

Predictive Factors and Management of Macular Edema after Retropupillary Iris-Claw Intraocular Lens Implantation in Aphakia: National Multicenter Audit—Report 2

 , , ,
on behalf of the Spanish Multicenter Iris-Claw IOL Study Group
, , ,
on behalf of the Spanish Multicenter Iris-Claw IOL Study Group
Abstract
1. Introduction
2. Materials and Methods
3. Results
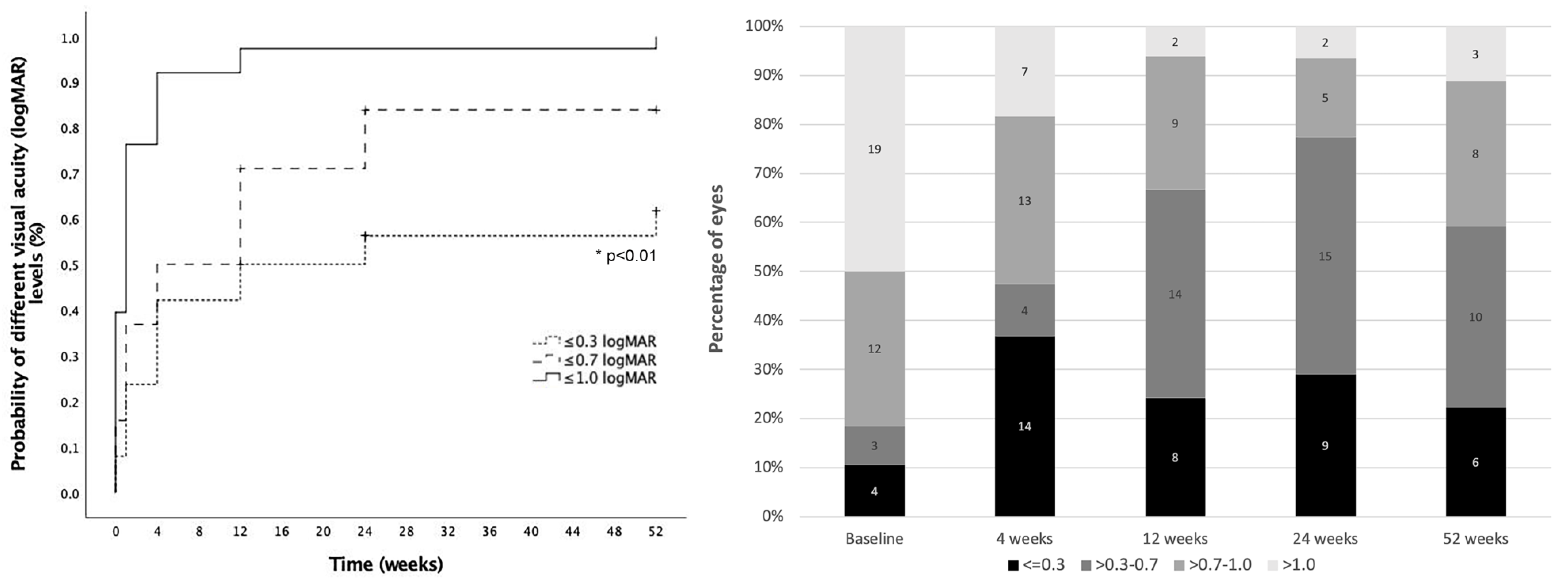
3.1. Macular Edema Development and Visual Outcomes
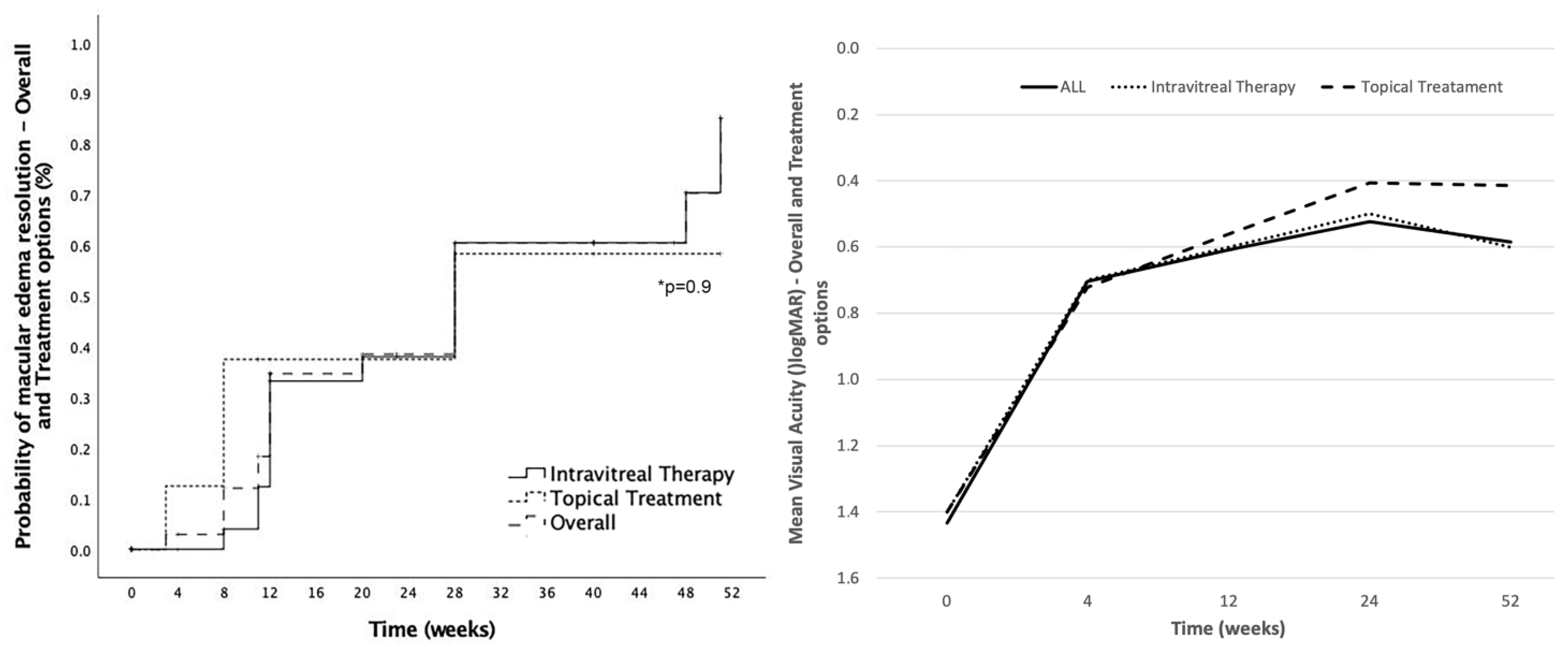
3.2. Management of Macular Edema
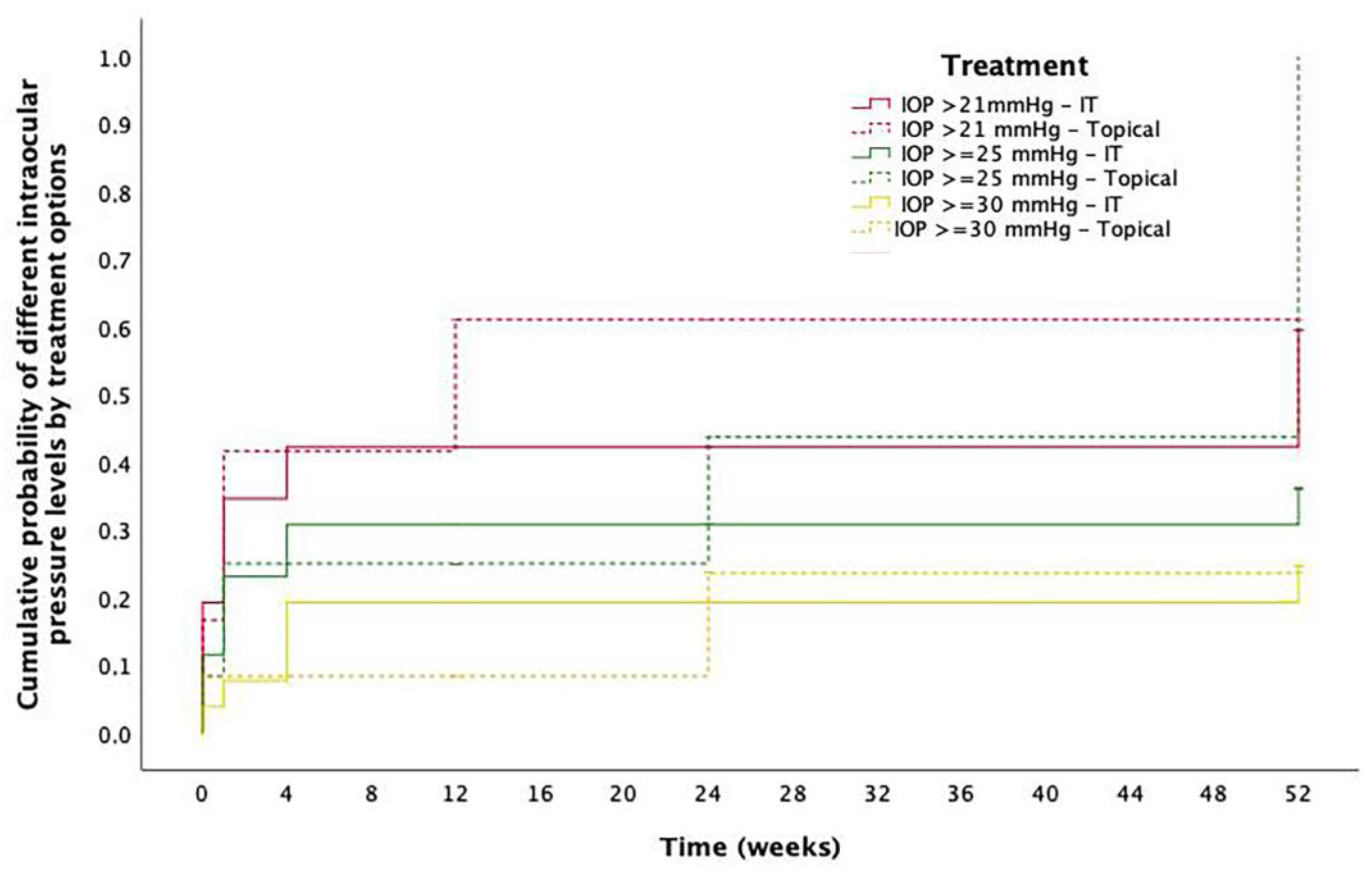
3.3. Other Complications
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Spanish Multicenter Iris-Claw IOL Study Group (Sorted by Participant Centers, Principal Investigator and in Alphabetical Order)
- Hospital Clínic de Barcelona, Barcelona (Coordinating center): Javier Zarranz-Ventura, Alfredo Adán, Carolina Bernal-Morales, Manuel J. Navarro-Angulo
- Althaia Xarxa Assistencial Universitària de Manresa: Eduard Pedemonte-Sarrias, Fátima Sánchez-Aparicio
- Hospital Clínico San Carlos, Madrid: Alicia Valverde
- Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain: Javier Ascaso, Olivia Esteban
- Hospital Donostia, San Sebastián: Cristina Irigoyen, Luis Ansa, Leire Juaristi, Miguel Ruiz-Miguel
- Hospital La Arruzafa, Córdoba: Juan Manuel Cubero-Parra, Juan Manuel Laborda, Consuelo Spínola-Muñoz
- Hospital Povisa, Vigo: Daniel Velazquez-Villoria
- Hospital Universitario de Basurto, Bilbao: Estibaliz Ispizua-Mendivil, M. Paz Mendivil-Soto
- Hospital Universitario Mútua Terrassa, Terrassa: Marina Barraso-Rodrigo, Sophia Bennis
- Hospital Universitario Ramon y Cajal, Madrid: Diego Ruiz-Casas, Marta Gómez-Mariscal, Julio José González-López
- Hospital Universitario Valme, Sevilla: Adrián Hernández-Martínez
- Hospital Universitario Virgen Macarena, Sevilla: Isabel Relimpio, Enrique Rodríguez-de-la-Rua, Ainhoa Roselló
- Hospital Universitario Virgen del Rocío, Sevilla: Mariano Rodriguez-Maqueda, José Luis Sánchez-Vicente, Amparo Toro-Fernández, Lorenzo Trujillo-Berraquero
