
Mechanisms and Prediction of Ischemic Stroke in Atrial Fibrillation Patients


Abstract
1. Introduction
2. Left Atrial Properties and Ischemic Stroke
2.1. Migration of Cardiac Thrombi
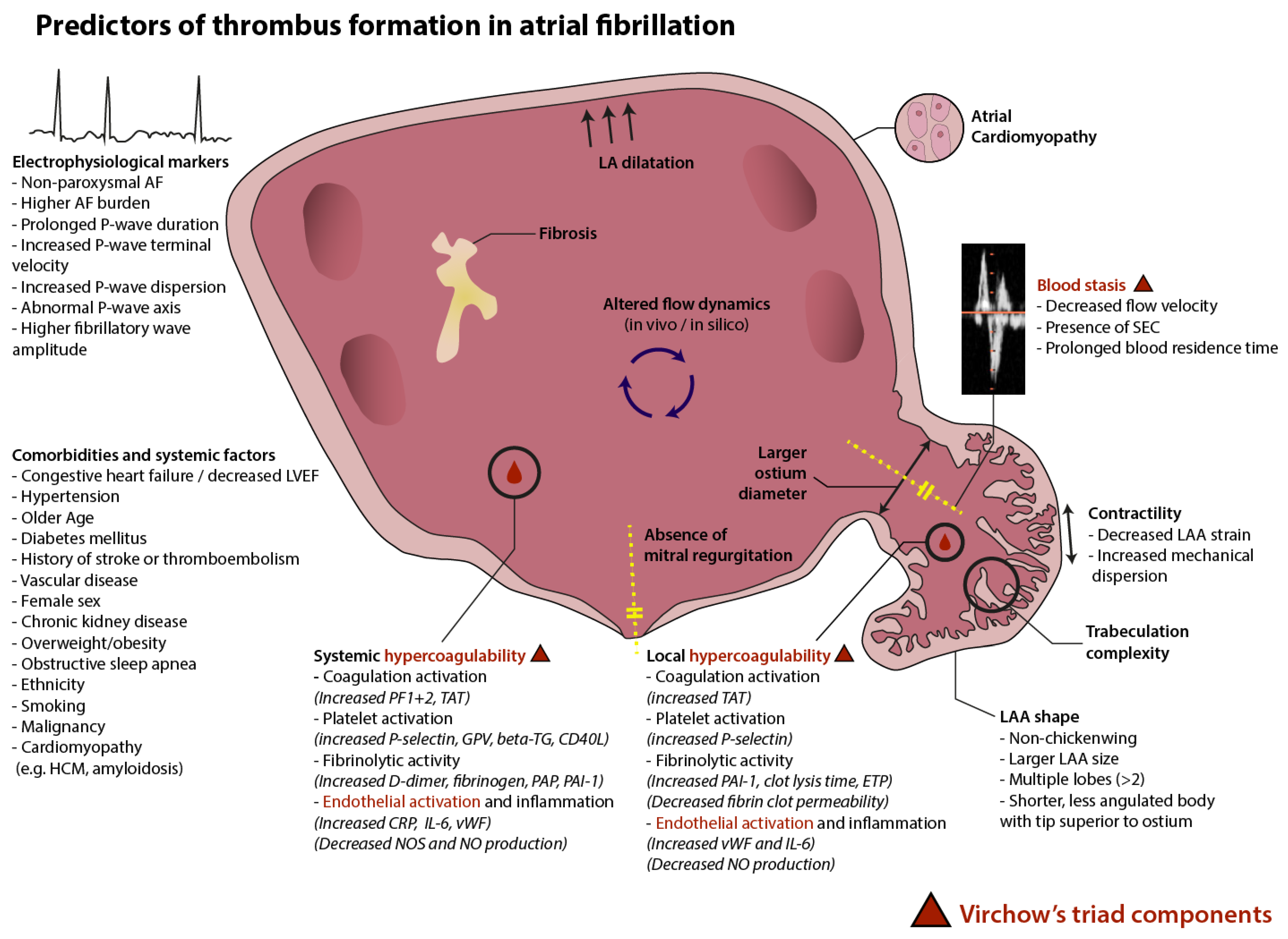
2.2. Virchow’s Triad in Atrial Fibrillation
2.3. Atrial Remodeling, Fibrosis, and Atrial Fibrillation
2.4. Atrial Cardiomyopathy
3. The Left Atrial Appendage as the Cradle of Thrombi
3.1. Morphologic Features
3.2. Flow Dynamics
3.3. Local Prothrombotic Milieu
4. Temporal Association between AF and Stroke
5. Comorbidities and Vascular Risk Profile
6. Future Directions
6.1. Causality of AF in Stroke
6.2. The Need for Improved Risk Stratification
6.3. A Dynamic Evaluation
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, Regional, and National Burden of Stroke and Its Risk Factors, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Wolf, P.A.; Abbott, R.D.; Kannel, W.B. Atrial Fibrillation as an Independent Risk Factor for Stroke: The Framingham Study. Stroke 1991, 22, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Stead, L.G.; Gilmore, R.M.; Bellolio, M.F.; Jain, A.; Rabinstein, A.A.; Decker, W.W.; Agarwal, D.; Brown, R.D. Cardioembolic but Not Other Stroke Subtypes Predict Mortality Independent of Stroke Severity at Presentation. Stroke Res. Treat. 2011, 2011, 281496. [Google Scholar] [CrossRef] [PubMed]
- Saxena, R.; Lewis, S.; Berge, E.; Sandercock, P.A.; Koudstaal, P.J. Risk of Early Death and Recurrent Stroke and Effect of Heparin in 3169 Patients with Acute Ischemic Stroke and Atrial Fibrillation in the International Stroke Trial. Stroke 2001, 32, 2333–2337. [Google Scholar] [CrossRef] [PubMed]
- Ayerbe, L.; Ayis, S.; Wolfe, C.D.A.; Rudd, A.G. Natural History, Predictors and Outcomes of Depression after Stroke: Systematic Review and Meta-Analysis. Br. J. Psychiatry J. Ment. Sci. 2013, 202, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Van Langevelde, K.; Šrámek, A.; Vincken, P.W.J.; van Rooden, J.K.; Rosendaal, F.R.; Cannegieter, S.C. Finding the Origin of Pulmonary Emboli with a Total-Body Magnetic Resonance Direct Thrombus Imaging Technique. Haematologica 2013, 98, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Laredo, C.; Zhao, Y.; Rudilosso, S.; Renú, A.; Pariente, J.C.; Chamorro, Á.; Urra, X. Prognostic Significance of Infarct Size and Location: The Case of Insular Stroke. Sci. Rep. 2018, 8, 9498. [Google Scholar] [CrossRef] [PubMed]
- Ding, W.Y.; Gupta, D.; Lip, G.Y.H. Atrial Fibrillation and the Prothrombotic State: Revisiting Virchow’s Triad in 2020. Heart 2020, 106, 1463–1468. [Google Scholar] [CrossRef]
- Zotz, R.J.; Müller, M.; Genth-Zotz, S.; Darius, H. Spontaneous Echo Contrast Caused by Platelet and Leukocyte Aggregates? Stroke 2001, 32, 1127–1133. [Google Scholar] [CrossRef]
- Fatkin, D.; Kelly, R.P.; Feneley, M.P. Relations between Left Atrial Appendage Blood Flow Velocity, Spontaneous Echocardiographic Contrast and Thromboembolic Risk in Vivo. J. Am. Coll. Cardiol. 1994, 23, 961–969. [Google Scholar] [CrossRef]
- Asakura, H.; Hifumi, S.; Jokaji, H.; Saito, M.; Kumabashiri, I.; Uotani, C.; Morishita, E.; Yamazaki, M.; Shibata, K.; Mizuhashi, K. Prothrombin Fragment F1 + 2 and Thrombin-Antithrombin III Complex Are Useful Markers of the Hypercoagulable State in Atrial Fibrillation. Blood Coagul. Fibrinolysis Int. J. Haemost. Thromb. 1992, 3, 469–473. [Google Scholar] [CrossRef]
- Wu, N.; Tong, S.; Xiang, Y.; Wu, L.; Xu, B.; Zhang, Y.; Ma, X.; Li, Y.; Song, Z.; Zhong, L. Association of Hemostatic Markers with Atrial Fibrillation: A Meta-Analysis and Meta-Regression. PLoS ONE 2015, 10, e0124716. [Google Scholar] [CrossRef] [PubMed]
- Ohara, K.; Inoue, H.; Nozawa, T.; Hirai, T.; Iwasa, A.; Okumura, K.; Lee, J.-D.; Shimizu, A.; Hayano, M.; Yano, K. Accumulation of Risk Factors Enhances the Prothrombotic State in Atrial Fibrillation. Int. J. Cardiol. 2008, 126, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Siegbahn, A.; Oldgren, J.; Andersson, U.; Ezekowitz, M.D.; Reilly, P.A.; Connolly, S.J.; Yusuf, S.; Wallentin, L.; Eikelboom, J.W. D-Dimer and Factor VIIa in Atrial Fibrillation—Prognostic Values for Cardiovascular Events and Effects of Anticoagulation Therapy. A RE-LY Substudy. Thromb. Haemost. 2016, 115, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Christersson, C.; Wallentin, L.; Andersson, U.; Alexander, J.H.; Ansell, J.; De Caterina, R.; Gersh, B.J.; Granger, C.B.; Hanna, M.; Horowitz, J.D.; et al. D-Dimer and Risk of Thromboembolic and Bleeding Events in Patients with Atrial Fibrillation—Observations from the ARISTOTLE Trial. J. Thromb. Haemost. 2014, 12, 1401–1412. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Hirai, T.; Nakagawa, K.; Kameyama, T.; Nozawa, T.; Asanoi, H.; Inoue, H. Left Atrial Appendage Function and Abnormal Hypercoagulability in Patients with Atrial Flutter. Chest 2003, 124, 1670–1674. