
Leishmania Infection during Ruxolitinib Treatment: The Cytokines-Based Immune Response in the Setting of Immunocompromised Patients

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
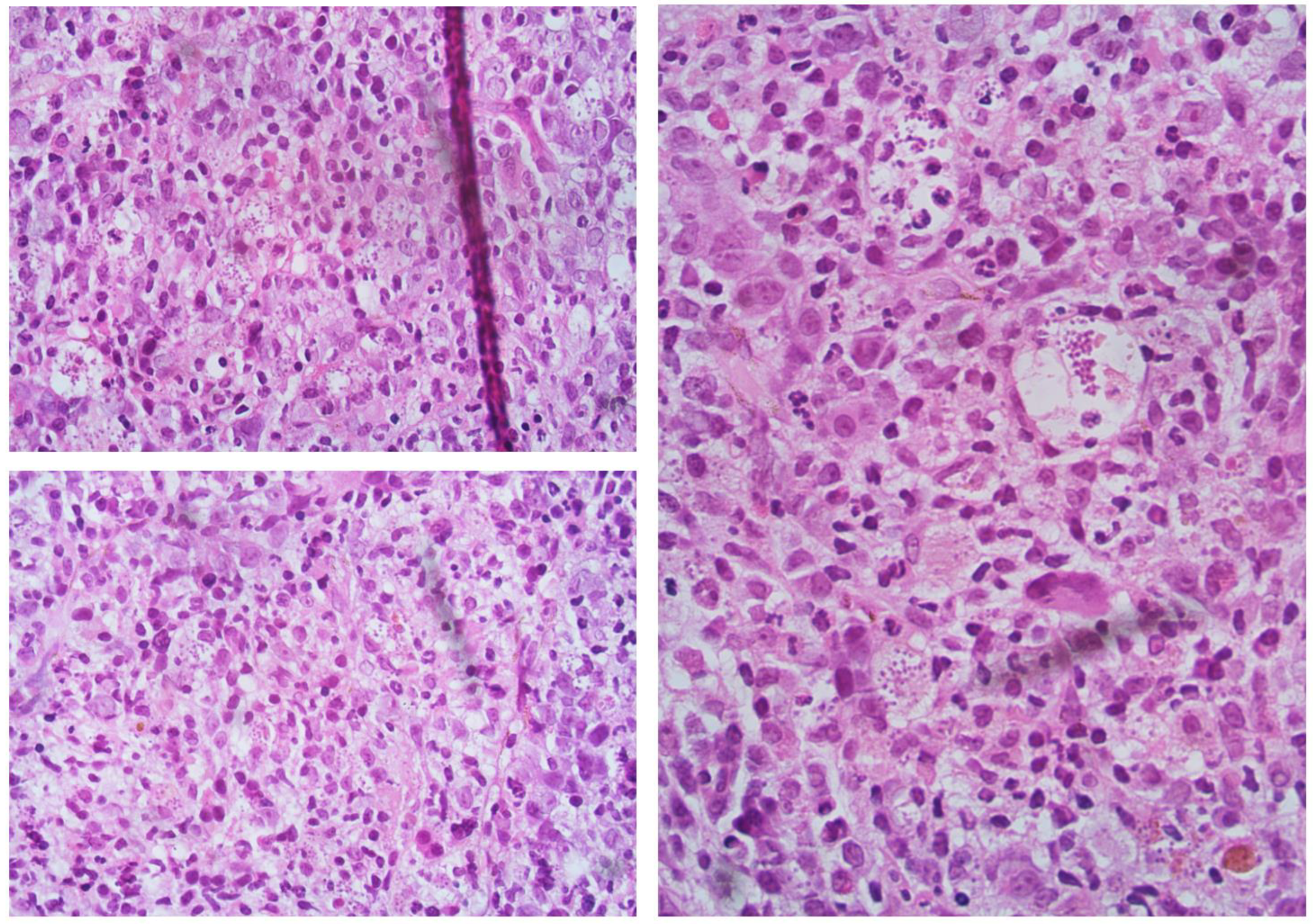
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tefferi, A.; Lasho, T.L.; Jimma, T.; Finke, C.M.; Gangat, N.; Vaidya, R.; Begna, K.H.; Al-Kali, A.; Ketterling, R.P.; Hanson, C.A.; et al. One Thousand Patients With Primary Myelofibrosis: The Mayo Clinic Experience. Mayo Clin. Proc. 2012, 87, 25–33. [Google Scholar] [CrossRef]
- Harrison, C.; Kiladjian, J.-J.; Al-Ali, H.K.; Gisslinger, H.; Waltzman, R.; Stalbovskaya, V.; McQuitty, M.; Hunter, D.S.; Levy, R.; Knoops, L.; et al. JAK Inhibition with Ruxolitinib versus Best Available Therapy for Myelofibrosis. N. Engl. J. Med. 2012, 366, 787–798. [Google Scholar] [CrossRef]
- Elli, E.M.; Baratè, C.; Mendicino, F.; Palandri, F.; Palumbo, G.A. Mechanisms Underlying the Anti-Inflammatory and Immunosuppressive Activity of Ruxolitinib. Front. Oncol. 2019, 9, 1186. [Google Scholar] [CrossRef] [PubMed]
- Cervantes, F.; Dupriez, B.; Pereira, A.; Passamonti, F.; Reilly, J.T.; Morra, E.; Vannucchi, A.M.; Mesa, R.A.; Demory, J.L.; Barosi, G.; et al. New Prognostic Scoring System for Primary Myelofibrosis Based on a Study of the International Working Group for Myelofibrosis Research and Treatment. Blood 2009, 113, 2895–2901. [Google Scholar] [CrossRef]
- Maffioli, M.; Mora, B.; Ball, S.; Iurlo, A.; Elli, E.M.; Finazzi, M.C.; Polverelli, N.; Rumi, E.; Caramella, M.; Carraro, M.C.; et al. A Prognostic Model to Predict Survival after 6 Months of Ruxolitinib in Patients with Myelofibrosis. Blood Adv. 2022, 6, 1855–1864. [Google Scholar] [CrossRef]
- Scalzulli, E.; Ielo, C.; Luise, C.; Musiu, P.; Bisegna, M.L.; Carmosino, I.; Assanto, G.M.; Martelli, M.; Breccia, M. RR6 Prognostic Model Provides Information about Survival for Myelofibrosis Treated with Ruxolitinib: Validation in a Real-Life Cohort. Blood Adv. 2022, 6, 4424–4426. [Google Scholar] [CrossRef] [PubMed]
- Duminuco, A.; Nardo, A.; Garibaldi, B.; Vetro, C.; Longo, A.; Giallongo, C.; di Raimondo, F.; Palumbo, G.A. Prediction of Survival and Prognosis Migration from Gold-Standard Scores in Myelofibrosis Patients Treated with Ruxolitinib Applying the RR6 Prognostic Model in a Monocentric Real-Life Setting. J. Clin. Med. 2022, 11, 7418. [Google Scholar] [CrossRef] [PubMed]
