
Incidence, Management, and Hospital Costs of Orthopaedic Injuries of E-Scooter Riders in Western Australia

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population
2.3. Inclusion Criteria
- Upper limb fractures and dislocations;
- Lower limb fractures and dislocations;
- Pelvic fractures;
- Spinal fractures.
2.4. Exclusion Criteria
2.5. Outcomes
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kobayashi, L.M.; Williams, E.; Brown, C.V.; Emigh, B.J.; Bansal, V.; Badiee, J.; Checchi, K.D.; Castillo, E.M.; Doucet, J. The e-merging e-pidemic of e-scooters. Trauma Surg. Acute Care Open 2019, 4, e000337. [Google Scholar] [CrossRef] [PubMed]
- Bozzi, A.D.; Aguilera, A. Shared E-Scooters: A Review of Uses, Health and Environmental Impacts, and Policy Implications of a New Micro-Mobility Service. Sustainability 2021, 13, 8676. [Google Scholar] [CrossRef]
- Eadie, K. Escooters Ready to Launch in the City of Light. Available online: https://perth.wa.gov.au/news-and-updates/all-news/escooters-ready-to-launch-in-the-city-of-light (accessed on 5 August 2023).
- Cohen, M. Australia: Cycling Trends Pre, During and Post-COVID. Available online: https://metrocount.com/cycling-trends-across-australia-pre-during-post-covid/ (accessed on 5 August 2023).
- Beck, S.; Barker, L.; Chan, A.; Stanbridge, S. Emergency department impact following the introduction of an electric scooter sharing service. Emerg. Med. Australas. 2020, 32, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Moran, J.; Buck, A.; Williams, J.; Piatkowski, T.; Unnikrishnan, R. Impact on the health service in the Top End, Northern Territory following the introduction of an electric scooter sharing service. Emerg. Med. Australas. 2023, 35, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Dela Cruz, N.; Morgan, C.; Tanna, S.; Talwar, C.; Dattani, R.; Sarraf, K.; Gibbons, C. Injury Patterns of e-scooter-related Orthopaedic Trauma in Central London: A Multicentre Study. Ann. R. Coll. Surg. Engl. 2022, 104, 187–194. [Google Scholar] [CrossRef]
- St John’s Ambulance. e-Scooter Accidents Can Prove Deadly, St John Warns during National Road Safety Week. Available online: https://stjohnwa.com.au/news/e-scooter-accidents-can-prove-deadly-st-john-warns-during-national-road-safety-week (accessed on 5 August 2023).
- Mitchell, G.; Tsao, H.; Randell, T.; Marks, J.; Mackay, P. Impact of electric scooters to a tertiary emergency department: 8-week review after implementation of a scooter share scheme. Emerg. Med. Australas. 2019, 31, 930–934. [Google Scholar] [CrossRef]
- Störmann, P.; Klug, A.; Nau, C.; Verboket, R.D.; Leiblein, M.; Müller, D.; Schweigkofler, U.; Hoffmann, R.; Marzi, I.; Lustenberger, T. Characteristics and Injury Patterns in Electric-Scooter Related Accidents—A Prospective Two-Center Report from Germany. J. Clin. Med. 2020, 9, 1569. [Google Scholar] [CrossRef]
- Toofany, M.; Mohsenian, S.; Shum, L.; Chan, H.; Brubacher, J. Injury Patterns and Circumstances Associated with Electric Scooter Collisions: A Scoping Review. Inj. Prev. 2021, 27, 490–499. [Google Scholar] [CrossRef]
- Bekhit, M.N.Z.; Le Fevre, J.; Bergin, C.J. Regional healthcare costs and burden of injury associated with electric scooters. Injury 2020, 51, 271–277. [Google Scholar] [CrossRef]
- Dhillon, N.K.; Juillard, C.; Barmparas, G.; Lin, T.-L.; Kim, D.Y.; Turay, D.; Seibold, A.R.; Kaminski, S.; Duncan, T.K.; Diaz, G.; et al. Electric Scooter Injury in Southern California Trauma Centers. J. Am. Coll. Surg. 2020, 231, 133–138. [Google Scholar] [CrossRef]