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, W.M.; Macy, E.; Cornell, E.S.; Nightingale, S.D.; Pearce, L.A.; Tracy, R.P.; Bovill, E.G. Plasmin-Alpha2-Antiplasmin Complex in Patients with Atrial Fibrillation. Stroke Prevention in Atrial Fibrillation Investigators. Thromb. Haemost. 1999, 82, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Mulder, B.A.; Geelhoed, B.; van der Harst, P.; Spronk, H.M.; Van Gelder, I.C.; Asselbergs, F.W.; Rienstra, M. Plasminogen Activator Inhibitor-1 and Tissue Plasminogen Activator and Incident AF: Data from the PREVEND Study. Int. J. Cardiol. 2018, 272, 208–210. [Google Scholar] [CrossRef]
- Wu, N.; Chen, X.; Cai, T.; Wu, L.; Xiang, Y.; Zhang, M.; Li, Y.; Song, Z.; Zhong, L. Association of Inflammatory and Hemostatic Markers with Stroke and Thromboembolic Events in Atrial Fibrillation: A Systematic Review and Meta-Analysis. Can. J. Cardiol. 2015, 31, 278–286. [Google Scholar] [CrossRef]
- Wang, X.; Xu, X.; Wang, W.; Huang, H.; Liu, F.; Wan, C.; Yao, Q.; Li, H.; Zhang, Z.; Song, Z. Risk Factors Associated with Left Atrial Appendage Thrombosis in Patients with Non-Valvular Atrial Fibrillation by Transesophageal Echocardiography. Int. J. Cardiovasc. Imaging 2023, 39, 1263–1273. [Google Scholar] [CrossRef]
- Drabik, L.; Wołkow, P.; Undas, A. Fibrin Clot Permeability as a Predictor of Stroke and Bleeding in Anticoagulated Patients with Atrial Fibrillation. Stroke 2017, 48, 2716–2722. [Google Scholar] [CrossRef]
- Baidildinova, G.; Nagy, M.; Jurk, K.; Wild, P.S.; ten Cate, H.; van der Meijden, P.E.J. Soluble Platelet Release Factors as Biomarkers for Cardiovascular Disease. Front. Cardiovasc. Med. 2021, 8, 684920. [Google Scholar] [CrossRef] [PubMed]
- Swiatkowska, M.; Cierniewska-Cieslak, A.; Pawlowska, Z.; Cierniewski, C.S. Dual Regulatory Effects of Nitric Oxide on Plasminogen Activator Inhibitor Type 1 Expression in Endothelial Cells. Eur. J. Biochem. 2000, 267, 1001–1007. [Google Scholar] [CrossRef] [PubMed]
- Conway, D.S.G.; Pearce, L.A.; Chin, B.S.P.; Hart, R.G.; Lip, G.Y.H. Prognostic Value of Plasma von Willebrand Factor and Soluble P-Selectin as Indices of Endothelial Damage and Platelet Activation in 994 Patients with Nonvalvular Atrial Fibrillation. Circulation 2003, 107, 3141–3145. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chung, M.K.; Martin, D.O.; Sprecher, D.; Wazni, O.; Kanderian, A.; Carnes, C.A.; Bauer, J.A.; Tchou, P.J.; Niebauer, M.J.; Natale, A.; et al. C-Reactive Protein Elevation in Patients with Atrial Arrhythmias: Inflammatory Mechanisms and Persistence of Atrial Fibrillation. Circulation 2001, 104, 2886–2891. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Takeishi, Y.; Hirono, O.; Itoh, M.; Matsui, M.; Nakamura, K.; Tamada, Y.; Kubota, I. C-Reactive Protein Elevation Predicts the Occurrence of Atrial Structural Remodeling in Patients with Paroxysmal Atrial Fibrillation. Heart Vessel. 2005, 20, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Lip, G.Y.H. The Prothrombotic State in Atrial Fibrillation: Pathophysiological and Management Implications. Cardiovasc. Res. 2019, 115, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Nattel, S.; Burstein, B.; Dobrev, D. Atrial Remodeling and Atrial Fibrillation: Mechanisms and Implications. Circ. Arrhythm. Electrophysiol. 2008, 1, 62–73. [Google Scholar] [CrossRef] [PubMed]
- Wijffels, M.C.; Kirchhof, C.J.; Dorland, R.; Allessie, M.A. Atrial Fibrillation Begets Atrial Fibrillation. A Study in Awake Chronically Instrumented Goats. Circulation 1995, 92, 1954–1968. [Google Scholar] [CrossRef]
- Dittrich, H.C.; Pearce, L.A.; Asinger, R.W.; McBride, R.; Webel, R.; Zabalgoitia, M.; Pennock, G.D.; Safford, R.E.; Rothbart, R.M.; Halperin, J.L.; et al. Left Atrial Diameter in Nonvalvular Atrial Fibrillation: An Echocardiographic Study. Am. Heart J. 1999, 137, 494–499. [Google Scholar] [CrossRef]
- Sanfilippo, A.J.; Abascal, V.M.; Sheehan, M.; Oertel, L.B.; Harrigan, P.; Hughes, R.A.; Weyman, A.E. Atrial Enlargement as a Consequence of Atrial Fibrillation. A Prospective Echocardiographic Study. Circulation 1990, 82, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Vinereanu, D.; Lopes, R.D.; Mulder, H.; Gersh, B.J.; Hanna, M.; de Barros E Silva, P.G.M.; Atar, D.; Wallentin, L.; Granger, C.B.; Alexander, J.H. Echocardiographic Risk Factors for Stroke and Outcomes in Patients with Atrial Fibrillation Anticoagulated with Apixaban or Warfarin. Stroke 2017, 48, 3266–3273. [Google Scholar] [CrossRef] [PubMed]
