Incidence and Risk Factors for Surgical Site Infection in Ankle Fractures: An Observational Study of 480 Patients in Sweden

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definitions
2.2. Statistical Analysis
3. Results
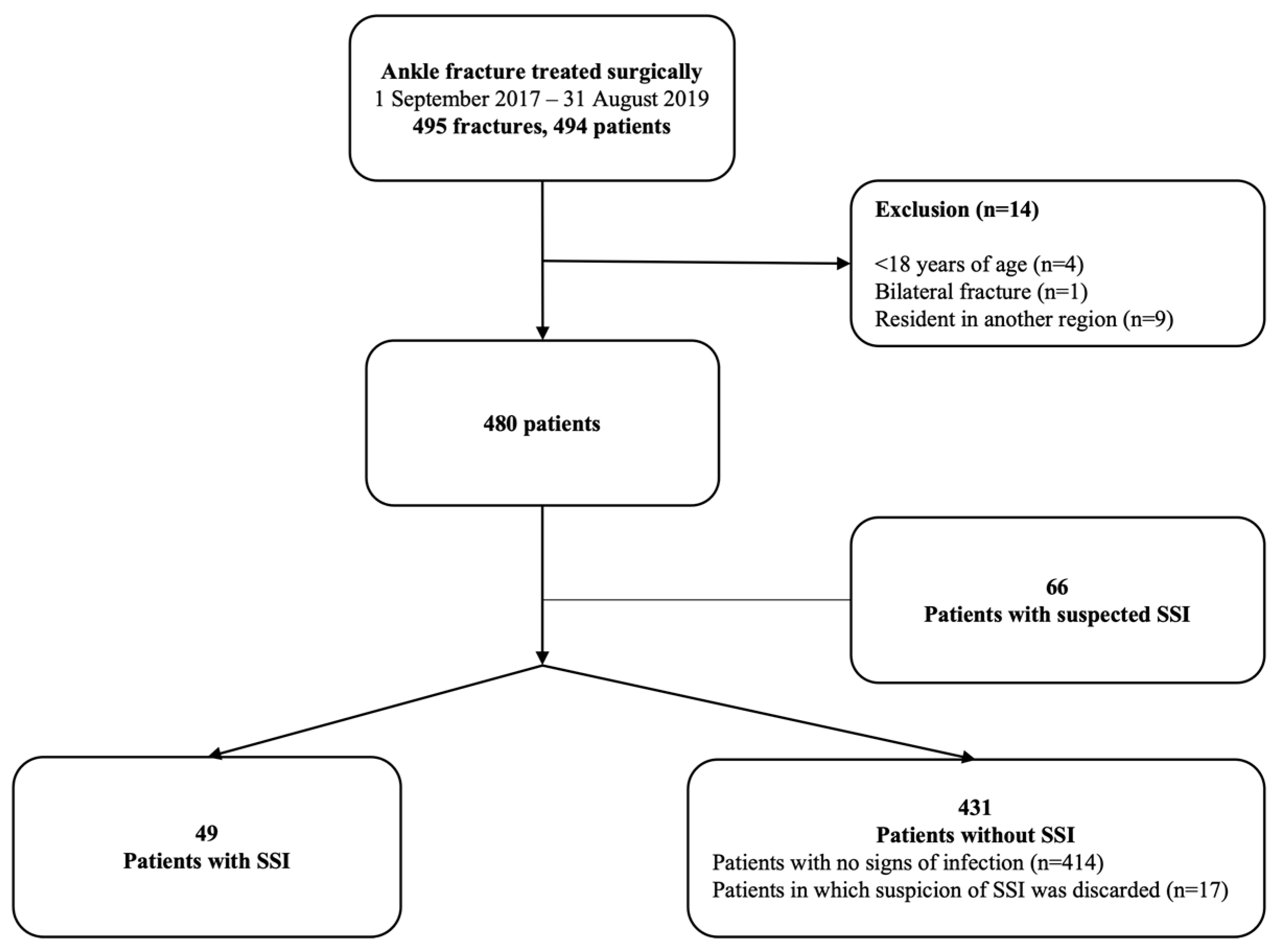
3.1. Study Cohort
3.2. Patients with a SSI
3.3. Microbiological Findings in the Infected Patients
3.4. Risk factors for SSI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bergh, C.; Wennergren, D.; Möller, M.; Brisby, H. Fracture incidence in adults in relation to age and gender: A study of 27,169 fractures in the Swedish Fracture Register in a well-defined catchment area. PLoS ONE 2020, 15, e0244291. [Google Scholar] [CrossRef] [PubMed]
- Rydberg, E.M.; Zorko, T.; Sundfeldt, M.; Möller, M.; Wennergren, D. Classification and treatment of lateral malleolar fractures—A single-center analysis of 439 ankle fractures using the Swedish Fracture Register. BMC Musculoskelet. Disord. 2020, 21, 521. [Google Scholar] [CrossRef] [PubMed]
- SooHoo, N.F.; Krenek, L.; Eagan, M.J.; Gurbani, B.; Ko, C.Y.; Zingmond, D.S. Complication rates following open reduction and internal fixation of ankle fractures. J. Bone Joint Surg. Am. 2009, 91, 1042–1049. [Google Scholar] [CrossRef]
- Olsen, L.L.; Møller, A.M.; Brorson, S.; Hasselager, R.B.; Sort, R. The impact of lifestyle risk factors on the rate of infection after surgery for a fracture of the ankle. Bone Joint J. 2017, 99, 225–230. [Google Scholar] [CrossRef]
- Kelly, E.G.; Cashman, J.P.; Groarke, P.J.; Morris, S.F. Risk factors for surgical site infection following operative ankle fracture fixation. Ir. J. Med. Sci. 2013, 182, 453–456. [Google Scholar] [CrossRef]
- Korim, M.T.; Payne, R.; Bhatia, M. A case-control study of surgical site infection following operative fixation of fractures of the ankle in a large, U.K. trauma unit. Bone Joint J. 2014, 96-b, 636–640. [Google Scholar] [CrossRef]
- Lachman, J.R.; Elkrief, J.I.; Pipitone, P.S.; Haydel, C.L. Comparison of Surgical Site Infections in Ankle Fracture Surgery With or Without the Use of Postoperative Antibiotics. Foot Ankle Int. 2018, 39, 1278–1282. [Google Scholar] [CrossRef]
- Liu, D.; Zhu, Y.; Chen, W.; Li, M.; Liu, S.; Zhang, Y. Multiple preoperative biomarkers are associated with incidence of surgical site infection following surgeries of ankle fractures. Int. Wound J. 2020, 17, 842–850. [Google Scholar] [CrossRef]
- Meng, J.; Sun, T.; Zhang, F.; Qin, S.; Li, Y.; Zhao, H. Deep surgical site infection after ankle fractures treated by open reduction and internal fixation in adults: A retrospective case-control study. Int. Wound J. 2018, 15, 971–977. [Google Scholar] [CrossRef]