- Raubenheimer, K.; Dodd, J.; Jarmin, M.J.; Sarvepalli, R.; Fatovich, D.M.; Weber, D.G. Western Australian State Trauma Registry analysis of incidence and injury patterns associated with e-Scooter injuries: 5-year retrospective case series. ANZ J. Surg. 2023, 93, 1890–1895. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Jami, M.; Geller, J.; Granger, C.; Geaney, L.; Aiyer, A. The impact of e-scooter injuries: A systematic review of 34 studies. Bone Jt. Open 2022, 3, 674–683. [Google Scholar] [CrossRef]
- Talia, A.J.; Clare, S.; Liew, S.M.; Edwards, E.R. Orthopaedic injuries due to electric scooter trauma presenting to a level 1 trauma centre before and after introduction of a scooter-sharing scheme. J. Orthop. 2023, 39, 42–44. [Google Scholar] [CrossRef]
- Iroz-Elardo, N.; Currans, K. Injury Burden of Introducing E-Scooters: A Review of E-Scooter Injury Studies Using Retrospective Review of Emergency Department Records, 2015–2019. Transp. Res. Rec. 2021, 2675, 1150–1159. [Google Scholar] [CrossRef]
- Shichman, I.; Shaked, O.; Factor, S.; Elbaz, E.; Khoury, A. Epidemiology of Fractures Sustained During Electric Scooter Accidents: A Retrospective Review of 563 Cases. J. Bone Joint Surg. Am. 2021, 103, 1125–1131. [Google Scholar] [CrossRef]
- Siow, M.Y.; Lavoie-Gagne, O.; Politzer, C.S.; Mitchell, B.C.; Harkin, W.E.; Flores, A.R.; Schwartz, A.K.; Girard, P.J.; Kent, W.T. Electric Scooter Orthopaedic Injury Demographics at an Urban Level I Trauma Center. J. Orthop. Trauma 2020, 34, e424–e429. [Google Scholar] [CrossRef] [PubMed]
- Ishmael, C.R.; Hsiue, P.P.; Zoller, S.D.; Wang, P.; Hori, K.R.; Gatto, J.D.; Li, R.; Jeffcoat, D.M.; Johnson, E.E.; Bernthal, N.M. An Early Look at Operative Orthopaedic Injuries Associated with Electric Scooter Accidents: Bringing High-Energy Trauma to a Wider Audience. J. Bone Joint Surg. Am. 2020, 102, e18. [Google Scholar] [CrossRef]
- Büyükceran, İ.; Ersoy, A.; Şay, C.Ş.; Coşkun, H.S.; Tomak, Y. The Epidemiology and the Treatment of Fractures Due to Electric Scooters: A Comparison of Pediatric and Adult Age Groups. Cureus 2023, 15, e37807. [Google Scholar] [CrossRef]
- Tischler, E.H.; Laurent Tsai, S.H.; Wolfert, A.J.; Suneja, N.; Naziri, Q.; Tischler, H.M. Orthopedic fracture hospitalizations are revving up from E-Scooter related injuries. J. Clin. Orthop. Trauma 2021, 23, 101607. [Google Scholar] [CrossRef]
- Hourston, G.J.M.; Ngu, A.; Hopkinson-Woolley, J.; Stöhr, K. Orthopedic injuries associated with use of electric scooters in the UK: A dangerous trend? Case series and review of the literature. Traffic Inj. Prev. 2021, 22, 242–245. [Google Scholar] [CrossRef] [PubMed]
- McNulty, M.; Look, N.; Strage, K.; Lauder, A. Orthopaedic Injuries after Introduction of Electric Scooters to Denver, Colorado. J. Am. Acad. Orthop. Surg. 2022, 30, 897–902. [Google Scholar] [CrossRef]
- LaGreca, M.; Didzbalis, C.J.; Oleck, N.C.; Weisberger, J.S.; Ayyala, H.S. Increasing Incidence of Hand and Distal Upper Extremity Injuries Associated With Electric Scooter Use. J. Hand Surg. 2022, 47, 478.e1–478.e7. [Google Scholar] [CrossRef] [PubMed]
- Coelho, A.; Feito, P.; Corominas, L.; Sánchez-Soler, J.F.; Pérez-Prieto, D.; Martínez-Diaz, S.; Alier, A.; Monllau, J.C. Electric Scooter-Related Injuries: A New Epidemic in Orthopedics. J. Clin. Med. 2021, 10, 3283. [Google Scholar] [CrossRef] [PubMed]
- Factor, S.; Shaked, O.; Atlan, F.; Pritsch, T.; Shichman, I. Electric Scooter-Related Upper Limb Fractures: Analysis of 458 Cases. J. Hand Surg. 2023, 48, 197.e1–197.e6. [Google Scholar] [CrossRef]
- Rizzo, M.G.; Allegra, P.R.; Yakkanti, R.; Luxenburg, D.; Dodds, S.D. Electric scooters as a source of orthopedic injuries at a Level-I trauma center. J. Orthop. 2022, 31, 86–91. [Google Scholar] [CrossRef]
- Liew, Y.; Wee, C.; Pek, J. New peril on our roads: A retrospective study of electric scooter-related injuries. Singapore Med. J. 2020, 61, 92–95. [Google Scholar] [CrossRef] [PubMed]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 5 August 2023).