- Instituto Oftalmológico La Esperanza, HM La Esperanza, Santiago de Compostela & Servicio de Oftalmología, Complejo Hospitalario Universitario, A Coruña: Joaquín Marticorena
References
- Kristianslund, O.; Råen, M.; Østern, A.E.; Drolsum, L. Late In-the-Bag Intraocular Lens Dislocation: A Randomized Clinical Trial Comparing Lens Repositioning and Lens Exchange. Ophthalmology 2017, 124, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Choragiewicz, T.; Rejdak, R.; Grzybowski, A.; Nowomiejska, K.; Moneta-Wielgoś, J.; Ozimek, M.; Jünemann, A.G.M. Outcomes of Sutureless Iris-Claw Lens Implantation. J. Ophthalmol. 2016, 2016, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Forlini, M.; Soliman, W.; Bratu, A.; Rossini, P.; Cavallini, G.M.; Forlini, C. Long-term follow-up of retropupillary iris-claw intraocular lens implantation: A retrospective analysis. BMC Ophthalmol. 2015, 15, 143. [Google Scholar] [CrossRef] [PubMed]
- Bernal-Morales, C.; Hernández-Martínez, A.; Navarro-Angulo, M.J.; Ruiz-Miguel, M.; Rodriguez-Maqueda, M.; Velazquez-Villoria, D.; Cubero-Parra, J.M.; Marticorena, J.; Ruiz-Casas, D.; Adan, A.; et al. Retropupillary Iris-Claw Intraocular Lens and Pars Plana Vitrectomy in Aphakia Management. Retina 2021, 41, 2048–2058. [Google Scholar] [CrossRef]
- Gonnermann, J.; Klamann, M.K.J.; Maier, A.; Rjasanow, J.; Joussen, A.M.; Bertelmann, E.; Rieck, P.W.; Torun, N. Visual outcome and complications after posterior iris-claw aphakic intraocular lens implantation. J. Cart. Refract. Surg. 2012, 38, 2139–2143. [Google Scholar] [CrossRef]
- Jayamadhury, G.; Potti, S.; Kumar, K.V.; Kumar, R.; Divyansh Mishra, K.; Nambula, S. Retropupillary fixation of iris-claw lens in visual rehabilitation of aphakic eyes. Indian J. Ophthalmol. 2016, 64, 743–746. [Google Scholar] [CrossRef]
- Mora, P.; Calzetti, G.; Favilla, S.; Forlini, M.; Tedesco, S.; Date, P.; Tagliavini, V.; Carta, A.; Frisina, R.; Pedrotti, E.; et al. Comparative Analysis of the Safety and Functional Outcomes of Anterior versus Retropupillary Iris-Claw IOL Fixation. J. Ophthalmol. 2018, 2018, 1–8. [Google Scholar] [CrossRef]
