
Relationships between Jumping Performance and Psychological Readiness to Return to Sport 6 Months Following Anterior Cruciate Ligament Reconstruction: A Cross-Sectional Study
 , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Recruitment
2.2. Surgical Technique and Rehabilitation Protocol
2.3. Follow-Up Assessment
2.4. Statistical Analysis
3. Results
3.1. Demographic Data
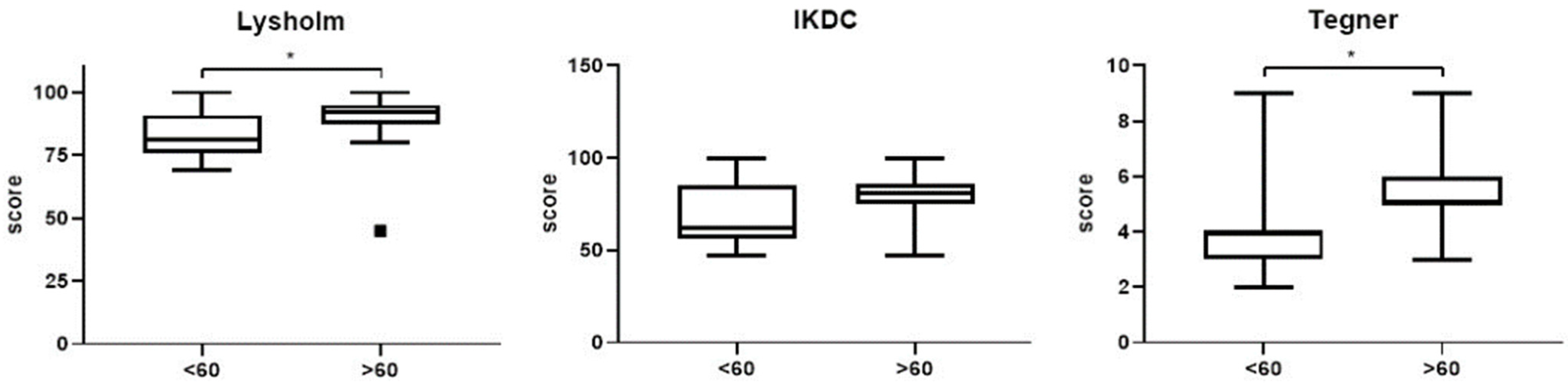
3.2. Subjective Knee Function
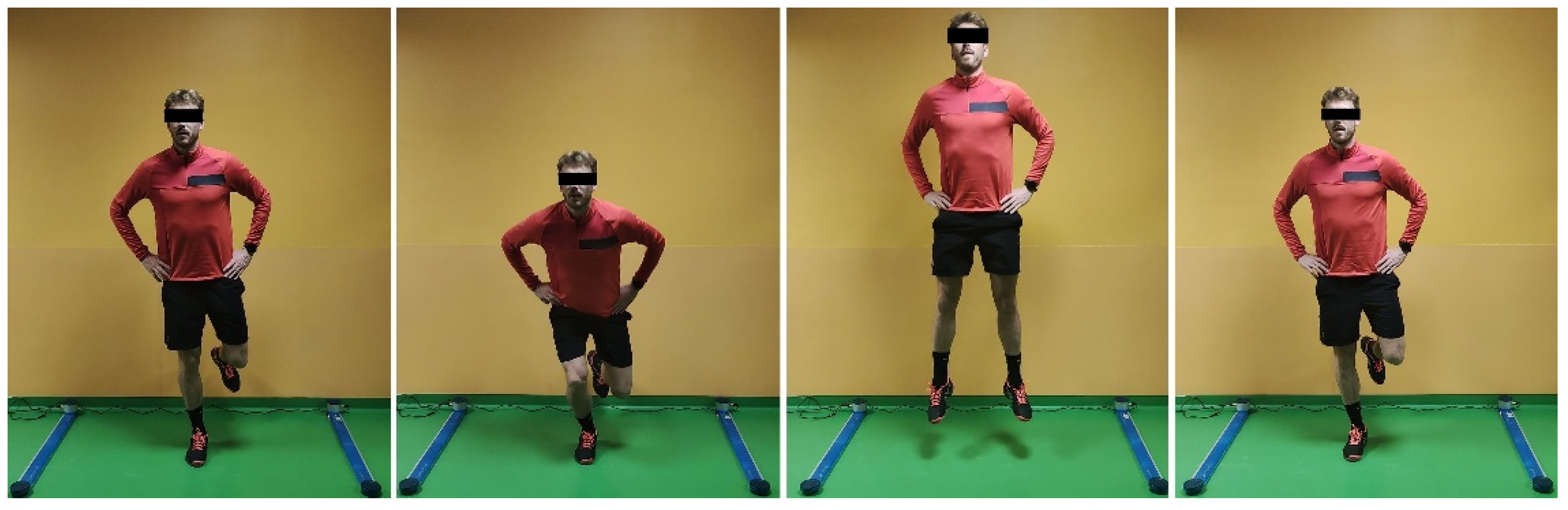
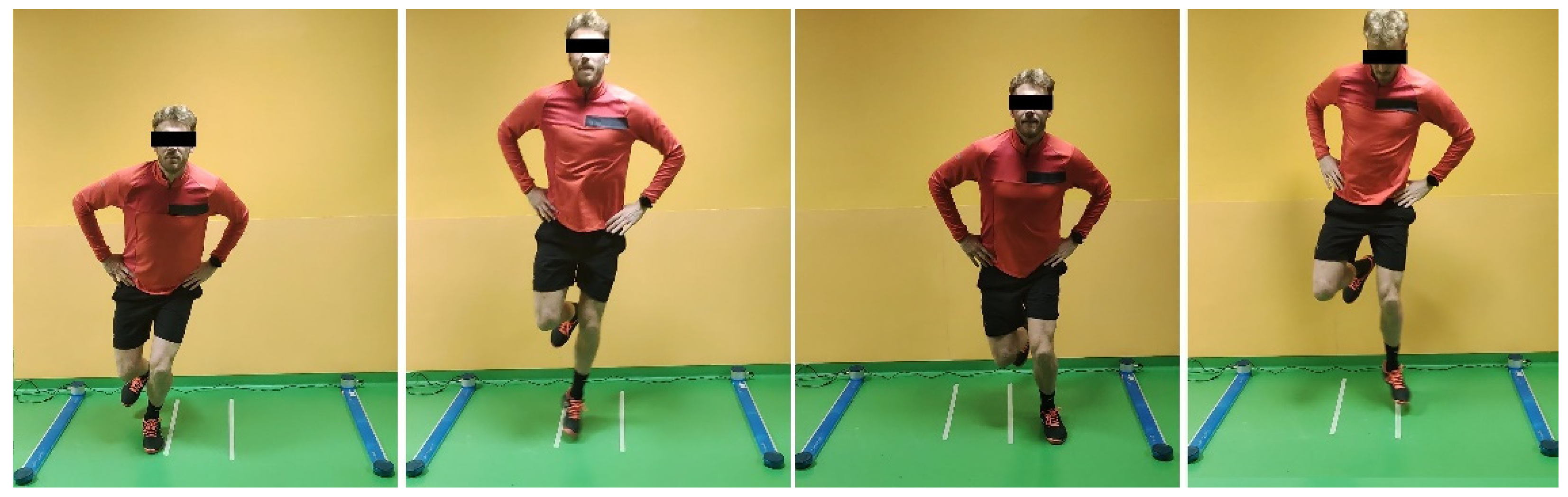
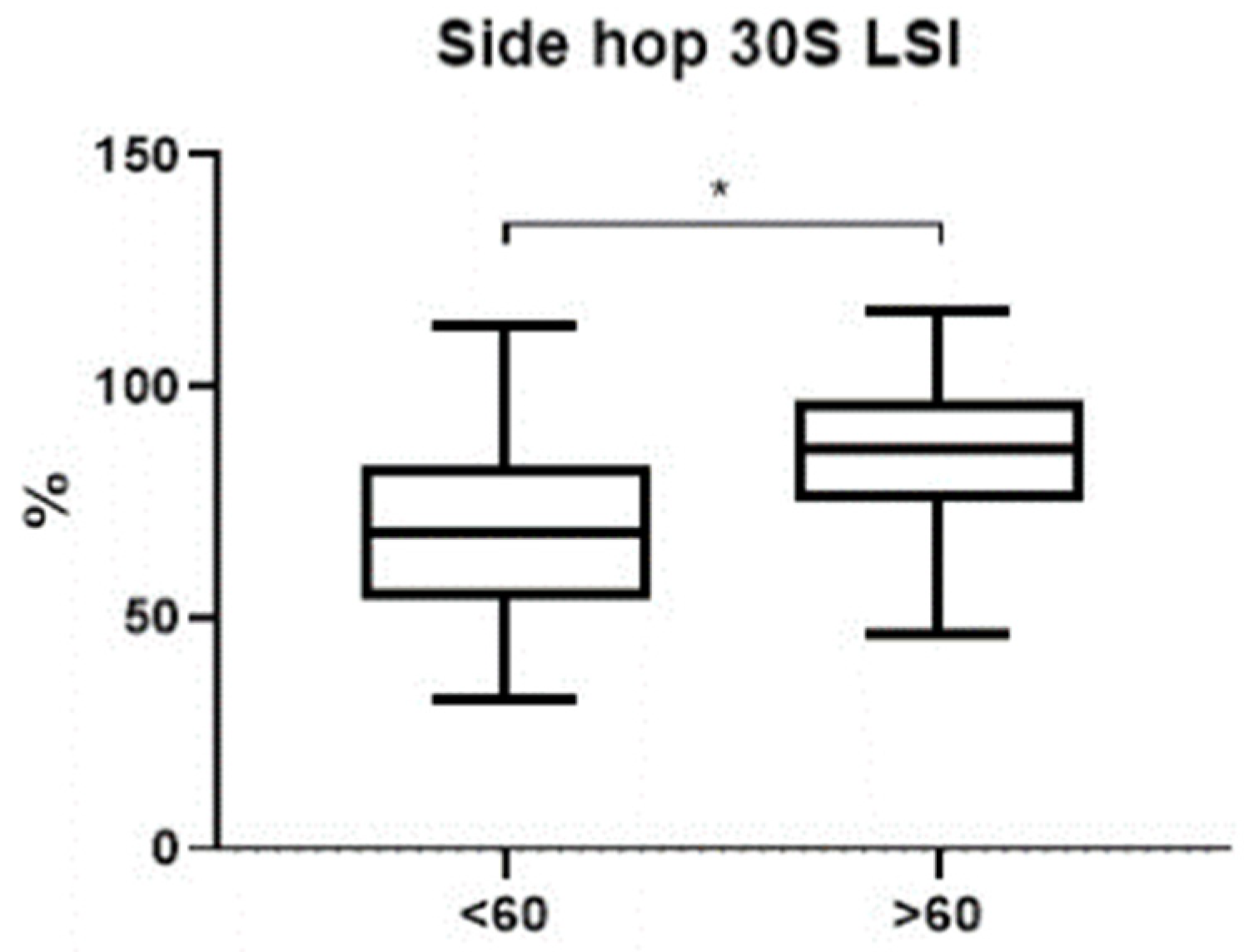
3.3. Jump Battery Tests
3.4. Results According to ACL-RSI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McCullough, K.A.; Phelps, K.D.; Spindler, K.P.; Matava, M.J.; Dunn, W.R.; Parker, R.D.; Group, M.; Reinke, E.K. Return to high school- and college-level football after anterior cruciate ligament reconstruction: A Multicenter Orthopaedic Outcomes Network (MOON) cohort study. Am. J. Sports Med. 2012, 49, 2523–2529. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Return-to-sport outcomes at 2 to 7 years after anterior cruciate ligament reconstruction surgery. Am. J. Sports Med. 2012, 40, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, V.H.; Jones, M.; Borque, K.A.; Balendra, G.; White, N.P.; Ball, S.V.; Williams, A. Rates and Levels of Elite Sport Participation at 5 Years after Revision ACL Reconstruction. Am. J. Sports Med. 2022, 50, 3762–3769. [Google Scholar] [CrossRef]
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to sport following anterior cruciate ligament reconstruction surgery: A systematic review and meta-analysis on the state of play. Br. J. Sports Med. 2011, 45, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Webster, K.E.; Feller, J.A. A research update on the state of play for return to sport after anterior cruciate ligament reconstruction. J. Orthop. Traumatol. 2019, 20, 10. [Google Scholar] [CrossRef] [PubMed]
