
Exploring Deep Cervical Compartments in Head and Neck Surgical Oncology through Augmented Reality Vision: A Proof of Concept

 ,
,  ,
,  , , and
, , and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Creation of the Virtual Patient
2.2.1. Imaging Acquisition Protocols
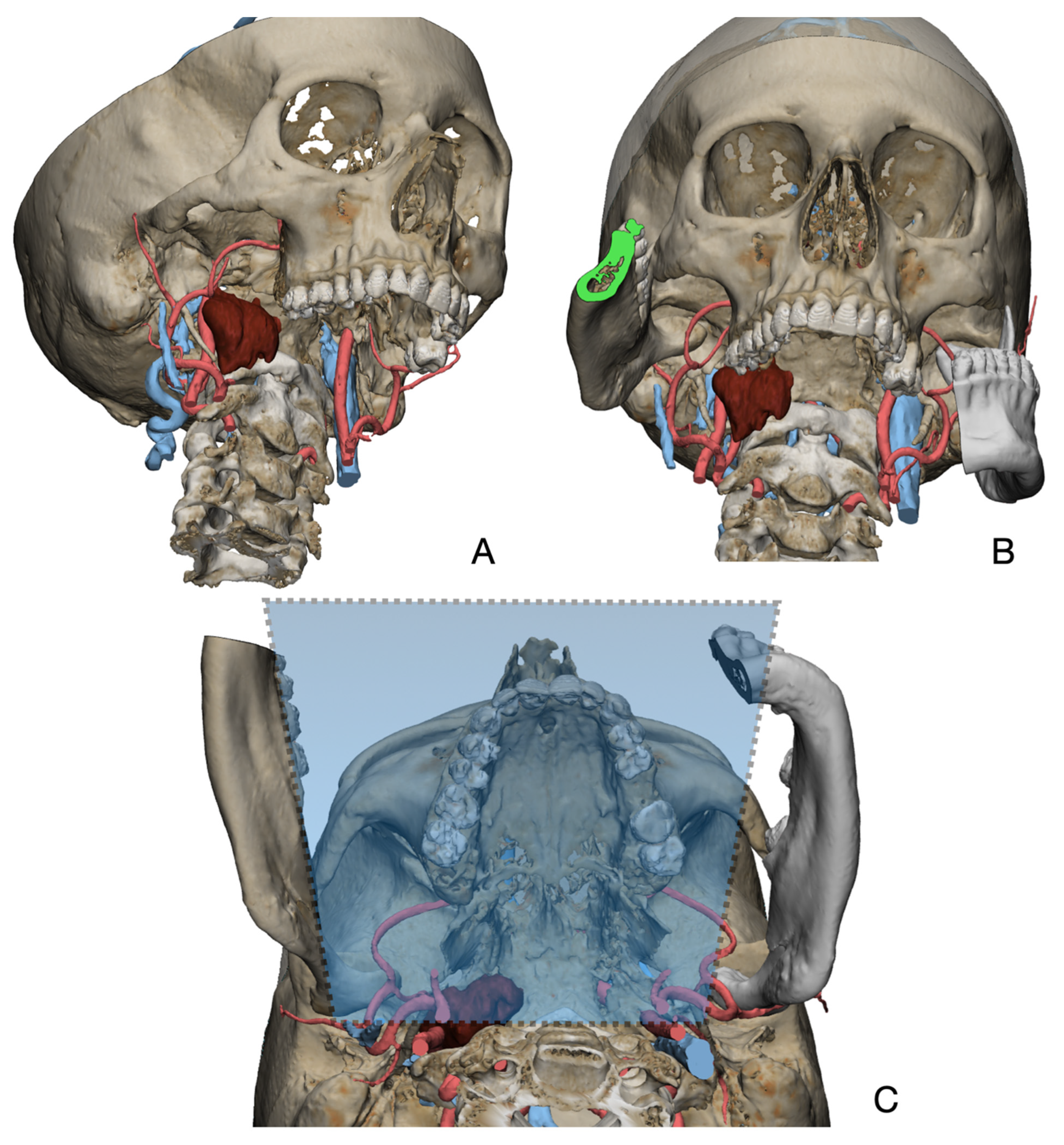
2.2.2. Segmentation and Virtual Surgical Planning
2.3. Surgery
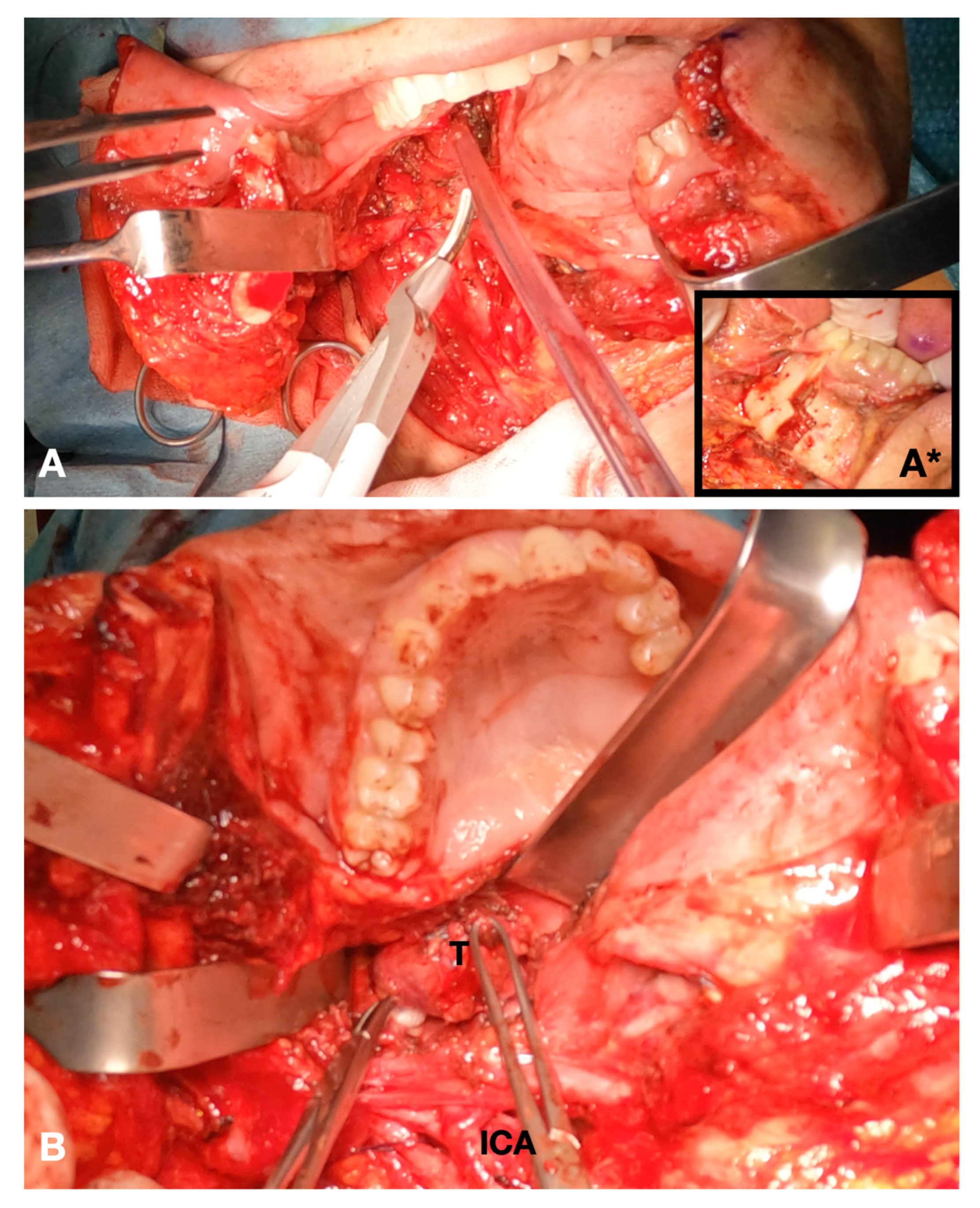
- For disease in the upper cervical tract, the inferior mandibular border was exposed in correspondence with the mandibular symphysis and parasymphyseal region. Incision of the mandible fornix continuing to the lateral mouth floor was performed to enable rotation of the hemimandible on the condylar pivot. During the sectioning of the lateral oral floor, attention was carried out to preserve the lingual nerve. Prebending and predrilling of screw holes for two osteosynthesis titanium plates were performed prior to completing the mandibular splint. A paramedian osteotomy between the roots of the canine and first premolar was accomplished by means of piezosurgical cut. The mandible was extrarotated on the disease side, and the mylohyoid muscle was further sectioned to fully widen the surgical access to the deep cervical neck compartments (Figure 2). After the mass was removed, the mandible was reconstructed using the premodeled titanium plates. Multilayer suture of the neck and intraoral mucosal suture of the mouth floor were completed.