- Scott, I.U.; Flynn, H.W.; Smiddy, W.E.; Murray, T.G.; Moore, J.K.; Lemus, D.R.; Feuer, W.J. Clinical features and outcomes of pars plana vitrectomy in patients with retained lens fragments. Ophthalmology 2003, 110, 1567–1572. [Google Scholar] [CrossRef]
- Bellocq, D.; Mathis, T.; Voirin, N.; Bentaleb, Z.M.; Sallit, R.; Denis, P.; Kodjikian, L. Incidence of Irvine Gass Syndrome after Phacoemulsification with Spectral-Domain Optical Coherence Tomography. Ocul. Immunol. Inflamm. 2019, 27, 1224–1231. [Google Scholar] [CrossRef]
- Chatziralli, I.; Theodossiadis, G.; Dimitriou, E.; Kazantzis, D.; Theodossiadis, P. Macular Edema after Successful Pars Plana Vitrectomy for Rhegmatogenous Retinal Detachment: Factors Affecting Edema Development and Considerations for Treatment. Ocul. Immunol. Inflamm. 2019, 00, 1–6. [Google Scholar] [CrossRef]
- Alam, M.R.; Arcinue, C.A.; Mendoza, N.B.; Freeman, W.R. Recalcitrant cystoid macular edema after pars plana vitrectomy. Retina 2016, 36, 1244–1251. [Google Scholar] [CrossRef]
- Nelson, M.L.; Martidis, A. Managing cystoid macular edema after cataract surgery. Curr. Opin. Ophthalmol. 2003, 14, 39–43. [Google Scholar] [CrossRef]
- Packer, M.; Lowe, J.; Fine, H. Incidence of acute postoperative cystoid macular edema in clinical practice. J. Cataract Refract. Surg. 2012, 38, 2108–2111. [Google Scholar] [CrossRef]
- Kim, S.J.; Martin, D.F.; Hubbard, G.B.; Srivastava, S.K.; Yan, J.; Bergstrom, C.S.; Aaberg, T.M. Incidence of Postvitrectomy Macular Edema Using Optical Coherence Tomography. Ophthalmology 2009, 116, 1531–1537. [Google Scholar] [CrossRef] [PubMed]
- Bellocq, D.; Korobelnik, J.F.; Burillon, C.; Voirin, N.; Dot, C.; Souied, E.; Conrath, J.; Milazzo, S.; Massin, P.; Baillif, S.; et al. Effectiveness and safety of dexamethasone implants for post-surgical macular oedema including Irvine-Gass syndrome: The EPISODIC study. Br. J. Ophthalmol. 2015, 99, 979–983. [Google Scholar] [CrossRef]