- Jordan, K.; Yaghi, S.; Poppas, A.; Chang, A.D.; Mac Grory, B.; Cutting, S.; Burton, T.; Jayaraman, M.; Tsivgoulis, G.; Sabeh, M.K.; et al. Left Atrial Volume Index Is Associated with Cardioembolic Stroke and Atrial Fibrillation Detection After Embolic Stroke of Undetermined Source. Stroke 2019, 50, 1997–2001. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Seo, Y.; Kawamatsu, N.; Sato, K.; Sugano, A.; Machino-Ohtsuka, T.; Kawamura, R.; Nakajima, H.; Igarashi, M.; Sekiguchi, Y.; et al. Complex Left Atrial Appendage Morphology and Left Atrial Appendage Thrombus Formation in Patients with Atrial Fibrillation. Circ. Cardiovasc. Imaging 2014, 7, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Brambatti, M.; Connolly, S.J.; Gold, M.R.; Morillo, C.A.; Capucci, A.; Muto, C.; Lau, C.P.; Van Gelder, I.C.; Hohnloser, S.H.; Carlson, M.; et al. Temporal Relationship between Subclinical Atrial Fibrillation and Embolic Events. Circulation 2014, 129, 2094–2099. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, N.W.E.; Neefs, J.; Kawasaki, M.; Nariswari, F.A.; Wesselink, R.; Fabrizi, B.; Jongejan, A.; Klaver, M.N.; Havenaar, H.; Hulsman, E.L.; et al. Extracellular Matrix Remodeling Precedes Atrial Fibrillation: Results of the PREDICT-AF Trial. Heart Rhythm. 2021, 18, 2115–2125. [Google Scholar] [CrossRef] [PubMed]
- Daccarett, M.; Badger, T.J.; Akoum, N.; Burgon, N.S.; Mahnkopf, C.; Vergara, G.; Kholmovski, E.; McGann, C.J.; Parker, D.; Brachmann, J.; et al. Association of Left Atrial Fibrosis Detected by Delayed-Enhancement Magnetic Resonance Imaging and the Risk of Stroke in Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2011, 57, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Akoum, N.; Fernandez, G.; Wilson, B.; Mcgann, C.; Kholmovski, E.; Marrouche, N. Association of Atrial Fibrosis Quantified Using LGE-MRI with Atrial Appendage Thrombus and Spontaneous Contrast on Transesophageal Echocardiography in Patients with Atrial Fibrillation. J. Cardiovasc. Electrophysiol. 2013, 24, 1104–1109. [Google Scholar] [CrossRef]
- Lankveld, T.; Zeemering, S.; Scherr, D.; Kuklik, P.; Hoffmann, B.A.; Willems, S.; Pieske, B.; Haïssaguerre, M.; Jaïs, P.; Crijns, H.J.; et al. Atrial Fibrillation Complexity Parameters Derived from Surface ECGs Predict Procedural Outcome and Long-Term Follow-Up of Stepwise Catheter Ablation for Atrial Fibrillation. Circ. Arrhythm. Electrophysiol. 2016, 9, e003354. [Google Scholar] [CrossRef]
- Zeemering, S.; Lankveld, T.A.R.; Bonizzi, P.; Limantoro, I.; Bekkers, S.C.A.M.; Crijns, H.J.G.M.; Schotten, U. The Electrocardiogram as a Predictor of Successful Pharmacological Cardioversion and Progression of Atrial Fibrillation. Europace 2018, 20, e96–e104. [Google Scholar] [CrossRef]
- Wang, Y.-S.; Chen, G.-Y.; Li, X.-H.; Zhou, X.; Li, Y.-G. Prolonged P-Wave Duration Is Associated with Atrial Fibrillation Recurrence after Radiofrequency Catheter Ablation: A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2017, 227, 355–359. [Google Scholar] [CrossRef] [PubMed]
- Kreimer, F.; Backhaus, J.F.; Krogias, C.; Pflaumbaum, A.; Mügge, A.; Gotzmann, M. P-Wave Parameters and Their Association with Thrombi and Spontaneous Echo Contrast in the Left Atrial Appendage. Clin. Cardiol. 2023, 46, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, A.; Norby, F.L.; Roetker, N.S.; Soliman, E.Z.; Koene, R.J.; Rooney, M.R.; O’Neal, W.T.; Shah, A.M.; Claggett, B.L.; Solomon, S.D.; et al. Refining Prediction of Atrial Fibrillation–Related Stroke Using the P 2 -CHA 2 DS 2 -VASc Score: ARIC and MESA. Circulation 2019, 139, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, B.; Karabulut, M.; Eroglu, E.; Tigen, K.; Bayrak, F.; Fotbolcu, H.; Basaran, Y. Fibrillatory Wave Amplitude as a Marker of Left Atrial and Left Atrial Appendage Function, and a Predictor of Thromboembolic Risk in Patients with Rheumatic Mitral Stenosis. Int. J. Cardiol. 2003, 91, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, A.N.; Chew, D.P.; Hartshorne, T.; Selvanayagam, J.B.; Aylward, P.E.; Sanders, P.; McGavigan, A.D. The Impact of Atrial Fibrillation Type on the Risk of Thromboembolism, Mortality, and Bleeding: A Systematic Review and Meta-Analysis. Eur. Heart J. 2016, 37, 1591–1602. [Google Scholar] [CrossRef] [PubMed]
- Healey, J.S.; Alings, M.; Ha, A.; Leong-Sit, P.; Birnie, D.H.; de Graaf, J.J.; Freericks, M.; Verma, A.; Wang, J.; Leong, D.; et al. Subclinical Atrial Fibrillation in Older Patients. Circulation 2017, 136, 1276–1283. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Colaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef] [PubMed]
- Goette, A.; Kalman, J.M.; Aguinaga, L.; Akar, J.; Cabrera, J.A.; Chen, S.A.; Chugh, S.S.; Corradi, D.; D’Avila, A.; Dobrev, D.; et al. EHRA/HRS/APHRS/SOLAECE Expert Consensus on Atrial Cardiomyopathies: Definition, Characterization, and Clinical Implication. EP Eur. 2016, 18, 1455–1490. [Google Scholar] [CrossRef]