- Legnani, C.; Peretti, G.M.; Del Re, M.; Borgo, E.; Ventura, A. Return to sports and re-rupture rate following anterior cruciate ligament reconstruction in amateur sportsman: Long-term outcomes. J. Sports Med. Phys. Fitness 2019, 59, 1902–1907. [Google Scholar] [CrossRef]
- Zhao, D.; Pan, J.K.; Lin, F.Z.; Luo, M.H.; Liang, G.H.; Zeng, L.F.; Huang, H.T.; Han, Y.H.; Xu, N.J.; Yang, W.Y.; et al. Risk Factors for Revision or Rerupture After Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2022, 3, 3635465221119787. [Google Scholar] [CrossRef]
- Crotty, N.M.N.; Daniels, K.A.J.; McFadden, C.; Cafferkey, N.; King, E. Relationship Between Isokinetic Knee Strength and Single-Leg Drop Jump Performance 9 Months after ACL Reconstruction. Orthop. J. Sports Med. 2022, 10, 23259671211063800. [Google Scholar] [CrossRef]
- Turk, R.; Shah, S.; Chilton, M.; Thomas, T.L.; Anene, C.; Mousad, A.; Le Breton, S.; Li, L.; Pettit, R.; Ives, K.; et al. Critical Criteria Recommendations: Return to Sport After ACL reconstruction requires evaluation of time after surgery of 8 months, >2 functional tests, psychological readiness, and quadriceps/hamstring strength. Arthroscopy 2022. [Google Scholar] [CrossRef]
- Chona, D.; Eriksson, K.; Young, S.W.; Denti, M.; Sancheti, P.K.; Safran, M.; Sherman, S. Return to sport following anterior cruciate ligament reconstruction: The argument for a multimodal approach to optimise decision-making: Current concepts. J. ISAKOS 2021, 6, 344–348. [Google Scholar] [CrossRef]
- Kotsifaki, A.; Van Rossom, S.; Whiteley, R.; Korakakis, V.; Bahr, R.; Sideris, V.; Jonkers, I. Single leg vertical jump performance identifies knee function deficits at return to sport after ACL reconstruction in male athletes. Br. J. Sports Med. 2022, 56, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Ventura, A.; Iori, S.; Legnani, C.; Terzaghi, C.; Borgo, E.; Albisetti, W. Single-bundle versus double-bundle anterior cruciate ligament reconstruction: Assessment with vertical jump test. Arthroscopy 2013, 29, 1201–1210. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, J.; Hirohata, K.; Ohji, S.; Ohmi, T.; Mitomo, S.; Koga, H.; Yagishita, K. Cross-sectional study on relationships between physical function and psychological readiness to return to sport after anterior cruciate ligament reconstruction. BMC Sports Sci. Med. Rehabil. 2022, 14, 97. [Google Scholar] [CrossRef] [PubMed]
- Ueda, Y.; Matsushita, T.; Shibata, Y.; Takiguchi, K.; Ono, K.; Kida, A.; Ono, R.; Nagai, K.; Hoshino, Y.; Matsumoto, T.; et al. Association Between Meeting Return-to-Sport Criteria and Psychological Readiness to Return to Sport after Anterior Cruciate Ligament Reconstruction. Orthop. J. Sports Med. 2022, 110, 23259671221093985. [Google Scholar] [CrossRef] [PubMed]
- King, E.; Richter, C.; Franklyn-Miller, A.; Franklyn-Miller, A.; Daniels, K.; Wadey, R.; Moran, R.; Strike, S. Whole-body biomechanical differences between limbs exist 9 months after ACL reconstruction across jump/landing tasks. Scand J. Med. Sci. Sports 2018, 28, 2567–2578. [Google Scholar] [CrossRef]
- Thomeé, R.; Neeter, C.; Gustavsson, A.; Thomeé, P.; Augustsson, J.; Eriksson, B.; Karlsson, J. Variability in leg muscle power and hop performance after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1143–1151. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A. Evaluation of the Responsiveness of the Anterior Cruciate Ligament Return to Sport After Injury (ACL-RSI) Scale. Orthop. J. Sports Med. 2021, 9, 23259671211031240. [Google Scholar] [CrossRef]
- Thiebat, G.; Cucchi, D.; Spreafico, A.; Muzzi, S.; Viganò, M.; Visconti, L.; Facchini, F.; de Girolamo, L. Italian version of the anterior cruciate ligament-return to sport after injury scale (IT ACL-RSI): Translation, cross-cultural adaptation, validation and ability to predict the return to sport at medium-term follow-up in a population of sport patients. Knee. Surg. Sports Traumatol. Arthrosc. 2022, 30, 270–279. [Google Scholar] [CrossRef]
