Relationship between Cervical Instability in the Course of Rheumatoid Arthritis and Pelvic Parameters of Sagittal Balance


 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
- At the C2–C3 level, the axial load of the skull and spine is divided.
- At the C2–C3 level, a connection/combination of two functionally and anatomically different parts of the cervical section occurs, i.e., the supraspinatus part, in which the structure, apart from flexion and extension, is subordinated to rotational function and is responsible for 75% of this movement of the occiput in relation to C2, and the subscapularis part, in which flexion, extension and lateral flexion are dominant [6].
- In a study of the impact of the instantaneous center of rotation (ICR) on the pathology of the cervical spine, it was found that most of the abnormal ICRs associated with neck pain are located at the C2–C3 and C3–C4 levels [39]. However, it has not yet been confirmed that an abnormal ICR is an indicator of damage to this segment. It has been found that it can be used to determine whether it is associated with muscle tone disorders or ligament tone disorders [6]. In both cases, we are dealing with a situation that corresponds to the response to overloading of the spinal structures.
5. Conclusions
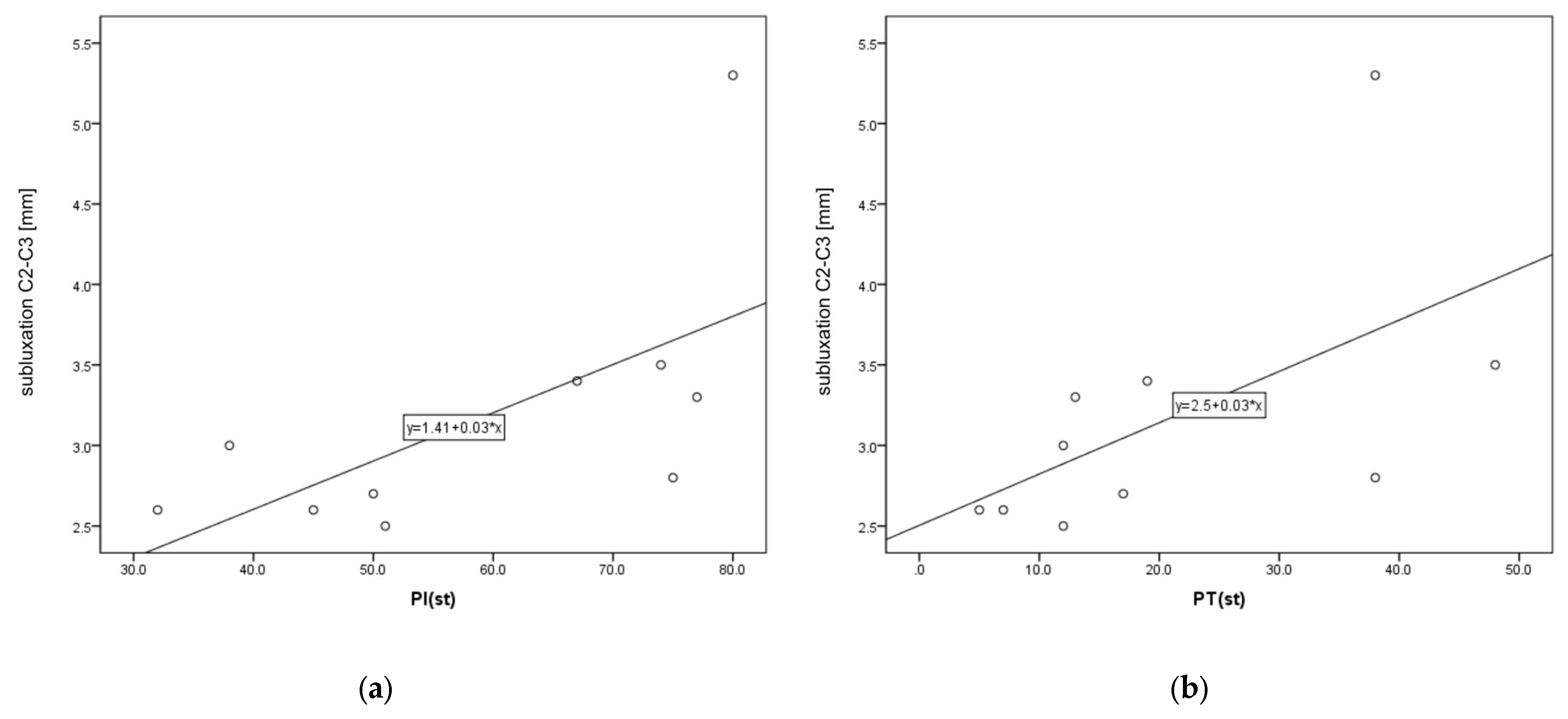
- A statistically significant positive correlation was found between C2–C3 instability and PI and PT. There was no statistical correlation between the pelvic parameters and LL and other levels of instability.