- Bellocq, D.; Pierre-Kahn, V.; Matonti, F.; Burillon, C.; Voirin, N.; Dot, C.; Akesbi, J.; Milazzo, S.; Baillif, S.; Soler, V.; et al. Effectiveness and safety of dexamethasone implants for postsurgical macular oedema including Irvine-Gass syndrome: The EPISODIC-2 study. Br. J. Ophthalmol. 2017, 101, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Benhamou, N.; Massin, P.; Haouchine, B.; Audren, F.; Tadayoni, R.; Gaudric, A. Intravitreal triamcinolone for refractory pseudophakic macular edema. Am. J. Ophthalmol. 2003, 135, 246–249. [Google Scholar] [CrossRef]
- Thach, A.B.; Dugel, P.U.; Flindall, R.J.; Sipperley, J.O.; Sneed, S.R. A comparison of retrobulbar versus sub-Tenon’s corticosteroid therapy for cystoid macular edema refractory to topical medications. Ophthalmology 1997, 104, 2003–2008. [Google Scholar] [CrossRef]
- Williams, G.A.; Haller, J.A.; Kuppermann, B.D.; Blumenkranz, M.S.; Weinberg, D.V.; Chou, C.; Whitcup, S.M. Dexamethasone Posterior-Segment Drug Delivery System in the Treatment of Macular Edema Resulting from Uveitis or Irvine-Gass Syndrome. Am. J. Ophthalmol. 2009, 147, 1048–1054.e2. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Russo, V.; Prascina, F.; Noci, N.D. Short-term safety and efficacy of intravitreal bevacizumab for pseudophakic cystoid macular EDEMA. Retina 2009, 29, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Mansoori, T.; Agraharam, S.G.; Sannapuri, S.; Manwani, S.; Balakrishna, N. Surgical outcomes of retropupillary-fixated iris-claw intraocular lens. J. Curr. Ophthalmol. 2020, 32, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Hernández Martínez, A.; Almeida González, C.V. Iris-claw intraocular lens implantation: Efficiency and safety according to technique. J. Cataract Refract. Surg. 2018, 44, 1186–1191. [Google Scholar] [CrossRef] [PubMed]
- Han, J.V.; Patel, D.V.; Squirrell, D.; McGhee, C.N.J. Cystoid macular oedema following cataract surgery: A review. Clin. Exp. Ophthalmol. 2019, 47, 346–356. [Google Scholar] [CrossRef]
- Munk, M.R.; Jampol, L.M.; Simader, C.; Huf, W.; Mittermüller, T.J.; Jaffe, G.J.; Schmidt-Erfurth, U. Differentiation of diabetic macular edema from pseudophakic cystoid macular edema by spectral-domain optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2015, 56, 6724–6733. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, D.R.; Dellaporta, A. Natural history of cystoid macular edema after cataract extraction. Am. J. Ophthalmol. 1974, 77, 445–447. [Google Scholar] [CrossRef]