- Aronson, N.; Herwaldt, B.L.; Libman, M.; Pearson, R.; Lopez-Velez, R.; Weina, P.; Carvalho, E.; Ephros, M.; Jeronimo, S.; Magill, A. Diagnosis and Treatment of Leishmaniasis: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Am. J. Trop. Med. Hyg. 2017, 96, 24–45. [Google Scholar] [CrossRef] [PubMed]
- Rane, S.G.; Reddy, E.P. Janus Kinases: Components of Multiple Signaling Pathways. Oncogene 2000, 19, 5662–5679. [Google Scholar] [CrossRef] [PubMed]
- Zeiser, R.; von Bubnoff, N.; Butler, J.; Mohty, M.; Niederwieser, D.; Or, R.; Szer, J.; Wagner, E.M.; Zuckerman, T.; Mahuzier, B.; et al. Ruxolitinib for Glucocorticoid-Refractory Acute Graft-versus-Host Disease. N. Engl. J. Med. 2020, 382, 1800–1810. [Google Scholar] [CrossRef]
- Maschmeyer, G.; de Greef, J.; Mellinghoff, S.C.; Nosari, A.; Thiebaut-Bertrand, A.; Bergeron, A.; Franquet, T.; Blijlevens, N.M.A.; Maertens, J.A. Infections Associated with Immunotherapeutic and Molecular Targeted Agents in Hematology and Oncology. A Position Paper by the European Conference on Infections in Leukemia (ECIL). Leukemia 2019, 33, 844–862. [Google Scholar] [CrossRef]
- Lussana, F.; Cattaneo, M.; Rambaldi, A.; Squizzato, A. Ruxolitinib-Associated Infections: A Systematic Review and Meta-Analysis. Am. J. Hematol. 2018, 93, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Verstovsek, S.; Mesa, R.A.; Gotlib, J.; Gupta, V.; DiPersio, J.F.; Catalano, J.V.; Deininger, M.W.N.; Miller, C.B.; Silver, R.T.; Talpaz, M.; et al. Long-Term Treatment with Ruxolitinib for Patients with Myelofibrosis: 5-Year Update from the Randomized, Double-Blind, Placebo-Controlled, Phase 3 COMFORT-I Trial. J. Hematol. Oncol. 2017, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Harrison, C.N.; Vannucchi, A.M.; Kiladjian, J.J.; Al-Ali, H.K.; Gisslinger, H.; Knoops, L.; Cervantes, F.; Jones, M.M.; Sun, K.; McQuitty, M.; et al. Long-Term Findings from COMFORT-II, a Phase 3 Study of Ruxolitinib vs Best Available Therapy for Myelofibrosis. Leukemia 2016, 30, 1701–1707. [Google Scholar] [CrossRef]
- Dioverti, M.V.; Abu Saleh, O.M.; Tande, A.J. Infectious Complications in Patients on Treatment with Ruxolitinib: Case Report and Review of the Literature. Infect. Dis. 2018, 50, 381–387. [Google Scholar] [CrossRef]
- van Griensven, J.; Carrillo, E.; López-Vélez, R.; Lynen, L.; Moreno, J. Leishmaniasis in Immunosuppressed Individuals. Clin. Microbiol. Infect. 2014, 20, 286–299. [Google Scholar] [CrossRef]