- Kamel, H.; Longstreth, W.T.J.; Tirschwell, D.L.; Kronmal, R.A.; Broderick, J.P.; Palesch, Y.Y.; Meinzer, C.; Dillon, C.; Ewing, I.; Spilker, J.A.; et al. The AtRial Cardiopathy and Antithrombotic Drugs in Prevention After Cryptogenic Stroke Randomized Trial: Rationale and Methods. Int. J. Stroke Off. J. Int. Stroke Soc. 2019, 14, 207–214. [Google Scholar] [CrossRef]
- Hart, R.G.; Sharma, M.; Mundl, H.; Kasner, S.E.; Bangdiwala, S.I.; Berkowitz, S.D.; Swaminathan, B.; Lavados, P.; Wang, Y.; Wang, Y.; et al. Rivaroxaban for Stroke Prevention after Embolic Stroke of Undetermined Source. N. Engl. J. Med. 2018, 378, 2191–2201. [Google Scholar] [CrossRef]
- Diener, H.-C.; Sacco, R.L.; Easton, J.D.; Granger, C.B.; Bernstein, R.A.; Uchiyama, S.; Kreuzer, J.; Cronin, L.; Cotton, D.; Grauer, C.; et al. Dabigatran for Prevention of Stroke after Embolic Stroke of Undetermined Source. N. Engl. J. Med. 2019, 380, 1906–1917. [Google Scholar] [CrossRef]
- Alkhouli, M.; Di Biase, L.; Natale, A.; Rihal, C.S.; Holmes, D.R.; Asirvatham, S.; Bartus, K.; Lakkireddy, D.; Friedman, P.A. Nonthrombogenic Roles of the Left Atrial Appendage: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2023, 81, 1063–1075. [Google Scholar] [CrossRef]
- Blackshear, J.L.; Odell, J.A. Appendage Obliteration to Reduce Stroke in Cardiac Surgical Patients with Atrial Fibrillation. Ann. Thorac. Surg. 1996, 61, 755–759. [Google Scholar] [CrossRef]
- Gwak, D.S.; Choi, W.C.; Kim, Y.W.; Kim, Y.S.; Hwang, Y.H. Impact of Left Atrial Appendage Morphology on Recurrence in Embolic Stroke of Undetermined Source and Atrial Cardiopathy. Front. Neurol. 2021, 12, 679320. [Google Scholar] [CrossRef] [PubMed]
- Di Biase, L.; Santangeli, P.; Anselmino, M.; Mohanty, P.; Salvetti, I.; Gili, S.; Horton, R.; Sanchez, J.E.; Bai, R.; Mohanty, S.; et al. Does the Left Atrial Appendage Morphology Correlate with the Risk of Stroke in Patients with Atrial Fibrillation? Results from a Multicenter Study. J. Am. Coll. Cardiol. 2012, 60, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Liang, E.; Fan, S.; Zheng, L.; Du, Z.; Liu, S.; Hu, F.; Fan, X.; Chen, G.; Ding, L.; et al. Relation of Left Atrial Appendage Morphology Determined by Computed Tomography to Prior Stroke or to Increased Risk of Stroke in Patients with Atrial Fibrillation. Am. J. Cardiol. 2019, 123, 1283–1286. [Google Scholar] [CrossRef]
- Ernst, G.; Stöllberger, C.; Abzieher, F.; Veit-Dirscherl, W.; Bonner, E.; Bibus, B.; Schneider, B.; Slany, J. Morphology of the Left Atrial Appendage. Anat. Rec. 1995, 242, 553–561. [Google Scholar] [CrossRef] [PubMed]
- Taina, M.; Vanninen, R.; Hedman, M.; Jäkälä, P.; Kärkkäinen, S.; Tapiola, T.; Sipola, P. Left Atrial Appendage Volume Increased in More than Half of Patients with Cryptogenic Stroke. PLoS ONE 2013, 8, e79519. [Google Scholar] [CrossRef] [PubMed]
- Lei, C.; Gao, Q.; Wei, R.; Li, Q.; Liu, X.; Wu, L.; Yao, Y.; Fan, H.; Zheng, Z. Fractal Geometry Illustrated Left Atrial Appendage Morphology That Predicted Thrombosis and Stroke in Patients with Atrial Fibrillation. Front. Cardiovasc. Med. 2022, 9, 779528. [Google Scholar] [CrossRef]
- Khurram, I.M.; Dewire, J.; Mager, M.; Maqbool, F.; Zimmerman, S.L.; Zipunnikov, V.; Beinart, R.; Marine, J.E.; Spragg, D.D.; Berger, R.D.; et al. Relationship between Left Atrial Appendage Morphology and Stroke in Patients with Atrial Fibrillation. Heart Rhythm 2013, 10, 1843–1849. [Google Scholar] [CrossRef]
- Bieging, E.T.; Morris, A.; Chang, L.; Dagher, L.; Marrouche, N.F.; Cates, J. Statistical Shape Analysis of the Left Atrial Appendage Predicts Stroke in Atrial Fibrillation. Int. J. Cardiovasc. Imaging 2021, 37, 2521–2527. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Candales, A.; Hernandez-Suarez, D.F. Strain Imaging Echocardiography: What Imaging Cardiologists Should Know. Curr. Cardiol. Rev. 2017, 13, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Saraçoğlu, E.; Ural, D.; Kılıç, S.; Vuruşkan, E.; Şahin, T.; Ağaçdiken Ağır, A. Left Atrial Appendage 2D-Strain Assessed by Transesophageal Echocardiography Is Associated with Thromboembolic Risk in Patients with Atrial Fibrillation. Turk Kardiyol. Dern. Ars. Turk Kardiyol. Derneginin Yayin Organidir 2019, 47, 111–121. [Google Scholar] [CrossRef]
- Ono, K.; Iwama, M.; Kawasaki, M.; Tanaka, R.; Watanabe, T.; Onishi, N.; Warita, S.; Kojima, T.; Kato, T.; Goto, Y.; et al. Motion of Left Atrial Appendage as a Determinant of Thrombus Formation in Patients with a Low CHADS2 Score Receiving Warfarin for Persistent Nonvalvular Atrial Fibrillation. Cardiovasc. Ultrasound 2012, 10, 50. [Google Scholar] [CrossRef] [PubMed]