- Sivaprasad, S.; Bunce, C.; Crosby-Nwaobi, R. Non-steroidal anti-inflammatory agents for treating cystoid macular oedema following cataract surgery. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef] [PubMed]
- Akay, F.; Isuk, M.U.; Akmaz, B.; Güven, Y.Z. Comparison of intravitreal anti-vascular endothelial growth factor agents and treatment results in Irvine-Gass syndrome. Int. J. Ophthalmol. 2020, 13, 1586–1591. [Google Scholar] [CrossRef]
- Sharma, A.; Bandello, F.; Loewenstein, A.; Kuppermann, B.D.; Lanzetta, P.; Zur, D.; Hilely, A.; Iglicki, M.; Veritti, D.; Wang, A.; et al. Current role of intravitreal injections in Irvine Gass syndrome-CRIIG study. Int. Ophthalmol. 2020, 40, 3067–3075. [Google Scholar] [CrossRef]
- Mitropoulos, P.G.; Chatziralli, I.P.; Peponis, V.G.; Drakos, E.; Parikakis, E.A. Intravitreal ranibizumab for the treatment of Irvine-Gass syndrome. Ocul. Immunol. Inflamm. 2015, 23, 225–231. [Google Scholar] [CrossRef]
- Medeiros, M.D.; Navarro, R.; Garcia-Arumí, J.; Mateo, C.; Corcóstegui, B. Dexamethasone intravitreal implant for treatment of patients with recalcitrant macular edema resulting from Irvine-Gass syndrome. Investig. Ophthalmol. Vis. Sci. 2013, 54, 3320–3324. [Google Scholar] [CrossRef] [PubMed]
- Mayer, W.J.; Kurz, S.; Wolf, A.; Kook, D.; Kreutzer, T.; Kampik, A.; Priglinger, S.; Haritoglou, C. Dexamethasone implant as an effective treatment option for macular edema due to Irvine-Gass syndrome Presented at the XXIX Club Gonin Meeting, Zurich, Switzerland, September 2014. J. Cataract Refract. Surg. 2015, 41, 1954–1961. [Google Scholar] [CrossRef] [PubMed]
- Klamann, A.; Böttcher, K.; Ackermann, P.; Geerling, G.; Schargus, M.; Guthoff, R. Intravitreal Dexamethasone Implant for the Treatment of Postoperative Macular Edema. Ophthalmologica 2017, 236, 181–185. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Chen, P.Y.; Chen, F.T.; Chen, Y.J.; Wang, J.K. Comparison of efficacy of intravitreal ranibizumab between non-vitrectomized and vitrectomized eyes with diabetic macular edema. Int. Ophthalmol. 2018, 38, 293–299. [Google Scholar] [CrossRef]