- Lattes, R.; Lasala, M.B. Chagas Disease in the Immunosuppressed Patient. Clin. Microbiol. Infect. 2014, 20, 300–309. [Google Scholar] [CrossRef]
- Krause, P.J.; Gewurz, B.E.; Hill, D.; Marty, F.M.; Vannier, E.; Foppa, I.M.; Furman, R.R.; Neuhaus, E.; Skowron, G.; Gupta, S.; et al. Persistent and Relapsing Babesiosis in Immunocompromised Patients. Clin. Infect. Dis. 2008, 46, 370–376. [Google Scholar] [CrossRef]
- Cota, G.F.; de Sousa, M.R.; Demarqui, F.N.; Rabello, A. The Diagnostic Accuracy of Serologic and Molecular Methods for Detecting Visceral Leishmaniasis in HIV Infected Patients: Meta-Analysis. PLoS Negl. Trop. Dis. 2012, 6, e1665. [Google Scholar] [CrossRef]
- Cota, G.F.; de Sousa, M.R.; de Freitas Nogueira, B.M.; Gomes, L.I.; Oliveira, E.; Assis, T.S.M.; de Mendonca, A.L.P.; Pinto, B.F.; Saliba, J.W.; Rabello, A. Comparison of Parasitological, Serological, and Molecular Tests for Visceral Leishmaniasis in HIV-Infected Patients: A Cross-Sectional Delayed-Type Study. Am. J. Trop. Med. Hyg. 2013, 89, 570–577. [Google Scholar] [CrossRef] [PubMed]
- Berman, J.D. Human Leishmaniasis: Clinical, Diagnostic, and Chemotherapeutic Developments in the Last 10 Years. Clin. Infect. Dis. 1997, 24, 684–703. [Google Scholar] [CrossRef]
- Farina, J.M.; García-Martínez, C.E.; Saldarriaga, C.; Pérez, G.E.; de Melo, M.B.; Wyss, F.; Sosa-Liprandi, A.; Ortiz-Lopez, H.I.; Gupta, S.; López-Santi, R.; et al. Leishmaniasis and Heart. Arch. Cardiol. Mex. 2022, 92, 85–93. [Google Scholar] [CrossRef]
- Martínez-Hernández, L.; Casamian-Sorrosal, D.; Barrera-Chacón, R.; Cuesta-Gerveno, J.M.; Belinchón-Lorenzo, S.; Gómez Nieto, L.C.; Duque-Carrasco, F.J. Comparison of Myocardial Damage among Dogs at Different Stages of Clinical Leishmaniasis and Dogs with Idiopathic Chronic Kidney Disease. Vet. J. 2017, 221, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Postorino, M.C.; Bellantoni, M.; Catalano, C.; Caridi, G.; de Rosa, M.; Seck, S.; Enia, G. Visceral Leishmaniasis Reactivation in Transplant Patients: A Minireview with Report of a New Case. J. Nephrol. 2011, 24, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, V.; Cordeiro-Da-Silva, A.; Laforge, M.; Silvestre, R.; Estaquier, J. Regulation of Immunity during Visceral Leishmania Infection. Parasites Vectors 2016, 9, 118. [Google Scholar] [CrossRef]
- Elmahallawy, E.K.; Alkhaldi, A.A.M.; Saleh, A.A. Host Immune Response against Leishmaniasis and Parasite Persistence Strategies: A Review and Assessment of Recent Research. Biomed. Pharmacother. 2021, 139, 111671. [Google Scholar] [CrossRef]