- A statistically significant negative correlation was observed between C1–C2 instability and the age of patients.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; Barton, A.; Burmester, G.R.; Emery, P.; Firestein, G.S.; Kavanaugh, A.; McInnes, I.B.; Solomon, D.H.; Strand, V.; et al. Rheumatoid arthritis. Nat. Rev. Dis. Primers 2018, 4, 18001. [Google Scholar] [CrossRef] [PubMed]
- Szczeklik, A. Interna 2020; Medycyna Praktyczna: Kraków, Poland, 2020; pp. 2030–2045. [Google Scholar]
- Canale, S.T.; Beaty, J.H. Campbell’s Operative Orthopedics, 12th ed.; MediPage: Warszawa, Poland, 2016; pp. 2019–2022. [Google Scholar]
- Wasserman, B.R.; Moskovich, R.; Razi, A.E. Rheumatoid arthritis of the cervical spine—Clinical considerations. Bull. NYU Hosp. Jt. Dis. 2011, 69, 136–148. [Google Scholar] [PubMed]
- Gillick, J.L.; Wainwright, J.; Das, K. Rheumatoid arthritis and the cervical spine: A review on the role of surgery. Int. J. Rheumatol. 2015, 2015, 252456. [Google Scholar] [CrossRef] [PubMed]
- Bogduk, N.; Mercer, S. Biomechanics of the cervical spine. I: Normal kinematics. Clin. Biomech. 2000, 15, 633–648. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.V.; Ludwig, S.C.; Silber, J.; Gelb, D.E.; Anderson, P.A.; Frank, L.; Vaccaro, A.R. Rheumatoid arthritis of the cervical spine. Spine J. 2004, 4, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Mathews, J.A. Wasting of the small hand muscles in upper and mid-cervical cord lesions. QJM 1998, 91, 691–700. [Google Scholar] [CrossRef][Green Version]
- Neva, M.H.; Myllykangas-Luosujarvi, R.; Kauppi, M. Mortality associated with cervical spine disorders: A population—Based study of 1666 patients with rheumatoid arthritis who died in Finland in 1989. Rheumatology 2001, 40, 123–127. [Google Scholar] [CrossRef][Green Version]
- Krauss, W.E.; Bledsoe, J.M.; Clarke, M.J.; Nottmeier, E.W.; Pichelmann, M.A. Rheumatoid arthritis of the craniovertebral junction. Neurosurgery 2010, 66 (Suppl. S3), 83–95. [Google Scholar] [CrossRef]
- Mańczak, M.; Gasik, R. Cervical spine instability in the course of rheumatoid arthritis—Imaging methods. Reumatologia 2017, 55, 201–207. [Google Scholar] [CrossRef]
- Zhu, S.; Xu, W.; Luo, Y.; Zhao, Y.; Liu, Y. Cervical spine involvement risk factors in rheumatoid arthritis: A meta-analysis. Int. J. Rheum. Dis. 2017, 20, 541–549. [Google Scholar] [CrossRef]
- Geraldo-Flores, N.A.; Merlos-López, R.J.; Rodríguez-Wong, J.A.; Ramírez-Hernández, S.; Espino-Lizarraga, M.J.; Pérez-Atanasio, J.M. La severidad de la artritisreumatoidecomo predictor oportuno de inestabilidad de la columna cervical asintomática [The severity of rheumatoid arthritis as a timely predictor of instability in the asymptomatic cervical spine]. Acta Ortop. Mex. 2018, 32, 342–346. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Yurube, T.; Sumi, M.; Nishida, K.; Miyamoto, H.; Kohyama, K.; Matsubara, T.; Miura, Y.; Hirata, H.; Sugiyama, D.; Doita, M. Accelerated development of cervical spine instabilities in rheumatoid arthritis: A prospective minimum 5-year cohort study. PLoS ONE 2014, 9, e88970. [Google Scholar] [CrossRef] [PubMed]
- Terashima, Y.; Yurube, T.; Hirata, H.; Sugiyama, D.; Sumi, M.; Hyogo Organization of Spinal Disorders. Predictive Risk Factors of Cervical Spine Instabilities in Rheumatoid Arthritis: A Prospective Multicenter Over 10-Year Cohort Study. Spine 2017, 42, 556–564. [Google Scholar] [CrossRef]
