
Serious Complications and Recurrence following Sacrospinous Ligament Fixation for the Correction of Apical Prolapse

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Outcomes
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghetti, C.; Lowder, J.L.; Ellison, R.; Krohn, M.A.; Moalli, P. Depressive symptoms in women seeking surgery for pelvic organ prolapse. Int. Urogynecol. J. 2010, 21, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Barber, M.D.; Maher, C. Epidemiology and outcome assessment of pelvic organ prolapse. Int. Urogynecol. J. 2013, 24, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Larouche, M.; Belzile, E.; Geoffrion, R. Surgical Management of Symptomatic Apical Pelvic Organ Prolapse: A Systematic Review and Meta-analysis. Obstet. Gynecol. 2021, 137, 1061–1073. [Google Scholar] [CrossRef] [PubMed]
- Summers, A.; Winkel, L.A.; Hussain, H.K.; DeLancey, J.O. The relationship between anterior and apical compartment support. Am. J. Obstet. Gynecol. 2006, 194, 1438–1443. [Google Scholar] [CrossRef] [PubMed]
- Tulikangas, P. Pelvic Organ Prolapse: ACOG Practice Bulletin, Number 214. Obstet. Gynecol. 2019, 134, e126–e142. [Google Scholar]
- Maher, C.; Feiner, B.; Baessler, K.; Christmann-Schmid, C.; Haya, N.; Brown, J. Surgery for women with apical vaginal prolapse. Cochrane Database Syst. Rev. 2016, 2017, CD012376. [Google Scholar] [CrossRef] [PubMed]
- Le Normand, L.; Cosson, M.; Cour, F.; Deffieux, X.; Donon, L.; Ferry, P.; Fatton, B.; Hermieu, J.-F.; Marret, H.; Meurette, G.; et al. Clinical practice guidelines: Synthesis of the guidelines for the surgical treatment of primary pelvic organ prolapse in women by the AFU, CNGOF, SIFUD-PP, SNFCP, and SCGP. J. Gynecol. Obstet. Biol. Reprod. 