- Gonçalves, M.B.; de Queiroz Alves, B.; Moura, R.; Magalhães, O.; Maia, A.; Belfort, R.; de Ávila, M.P.; Zas, M.; Saravia, M.; Lousas, M.; et al. INTRAVITREAL DEXAMETHASONE IMPLANT MIGRATION INTO THE ANTERIOR CHAMBER: A Multicenter Study From the Pan-American Collaborative Retina Study Group. Retina 2020, 40, 825–832. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Eyes with Postoperative Macular Edema | Eyes without Postoperative Macular Edema | |||||||
|---|---|---|---|---|---|---|---|---|
| Total | Complicated Cataract Surgery | IOL Luxation | p-Value | Total | Complicated Cataract Surgery | IOL Luxation | p-Value | |
| 38 eyes | 57.9% (22/38) | 42.1% (16/38) | - | 260 eyes | 39.6% (103/260) | 60.4% (157/260) | ||
| Gender (Male %) | 68.4 (26/38) | 72.7 (16/22) | 62.5 (10/16) | 0.51 | 56.1 (146/260) | 49.5 (51/103) | 60.5 (95/157) | 0.08 |
| Age (years) | 0.17 | 0.28 | ||||||
| (Mean ± SD) | 73.3 ± 11.8 | 74.1 ± 10.9 | 79.0 ± 11.6 | 73.1 ± 1.2 | 74.0 ± 13.7 | 72.1 ± 15.4 | ||
| (Median; IQR) | 76.0; 9.5 | 78.0; 12 | 82; 7.5 | 76; 16 | 77.5; 12.7 | 76; 16 | ||
| Preoperative VA (logMAR) | 1.4 ± 0.8 | 1.7 ± 0.7 | 1.2 ± 0.8 | 0.06 | 1.19 ± 0.7 | 1.3 ± 1.3 | 1.1 ± 0.7 | 0.02 |
| 1.4; 1.0 | 1.8; 1 | 1.0; 1.3 | 1; 1.3 | 1.3;1.5 | 1; 1.3 | |||
| Preoperative IOP (mmHg) | 17.4 ± 7.4 | 16.8 ± 5.0 | 18.2 ± 10.3 | 0.60 | 17.5 ± 6.9 | 16.7 ± 1.3 | 17.9 ± 6.7 | 0.21 |
| 16; 7.5 | 16; 6 | 16.0; 8 | 16; 6 | 16; 5 | 16; 6 | |||
| Axial length (mm) | 23.9 ± 2.1 | 24.0 ± 2.4 23.3; 1.5 | 23.6 ± 1.4 23.1; 1.3 | 0.71 | 24.0 ± 2.0 23.6; 2.4 | 23.1 ± 1 0.3 22.9; 1.4 | 24.5 ± 2.2 24.1; 2.6 | <0.01 |
| Diabetes mellitus (%) | 18.4 (7/38) | 18.2 (4/22) | 18.7 (3/16) | 0.89 | 14.2 (37/260) | 16.5 (17/103) | 12.7 (20/157) | 0.34 |
| Diabetic retinopathy (%) | 18.4 (7/38) | 18.2 (4/22) | 18.7 (3/16) | 6.9 (18/260) | 9.7 (10/103) | 5.1 (8/157) | ||
| -Non-proliferative: | ||||||||
| -Mild (%) | 42.8 (3/7) | 50 (2/4) | 33.3 (1/3) | 77.8 (14/18) | 80 (8/10) | 75 (6/8) | ||
| -Moderate (%) | 28.6 (2/7) | 25 (1/4) | 33.3 (1/3) | 22.2 (4/18) | 20 (2/10) | 25 (2/8) | ||