- For disease in the middle or lower cervical tract, the transmandibular approach was not generally deemed necessary. In this case, the surgical approach considered the steps for the traditional neck dissection surgery.
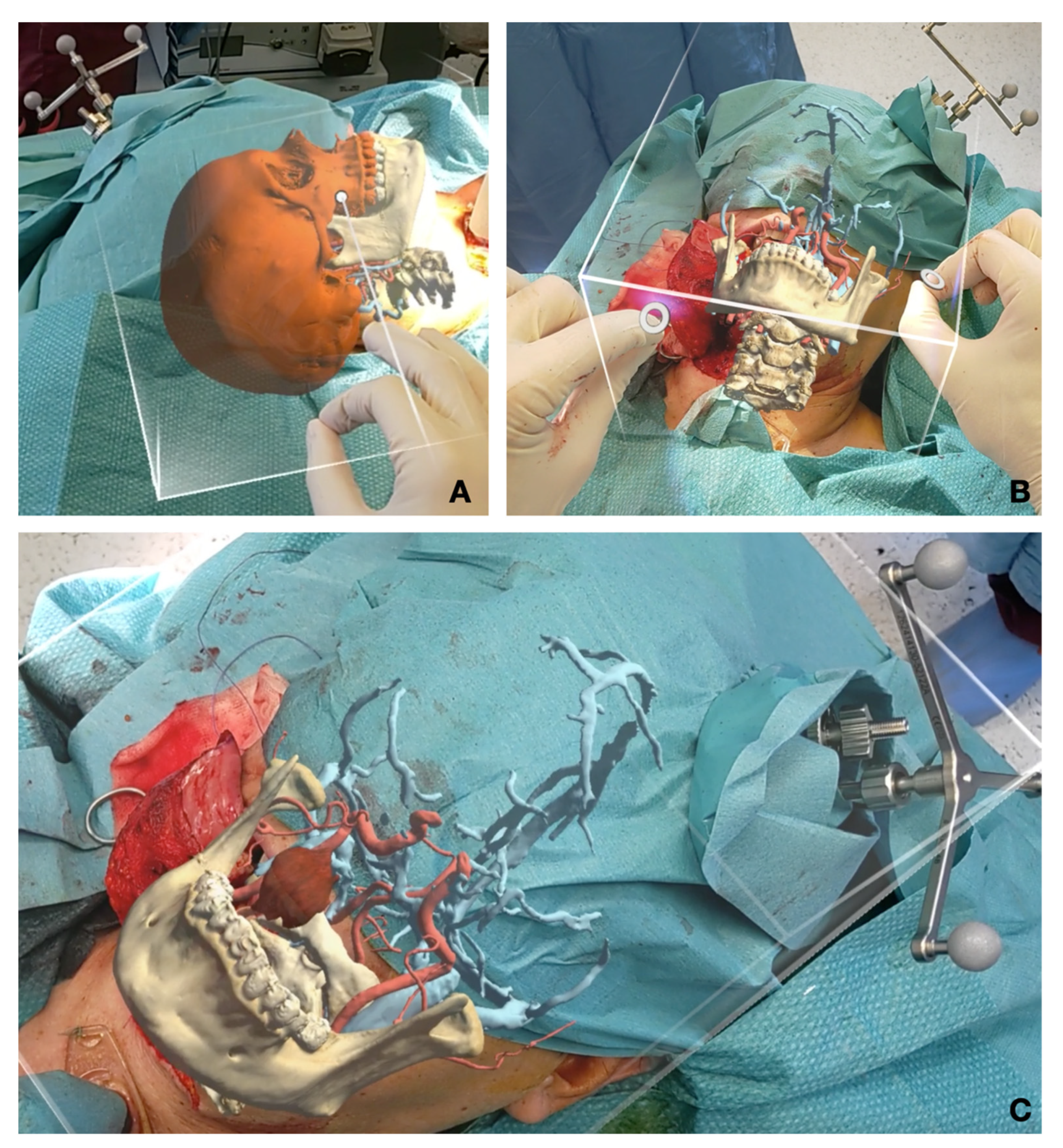
2.4. Augmented Reality
2.5. Literature Review
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bücking, T.M.; Hill, E.R.; Robertson, J.L.; Maneas, E.; Plumb, A.A.; Nikitichev, D.I. From Medical Imaging Data to 3D Printed Anatomical Models. PLoS ONE 2017, 12, e0178540. [Google Scholar] [CrossRef] [PubMed]
- Tel, A.; Bagatto, D.; Costa, F.; Sembronio, S.; Robiony, M. Anatomical Computerized Exploration to Excise Malignancies in Deep Facial Compartments: An Advanced Virtual Reality Protocol for a Tailored Surgical Approach. Front. Oncol. 2022, 12, 875990. [Google Scholar] [CrossRef] [PubMed]
- Azarmehr, I.; Stokbro, K.; Bell, R.B.; Thygesen, T. Surgical Navigation: A Systematic Review of Indications, Treatments, and Outcomes in Oral and Maxillofacial Surgery. J. Oral Maxillofac. Surg. 2017, 75, 1987–2005. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, J.M.; Daly, M.J.; Chan, H.; Qiu, J.; Goldstein, D.; Muhanna, N.; de Almeida, J.R.; Irish, J.C. Accuracy and Reproducibility of Virtual Cutting Guides and 3D-Navigation for Osteotomies of the Mandible and Maxilla. PLoS ONE 2017, 12, e0173111. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Badiali, G.; Cercenelli, L.; Bortolani, B.; Marcelli, E.; Cipriani, R.; Contedini, F.; Marchetti, C.; Tarsitano, A. Combination of CAD/CAM and Augmented Reality in Free Fibula Bone Harvest. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2510. [Google Scholar] [CrossRef]
- Ceccariglia, F.; Cercenelli, L.; Badiali, G.; Marcelli, E.; Tarsitano, A. Application of Augmented Reality to Maxillary Resections: A Three-Dimensional Approach to Maxillofacial Oncologic Surgery. J. Pers. Med. 2022, 12, 2047. [Google Scholar] [CrossRef] [PubMed]
- Scherl, C.; Stratemeier, J.; Rotter, N.; Hesser, J.; Schönberg, S.O.; Servais, J.J.; Männle, D.; Lammert, A. Augmented Reality with HoloLens® in Parotid Tumor Surgery: A Prospective Feasibility Study. ORL 2021, 83, 439–448. [Google Scholar] [CrossRef]