- Ovaska, M.T.; Mäkinen, T.J.; Madanat, R.; Huotari, K.; Vahlberg, T.; Hirvensalo, E.; Lindahl, J. Risk factors for deep surgical site infection following operative treatment of ankle fractures. J. Bone Joint Surg. Am. 2013, 95, 348–353. [Google Scholar]
- Rascoe, A.S.; Kavanagh, M.D.; Audet, M.A.; Hu, E.; Vallier, H.A. Factors associating with surgical site infection following operative management of malleolar fractures at an urban level 1 trauma center. OTA Int. 2020, 3, e077. [Google Scholar] [CrossRef] [PubMed]
- Richardson, N.G.; Swiggett, S.J.; Pasternack, J.B.; Vakharia, R.M.; Kang, K.K.; Abdelgawad, A. Comparison study of patient demographics and risk factors for surgical site infections following open reduction and internal fixation for lateral malleolar ankle fractures within the medicare population. Foot Ankle Surg. 2021, 27, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Saithna, A.; Moody, W.; Jenkinson, E.; Almazedi, B.; Sargeant, I. The influence of timing of surgery on soft tissue complications in closed ankle fractures. Eur. J. Orthop. Surg. Traumatol. 2009, 19, 481–484. [Google Scholar] [CrossRef]
- Sato, T.; Takegami, Y.; Sugino, T.; Bando, K.; Fujita, T.; Imagama, S. Smoking and trimalleolar fractures are risk factors for infection after open reduction and internal fixation of closed ankle fractures: A multicenter retrospective study of 1201 fractures. Injury 2021, 52, 1959–1963. [Google Scholar] [CrossRef]
- Sun, R.; Li, M.; Wang, X.; Li, X.; Wu, L.; Chen, Z.; Chen, K. Surgical site infection following open reduction and internal fixation of a closed ankle fractures: A retrospective multicenter cohort study. Int. J. Surg. 2017, 48, 86–91. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, H.; Tang, Y.; Zhao, H.; Qin, S.; Xu, L.; Xia, Z.; Zhang, F. Incidence and risk factors for surgical site infection after open reduction and internal fixation of ankle fracture: A retrospective multicenter study. Medicine 2018, 97, e9901. [Google Scholar] [CrossRef]
- Thangarajah, T.; Prasad, P.S.; Narayan, B. Surgical site infections following open reduction and internal fixation of ankle fractures. Open Orthop. J. 2009, 3, 56–60. [Google Scholar] [CrossRef]
- Zalavras, C.G.; Christensen, T.; Rigopoulos, N.; Holtom, P.; Patzakis, M.J. Infection following operative treatment of ankle fractures. Clin. Orthop. Relat. Res. 2009, 467, 1715–1720. [Google Scholar] [CrossRef]
- World Health Organization. Antimicrobial Resistance: Global Report on Surveillance; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Broex, E.C.; van Asselt, A.D.; Bruggeman, C.A.; van Tiel, F.H. Surgical site infections: How high are the costs? J. Hosp. Infect. 2009, 72, 193–201. [Google Scholar] [CrossRef]
- Andersson, A.E.; Bergh, I.; Karlsson, J.; Nilsson, K. Patients’ experiences of acquiring a deep surgical site infection: An interview study. Am. J. Infect. Control. 2010, 38, 711–717. [Google Scholar] [CrossRef]