- Baek, I.W.; Joo, Y.B.; Park, K.S.; Kim, K.J. Risk factors for cervical spine instability in patients with rheumatoid arthritis. Clin. Rheumatol. 2021, 40, 547–555. [Google Scholar] [CrossRef] [PubMed]
- Kaito, T.; Ohshima, S.; Fujiwara, H.; Makino, T.; Takenaka, S.; Sakai, Y.; Yoshikawa, H. Predictors for progression of two different types of cervical lesions in rheumatoid arthritis treated with biologic agents. J. Orthop. Sci. 2019, 24, 214–218. [Google Scholar] [CrossRef]
- Dubousset, J. Spinal Alignment, Balance and Harmony through the Ages. Int. J. Orth. 2019, 2, 019–024. [Google Scholar]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Colebatch, A.N.; Edwards, C.J.; Østergaard, M.; van der Heijde, D.; Balint, P.V.; D’Agostino, M.-A.; Forslind, K.; Grassi, W.; Haavardsholm, E.A.; Haugeberg, G.; et al. EULAR recommendations for the use of imaging of the joints in the clinical management of rheumatoid arthritis. Ann. Rheum. Dis. 2013, 72, 804–814. [Google Scholar] [CrossRef]
- Joaquim, A.F.; Ghizoni, E.; Tedeschi, H.; Appenzeller, S.; Riew, K.D. Radiological evaluation of cervical spine involvement in rheumatoid arthritis. Neurosurg. Focus 2015, 38, E4. [Google Scholar] [CrossRef]
- Siempis, T.; Tsakiris, C.; Anastasia, Z.; Alexiou, G.A.; Voulgaris, S.; Argyropoulou, M.I. Radiological assessment and surgical management of cervical spine involvement in patients with rheumatoid arthritis. Rheumatol. Int. 2023, 43, 195–208. [Google Scholar] [CrossRef]
- Yurube, T.; Sumi, M.; Nishida, K.; Miyamoto, H.; Kohyama, K.; Matsubara, T.; Miura, Y.; Sugiyama, D.; Doita, M.; Kobe Spine Conference. Incidence and aggravation of cervical spine instabilities in rheumatoid arthritis: A prospective minimum 5-year follow-up study of patients initially without cervical involvement. Spine 2012, 37, 2136–2144. [Google Scholar] [CrossRef]
- Yonezawa, T.; Tsuji, H.; Matsui, H.; Hirano, N. Subaxial lesions in rheumatoid arthritis. Radiographic factors suggestive of lower cervical myelopathy. Spine 1995, 20, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Faro, F.D.; Marks, M.C.; Pawelek, J.; Newton, P.O. Evaluation of a functional position for lateral radiograph acquisition in adolescent idiopathic scoliosis. Spine 2004, 29, 2284–2289. [Google Scholar] [CrossRef] [PubMed]
- Cirillo Totera, J.I.; Fleiderman Valenzuela, J.G.; Garrido Arancibia, J.A.; Pantoja Contreras, S.T.; Beaulieu Lalanne, L.; Alvarez-Lemos, F.L. Sagittal balance: From theory to clinical practice. EFORT Open Rev. 2021, 6, 1193–1202. [Google Scholar] [CrossRef] [PubMed]
- Masamoto, K.; Otsuki, B.; Fujibayashi, S.; Shima, K.; Ito, H.; Furu, M.; Hashimoto, M.; Tanaka, M.; Lyman, S.; Yoshitomi, H.; et al. Factors influencing spinal sagittal balance, bone mineral density, and Oswestry Disability Index outcome measures in patients with rheumatoid arthritis. Eur. Spine J. 2018, 27, 406–415. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Lee, J.S.; Shin, J.K.; Goh, T.S. Correlations Between Sagittal Spinal Balance and Quality of Life in Rheumatoid Arthritis. Clin. Spine Surg. 2017, 30, E412–E417. [Google Scholar] [CrossRef]
- Ha, B.J.; Won, Y.D.; Ryu, J.I.; Han, M.H.; Cheong, J.H.; Kim, J.M.; Chun, H.J.; Bak, K.H.; Bae, I.S. Relationship between the atlantodental interval and T1 slope after atlantoaxial fusion in patients with rheumatoid arthritis. BMC Surg. 2020, 20, 269. [Google Scholar] [CrossRef]
- Iizuka, H.; Iizuka, Y.; Okamura, K.; Yonemoto, Y.; Mieda, T.; Takagishi, K. Bony ankylosis of the facet joint of the cervical spine in rheumatoid arthritis: Its characteristics and relationship to the clinical findings. Mod. Rheumatol. 2017, 27, 801–805. [Google Scholar] [CrossRef]