2016, 45, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- Richter, K. Massive eversion of the vagina: Pathogenesis, diagnosis, and therapy of the “true” prolapse of the vaginal stump. Clin. Obstet. Gynecol. 1982, 25, 897–912. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, R.P.; Tomezsko, J.E.; Winkler, H.A.; Koduri, S.; Culligan, P.J.; Sand, P.K. Anterior or posterior sacrospinous vaginal vault suspension: Long-term anatomic and functional evaluation. Obstet. Gynecol. 2001, 98, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Holt, E. US FDA rules manufacturers to stop selling mesh devices. Lancet 2019, 393, 1686. [Google Scholar] [CrossRef] [PubMed]
- Fritel, X.; de Tayrac, R.; de Keizer, J.; Campagne-Loiseau, S.; Cosson, M.; Ferry, P.; Deffieux, X.; Lucot, J.; Wagner, L.; Debodinance, P.; et al. Serious complications and recurrences after pelvic organ prolapse surgery for 2309 women in the VIGI-MESH registry. BJOG 2021, 129, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Bump, R.; Mattiasson, A.; Bø, K.; Brubaker, L.P.; DeLancey, J.O.; Klarskov, P.; Shull, B.L.; Smith, A.R. The Standardization of Terminology of Female Pelvic Organ Prolapse and Pelvic Floor Dysfunction. In Textbook of Female Urology and Urogynecology, 3rd ed.; CRC Press: Boca Raton, FL, USA, 2010; pp. 1113–1120. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Feiner, B.; Baessler, K.; Christmann-Schmid, C.; Haya, N.; Marjoribanks, J. Transvaginal mesh or grafts compared with native tissue repair for vaginal prolapse. Cochrane Database Syst. Rev. 2016, 2, CD012079. [Google Scholar] [CrossRef] [PubMed]
- Nager, C.W.; Visco, A.G.; Richter, H.E.; Rardin, C.R.; Komesu, Y.; Harvie, H.S.; Zyczynski, H.M.; Paraiso, M.F.R.; Mazloomdoost, D.; Sridhar, A.; et al. Effect of sacrospinous hysteropexy with graft vs. vaginal hysterectomy with uterosacral ligament suspension on treatment failure in women with uterovaginal prolapse: 5-year results of a randomized clinical trial. Am. J. Obstet. Gynecol. 2021, 225, 153.e1–153.e31. [Google Scholar] [CrossRef] [PubMed]