- Cahill, J.L.; Shadbolt, B.; Scarvell, J.M.; Smith, P.N. Quality of life after infection in total joint replacement. J. Orthop. Surg. 2008, 16, 58–65. [Google Scholar] [CrossRef]
- Schade, M.A.; Hollenbeak, C.S. Early Postoperative Infection Following Open Reduction Internal Fixation Repair of Closed Malleolar Fractures. Foot Ankle Spec. 2018, 11, 335–341. [Google Scholar] [CrossRef]
- Gowd, A.K.; Bohl, D.D.; Hamid, K.S.; Lee, S.; Holmes, G.B.; Lin, J. Longer Operative Time Is Independently Associated With Surgical Site Infection and Wound Dehiscence Following Open Reduction and Internal Fixation of the Ankle. Foot Ankle Spec. 2020, 13, 104–111. [Google Scholar] [CrossRef]
- Carragee, E.J.; Csongradi, J.J.; Bleck, E.E. Early complications in the operative treatment of ankle fractures : Influence of delay before operation. J. Bone Jt. Surg. Br. Vol. 1991, 73, 79–82. [Google Scholar] [CrossRef]
- Schepers, T.; De Vries, M.R.; Van Lieshout, E.M.; Van der Elst, M. The timing of ankle fracture surgery and the effect on infectious complications; a case series and systematic review of the literature. Int. Orthop. 2013, 37, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Wennergren, D.; Ekholm, C.; Sandelin, A.; Möller, M. The Swedish fracture register: 103,000 fractures registered. BMC Musculoskelet. Disord. 2015, 16, 338. [Google Scholar] [CrossRef] [PubMed]
- Möller, M.; Wolf, O.; Bergdahl, C.; Mukka, S.; Rydberg, E.M.; Hailer, N.P.; Ekelund, J.; Wennergren, D. The Swedish Fracture Register—Ten years of experience and 600,000 fractures collected in a National Quality Register. BMC Musculoskelet. Disord. 2022, 23, 141. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.J.; Morgenstern, M.; McNally, M.A.; Moriarty, T.F.; McFadyen, I.; Scarborough, M.; Athanasou, N.A.; Ochsner, P.E.; Kuehl, R.; Raschke, M.; et al. Fracture-related infection: A consensus on definition from an international expert group. Injury 2018, 49, 505–510. [Google Scholar] [CrossRef] [PubMed]
- ECDC. European Centre for Disease Prevention and Control (ECDC)/European Medicines Agency (EMEA) Joint Technical report: The Bacterial Challenge: Time to React; ECDC: Solna, Stockholm, 2009. [Google Scholar]
- Shao, J.; Zhang, H.; Yin, B.; Li, J.; Zhu, Y.; Zhang, Y. Risk factors for surgical site infection following operative treatment of ankle fractures: A systematic review and meta-analysis. Int. J. Surg. 2018, 56, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Neumann, A.P.; Kroker, L.; Beyer, F.; Rammelt, S. Complications following surgical treatment of posterior malleolar fractures: An analysis of 300 cases. Arch. Orthop. Trauma. Surg. 2023, 143, 3129–3136. [Google Scholar] [CrossRef]