- Ito, H.; Neo, M.; Sakamoto, T.; Fujibayashi, S.; Yoshitomi, H.; Nakamura, T. Subaxial subluxation after atlantoaxial transarticular screw fixation in rheumatoid patients. Eur. Spine J. 2009, 18, 869–876. [Google Scholar] [CrossRef]
- Wu, X.; Qi, Y.; Tan, M.; Yi, P.; Yang, F.; Tang, X.; Hao, Q. Incidence and risk factors for adjacent segment degeneration following occipitoaxial fusion for atlantoaxial instability in non-rheumatoid arthritis. Arch. Orthop. Trauma Surg. 2018, 138, 921–927. [Google Scholar] [CrossRef]
- Kurogochi, D.; Takahashi, J.; Uehara, M.; Ikegami, S.; Kuraishi, S.; Futatsugi, T.; Oba, H.; Takizawa, T.; Munakata, R.; Hatakenaka, T.; et al. Ten-Year Results of Reconstruction for Rheumatoid Cervical Spine Lesions and Occurrence Factor of Subaxial Subluxation. Asian Spine J. 2019, 13, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Barrey, C.; Roussouly, P.; Le Huec, J.C.; D’Acunzi, G.; Perrin, G. Compensatory mechanisms contributing to keep the sagittal balance of the spine. Eur. Spine J. 2013, 22 (Suppl. S6), S834–S841. [Google Scholar] [CrossRef]
- Roussouly, P.; Pinheiro-Franco, J.; Labelle, H.; Gechren, M. Sagittal Balance of the Spine: From Normal to Pathology: A Key for Treatment Strategy, 1st ed.; Normative Values Following Age and Populations; Thieme: New York, NY, USA, 2019; pp. 74–79. [Google Scholar]
- Błaszczyk, J. Biomechanikakliniczna, Podręcznikdlastudentówmedycynyifizjoterapii; WydawnictwoLekarskie PZWL: Warszawa, Poland, 2004; pp. 19–23. [Google Scholar]
- Scheer, J.K.; Tang, J.A.; Smith, J.S.; Acosta, F.L., Jr.; Protopsaltis, T.S.; Blondel, B.; Bess, S.; Shaffrey, C.I.; Deviren, V.; Lafage, V.; et al. Cervical spine alignment, sagittal deformity, and clinical implications: A review. J. Neurosurg. Spine 2013, 19, 141–159. [Google Scholar] [CrossRef] [PubMed]
- Louis, R. Spinal stability as defined by the three-column spine concept. Anat. Clin. 1985, 7, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Amevo, B.; Aprill, C.; Bogduk, N. Abnormal instantaneous axes of rotation in patients with neck pain. Spine 1992, 17, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Duval-Beaupère, G.; Schmidt, C.; Cosson, P. A Barycentremetric study of the sagittal shape of spine and pelvis: The conditions required for an economic standing position. Ann. Biomed. Eng. 1992, 20, 451–462. [Google Scholar] [CrossRef]
- During, J.; Goudfrooij, H.; Keessen, W.; Beeker, T.W.; Crowe, A. Toward standards for posture. Postural characteristics of the lower back system in normal and pathologic conditions. Spine 1985, 10, 83–87. [Google Scholar] [CrossRef]
- Legaye, J.; Duval-Beaupère, G.; Hecquet, J.; Marty, C. Pelvic incidence: A fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur. Spine J. 1998, 7, 99–103. [Google Scholar] [CrossRef]
- Jackson, R.P.; McManus, A.C. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size. A prospective controlled clinical study. Spine 1994, 19, 1611–1618. [Google Scholar] [CrossRef]
- Kim, Y.C.; Lenke, L.G.; Lee, S.J.; Gum, J.L.; Wilartratsami, S.; Blanke, K.M. The cranial sagittal vertical axis (CrSVA) is a better radiographic measure to predict clinical outcomes in adult spinal deformity surgery than the C7 SVA: A monocentric study. Eur. Spine J. 2017, 26, 2167–2175. [Google Scholar] [CrossRef]
- Schwab, F.; Lafage, V.; Boyce, R.; Skalli, W.; Farcy, J.P. Gravity line analysis in adult volunteers: Age-related correlation with spinal parameters, pelvic parameters, and foot position. Spine 2006, 31, E959–E967. [Google Scholar] [CrossRef] [PubMed]