- Solomon, E.R.; Marie, P.S.; Jones, K.A.; Harmanli, O. Anterior Bilateral Sacrospinous Ligament Fixation: A Safe Route for Apical Repair. Female Pelvic Med. Reconstr. Surg. 2020, 26, e33–e36. [Google Scholar] [CrossRef] [PubMed]
- Yadav, G.S.; Gaddam, N.; Rahn, D.D. A Comparison of Perioperative Outcomes, Readmission, and Reoperation for Sacrospinous Ligament Fixation, Uterosacral Ligament Suspension, and Minimally Invasive Sacrocolpopexy. Female Pelvic Med. Reconstr. Surg. 2020, 27, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Delacroix, C.; Allegre, L.; Chatziioannidou, K.; Gérard, A.; Fatton, B.; de Tayrac, R. Anterior bilateral sacrospinous ligament fixation with concomitant anterior native tissue repair: A pilot study. Int. Urogynecol. J. 2022, 33, 3519–3527. [Google Scholar] [CrossRef] [PubMed]
- Nager, C.W.; Visco, A.G.; E Richter, H.; Rardin, C.R.; Rogers, R.G.; Harvie, H.S.; Zyczynski, H.M.; Paraiso, M.F.R.; Mazloomdoost, D.; Grey, S.; et al. Effect of vaginal mesh hysteropexy vs. vaginal hysterectomy with uterosacral ligament suspension on treatment failure in women with uterovaginal prolapse: A randomized clinical trial. J. Am. Med. Assoc. 2019, 322, 1054–1065. [Google Scholar] [CrossRef] [PubMed]
- Salman, S.; Babaoglu, B.; Kumbasar, S.; Bestel, M.; Gencer, F.K.; Tuna, G.; Besimoglu, B.; Yüksel, S.; Uçar, E. Comparison of Unilateral and Bilateral Sacrospinous Ligament Fixation Using Minimally Invasive Anchorage. Geburtshilfe Und Frauenheilkd. 2019, 79, 976–982. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
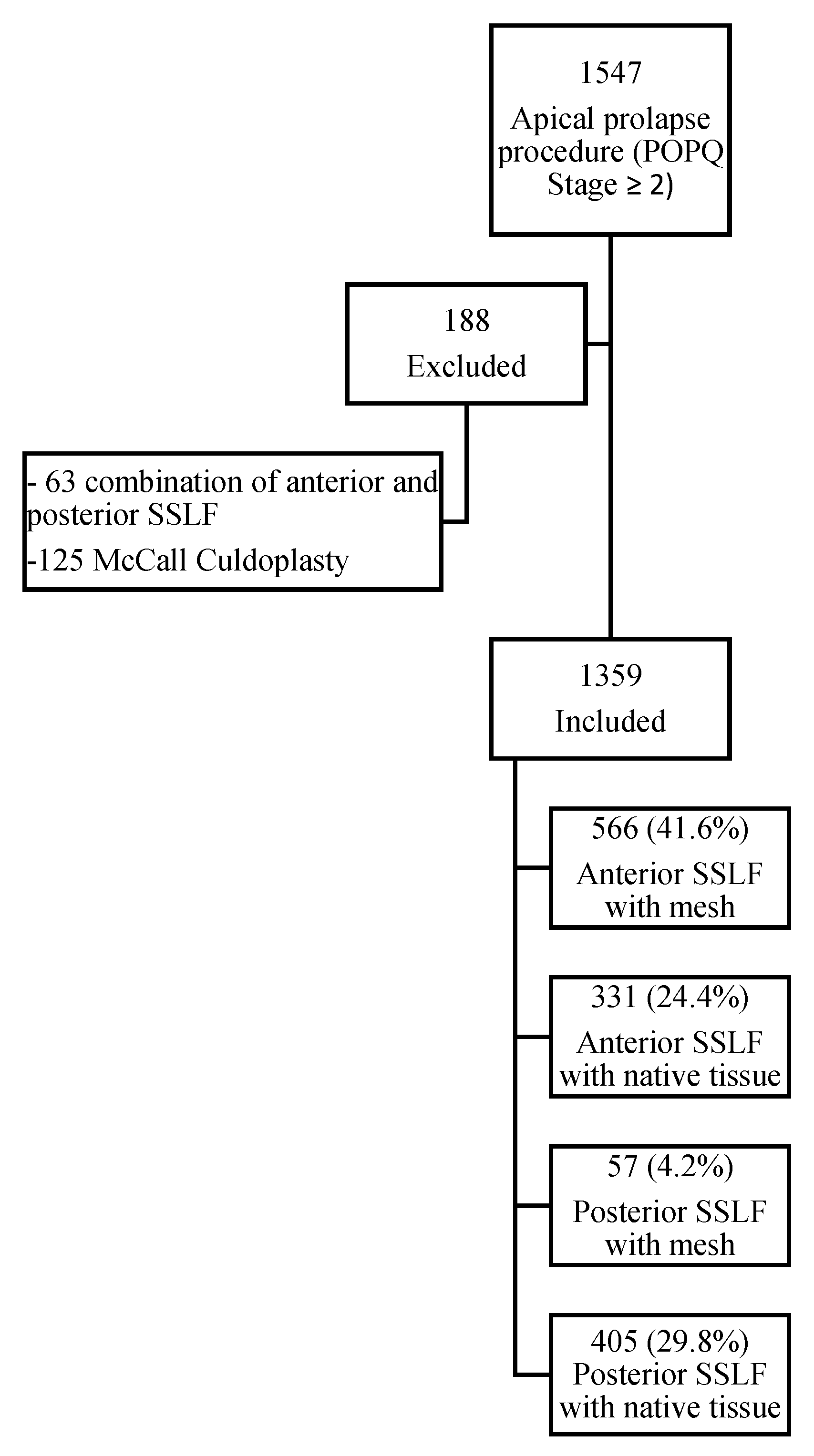
