Cell Permeability by Increasing MMP-9: Possible Role of Glial Cells in Endothelial Barrier Function. Investig. Ophthalmol. Vis. Sci. 2001, 42, 853–859. [Google Scholar]
- Chan, T.C.Y.; Ye, C.; Chan, K.P.; Chu, K.O.; Jhanji, V. Evaluation of Point-of-Care Test for Elevated Tear Matrix Metalloproteinase 9 in Post-LASIK Dry Eyes. Br. J. Ophthalmol. 2016, 100, 1188–1191. [Google Scholar] [CrossRef] [PubMed]
- Sobrin, L.; Liu, Z.; Monroy, D.C.; Solomon, A.; Selzer, M.G.; Lokeshwar, B.L.; Pflugfelder, S.C. Regulation of MMP-9 Activity in Human Tear Fluid and Corneal Epithelial Culture Supernatant. Investig. Ophthalmol. Vis. Sci. 2000, 41, 1703–1709. [Google Scholar]
- Li, D.-Q.; Chen, Z.; Song, X.J.; Luo, L.; Pflugfelder, S.C. Stimulation of Matrix Metalloproteinases by Hyperosmolarity via a JNK Pathway in Human Corneal Epithelial Cells. Investig. Ophthalmol. Vis. Sci. 2004, 45, 4302–4311. [Google Scholar] [CrossRef]
- Leung, E.W.; Medeiros, F.A.; Weinreb, R.N. Prevalence of Ocular Surface Disease in Glaucoma Patients. J. Glaucoma 2008, 17, 350–355. [Google Scholar] [CrossRef]
- Sambursky, R.; Davitt, W.F.; Latkany, R.; Tauber, S.; Starr, C.; Friedberg, M.; Dirks, M.S.; McDonald, M. Sensitivity and Specificity of a Point-of-Care Matrix Metalloproteinase 9 Immunoassay for Diagnosing Inflammation Related to Dry Eye. JAMA Ophthalmol. 2013, 131, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Epstein, S.P.; Chen, D.; Asbell, P.A. Evaluation of Biomarkers of Inflammation in Response to Benzalkonium Chloride on Corneal and Conjunctival Epithelial Cells. J. Ocul. Pharmacol. Ther. 2009, 25, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Cvenkel, B.; Štunf, Š.; Srebotnik Kirbiš, I.; Strojan Fležar, M. Symptoms and Signs of Ocular Surface Disease Related to Topical Medication in Patients with Glaucoma. Clin. Ophthalmol. 2015, 9, 625–631. [Google Scholar] [CrossRef] [PubMed]
- Steven, D.W.; Alaghband, P.; Lim, K.S. Preservatives in Glaucoma Medication. Br. J. Ophthalmol. 2018, 102, 1497–1503. [Google Scholar] [CrossRef]
- Uusitalo, H.; Egorov, E.; Kaarniranta, K.; Astakhov, Y.; Ropo, A. Benefits of Switching from Latanoprost to Preservative-Free Tafluprost Eye Drops: A Meta-Analysis of Two Phase IIIb Clinical Trials. Clin. Ophthalmol. 2016, 10, 445–454. [Google Scholar] [CrossRef]
- Walimbe, T.; Chelerkar, V.; Bhagat, P.; Joshi, A.; Raut, A. Effect of Benzalkonium Chloride-Free Latanoprost Ophthalmic Solution on Ocular Surface in Patients with Glaucoma. Clin. Ophthalmol. 2016, 10, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Batra, R.; Tailor, R.; Mohamed, S. Ocular Surface Disease Exacerbated Glaucoma: Optimizing the Ocular Surface Improves Intraocular Pressure Control. J. Glaucoma 2014, 23, 56–60. [Google Scholar] [CrossRef]
- Rouland, J.-F.; Traverso, C.E.; Stalmans, I.; Fekih, L.E.; Delval, L.; Renault, D.; Baudouin, C. T2345 Study Group Efficacy and Safety of Preservative-Free Latanoprost Eyedrops, Compared with BAK-Preserved Latanoprost in Patients with Ocular Hypertension or Glaucoma. Br. J. Ophthalmol. 2013, 97, 196–200. [Google Scholar] [CrossRef]