- Mangram, A.J.; Horan, T.C.; Pearson, M.L.; Silver, L.C.; Jarvis, W.R. Guideline for Prevention of Surgical Site Infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am. J. Infect. Control. 1999, 27, 97–132, quiz 3–4, discussion 96. [Google Scholar] [CrossRef] [PubMed]
- Concato, J.; Peduzzi, P.; Holford, T.R.; Feinstein, A.R. Importance of events per independent variable in proportional hazards analysis. I. Background, goals, and general strategy. J. Clin. Epidemiol. 1995, 48, 1495–1501. [Google Scholar] [CrossRef] [PubMed]
- Vittinghoff, E.; McCulloch, C.E. Relaxing the rule of ten events per variable in logistic and Cox regression. Am. J. Epidemiol. 2007, 165, 710–718. [Google Scholar] [CrossRef] [PubMed]
- SFS 2008:355 Patient Data Act (Swe). Sect. Chapter 7. Available online: https://www.riksdagen.se/sv/dokument-och-lagar/dokument/svensk-forfattningssamling/patientdatalag-2008355_sfs-2008-355/ (accessed on 8 October 2023).

{kind=link}
| Surgical Site Infection: | |
|---|---|
| Superficial | If ≥1 of the following was present within a year of index surgery:
|
| Deep | If a reoperation, due to clinical signs of infection, occurred within a year of index surgery and ≥1 of the following was present:
|
| Characteristics | Median (IQR, Range) |
|---|---|
| Age | 55 (29, 18–93) |
| Female sex, n (%) | 286 (59.6) |
| BMI | 27.0 (6.5, 17.7–63.2) |
| Time until surgery (h) | 72.5 (131, 3–1085) |
| Duration of surgery (min) | 88 (48, 9–300) |
| Length of stay (days) | 3 (5, 0–33) |
| Type of Fracture | Infection Incidence—n (%) |
|---|---|
| All | 49 (10.2) |
| Superficial | 35 (7.3) |
| Deep | 14 (2.9) |
| Closed | 39 (8.7) |
| Superficial | 28 (6.2) |
| Deep | 11 (2.4) |
| Open | 10 (32.3) |
| Superficial | 7 (22.6) |
| Deep | 3 (9.7) |
| Characteristics | Infected—n (%) 49 (100) | Non-Infected—n (%) 431 (100) | p-Value |
|---|---|---|---|
| Age +, median (IQR, range) | 61 (25, 21–93) | 55 (29, 18–91) | 0.016 |
| Female sex | 30 (61) | 256 (59) | 0.805 |
| Diabetes * | 6 (12) | 36 (8) | 0.419 |
| Smoking | 12 (24) | 68 (16) | 0.154 |
| ASA 1–2 | 41 (84) | 386 (90) | 0.213 |
| ASA 3–4 | 8 (16) | 45 (10) | |
| BMI *: | 0.374 | ||
| <18.5 | 1 (2) | 1 (0) | |
| 18.5–24.9 | 15 (31) | 127 (29) | |
| 25–30 | 18 (38) | 162 (38) | |
| >30 | 14 (29) | 123 (29) | |
| Open fracture * | 10 (20) | 21 (5) | <0.001 |
| Time until surgery <24 h | 8 (16) | 79 (18) | 0.632 |
| 24-72 h | 12 (24) | 131 (30) | |
| >72 h | 27 (55) | 212 (49) | |
| Duration of surgery >90 min | 25 (51) | 193 (45) | 0.601 |
| LAF | 24 (49) | 247 (57) | 0.228 |
| Temporary external fixation * | 7 (14) | 35 (8) | 0.176 |
| Head surgeon: | 0.249 | ||
| Resident | 15 (31) | 165 (38) | |
| Specialist | 12 (25) | 124 (29) | |
| Consultant | 22 (45) | 141 (33) | |