- Condino, S.; Fida, B.; Carbone, M.; Cercenelli, L.; Badiali, G.; Ferrari, V.; Cutolo, F. Wearable Augmented Reality Platform for Aiding Complex 3D Trajectory Tracing. Sensors 2020, 20, 1612. [Google Scholar] [CrossRef]
- Basnet, B.R.; Alsadoon, A.; Withana, C.; Deva, A.; Paul, M. A Novel Noise Filtered and Occlusion Removal: Navigational Accuracy in Augmented Reality-Based Constructive Jaw Surgery. J. Oral Maxillofac. Surg. 2018, 22, 385–401. [Google Scholar] [CrossRef]
- Badiali, G.; Ferrari, V.; Cutolo, F.; Freschi, C.; Caramella, D.; Bianchi, A.; Marchetti, C. Augmented Reality as an Aid in Maxillofacial Surgery: Validation of a Wearable System Allowing Maxillary Repositioning. J. Cranio Maxillofac. Surg. 2014, 42, 1970–1976. [Google Scholar] [CrossRef]
- Ahn, J.; Choi, H.; Hong, J.; Hong, J. Tracking Accuracy of a Stereo Camera-Based Augmented Reality Navigation System for Orthognathic Surgery. J. Oral Maxillofac. Surg. 2019, 77, 1070.e1–1070.e11. [Google Scholar] [CrossRef]
- Cercenelli, L.; Babini, F.; Badiali, G.; Battaglia, S.; Tarsitano, A.; Marchetti, C.; Marcelli, E. Augmented Reality to Assist Skin Paddle Harvesting in Osteomyocutaneous Fibular Flap Reconstructive Surgery: A Pilot Evaluation on a 3D-Printed Leg Phantom. Front. Oncol. 2022, 11, 804748. [Google Scholar] [CrossRef] [PubMed]
- Tel, A.; Arboit, L.; Sembronio, S.; Costa, F.; Nocini, R.; Robiony, M. The Transantral Endoscopic Approach: A Portal for Masses of the Inferior Orbit—Improving Surgeons’ Experience through Virtual Endoscopy and Augmented Reality. Front. Surg. 2021, 8, 715262. [Google Scholar] [CrossRef] [PubMed]
- Meglioli, M.; Naveau, A.; Macaluso, G.M.; Catros, S. 3D Printed Bone Models in Oral and Cranio-Maxillofacial Surgery: A Systematic Review. 3D Print. Med. 2020, 6, 30. [Google Scholar] [CrossRef] [PubMed]
- Murtezani, I.; Sharma, N.; Thieringer, F.M. Medical 3D Printing with a Focus on Point-of-Care in Cranio- and Maxillofacial Surgery. A Systematic Review of Literature. Ann. 3D Print. Med. 2022, 6, 100059. [Google Scholar] [CrossRef]
- Schramm, A.; Suarez-Cunqueiro, M.M.; Barth, E.L.; Essig, H.; Bormann, K.-H.; Kokemueller, H.; Rücker, M.; Gellrich, N.-C. Computer-Assisted Navigation in Craniomaxillofacial Tumors. J. Craniofac. Surg. 2008, 19, 1067–1074. [Google Scholar] [CrossRef]