- Su, B.; Sun, S.-K.; Dai, X.-J.; Ma, C.-S.; Zhou, B.-Y. The Novel Left Atrial Appendage Strain Parameters Are Associated with Thrombosis Risk in Patients with Non-Valvular Atrial Fibrillation. Echocardiogr. Mt. Kisco N 2023, 40, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Providência, R.; Faustino, A.; Ferreira, M.J.; Gonçalves, L.; Trigo, J.; Botelho, A.; Barra, S.; Boveda, S. Evaluation of Left Atrial Deformation to Predict Left Atrial Stasis in Patients with Non-Valvular Atrial Fibrillation—A Pilot-Study. Cardiovasc. Ultrasound 2013, 11, 44. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mao, Y.; Ma, M.; Yang, Y.; Yu, C.; Wang, Y.; Jiang, R.; Jiang, C. Left Atrial Appendage Mechanical Dispersion Provides Incremental Value for Thromboembolic Risk Stratification over CHA2DS2-VASc Score in Nonvalvular Atrial Fibrillation. Int. J. Cardiol. 2020, 307, 41–47. [Google Scholar] [CrossRef]
- Goldman, M.E.; Pearce, L.A.; Hart, R.G.; Zabalgoitia, M.; Asinger, R.W.; Safford, R.; Halperin, J.L. Pathophysiologic Correlates of Thromboembolism in Nonvalvular Atrial Fibrillation: I. Reduced Flow Velocity in the Left Atrial Appendage (The Stroke Prevention in Atrial Fibrillation [SPAF-III] Study). J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 1999, 12, 1080–1087. [Google Scholar] [CrossRef]
- Kamp, O.; Verhorst, P.M.; Welling, R.C.; Visser, C.A. Importance of Left Atrial Appendage Flow as a Predictor of Thromboembolic Events in Patients with Atrial Fibrillation. Eur. Heart J. 1999, 20, 979–985. [Google Scholar] [CrossRef]
- Handke, M.; Harloff, A.; Hetzel, A.; Olschewski, M.; Bode, C.; Geibel, A. Left Atrial Appendage Flow Velocity as a Quantitative Surrogate Parameter for Thromboembolic Risk: Determinants and Relationship to Spontaneous Echocontrast and Thrombus Formation. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2005, 18, 1366–1372. [Google Scholar] [CrossRef]
- Chen, L.; Xu, C.; Chen, W.; Zhang, C. Left Atrial Appendage Orifice Area and Morphology Is Closely Associated with Flow Velocity in Patients with Nonvalvular Atrial Fibrillation. BMC Cardiovasc. Disord. 2021, 21, 442. [Google Scholar] [CrossRef] [PubMed]
- Paciaroni, M.; Agnelli, G.; Caso, V.; Silvestrelli, G.; Seiffge, D.J.; Engelter, S.; De Marchis, G.M.; Polymeris, A.; Zedde, M.L.; Yaghi, S.; et al. Causes and Risk Factors of Cerebral Ischemic Events in Patients with Atrial Fibrillation Treated with Non-Vitamin K Antagonist Oral Anticoagulants for Stroke Prevention: The RENo Study. Stroke 2019, 50, 2168–2174. [Google Scholar] [CrossRef]
- Castellani, C.; Gao, Y.; Kim, H.; Thompson, C.; Ning, J.; Lohr, N.; Welsh, A.; Berger, M. Left Atrial Appendage Structural Characteristics Predict Thrombus Formation. J. Cardiovasc. Electrophysiol. 2023, 34, 1683–1689. [Google Scholar] [CrossRef]
- Lee, J.M.; Seo, J.; Uhm, J.-S.; Kim, Y.J.I.N.; Lee, H.-J.; Kim, J.-Y.; Sung, J.-H.; Pak, H.-N.; Lee, M.-H.; Joung, B. Why Is Left Atrial Appendage Morphology Related to Strokes? An Analysis of the Flow Velocity and Orifice Size of the Left Atrial Appendage. J. Cardiovasc. Electrophysiol. 2015, 26, 922–927. [Google Scholar] [CrossRef] [PubMed]
- Nakagami, H.; Yamamoto, K.; Ikeda, U.; Mitsuhashi, T.; Goto, T.; Shimada, K. Mitral Regurgitation Reduces the Risk of Stroke in Patients with Nonrheumatic Atrial Fibrillation. Am. Heart J. 1998, 136, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Blackshear, J.L.; Pearce, L.A.; Asinger, R.W.; Dittrich, H.C.; Goldman, M.E.; Zabalgoitia, M.; Rothbart, R.M.; Halperin, J.L. Mitral Regurgitation Associated with Reduced Thromboembolic Events in High-Risk Patients with Nonrheumatic Atrial Fibrillation. Stroke Prevention in Atrial Fibrillation Investigators. Am. J. Cardiol. 1993, 72, 840–843. [Google Scholar] [CrossRef]
- Bisson, A.; Bernard, A.; Bodin, A.; Clementy, N.; Babuty, D.; Lip, G.Y.H.; Fauchier, L. Stroke and Thromboembolism in Patients with Atrial Fibrillation and Mitral Regurgitation. Circ. Arrhythm. Electrophysiol. 2019, 12, e006990. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Marin, F.; Camm, A.J.; Lip, G.Y.H. Stroke and Thromboembolism in Atrial Fibrillation. Circ. J. Off. J. Jpn. Circ. Soc. 2012, 76, 2289–2304. [Google Scholar] [CrossRef]
- Uziębło-Życzkowska, B.; Krzesiński, P.; Jurek, A.; Kapłon-Cieślicka, A.; Gorczyca, I.; Budnik, M.; Gielerak, G.; Kiliszek, M.; Gawałko, M.; Scisło, P.; et al. Left Ventricular Ejection Fraction Is Associated with the Risk of Thrombus in the Left Atrial Appendage in Patients with Atrial Fibrillation. Cardiovasc. Ther. 2020, 2020, 3501749. [Google Scholar] [CrossRef]
- Atrial Fibrillation Investigators: Atrial Fibrillation Anticoagulation Study; European Atrial Fibrillation Study; Stroke Prevention in Atrial Fibrillation Study; Boston Area Anticoagulation Trial for Atrial Fibrillation Study; Canadian Atrial Fibrillation Study; Veterans Affairs Prevention in Atrial Fibrillation Study. Echocardiographic Predictors of Stroke in Patients With Atrial Fibrillation: A Prospective Study of 1066 Patients from 3 Clinical Trials. Arch. Intern. Med. 1998, 158, 1316–1320. [Google Scholar] [CrossRef]