| -Severe (%) | 0 (0/7) | - | - | 0 (0/18) | 0 (0/10) | 0 (0/8) | ||
| -Proliferative (%) | 28.6 (2/7) | 25 (1/4) | 33.3 (1/3) | 0 (0/18) | 0 (0/10) | 0 (0/8) | ||
| Central Retinal Thickness (μm) | 0.74 | 0.90 | ||||||
| (Mean ± SD) | 273.4 ± 58.0 | 276.27 ± 65.8 | 263.0 ± 6.1 | 241.0 ± 65.5 | 242.2 ± 1.3 | 240.2 ± 78.5 | ||
| (Median; IQR) | 263.5; 58.5 | 267; 87 | 260; 5.5 | 249; 40 | 248; 35 | 251; 43.7 | ||
| Pseudoexfoliation (%) | 21.0 (8/38) | 18.2 (4/22) | 25 (4/16) | 0.67 | 28.5 (74/260) | 26.2 (27/103) | 29.9 (47/157) | 0.47 |
| Glaucoma (%) | 21.0 (8/38) | 27.3 (6/22) | 12.5 (2/16) | 0.26 | 20 (52/260) | 17.5 (18/103) | 21.6 (34/157) | 0.42 |
| High Myopia (%) | 5.3 (2/38) | 4.5 (1/22) | 6.2 (1/16) | 0.82 | 12.7 (33/260) | 5.8 (6/103) | 17.2 (27/157) | <0.01 |
| Uveitis (%) | 2.6 (1/38) | 4.5 (1/22) | - | - | 3.5 (9/260) | 4.8 (5/103) | 2.5 (4/157) | 0.28 |
| Branch Retinal Vein Occlusion (%) | 2.6 (1/38) | 4.5 (1/22) | - | - | 0.8 (2/260) | 0.9 (1/103) | 0.6 (1/157) | 0.76 |
| Postoperative Macular Edema (n = 38) (%) | No Postoperative Macular Edema (n = 260) (%) | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|---|
| p-Value | OR | 95% CI | p-Value | OR | 95% CI | |||
| Complicated cataract surgery | 57.9 (22/38) | 37.7 (100/260) | 0.02 | 2.27 | 1.38–4.52 | 0.04 | 2.03 | 1.01–4.18 |
| Pseudoexfoliation | 21.1 (8/38) | 29.1 (77/260) | 0.30 | 0.65 | 0.29–1.48 | 0.29 | 0.61 | 0.24–1.53 |
| Diabetes Mellitus | 18.4 (7/38) | 14.3 (38/260) | 0.51 | 1.35 | 0.55–3.28 | 0.52 | 1.35 | 0.54–3.39 |
| Glaucoma | 21.6 (8/38) | 20.3 (53/260) | 0.85 | 1.08 | 0.47–2.51 | 0.75 | 1.16 | 0.47–2.87 |
| High myopia | 5.3 (2/38) | 14.3 (38/260) | 0.12 | 0.33 | 0.08–1.44 | 0.22 | 0.39 | 0.09–1.74 |
| Uveitis | 2.6 (1/38) | 3.8 (9/260) | 0.72 | 0.69 | 0.08–5.59 | 0.65 | 0.60 | 0.07–5.12 |
| Treatment | Total | Dexamethasone | Anti-VEGF | Mixed Treatment | Topical Treatment | |
|---|---|---|---|---|---|---|
| Number of patients | 38 | 50% (19/38) | 7.9% (3/38) | 10.5% (4/38) | 31.6% (12/38) | |
| Number of intravitreal injections per patient | 1 injection | 57.9% (11/19) | 33.3% (1/3) | 1 Anti-VEGF + 1 DEX implant | 75% (3/4) | NSAIDs new |