- Solomon, A.; Dursun, D.; Liu, Z.; Xie, Y.; Macri, A.; Pflugfelder, S.C. Pro- and Anti-Inflammatory Forms of Interleukin-1 in the Tear Fluid and Conjunctiva of Patients with Dry-Eye Disease. Investig. Ophthalmol. Vis. Sci. 2001, 42, 2283–2292. [Google Scholar]
- Schönbeck, U.; Mach, F.; Libby, P. Generation of Biologically Active IL-1 Beta by Matrix Metalloproteinases: A Novel Caspase-1-Independent Pathway of IL-1 Beta Processing. J. Immunol. 1998, 161, 3340–3346. [Google Scholar] [CrossRef]
- Honrubia, F.; García-Sánchez, J.; Polo, V.; de la Casa, J.M.M.; Soto, J. Conjunctival Hyperaemia with the Use of Latanoprost versus Other Prostaglandin Analogues in Patients with Ocular Hypertension or Glaucoma: A Meta-Analysis of Randomised Clinical Trials. Br. J. Ophthalmol. 2009, 93, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.W.; Seo, J.H.; Lim, S.-H. Evaluation of Ocular Surface Disease in Elderly Patients with Glaucoma: Expression of Matrix Metalloproteinase-9 in Tears. Eye 2021, 35, 892–900. [Google Scholar] [CrossRef] [PubMed]
- Woodward, D.F.; Krauss, A.H.; Chen, J.; Lai, R.K.; Spada, C.S.; Burk, R.M.; Andrews, S.W.; Shi, L.; Liang, Y.; Kedzie, K.M.; et al. The Pharmacology of Bimatoprost (Lumigan). Surv. Ophthalmol. 2001, 45 (Suppl. S4), S337–S345. [Google Scholar] [CrossRef] [PubMed]
- Woodward, D.F.; Krauss, A.H.-P.; Chen, J.; Liang, Y.; Li, C.; Protzman, C.E.; Bogardus, A.; Chen, R.; Kedzie, K.M.; Krauss, H.A.; et al. Pharmacological Characterization of a Novel Antiglaucoma Agent, Bimatoprost (AGN 192024). J. Pharmacol. Exp. Ther. 2003, 305, 772–785. [Google Scholar] [CrossRef] [PubMed]
- Sharif, N.A.; Kelly, C.R.; Crider, J.Y. Agonist Activity of Bimatoprost, Travoprost, Latanoprost, Unoprostone Isopropyl Ester and Other Prostaglandin Analogs at the Cloned Human Ciliary Body FP Prostaglandin Receptor. J. Ocul. Pharmacol. Ther. 2002, 18, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Maxey, K.M.; Johnson, J.L.; LaBrecque, J. The Hydrolysis of Bimatoprost in Corneal Tissue Generates a Potent Prostanoid FP Receptor Agonist. Surv. Ophthalmol. 2002, 47 (Suppl. S1), S34–S40. [Google Scholar] [CrossRef]
- Rodrigues, G.B.; Abe, R.Y.; Zangalli, C.; Sodre, S.L.; Donini, F.A.; Costa, D.C.; Leite, A.; Felix, J.P.; Torigoe, M.; Diniz-Filho, A.; et al. Neovascular Glaucoma: A Review. Int. J. Retin. Vitr. 2016, 2, 26. [Google Scholar] [CrossRef]
- Saccà, S.; Pascotto, A.; Siniscalchi, C.; Rolando, M. Ocular Complications of Latanoprost in Uveitic Glaucoma: Three Case Reports. J. Ocul. Pharmacol. Ther. 2001, 17, 107–113. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | Controls (n = 24) | Latanoprost PF (n = 11) | Bimatoprost PF (n = 9) |
|---|---|---|---|
| Age ± SD | 68.38 ± 12.15 | 69.9 ± 6.8 | 69 ± 10.1 |
| Male/Female | 14/10 | 7/4 | 5/4 |
| Treatment Duration (months) | - | 7.1 ± 0.83 | 6.67 ± 0.71 |
| MMP-9 (<40 ng/mL) | Control (n = 24) | Latanoprost PF (n = 11) | Bimatoprost PF (n = 9) |
|---|---|---|---|
| Negative | 22 (91.67%) | 8 (72.73%) | 1 (11.11%) |