- McPherson, A.L.; Feller, J.A.; Hewett, T.E.; Webster, K.E. Psychological readiness to return to sport is associated with Second anterior cruciate ligament injuries. Am. J. Sports Med. 2019, 47, 857–862. [Google Scholar] [CrossRef]
- Lysholm, J.; Gillquist, J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am. J. Sports Med. 1982, 10, 150–154. [Google Scholar] [CrossRef]
- Padua, R.; Bondì, R.; Ceccarelli, E.; Bondì, L.; Romanini, E.; Zanoli, G.; Campi, S. Italian Version of the International Knee Documentation Committee Subjective Knee Form: Cross-Cultural Adaptation and Validation. Arthroscopy 2004, 20, 819–823. [Google Scholar] [CrossRef] [PubMed]
- Tegner, Y.; Lysholm, J. Rating systems in the evaluation of knee ligament injuries. Clin. Orthop. Relat. Res. 1985, 198, 43–49. [Google Scholar] [CrossRef]
- Gustavsson, A.; Neeter, C.; Thomeé, P.; Silbernagel, K.G.; Augustsson, J.; Thomeé, R.; Karlsson, J. A test battery for evaluating hop performance in patients with an ACL injury and patients who have undergone ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2006, 4, 778–788. [Google Scholar] [CrossRef]
- Ma, B.; Zhang, T.T.; Jia, Y.D.; Wang, H.; Zhu, X.Y.; Zhang, W.J.; Li, X.M.; Liu, H.B.; Xie, D. Characteristics of vertical drop jump to screen the anterior cruciate ligament injury. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 7395–7403. [Google Scholar] [PubMed]
- Aizawa, J.; Hirohata, K.; Ohji, S.; Ohmi, T.; Koga, H.; Yagishita, K. Factors associated with psychological readiness to return to sports with cutting, pivoting, and jumplandings after primary ACL reconstruction. Orthop. J. Sports Med. 2020, 8, 2325967120964484. [Google Scholar] [PubMed]