- Roussouly, P.; Pinheiro-Franco, J.L. Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur. Spine J. 2011, 20 (Suppl. S5), 609–618. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Instability | Definition |
|---|---|
| AAS (atlantoaxial subluxation) | Weakening or rupture of ligaments and subchondral bone erosion in the atlantoaxial C1–C2 joints. |
| SAS (subaxial subluxation) | Subluxation in the joints C2–C7 due to destruction of the joint surface and the ligaments between the processes spinosis. |
| CS (cranial settling) | Vertical translocation of dens C0–C2 into the foramen magnum. |
| Parameter | Definition |
|---|---|
| LL (Lumbar Lordosis) | Measured between the upper endplate L1 and the upper endplate S1. |
| PI (Pelvic Incidence) | The angle formed between the perpendicular line to the center point of the superior sacrum endplate surface and the line connecting from the said center point to the center of the femur head. |
| PT (Pelvic Tilt) | This is the angle between the upper plumb line from the femur head center and the center point of the superior sacrum endplate surface. |
| SS (Sacral Slope) | This is the angle between a horizontal line and the slope of the superior sacral endplate surface. |
| C1–C2 (n = 47) | C1–C2 AAS (n = 27) | C2–C3 SAS (n = 10) | C3–C4 SAS (n = 15) | C4–C5 SAS (n = 21) | C5–C6 SAS (n = 9) | |
|---|---|---|---|---|---|---|
| LL(st) | 0.041 | 0.006 | −0.322 | −0.168 | −0.084 | 0.443 |
| PI(st) | 0.077 | −0.238 | 0.663 | 0.320 | −0.084 | −0.219 |
| PT(st) | 0.164 | −0.014 | 0.758 | 0.213 | 0.132 | −0.266 |
| SS(st) | −0.005 | −0.316 | 0.215 | 0.323 | −0.156 | 0.184 |
| age | −0.303 | −0.073 | −0.261 | 0.050 | 0.168 | −0.333 |
| disease duration | 0.133 | 0.081 | 0.500 | −0.463 | 0.315 | −0.545 |
| AAS | Without AAS | p | |||
|---|---|---|---|---|---|
| Me (IQR) | n | Me (IQR) | n | ||
| LL(st) | 54 (30–64) | 27 | 48 (34–56) | 20 | 0.576 |
| PI(st) | 53 (44–69) | 27 | 49 (41–56) | 19 | 0.246 |
| PT(st) | 16 (12–28) | 27 | 18 (13–20) | 19 | 0.441 |
| SS(st) | 36 (27–42) | 27 | 32 (26–38) | 20 | 0.401 |
| age | 64 (58–70) | 27 | 71 (63–76) | 20 | 0.039 |
| disease duration | 20 (12–30) | 26 | 15 (10–25) | 19 | 0.395 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wróblewski, R.; Koszela, K.; Mańczak, M.; Sudoł-Szopińska, I.; Gasik, R. Relationship between Cervical Instability in the Course of Rheumatoid Arthritis and Pelvic Parameters of Sagittal Balance. J. Clin. Med. 2023, 12, 6507. https://doi.org/10.3390/jcm12206507
Wróblewski R, Koszela K, Mańczak M, Sudoł-Szopińska I, Gasik R. Relationship between Cervical Instability in the Course of Rheumatoid Arthritis and Pelvic Parameters of Sagittal Balance. Journal of Clinical Medicine. 2023; 12(20):6507. https://doi.org/10.3390/jcm12206507
Chicago/Turabian StyleWróblewski, Robert, Kamil Koszela, Małgorzata Mańczak, Iwona Sudoł-Szopińska, and Robert Gasik. 2023. "Relationship between Cervical Instability in the Course of Rheumatoid Arthritis and Pelvic Parameters of Sagittal Balance" Journal of Clinical Medicine 12, no. 20: 6507. https://doi.org/10.3390/jcm12206507
APA StyleWróblewski, R., Koszela, K., Mańczak, M., Sudoł-Szopińska, I., & Gasik, R. (2023). Relationship between Cervical Instability in the Course of Rheumatoid Arthritis and Pelvic Parameters of Sagittal Balance. Journal of Clinical Medicine, 12(20), 6507. https://doi.org/10.3390/jcm12206507