| Length of stay (days) +, median (IQR, range) | 4 (8, 0–20) | 3 (5, 0–33) | 0.037 |
| No. of follow-ups +, median (IQR, range) | 5 (7, 1–26) | 3 (2, 0–24) | <0.001 |
|
Frequency—n (%) 49 (100) | |
|---|---|
| Positive microbiological count | 26 (53) |
| Monomicrobial infections | 18 (37) |
| S. aureus | 12 (24) |
| MRSA | 1 (2) |
| CoNS | 1 (2) |
| Corynebacterium striatum | 1 (2) |
| Acinetobacter | 1 (2) |
| Group G β-hemolytic streptococci | 1 (2) |
| Escherichia coli | 1 (2) |
| Polymicrobial infections | 8 (16) |
| S. aureus + Enterobacter cloacae | 1 (2) |
| CoNS + MRSA | 1 (2) |
| CoNS + Clostridium | 1 (2) |
| CoNS + Pseudomonas | 1 (2) |
| CoNS + Enterobacter cloacae | 2 (4) |
| Corynebacterium striatum + Proteus vulgaris/penneri | 1 (2) |
| Corynebacterium striatum + Peptoniphilus | 1 (2) |
| Mixed Gram-positive bacteria | 4 (8) |
| Negative count | 3 (6) |
| No samples available | 16 (33) |
| Variables | Hazard Ratio | 95% C.I. | p-Value |
|---|---|---|---|
| Age * | 1.016 | 1.00–1.36 | 0.122 |
| Male sex | 1.072 | 0.56–2.05 | 0.834 |
| Diabetes | 1.407 | 0.53–3.71 | 0.490 |
| Smoking | 1.232 | 0.58–2.64 | 0.591 |
| ASA 3–4 | 0.866 | 0.33–2.56 | 0.768 |
| BMI * | 0.991 | 0.93–1.06 | 0.789 |
| Open | 2.960 | 1.26–6.96 | 0.013 |
| Time from ER to surgery * | 1.001 | 1.00–1.00 | 0.227 |
| Duration of surgery * | 1.000 | 1.00–1.00 | 0.990 |
| OR without LAF | 1.221 | 0.65–2.28 | 0.532 |
| External fixation | 1.045 | 0.39–2.80 | 0.930 |
| Head surgeon: Resident | 0.993 | 0.45–2.18 | 0.986 |
| Specialist | Ref. | 0.797 | |
| Consultant | 1.245 | 0.58–2.69 | 0.576 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bergström, J.; Möller Rydberg, E.; Wennergren, D.; Svensson Malchau, K. Incidence and Risk Factors for Surgical Site Infection in Ankle Fractures: An Observational Study of 480 Patients in Sweden. J. Clin. Med. 2023, 12, 6464. https://doi.org/10.3390/jcm12206464
Bergström J, Möller Rydberg E, Wennergren D, Svensson Malchau K. Incidence and Risk Factors for Surgical Site Infection in Ankle Fractures: An Observational Study of 480 Patients in Sweden. Journal of Clinical Medicine. 2023; 12(20):6464. https://doi.org/10.3390/jcm12206464
Chicago/Turabian StyleBergström, Johanna, Emilia Möller Rydberg, David Wennergren, and Karin Svensson Malchau. 2023. "Incidence and Risk Factors for Surgical Site Infection in Ankle Fractures: An Observational Study of 480 Patients in Sweden" Journal of Clinical Medicine 12, no. 20: 6464. https://doi.org/10.3390/jcm12206464
APA StyleBergström, J., Möller Rydberg, E., Wennergren, D., & Svensson Malchau, K. (2023). Incidence and Risk Factors for Surgical Site Infection in Ankle Fractures: An Observational Study of 480 Patients in Sweden. Journal of Clinical Medicine, 12(20), 6464. https://doi.org/10.3390/jcm12206464