- Webster, K.E.; Nagelli, C.V.; Hewett, T.E.; Feller, J.A. Factors associated with psychological readiness to return to sport after anterior cruciate ligament reconstruction surgery. Am. J. Sports Med. 2018, 46, 1545–1550. [Google Scholar] [CrossRef] [PubMed]
- Sadeqi, M.; Klouche, S.; Bohu, Y.; Herman, S.; Lefevre, N.; Gerometta, A. Progression of the psychological ACLRSI score and return to sport after anterior cruciate ligament reconstruction: A prospective 2-Year follow-up study from the French prospective anterior cruciate ligament reconstruction cohort study (FAST). Orthop. J. Sports Med. 2018, 6, 2325967118812819. [Google Scholar] [PubMed]
- Senorski, E.H.; Svantesson, E.; Beischer, S.; Thomeé, C.; Thomeé, R.; Karlsson, J.; Samuelsson, K. Low 1-Year Return-to-Sport Rate After Anterior Cruciate Ligament Reconstruction Regardless of Patient and Surgical Factors A Prospective Cohort Study of 272 Patients. Am. J. Sports Med. 2018, 46, 1551–1558. [Google Scholar] [CrossRef] [PubMed]
- Raizah, A.; Alhefzi, A.; Alshubruqi, A.A.M.; Hoban, M.A.M.A.; Ahmad, I.; Ahmad, F. Perceived Kinesiophobia and Its Association with Return to Sports Activity Following Anterior Cruciate Ligament Reconstruction Surgery: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 10776. [Google Scholar] [CrossRef]
- Sánchez Romero, E.A.; Lim, T.; Alonso Pérez, J.L.; Castaldo, M.; Martínez Lozano, P.; Villafañe, J.H. Identifying Clinical and MRI Characteristics Associated with Quality of Life in Patients with Anterior Cruciate Ligament Injury: Prognostic Factors for Long-Term. Int. J. Environ. Res. Public Health. 2021, 18, 12845. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | ACL-RSI > 60 | ACL-RSI < 60 | p-Value | |
|---|---|---|---|---|
| No. of patients | 31 | 20 | 11 | |
| Gender Male Female | 29 2 | 19 1 | 10 1 | |
| Mean ACL-RSI score (SD) | 68.3 (16.2) | 78.2 (9.1) | 50.2 (8.5) | |