| Total Population N = 1359 | Anterior SSLF with Mesh N = 566 | Anterior SSLF with Native Tissue N = 331 | Posterior SSLF with Mesh N = 57 | Posterior SSLF with Native Tissue N = 405 | p | |
|---|---|---|---|---|---|---|
| Age mean (SD) | 69.4 (9.2) | 70.2 (7.3) | 69.4 (9.8) | 68.1 (7.8) | 68.6 (11) | 0.22 |
| BMI mean (SD) | 26.2 (4.5) | 26.3 (4.5) | 25.7 (4.3) | 27.5 (4.0) | 26.4 (4.8) | <0.01 |
| Smoking n (%) | 61 (4.6) | 21 (3.8) | 18 (5.6) | 4 (7.0) | 18 (4.7) | 0.43 |
| Diabetes n (%) | 143 (11.1) | 73 (13.4) | 28 (9.2) | 3 (5.4) | 39 (10.1) | 0.10 |
| Sexually active n (%) | 453 (39.0) | 174 (35.4) | 108 (39.8) | 20 (40.0) | 151 (43.3) | 0.14 |
| Menopausal status n (%) | 1261 (94.0) | 550 (97.3) | 301 (93.8) | 56 (98.2) | 354 (88.9) | <0.01 |
| ASA score | 0.64 | |||||
| 1 n (%) | 329 (24.2) | 135 (23.9) | 80 (24.2) | 15 (26.3) | 99 (24.4) | |
| 2 n (%) | 826 (60.8) | 346 (61.1) | 209 (63.1) | 31 (54.4) | 240 (59.3) | |
| 3 n (%) | 142 (10.4) | 68 (12.0) | 26 (7.9) | 8 (14.0) | 40 (9.9) | |
| 4 n (%) | 2 (0.1) | 2 (0.4) | 0 | 0 | 0 | |
| Past Surgical History | ||||||
| Subtotal Hysterectomy n (%) | 61 (4.5) | 23 (4.1) | 9 (2.7) | 4 (7.0) | 25 (6.1) | 0.09 |
| Total Hysterectomy n (%) | 273 (20.1) | 93 (16.4) | 42 (12.7) | 17 (29.8) | 121 (29.9) | <0.01 |
| SUI surgery with mesh n (%) | 110 (8.1) | 38 (6.7) | 24 (7.3) | 7 (12.2) | 41 (10.1) | 0.13 |
| SUI surgery without mesh n (%) | 58 (4.3) | 18 (3.2) | 9 (2.7) | 6 (10.5) | 25 (6.2) | <0.01 |
| POP surgery with mesh n (%) | 172 (12.7) | 62 (11.0) | 31 (9.4) | 19 (33.3) | 60 (14.8) | <0.01 |
| POP surgery without mesh n (%) | 132 (9.7) | 61 (10.8) | 15 (4.5) | 7 (12.3) | 49 (12.1) | <0.01 |
| Rectal prolapse with mesh n (%) | 13 (1.0) | 6 (1.1) | 2 (0.6) | 0 | 5 (1.2) | 0.84 |
| Rectal prolapse without mesh n (%) | 22 (1.6) | 10 (1.8) | 3 (0.9) | 1 (1.8) | 8 (2.0) | 0.63 |