| 2 injections | 36.8% (7/19) | 66.6%% (2/3) | - | NSAIDs classic | ||
| 3 injections | 5.3% (1/19) | - | 1 Anti-VEGF + 2 DEX implants | 25% (1/4) | Topical steroids | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernal-Morales, C.; Navarro-Angulo, M.J.; Rodriguez-Maqueda, M.; Velazquez-Villoria, D.; Cubero-Parra, J.M.; Marticorena, J.; Hernández-Martínez, A.; Ruiz-Miguel, M.; Adan, A.; Ruiz-Casas, D.; et al. Predictive Factors and Management of Macular Edema after Retropupillary Iris-Claw Intraocular Lens Implantation in Aphakia: National Multicenter Audit—Report 2. J. Clin. Med. 2023, 12, 436. https://doi.org/10.3390/jcm12020436
Bernal-Morales C, Navarro-Angulo MJ, Rodriguez-Maqueda M, Velazquez-Villoria D, Cubero-Parra JM, Marticorena J, Hernández-Martínez A, Ruiz-Miguel M, Adan A, Ruiz-Casas D, et al. Predictive Factors and Management of Macular Edema after Retropupillary Iris-Claw Intraocular Lens Implantation in Aphakia: National Multicenter Audit—Report 2. Journal of Clinical Medicine. 2023; 12(2):436. https://doi.org/10.3390/jcm12020436
Chicago/Turabian StyleBernal-Morales, Carolina, Manuel Javier Navarro-Angulo, Mariano Rodriguez-Maqueda, Daniel Velazquez-Villoria, Juan Manuel Cubero-Parra, Joaquín Marticorena, Adrián Hernández-Martínez, Miguel Ruiz-Miguel, Alfredo Adan, Diego Ruiz-Casas, and et al. 2023. "Predictive Factors and Management of Macular Edema after Retropupillary Iris-Claw Intraocular Lens Implantation in Aphakia: National Multicenter Audit—Report 2" Journal of Clinical Medicine 12, no. 2: 436. https://doi.org/10.3390/jcm12020436
APA StyleBernal-Morales, C., Navarro-Angulo, M. J., Rodriguez-Maqueda, M., Velazquez-Villoria, D., Cubero-Parra, J. M., Marticorena, J., Hernández-Martínez, A., Ruiz-Miguel, M., Adan, A., Ruiz-Casas, D., & Zarranz-Ventura, J., on behalf of the Spanish Multicenter Iris-Claw IOL Study Group. (2023). Predictive Factors and Management of Macular Edema after Retropupillary Iris-Claw Intraocular Lens Implantation in Aphakia: National Multicenter Audit—Report 2. Journal of Clinical Medicine, 12(2), 436. https://doi.org/10.3390/jcm12020436