- Hohlweg-Majert, B.; Schön, R.; Schmelzeisen, R.; Gellrich, N.-C.; Schramm, A. Navigational Maxillofacial Surgery Using Virtual Models. World J. Surg. 2005, 29, 1530–1538. [Google Scholar] [CrossRef]
- Rana, M.; Essig, H.; Eckardt, A.M.; Tavassol, F.; Ruecker, M.; Schramm, A.; Gellrich, N.-C. Advances and Innovations in Computer-Assisted Head and Neck Oncologic Surgery. J. Craniofac. Surg. 2012, 23, 272–278. [Google Scholar] [CrossRef]
- Tel, A.; Arboit, L.; De Martino, M.; Isola, M.; Sembronio, S.; Robiony, M. Systematic Review of the Software Used for Virtual Surgical Planning in Craniomaxillofacial Surgery over the Last Decade. Int. J. Oral Maxillofac. Surg. 2022, 52, S0901502722004611. [Google Scholar] [CrossRef]
- Ignat, M.; Pérouse, M.; Lefebvre, F.; Kadoche, D.; Imperiale, A.; Swanstrom, L.; Vix, M.; Mutter, D. Original Preoperative Localization Technique of Parathyroid Adenomas by 3-Dimensional Virtual Neck Exploration. Surg. Innov. 2021, 28, 261–271. [Google Scholar] [CrossRef]
- D’Agostino, J.; Wall, J.; Soler, L.; Vix, M.; Duh, Q.-Y.; Marescaux, J. Virtual Neck Exploration for Parathyroid Adenomas: A First Step toward Minimally Invasive Image-Guided Surgery. JAMA Surg. 2013, 148, 232. [Google Scholar] [CrossRef] [PubMed]
- Cutolo, F.; Cattari, N.; Fontana, U.; Ferrari, V. Optical See-Through Head-Mounted Displays with Short Focal Distance: Conditions for Mitigating Parallax-Related Registration Error. Front. Robot. AI 2020, 7, 572001. [Google Scholar] [CrossRef] [PubMed]
- Gsaxner, C.; Pepe, A.; Li, J.; Ibrahimpasic, U.; Wallner, J.; Schmalstieg, D.; Egger, J. Augmented Reality for Head and Neck Carcinoma Imaging: Description and Feasibility of an Instant Calibration, Markerless Approach. Comput. Methods Programs Biomed. 2021, 200, 105854. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age and Sex | Virtual Surgical Planning | Disease and Location | Imaging Protocol | AR Device |
|---|---|---|---|---|
| 63, F |  | Persistent Schwannoma surrounding ICA |
| Microsoft Hololens 2 |
| 72, M |  | Paraganglioma located at ICA and ECA bifurcation |
| iPad |
| 59, M | 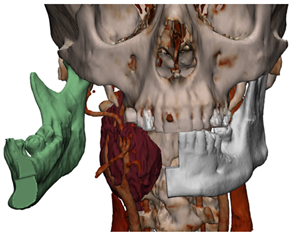 | Paraganglioma located at ICA and ECA bifurcation |
| iPad |