- Demirkiran, A.; Hassell, M.E.C.J.; Garg, P.; Elbaz, M.S.M.; Delewi, R.; Greenwood, J.P.; Piek, J.J.; Plein, S.; van der Geest, R.J.; Nijveldt, R. Left Ventricular Four-Dimensional Blood Flow Distribution, Energetics, and Vorticity in Chronic Myocardial Infarction Patients with/without Left Ventricular Thrombus. Eur. J. Radiol. 2022, 150, 110233. [Google Scholar] [CrossRef]
- Markl, M.; Lee, D.C.; Furiasse, N.; Carr, M.; Foucar, C.; Ng, J.; Carr, J.; Goldberger, J.J. Left Atrial and Left Atrial Appendage 4D Blood Flow Dynamics in Atrial Fibrillation. Circ. Cardiovasc. Imaging 2016, 9, e004984. [Google Scholar] [CrossRef] [PubMed]
- Cha, M.J.; An, D.-G.; Kang, M.; Kim, H.M.; Kim, S.-W.; Cho, I.; Hong, J.; Choi, H.; Cho, J.-H.; Shin, S.Y.; et al. Correct Closure of the Left Atrial Appendage Reduces Stagnant Blood Flow and the Risk of Thrombus Formation: A Proof-of-Concept Experimental Study Using 4D Flow Magnetic Resonance Imaging. Korean J. Radiol. 2023, 24, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Bäck, S.; Henriksson, L.; Bolger, A.F.; Carlhäll, C.-J.; Persson, A.; Karlsson, M.; Ebbers, T. Assessment of Transmitral and Left Atrial Appendage Flow Rate from Cardiac 4D-CT. Commun. Med. 2023, 3, 22. [Google Scholar] [CrossRef] [PubMed]
- Rigatelli, G.; Zuin, M.; Roncon, L. Increased Blood Residence Time as Markers of High-Risk Patent Foramen Ovale. Transl. Stroke Res. 2023, 14, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Fang, R.; Li, Y.; Zhang, Y.; Chen, Q.; Liu, Q.; Li, Z. Impact of Left Atrial Appendage Location on Risk of Thrombus Formation in Patients with Atrial Fibrillation. Biomech. Model. Mechanobiol. 2021, 20, 1431–1443. [Google Scholar] [CrossRef] [PubMed]
- Durán, E.; García-Villalba, M.; Martínez-Legazpi, P.; Gonzalo, A.; McVeigh, E.; Kahn, A.M.; Bermejo, J.; Flores, O.; Del Álamo, J.C. Pulmonary Vein Flow Split Effects in Patient-Specific Simulations of Left Atrial Flow. Comput. Biol. Med. 2023, 163, 107128. [Google Scholar] [CrossRef] [PubMed]
- Pons, M.I.; Mill, J.; Fernandez-Quilez, A.; Olivares, A.L.; Silva, E.; De Potter, T.; Camara, O. Joint Analysis of Morphological Parameters and In Silico Haemodynamics of the Left Atrial Appendage for Thrombogenic Risk Assessment. J. Interv. Cardiol. 2022, 2022, 9125224. [Google Scholar] [CrossRef]
- Bartus, K.; Litwinowicz, R.; Natorska, J.; Zabczyk, M.; Undas, A.; Kapelak, B.; Lakkireddy, D.; Lee, R.J. Coagulation Factors and Fibrinolytic Activity in the Left Atrial Appendage and Other Heart Chambers in Patients with Atrial Fibrillation: Is There a Local Intracardiac Prothrombotic State? (HEART-CLOT Study). Int. J. Cardiol. 2020, 301, 103–107. [Google Scholar] [CrossRef]
- Xu, B.; Du, Y.; Xu, C.; Sun, Y.; Peng, F.; Wang, S.; Pan, J.; Lou, Y.; Xing, Y. Left Atrial Appendage Morphology and Local Thrombogenesis-Related Blood Parameters in Patients with Atrial Fibrillation. J. Am. Heart Assoc. 2021, 10, e020406. [Google Scholar] [CrossRef]
- Tóth, N.K.; Csanádi, Z.; Hajas, O.; Kiss, A.; Nagy-Baló, E.; Kovács, K.B.; Sarkady, F.; Muszbek, L.; Bereczky, Z.; Csiba, L.; et al. Intracardiac Hemostasis and Fibrinolysis Parameters in Patients with Atrial Fibrillation. BioMed Res. Int. 2017, 2017, 3678017. [Google Scholar] [CrossRef] [PubMed]
- Litwinowicz, R.; Natorska, J.; Zabczyk, M.; Kapelak, B.; Lakkireddy, D.; Vuddanda, V.; Bartus, K. Changes in Fibrinolytic Activity and Coagulation Factors after Epicardial Left Atrial Appendage Closure in Patients with Atrial Fibrillation. J. Thorac. Dis. 2020, 14, 4226. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Li, Z.; Goette, A.; Mera, F.; Honeycutt, C.; Feterik, K.; Wilcox, J.N.; Dudley, S.C.J.; Harrison, D.G.; Langberg, J.J. Downregulation of Endocardial Nitric Oxide Synthase Expression and Nitric Oxide Production in Atrial Fibrillation: Potential Mechanisms for Atrial Thrombosis and Stroke. Circulation 2002, 106, 2854–2858. [Google Scholar] [CrossRef]
- Camen, S.; Ojeda, F.M.; Niiranen, T.; Gianfagna, F.; Vishram-Nielsen, J.K.; Costanzo, S.; Söderberg, S.; Vartiainen, E.; Donati, M.B.; Løchen, M.-L.; et al. Temporal Relations between Atrial Fibrillation and Ischaemic Stroke and Their Prognostic Impact on Mortality. EP Eur. 2020, 22, 522–529. [Google Scholar] [CrossRef]
- Daoud, E.G.; Glotzer, T.V.; Wyse, D.G.; Ezekowitz, M.D.; Hilker, C.; Koehler, J.; Ziegler, P.D. Temporal Relationship of Atrial Tachyarrhythmias, Cerebrovascular Events, and Systemic Emboli Based on Stored Device Data: A Subgroup Analysis of TRENDS. Heart Rhythm 2011, 8, 1416–1423. [Google Scholar] [CrossRef] [PubMed]