| Positive | 2 (8.33%) | 3 (27.27%) | 8 (88.89%) |
| Patients | Group | InflammaDry | Schirmer’s Test (mm) | TBUT (s) |
|---|---|---|---|---|
| 1 | Control | Negative | 14 | 10 |
| 2 | Control | Negative | 12 | 15 |
| 3 | Control | Negative | 12 | 14 |
| 4 | Control | Negative | 12 | 12 |
| 5 | Control | Negative | 15 | 13 |
| 6 | Control | Negative | 20 | 17 |
| 7 | Control | Negative | 18 | 11 |
| 8 | Control | Positive | 18 | 10 |
| 9 | Control | Negative | 15 | 11 |
| 10 | Control | Negative | 20 | 12 |
| 11 | Control | Negative | 18 | 12 |
| 12 | Control | Negative | 12 | 12 |
| 13 | Control | Negative | 14 | 12 |
| 14 | Control | Negative | 15 | 12 |
| 15 | Control | Negative | 14 | 12 |
| 16 | Control | Negative | 14 | 11 |
| 17 | Control | Positive | 14 | 11 |
| 18 | Control | Negative | 28 | 11 |
| 19 | Control | Negative | 27 | 11 |
| 20 | Control | Negative | 14 | 14 |
| 21 | Control | Negative | 13 | 12 |
| 22 | Control | Negative | 25 | 12 |
| 23 | Control | Negative | 14 | 12 |
| 24 | Control | Negative | 17 | 12 |
| 25 | Latanoprost PF | Negative | 22 | 9 |
| 26 | Latanoprost PF | Positive | 28 | 14 |
| 27 | Latanoprost PF | Positive | 9 | 6 |
| 28 | Latanoprost PF | Negative | 25 | 7 |
| 29 | Latanoprost PF | Negative | 3 | 12 |
| 30 | Latanoprost PF | Negative | 11 | 30 |
| 31 | Latanoprost PF | Negative | 10 | 18 |
| 32 | Latanoprost PF | Negative | 17 | 12 |
| 33 | Latanoprost PF | Negative | 12 | 9 |
| 34 | Latanoprost PF | Positive | 17 | 6 |
| 35 | Latanoprost PF | Negative | 17 | 19 |
| 36 | Bimatoprost PF | Positive | 4 | 7 |
| 37 | Bimatoprost PF | Positive | 13 | 13 |
| 38 | Bimatoprost PF | Positive | 22 | 15 |
| 39 | Bimatoprost PF | Positive | 7 | 10 |
| 40 | Bimatoprost PF | Positive | 12 | 13 |
| 41 | Bimatoprost PF | Negative | 20 | 11 |
| 42 | Bimatoprost PF | Positive | 5 | 10 |
| 43 | Bimatoprost PF | Positive | 8 | 6 |
| 44 | Bimatoprost PF | Positive | 11 | 12 |
| Control (n = 24) | Latanoprost PF (n = 11) | Bimatoprost PF (n = 9) | |
|---|---|---|---|
| Schirmer’s Test (mm) | 16.46 ± 4.6 | 15.55 ± 7.46 | 11.3 ± 6.28 |
| TBUT (s) | 12.12 ± 1.6 | 12.9 ± 7.2 | 10.78 ± 2.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimtsas, G.S.; Tsiogka, A.; Moschos, M.M. Latanoprost PF vs. Bimatoprost PF: Which Treats the Ocular Surface Better? J. Clin. Med. 2023, 12, 6732. https://doi.org/10.3390/jcm12216732
Dimtsas GS, Tsiogka A, Moschos MM. Latanoprost PF vs. Bimatoprost PF: Which Treats the Ocular Surface Better? Journal of Clinical Medicine. 2023; 12(21):6732. https://doi.org/10.3390/jcm12216732
Chicago/Turabian StyleDimtsas, Georgios S., Anastasia Tsiogka, and Marilita M. Moschos. 2023. "Latanoprost PF vs. Bimatoprost PF: Which Treats the Ocular Surface Better?" Journal of Clinical Medicine 12, no. 21: 6732. https://doi.org/10.3390/jcm12216732
APA StyleDimtsas, G. S., Tsiogka, A., & Moschos, M. M. (2023). Latanoprost PF vs. Bimatoprost PF: Which Treats the Ocular Surface Better? Journal of Clinical Medicine, 12(21), 6732. https://doi.org/10.3390/jcm12216732