| Total Population | Anterior SSLF with Mesh | Anterior SSLF with Native Tissue | Posterior SSLF with Mesh | Posterior SSLF with Native Tissue | p | |
|---|---|---|---|---|---|---|
| N | 1359 | 566 | 331 | 57 | 405 | |
| Bilateral procedure (%) | 1102 (81.1) | 564 (99.7) | 316 (95.5) | 57 (100.0) | 165 (40.7) | <0.01 |
| N | 1309 | 549 | 322 | 56 | 382 | |
| Mean surgical Time (±SD) | 76.1 (±41) | 77.5 (±43.1) | 75.3 (±41.6) | 64.5 (±36.3) | 76.3 (±37.6) | 0.12 |
| N | 1310 | 550 | 321 | 54 | 385 | |
| Mean blood loss (±SD) | 59.7 (±81.7) | 66.4 (±80.5) | 53 (±78.1) | 21.9 (±32.1) | 60.9 (±89.2) | <0.01 |
| Total Population N = 1359 | Anterior SSLF with Mesh N = 566 | Anterior SSLF with Native Tissue N = 331 | Posterior SSLF with Mesh N = 57 | Posterior SSLF with Native Tissue N = 405 | |
|---|---|---|---|---|---|
| Complications n (%) | 34 (2.5) | 20 (3.5) | 7 (2.1) | 2 (3.5) | 5 (1.2) |
| Grade IIIA n (%) | 5 (0.4) | 5 (0.9) | 0 | 0 | 0 |
| Grade IIIB n (%) | 28 (2.1) | 15 (2.7) | 6 (1.8) | 2 (3.5) | 5 (1.2) |
| Grade IVA n (%) | 1 (0.07) | 0 | 1 (0.3) | 0 | 0 |
| N | % | |
|---|---|---|
| Vaginal mesh exposure | 6 | 0.44 |
| Bladder injury | 6 | 0.44 |
| Urinary retention | 5 | 0.37 |
| Ureteral obstruction | 4 | 0.29 |
| Delayed wound of healing or granuloma | 3 | 0.22 |
| Hematoma | 2 | 0.15 |
| Vaginal suture bleeding | 2 | 0.15 |
| Thigh pain | 2 | 0.15 |
| Bladder clot removal | 1 | 0.07 |
| Unadjusted HR [95% CI] | p-Value | Adjusted by IPTW HR [95% CI] | p-Value | |
|---|---|---|---|---|
| Complication risk | ||||
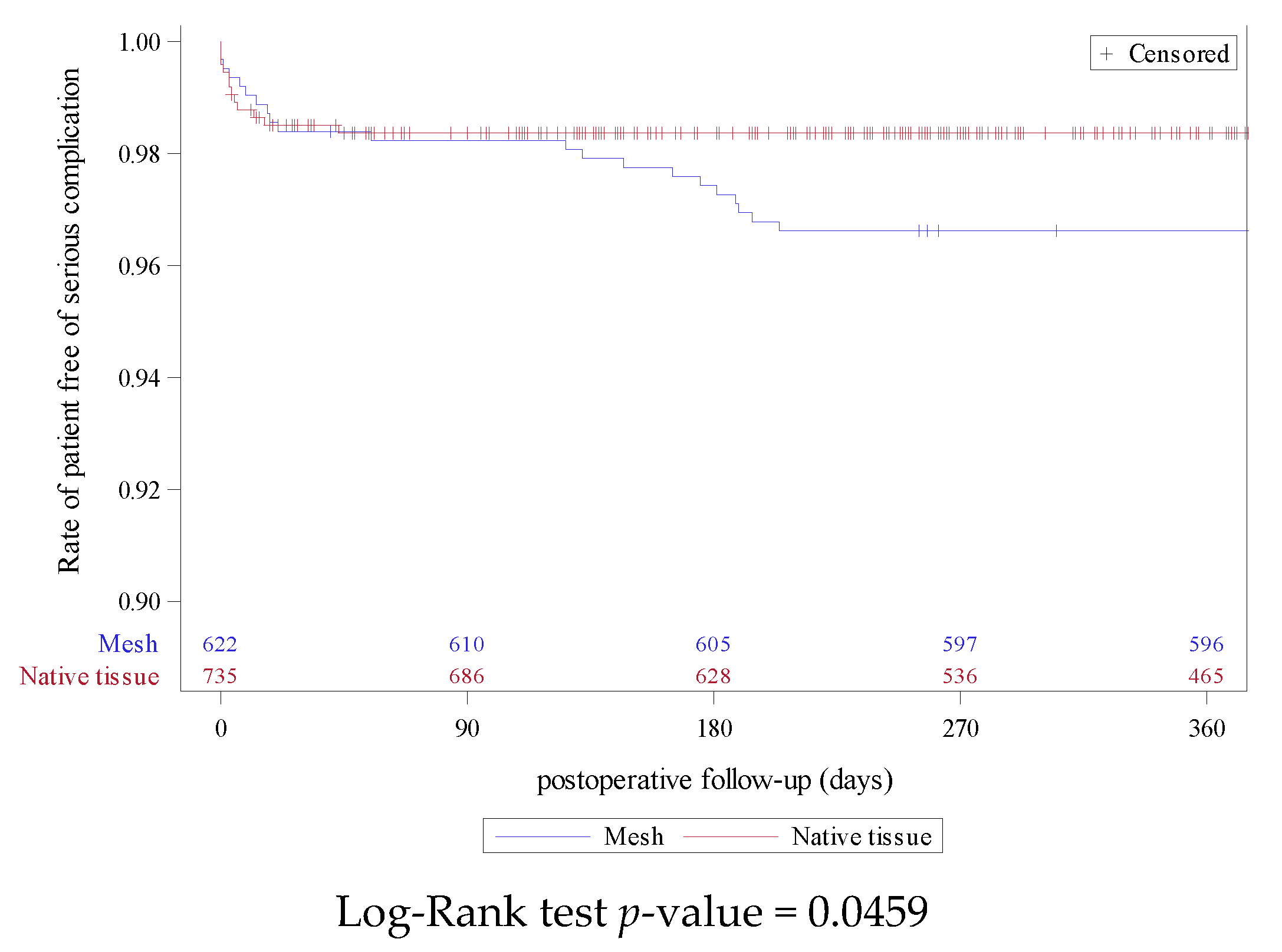
| Mesh vs. Native tissue | 2.12 [1.05; 4.26] | 0.0359 | 1.26 [0.73; 2.17] | 0.4001 |
| Ant. SSLF vs. Post. SSLF | 2 [0.88; 4.59] | 0.1004 | 1.43 [0.88; 2.33] | 0.1511 |