- Abduljabbar, R.L.; Liyanage, S.; Dia, H. The role of micro-mobility in shaping sustainable cities: A systematic literature review. Transp. Res. Part Transp. Environ. 2021, 92, 102734. [Google Scholar] [CrossRef]
- Olabi, A.G.; Wilberforce, T.; Obaideen, K.; Sayed, E.T.; Shehata, N.; Alami, A.H.; Abdelkareem, M.A. Micromobility: Progress, benefits, challenges, policy and regulations, energy sources and storage, and its role in achieving sustainable development goals. Int. J. Thermofluids 2023, 17, 100292. [Google Scholar] [CrossRef]
- Cantatore, J. Beam to Double e-Scooters Geofence Area in Bunbury. Available online: https://www.bunburyherald.com.au/news/south-west/beam-to-double-e-scooters-geofence-area-in-bunbury-c-7441552 (accessed on 5 August 2023).
- City of Perth. City of Perth Announces eScooter Trial. Available online: https://www.governmentnews.com.au/city-of-perth-announces-escooter-trial/ (accessed on 5 August 2023).
- Zuniga-Garcia, N.; Tec, M.; Scott, J.G.; Machemehl, R.B. Evaluation of e-scooters as transit last-mile solution. Transp. Res. Part C Emerg. Technol. 2022, 139, 103660. [Google Scholar] [CrossRef]
- Moldovan, F.; Moldovan, L.; Bataga, T. The Environmental Sustainability Assessment of an Orthopedics Emergency Hospital Supported by a New Innovative Framework. Sustainability 2023, 15, 13402. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Variable | Total Cohort (n = 61) | Admitted (n = 32) | Discharged from ED (n = 29) | p Value |
|---|---|---|---|---|
| Age (yrs) | 43 (33–53) | 45 (37–52) | 37 (33–55) | 0.5 |
| Sex (male: female) | 49:12 | 25:7 | 24:5 | 0.88 |
| LOS | 1 (0–4) | 4 (3–8) | - | Not applicable |
| Number of OPC appointments | 3 (1–5) | 4 (3–5) | 2 (0–3) | <0.01 |
| Days to first OPC | 14 (10–21) | 20 (14–23) | 11 (9–14) | <0.01 |
| Number of “did-not-attend” clinic | 0 (0–1) | 0 (0–1) | 0 (0–1) | Not applicable |
| Surgery | ||||
| Yes | 22/61 (36%) | 20/32 (63%) | 2/30 (7%) | <0.01 |
| Days to surgery | 2 (1–6) | 2 (1–5) | 9 (7–10) | Not assessed |
| Anatomical Location | Total Cohort (n = 61) | Operative Management (n = 22) | Non-Operative Management (n = 39) |