- Vouldoukis, I.; Bécherel, P.A.; Riveros-Moreno, V.; Arock, M.; da Silva, O.; Debré, P.; Mazier, D.; Mossalayi, M.D. Interleukin-10 and Interleukin-4 Inhibit Intracellular Killing of Leishmania Infantum and Leishmania Major by Human Macrophages by Decreasing Nitric Oxide Generation. Eur. J. Immunol. 1997, 27, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Veletic, I.; Prijic, S.; Manshouri, T.; Nogueras-Gonzalez, G.M.; Verstovsek, S.; Estrov, Z. Altered T-Cell Subset Repertoire Affects Treatment Outcome of Patients with Myelofibrosis. Haematologica 2021, 106, 2384–2396. [Google Scholar] [CrossRef]
- Wherry, E.J. T Cell Exhaustion. Nat. Immunol. 2011, 12, 492–499. [Google Scholar] [CrossRef]
- Yi, J.S.; Cox, M.A.; Zajac, A.J. T-Cell Exhaustion: Characteristics, Causes and Conversion. Immunology 2010, 129, 474–481. [Google Scholar] [CrossRef]
- Huarte, E.; Peel, M.T.; Verbist, K.; Fay, B.L.; Bassett, R.; Albeituni, S.; Nichols, K.E.; Smith, P.A. Ruxolitinib, a JAK1/2 Inhibitor, Ameliorates Cytokine Storm in Experimental Models of Hyperinflammation Syndrome. Front. Pharmacol. 2021, 12, 650295. [Google Scholar] [CrossRef] [PubMed]
- Chughlay, M.F.; Barnes, K.I.; el Gaaloul, M.; Abla, N.; Möhrle, J.J.; Griffin, P.; van Giersbergen, P.; Reuter, S.E.; Schultz, H.B.; Kress, A.; et al. Safety, Tolerability, Pharmacokinetics, and Pharmacodynamics of Coadministered Ruxolitinib and Artemether-Lumefantrine in Healthy Adults. Antimicrob. Agents Chemother. 2022, 66, 1584–1605. [Google Scholar] [CrossRef] [PubMed]
- McLornan, D.P.; Khan, A.A.; Harrison, C.N. Immunological Consequences of JAK Inhibition: Friend or Foe? Curr. Hematol. Malig. Rep. 2015, 10, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Cui, T.; Wang, J.; Wang, Z. The Treatment Based on Ruxolitinib and Amphotericin B Is Effective for Relapsed Leishmaniasis-Related Hemophagocytic Lymphohistiocytosis: A Case Report and Literature Review. Infect. Drug. Resist. 2022, 15, 6625–6629. [Google Scholar] [CrossRef]
- Fiorino, F.; Sicuranza, A.; Ciabattini, A.; Santoni, A.; Pastore, G.; Simoncelli, M.; Polvere, J.; Galimberti, S.; Auddino, S.; Baratè, C.; et al. The Slower Antibody Response in Myelofibrosis Patients after Two Doses of MRNA SARS-CoV-2 Vaccine Calls for a Third Dose. Biomedicines 2021, 9, 1480. [Google Scholar] [CrossRef] [PubMed]