| Recurrence risk | ||||
| Mesh vs. Native tissue | 0.5 [0.27; 0.9] | 0.0206 | 0.42 [0.26; 0.68] | 0.0004 |
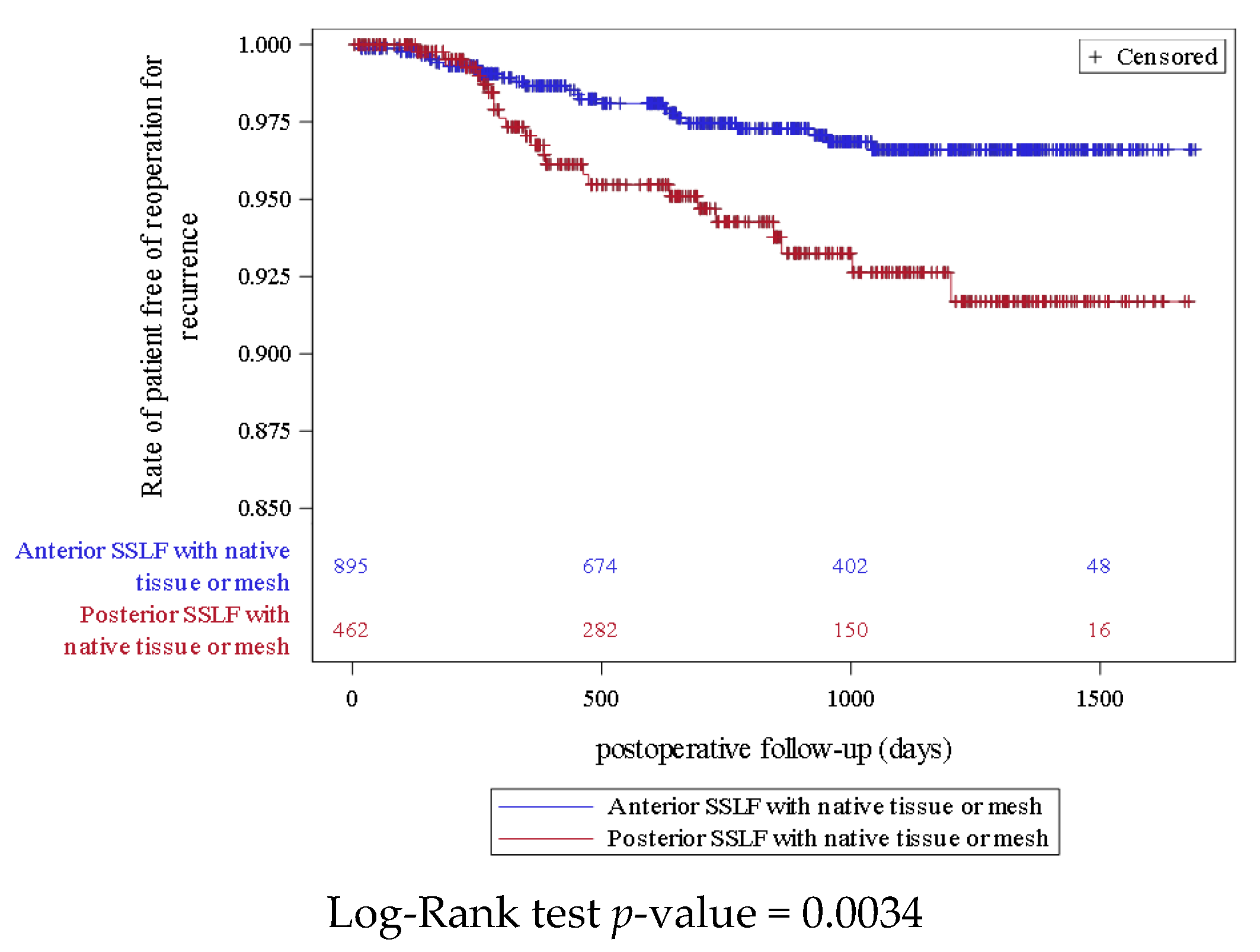
| Ant. SSLF vs. Post. SSLF | 0.43 [0.24; 0.77] | 0.0044 | 0.67 [0.46; 0.99] | 0.043 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Gracia, S.; Fatton, B.; Cosson, M.; Campagne-Loiseau, S.; Ferry, P.; Lucot, J.-P.; Debodinance, P.; Panel, L.; Deffieux, X.; Garbin, O.; et al. Serious Complications and Recurrence following Sacrospinous Ligament Fixation for the Correction of Apical Prolapse. J. Clin. Med. 2023, 12, 468. https://doi.org/10.3390/jcm12020468
De Gracia S, Fatton B, Cosson M, Campagne-Loiseau S, Ferry P, Lucot J-P, Debodinance P, Panel L, Deffieux X, Garbin O, et al. Serious Complications and Recurrence following Sacrospinous Ligament Fixation for the Correction of Apical Prolapse. Journal of Clinical Medicine. 2023; 12(2):468. https://doi.org/10.3390/jcm12020468
Chicago/Turabian StyleDe Gracia, Susie, Brigitte Fatton, Michel Cosson, Sandrine Campagne-Loiseau, Philippe Ferry, Jean-Philippe Lucot, Philippe Debodinance, Laure Panel, Xavier Deffieux, Olivier Garbin, and et al. 2023. "Serious Complications and Recurrence following Sacrospinous Ligament Fixation for the Correction of Apical Prolapse" Journal of Clinical Medicine 12, no. 2: 468. https://doi.org/10.3390/jcm12020468
APA StyleDe Gracia, S., Fatton, B., Cosson, M., Campagne-Loiseau, S., Ferry, P., Lucot, J.-P., Debodinance, P., Panel, L., Deffieux, X., Garbin, O., Lamblin, G., Carlier-Guérin, C., Ramanah, R., Fauconnier, A., Serrand, C., Fritel, X., & de Tayrac, R. (2023). Serious Complications and Recurrence following Sacrospinous Ligament Fixation for the Correction of Apical Prolapse. Journal of Clinical Medicine, 12(2), 468. https://doi.org/10.3390/jcm12020468