- Singer, D.E.; Ziegler, P.D.; Koehler, J.L.; Sarkar, S.; Passman, R.S. Temporal Association Between Episodes of Atrial Fibrillation and Risk of Ischemic Stroke. JAMA Cardiol. 2021, 6, 1364. [Google Scholar] [CrossRef] [PubMed]
- Turakhia, M.P.; Ziegler, P.D.; Schmitt, S.K.; Chang, Y.; Fan, J.; Than, C.T.; Keung, E.K.; Singer, D.E. Atrial Fibrillation Burden and Short-Term Risk of Stroke: Case-Crossover Analysis of Continuously Recorded Heart Rhythm From Cardiac Electronic Implanted Devices. Circ. Arrhythm. Electrophysiol. 2015, 8, 1040–1047. [Google Scholar] [CrossRef]
- Kirchhof, P.; Toennis, T.; Goette, A.; Camm, A.J.; Diener, H.C.; Becher, N.; Bertaglia, E.; Blomstrom Lundqvist, C.; Borlich, M.; Brandes, A.; et al. Anticoagulation with Edoxaban in Patients with Atrial High-Rate Episodes. N. Engl. J. Med. 2023, 389, 1167–1179. [Google Scholar] [CrossRef]
- Ambrosio, G.; Camm, A.J.; Bassand, J.-P.; Corbalan, R.; Kayani, G.; Carluccio, E.; Mantovani, L.G.; Virdone, S.; Kakkar, A.K.; GARFIELD-AF Investigators. Characteristics, treatment, and outcomes of newly diagnosed atrial fibrillation patients with heart failure: GARFIELD-AF. ESC Heart Fail. 2021, 8, 1139–1149. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Nieuwlaat, R.; Pisters, R.; Lane, D.A.; Crijns, H.J.G.M.; Andresen, D.; Camm, A.J.; Davies, W.; Capucci, A.; Olsson, B.; et al. Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in Atrial Fibrillation Using a Novel Risk Factor-Based Approach: The Euro Heart Survey on Atrial Fibrillation. Chest 2010, 137, 263–272. [Google Scholar] [CrossRef]
- Szymanski, F.M.; Lip, G.Y.H.; Filipiak, K.J.; Platek, A.E.; Hrynkiewicz-Szymanska, A.; Opolski, G. Stroke Risk Factors Beyond the CHA2DS2-VASc Score: Can We Improve Our Identification of “High Stroke Risk” Patients with Atrial Fibrillation? Am. J. Cardiol. 2015, 116, 1781–1788. [Google Scholar] [CrossRef] [PubMed]
- Friberg, L.; Benson, L.; Lip, G.Y.H. Balancing Stroke and Bleeding Risks in Patients with Atrial Fibrillation and Renal Failure: The Swedish Atrial Fibrillation Cohort Study. Eur. Heart J. 2015, 36, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Bonde, A.N.; Lip, G.Y.H.; Kamper, A.-L.; Hansen, P.R.; Lamberts, M.; Hommel, K.; Hansen, M.L.; Gislason, G.H.; Torp-Pedersen, C.; Olesen, J.B. Net Clinical Benefit of Antithrombotic Therapy in Patients with Atrial Fibrillation and Chronic Kidney Disease. J. Am. Coll. Cardiol. 2014, 64, 2471–2482. [Google Scholar] [CrossRef] [PubMed]
- Segan, L.; Nanayakkara, S.; Spear, E.; Shirwaiker, A.; Chieng, D.; Prabhu, S.; Sugumar, H.; Ling, L.; Kaye, D.M.; Kalman, J.M.; et al. Identifying Patients at High Risk of Left Atrial Appendage Thrombus Before Cardioversion: The CLOTS-AF Score. J. Am. Heart Assoc. 2023, 12, e029259. [Google Scholar] [CrossRef] [PubMed]
- Piccini, J.P.; Stevens, S.R.; Chang, Y.; Singer, D.E.; Lokhnygina, Y.; Go, A.S.; Patel, M.R.; Mahaffey, K.W.; Halperin, J.L.; Breithardt, G.; et al. Renal Dysfunction as a Predictor of Stroke and Systemic Embolism in Patients With Nonvalvular Atrial Fibrillation: Validation of the R 2 CHADS 2 Index in the ROCKET AF (Rivaroxaban Once-Daily, Oral, Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation) and ATRIA (AnTicoagulation and Risk Factors In Atrial Fibrillation) Study Cohorts. Circulation 2013, 127, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Chao, T.-F.; Lin, Y.-J.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Tuan, T.-C.; Liao, J.-N.; Chung, F.-P.; Hsieh, M.-H.; Chen, S.-A. R2CHADS2 Score and Thromboembolic Events After Catheter Ablation of Atrial Fibrillation in Comparison with the CHA2DS2-VASc Score. Can. J. Cardiol. 2014, 30, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Singer, D.E.; Chang, Y.; Borowsky, L.H.; Fang, M.C.; Pomernacki, N.K.; Udaltsova, N.; Reynolds, K.; Go, A.S. A New Risk Scheme to Predict Ischemic Stroke and Other Thromboembolism in Atrial Fibrillation: The ATRIA Study Stroke Risk Score. J. Am. Heart Assoc. 2013, 2, e000250. [Google Scholar] [CrossRef]
- Fox, K.A.A.; Lucas, J.E.; Pieper, K.S.; Bassand, J.-P.; Camm, A.J.; Fitzmaurice, D.A.; Goldhaber, S.Z.; Goto, S.; Haas, S.; Hacke, W.; et al. Improved Risk Stratification of Patients with Atrial Fibrillation: An Integrated GARFIELD-AF Tool for the Prediction of Mortality, Stroke and Bleed in Patients with and without Anticoagulation. BMJ Open 2017, 7, e017157. [Google Scholar] [CrossRef]
- Bassand, J.-P.; Accetta, G.; Al Mahmeed, W.; Corbalan, R.; Eikelboom, J.; Fitzmaurice, D.A.; Fox, K.A.A.; Gao, H.; Goldhaber, S.Z.; Goto, S.; et al. Risk Factors for Death, Stroke, and Bleeding in 28,628 Patients from the GARFIELD-AF Registry: Rationale for Comprehensive Management of Atrial Fibrillation. PLoS ONE 2018, 13, e0191592. [Google Scholar] [CrossRef]