- Piyasiri, S.B.; Samaranayake, T.N.; Silva, H.; Manamperi, N.H.; Karunaweera, N.D. ELISA-Based Evaluation of Antibody Response to Leishmania in a Region Endemic for Cutaneous Leishmaniasis. Parasite Immunol. 2022, 44, e12940. [Google Scholar] [CrossRef]
- Guglielmelli, P.; Mazzoni, A.; Maggi, L.; Kiros, S.T.; Zammarchi, L.; Pilerci, S.; Rocca, A.; Spinicci, M.; Borella, M.; Bartoloni, A.; et al. Impaired Response to First SARS-CoV-2 Dose Vaccination in Myeloproliferative Neoplasm Patients Receiving Ruxolitinib. Am. J. Hematol. 2021, 96, E408–E410. [Google Scholar] [CrossRef]


{kind=link}
| T-CD4+ | T-CD8+ | |||||||
|---|---|---|---|---|---|---|---|---|
| INFγ+ | TNFα+ | IL-2+ | IL-4+ | IL-17+ | INFγ+ | TNFα+ | IL-2+ | |
| At diagnosis | 7.01 | 32.5 | 21.2 | 6.36 | 3 | 16.75 | 17.6 | 9.4 |
| +21 | 25.2 | 75 | 63.4 | 3.28 | 2.11 | 56 | 63.4 | 41 |
| +42 | 18.7 | 58.7 | 52.8 | 0.6 | 1.64 | 42.5 | 48 | 34.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duminuco, A.; Scarso, S.; Cupri, A.; Parrinello, N.L.; Villari, L.; Scuderi, G.; Giunta, G.; Leotta, S.; Milone, G.A.; Giuffrida, G.; et al. Leishmania Infection during Ruxolitinib Treatment: The Cytokines-Based Immune Response in the Setting of Immunocompromised Patients. J. Clin. Med. 2023, 12, 578. https://doi.org/10.3390/jcm12020578
Duminuco A, Scarso S, Cupri A, Parrinello NL, Villari L, Scuderi G, Giunta G, Leotta S, Milone GA, Giuffrida G, et al. Leishmania Infection during Ruxolitinib Treatment: The Cytokines-Based Immune Response in the Setting of Immunocompromised Patients. Journal of Clinical Medicine. 2023; 12(2):578. https://doi.org/10.3390/jcm12020578
Chicago/Turabian StyleDuminuco, Andrea, Salvatore Scarso, Alessandra Cupri, Nunziatina Laura Parrinello, Loredana Villari, Grazia Scuderi, Giuliana Giunta, Salvatore Leotta, Giulio Antonio Milone, Giulia Giuffrida, and et al. 2023. "Leishmania Infection during Ruxolitinib Treatment: The Cytokines-Based Immune Response in the Setting of Immunocompromised Patients" Journal of Clinical Medicine 12, no. 2: 578. https://doi.org/10.3390/jcm12020578
APA StyleDuminuco, A., Scarso, S., Cupri, A., Parrinello, N. L., Villari, L., Scuderi, G., Giunta, G., Leotta, S., Milone, G. A., Giuffrida, G., Palumbo, G. A., & Milone, G. (2023). Leishmania Infection during Ruxolitinib Treatment: The Cytokines-Based Immune Response in the Setting of Immunocompromised Patients. Journal of Clinical Medicine, 12(2), 578. https://doi.org/10.3390/jcm12020578