| 76, F |  | Persistance of deep parotid lobe pleomorphic adenoma |
| Microsoft Hololens 2 |
| 78, M |  | Single cervical metastasis from squamocellular carcinoma of the oral oral cavity |
| Microsoft Hololens 2 |
| Author and Year | Anatomical Region | AR Hardware | AR Software | Clinical Application | Purpose |
|---|---|---|---|---|---|
| [5] | Leg (for reconstructive purposes) | Tablet/Smartphone | Unity 3D | AR assisted fibula flap harvest | Validate a markerless recognition |
| [6] | Maxillary | Hololens | Unity 3D + Vuforia Engine | Maxillary tumor resection | Validate AR osteotomies in surgical HN oncology |
| [7] | Parotid | Hololens | Unity 3D; Visual Studio | Intraoperative registration and structure recognition | Pilot study |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tel, A.; Zeppieri, M.; Robiony, M.; Sembronio, S.; Vinayahalingam, S.; Pontoriero, A.; Pergolizzi, S.; Angileri, F.F.; Spadea, L.; Ius, T. Exploring Deep Cervical Compartments in Head and Neck Surgical Oncology through Augmented Reality Vision: A Proof of Concept. J. Clin. Med. 2023, 12, 6650. https://doi.org/10.3390/jcm12206650
Tel A, Zeppieri M, Robiony M, Sembronio S, Vinayahalingam S, Pontoriero A, Pergolizzi S, Angileri FF, Spadea L, Ius T. Exploring Deep Cervical Compartments in Head and Neck Surgical Oncology through Augmented Reality Vision: A Proof of Concept. Journal of Clinical Medicine. 2023; 12(20):6650. https://doi.org/10.3390/jcm12206650
Chicago/Turabian StyleTel, Alessandro, Marco Zeppieri, Massimo Robiony, Salvatore Sembronio, Shankeeth Vinayahalingam, Antonio Pontoriero, Stefano Pergolizzi, Filippo Flavio Angileri, Leopoldo Spadea, and Tamara Ius. 2023. "Exploring Deep Cervical Compartments in Head and Neck Surgical Oncology through Augmented Reality Vision: A Proof of Concept" Journal of Clinical Medicine 12, no. 20: 6650. https://doi.org/10.3390/jcm12206650
APA StyleTel, A., Zeppieri, M., Robiony, M., Sembronio, S., Vinayahalingam, S., Pontoriero, A., Pergolizzi, S., Angileri, F. F., Spadea, L., & Ius, T. (2023). Exploring Deep Cervical Compartments in Head and Neck Surgical Oncology through Augmented Reality Vision: A Proof of Concept. Journal of Clinical Medicine, 12(20), 6650. https://doi.org/10.3390/jcm12206650