- Zhu, W.; Fu, L.; Ding, Y.; Huang, L.; Xu, Z.; Hu, J.; Hong, K. Meta-Analysis of ATRIA versus CHA2DS2-VASc for Predicting Stroke and Thromboembolism in Patients with Atrial Fibrillation. Int. J. Cardiol. 2017, 227, 436–442. [Google Scholar] [CrossRef]
- Essien, U.R.; Chiswell, K.; Kaltenbach, L.A.; Wang, T.Y.; Fonarow, G.C.; Thomas, K.L.; Turakhia, M.P.; Benjamin, E.J.; Rodriguez, F.; Fang, M.C.; et al. Association of Race and Ethnicity with Oral Anticoagulation and Associated Outcomes in Patients With Atrial Fibrillation: Findings From the Get With The Guidelines–Atrial Fibrillation Registry. JAMA Cardiol. 2022, 7, 1207. [Google Scholar] [CrossRef] [PubMed]
- Calvert, P.; Tamirisa, K.; Al-Ahmad, A.; Lip, G.Y.H.; Gupta, D. Racial and Ethnic Disparities in Stroke Prevention for Atrial Fibrillation. Am. J. Med. 2023, 136, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Kabra, R.; Girotra, S.; Vaughan Sarrazin, M. Refining Stroke Prediction in Atrial Fibrillation Patients by Addition of African-American Ethnicity to CHA 2 DS 2 -VASc Score. J. Am. Coll. Cardiol. 2016, 68, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Overvad, T.F.; Rasmussen, L.H.; Skjøth, F.; Overvad, K.; Lip, G.Y.H.; Larsen, T.B. Body Mass Index and Adverse Events in Patients with Incident Atrial Fibrillation. Am. J. Med. 2013, 126, 640.e9–640.e17. [Google Scholar] [CrossRef] [PubMed]
- Yaranov, D.M.; Smyrlis, A.; Usatii, N.; Butler, A.; Petrini, J.R.; Mendez, J.; Warshofsky, M.K. Effect of Obstructive Sleep Apnea on Frequency of Stroke in Patients with Atrial Fibrillation. Am. J. Cardiol. 2015, 115, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Szymanski, F.M.; Filipiak, K.J.; Platek, A.E.; Hrynkiewicz-Szymanska, A.; Karpinski, G.; Opolski, G. Assessment of CHADS2 and CHA2DS2-VASc Scores in Obstructive Sleep Apnea Patients with Atrial Fibrillation. Sleep Breath. 2015, 19, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Verdecchia, P.; Porcellati, C.; Reboldi, G.; Gattobigio, R.; Borgioni, C.; Pearson, T.A.; Ambrosio, G. Left Ventricular Hypertrophy as an Independent Predictor of Acute Cerebrovascular Events in Essential Hypertension. Circulation 2001, 104, 2039–2044. [Google Scholar] [CrossRef] [PubMed]
- Yaghi, S.; Kamel, H. Stratifying Stroke Risk in Atrial Fibrillation: Beyond Clinical Risk Scores. Stroke 2017, 48, 2665–2670. [Google Scholar] [CrossRef]
- Cai, Y.; Xiong, Q.; Chen, S.; Jiang, X.; Liao, J.; Chen, W.; Zou, L.; Su, L.; Zhu, Y.; Yin, Y.; et al. Left Atrial Appendage Thrombus in Patients with Nonvalvular Atrial Fibrillation before Catheter Ablation and Cardioversion: Risk Factors beyond the CHA2DS2-VASc Score. J. Cardiovasc. Dev. Dis. 2022, 9, 46. [Google Scholar] [CrossRef]
- Malik, V.; Ganesan, A.N.; Selvanayagam, J.B.; Chew, D.P.; McGavigan, A.D. Is Atrial Fibrillation a Stroke Risk Factor or Risk Marker? An Appraisal Using the Bradford Hill Framework for Causality. Heart Lung Circ. 2020, 29, 86–93. [Google Scholar] [CrossRef]
- Friberg, L.; Rosenqvist, M.; Lip, G.Y.H. Evaluation of Risk Stratification Schemes for Ischaemic Stroke and Bleeding in 182 678 Patients with Atrial Fibrillation: The Swedish Atrial Fibrillation Cohort Study. Eur. Heart J. 2012, 33, 1500–1510. [Google Scholar] [CrossRef]
- Chao, T.-F.; Liao, J.-N.; Tuan, T.-C.; Lin, Y.-J.; Chang, S.-L.; Lo, L.-W.; Hu, Y.-F.; Chung, F.-P.; Chen, T.-J.; Lip, G.Y.H.; et al. Incident Co-Morbidities in Patients with Atrial Fibrillation Initially with a CHA2DS2-VASc Score of 0 (Males) or 1 (Females): Implications for Reassessment of Stroke Risk in Initially ‘Low-Risk’ Patients. Thromb. Haemost. 2019, 119, 1162–1170. [Google Scholar] [CrossRef]


{kind=link}
| Study | n | Study Design | Main Results |
|---|---|---|---|
| Daoud et al., 2021 [95] | 40 |
|
|
| Brambatti et al., 2014 [35] | 51 |
|
|
| Turakhia et al., 2015 [97] | 187 |
|
|
| Singer et al., 2021 [96] | 891 |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aarnink, E.; Zabern, M.; Boersma, L.; Glikson, M. Mechanisms and Prediction of Ischemic Stroke in Atrial Fibrillation Patients. J. Clin. Med. 2023, 12, 6491. https://doi.org/10.3390/jcm12206491
Aarnink E, Zabern M, Boersma L, Glikson M. Mechanisms and Prediction of Ischemic Stroke in Atrial Fibrillation Patients. Journal of Clinical Medicine. 2023; 12(20):6491. https://doi.org/10.3390/jcm12206491
Chicago/Turabian StyleAarnink, Errol, Maxime Zabern, Lucas Boersma, and Michael Glikson. 2023. "Mechanisms and Prediction of Ischemic Stroke in Atrial Fibrillation Patients" Journal of Clinical Medicine 12, no. 20: 6491. https://doi.org/10.3390/jcm12206491
APA StyleAarnink, E., Zabern, M., Boersma, L., & Glikson, M. (2023). Mechanisms and Prediction of Ischemic Stroke in Atrial Fibrillation Patients. Journal of Clinical Medicine, 12(20), 6491. https://doi.org/10.3390/jcm12206491