| Mean age at surgery (SD) (yr) | 34.6 (11.7) | 34.7 (11.4) | 34.4 (12.5) | 0.9 |
| Mean BMI (SD) | 25.1 (3.2) | 25.4 (3.4) | 24.5 (2.7) | 0.4 |
| Pre-Operative | Follow-Up | p-Value | |
|---|---|---|---|
| Lysholm score (mean, SD) | 68.4 (15.6) | 87.1 (11.2) | <0.001 |
| Mean ACL-RSI score (SD) | 51.9 (13.0) | 77.1 (14.6) | <0.001 |
| Mean age at surgery (SD) (yr) | 46.2 (23.2) | 68.3 (16.2) | <0.001 |
| Tegner activity level (mean, SD) | 4.2 (2.4) | 5.1 (1.8) | 0.161 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Legnani, C.; Del Re, M.; Viganò, M.; Peretti, G.M.; Borgo, E.; Ventura, A. Relationships between Jumping Performance and Psychological Readiness to Return to Sport 6 Months Following Anterior Cruciate Ligament Reconstruction: A Cross-Sectional Study. J. Clin. Med. 2023, 12, 626. https://doi.org/10.3390/jcm12020626
Legnani C, Del Re M, Viganò M, Peretti GM, Borgo E, Ventura A. Relationships between Jumping Performance and Psychological Readiness to Return to Sport 6 Months Following Anterior Cruciate Ligament Reconstruction: A Cross-Sectional Study. Journal of Clinical Medicine. 2023; 12(2):626. https://doi.org/10.3390/jcm12020626
Chicago/Turabian StyleLegnani, Claudio, Matteo Del Re, Marco Viganò, Giuseppe M. Peretti, Enrico Borgo, and Alberto Ventura. 2023. "Relationships between Jumping Performance and Psychological Readiness to Return to Sport 6 Months Following Anterior Cruciate Ligament Reconstruction: A Cross-Sectional Study" Journal of Clinical Medicine 12, no. 2: 626. https://doi.org/10.3390/jcm12020626
APA StyleLegnani, C., Del Re, M., Viganò, M., Peretti, G. M., Borgo, E., & Ventura, A. (2023). Relationships between Jumping Performance and Psychological Readiness to Return to Sport 6 Months Following Anterior Cruciate Ligament Reconstruction: A Cross-Sectional Study. Journal of Clinical Medicine, 12(2), 626. https://doi.org/10.3390/jcm12020626