|---|---|---|---|
| Upper Limb Injuries | 33 | ||
| Scapula | 2 | 0 | 2 |
| AC Joint Dislocation | 1 | 0 | 1 |
| Clavicle | 6 | 1 | 5 |
| Humerus | 4 | 1 | 3 |
| Radius | 20 | 3 | 17 |
| Lower Limb Injuries | 31 | ||
| Pelvis | 5 | 4 | 1 |
| Neck of femur | 1 | 1 | 0 |
| Femoral shaft | 3 | 3 | 0 |
| Tibial plateau | 4 | 4 | 0 |
| Tibial shaft | 8 | 5 | 3 |
| Fibula | 4 | 4 | 0 |
| Patella | 1 | 1 | 0 |
| Ligamentous Knee Injury | 2 | 2 | 0 |
| Ankle | 3 | 1 | 2 |
| Spinal Injuries | 11 | ||
| Cervical Spine | 3 | 1 | 0 |
| Thoracic Spine | 5 | 1 | 4 |
| Lumbar Spine | 3 | 1 | 2 |
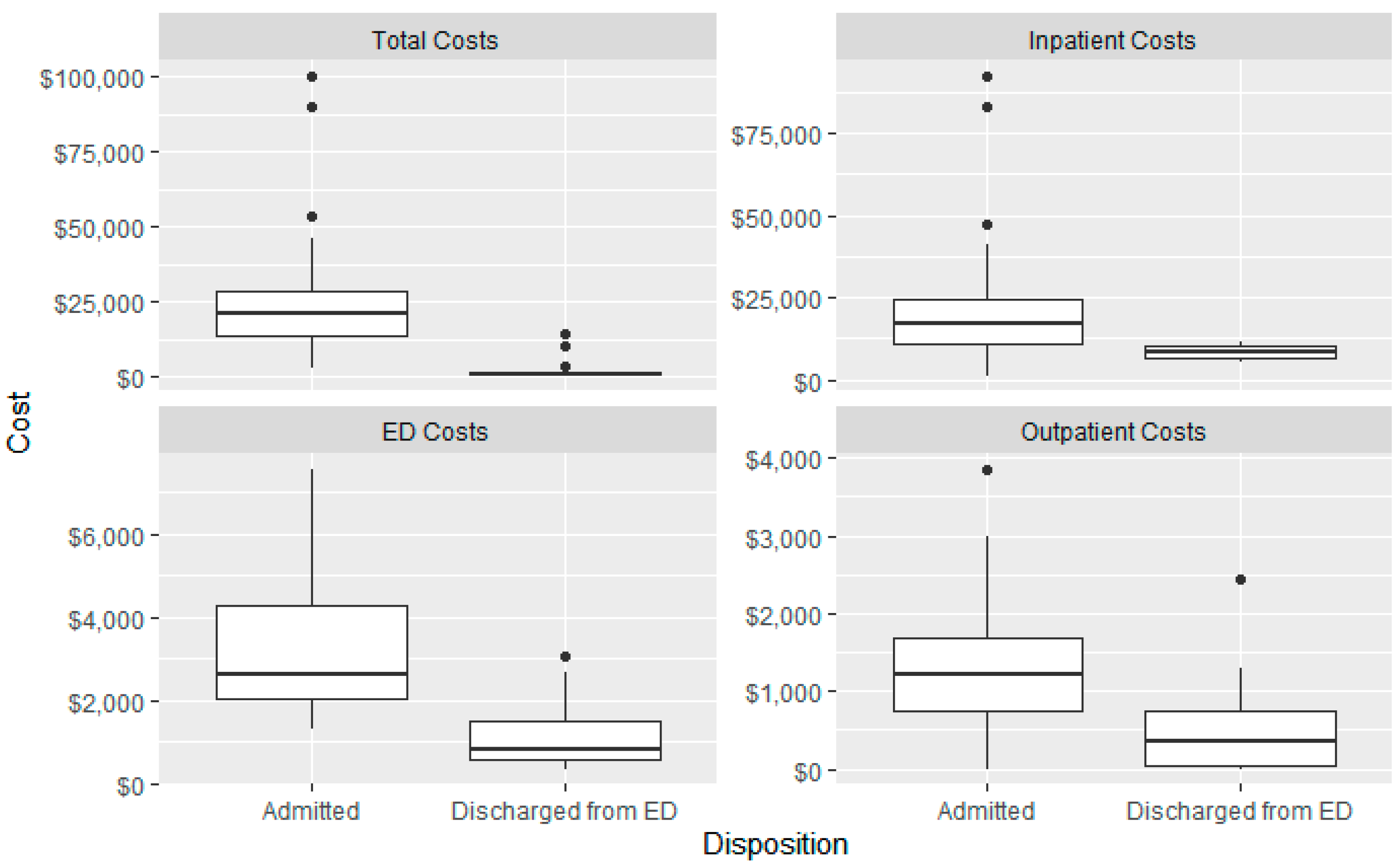
| Cost Type | Median Cost (IQR) |
|---|---|
| ED Costs | AU$1748.30 (AU$937.20–AU$2763.90) |
| Inpatient Costs | AU$16,236.00 (AU$8936.00–AU$24,099.00) |
| Outpatient Costs | AU$756.40 (AU$ 122.80–AU$1283.10) |
| Total Costs | AU$5880.60 (AU$1283.10–AU$21,150.90) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raubenheimer, K.; Szeliga, K.; Manara, J.R.; Fatovich, D.M.; Plant, J.G.A.; Blakeney, W.G. Incidence, Management, and Hospital Costs of Orthopaedic Injuries of E-Scooter Riders in Western Australia. J. Clin. Med. 2023, 12, 6591. https://doi.org/10.3390/jcm12206591
Raubenheimer K, Szeliga K, Manara JR, Fatovich DM, Plant JGA, Blakeney WG. Incidence, Management, and Hospital Costs of Orthopaedic Injuries of E-Scooter Riders in Western Australia. Journal of Clinical Medicine. 2023; 12(20):6591. https://doi.org/10.3390/jcm12206591
Chicago/Turabian StyleRaubenheimer, Kyle, Katherine Szeliga, Jonathan R. Manara, Daniel M. Fatovich, James G. A. Plant, and William G. Blakeney. 2023. "Incidence, Management, and Hospital Costs of Orthopaedic Injuries of E-Scooter Riders in Western Australia" Journal of Clinical Medicine 12, no. 20: 6591. https://doi.org/10.3390/jcm12206591
APA StyleRaubenheimer, K., Szeliga, K., Manara, J. R., Fatovich, D. M., Plant, J. G. A., & Blakeney, W. G. (2023). Incidence, Management, and Hospital Costs of Orthopaedic Injuries of E-Scooter Riders in Western Australia. Journal of Clinical Medicine, 12(20), 6591. https://doi.org/10.3390/jcm12206591