Clinicohistological Characteristics of Patients with Oral Lichenoid Mucositis: A Retrospective Study for Dental Hospital Records


Abstract
:1. Introduction
2. Methods
Statistical Analysis and Data Management
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| MT | malignant transformation |
| OLL | oral lichenoid reaction |
| OLM | oral lichenoid mucositis |
| OLP | oral lichen planus |
| OSCC | oral squamous cell carcinoma |
References
- Cheng, Y.-S.L.; Gould, A.; Kurago, Z.; Fantasia, J.; Muller, S. Diagnosis of Oral Lichen Planus: A Position Paper of the American Academy of Oral and Maxillofacial Pathology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 332–354. [Google Scholar] [PubMed]
- Li, C.; Tang, X.; Zheng, X.; Ge, S.; Wen, H.; Lin, X.; Lu, L. Global Prevalence and Incidence Estimates of Oral Lichen Planus: A Systematic Review and Meta-Analysis. JAMA Dermatol. 2020, 156, 172–181. [Google Scholar] [PubMed]
- Ismail, S.B.; Kumar, S.K.; Zain, R.B. Oral Lichen Planus and Lichenoid Reactions: Etiopathogenesis, Diagnosis, Management and Malignant Transformation. J. Oral Sci. 2007, 49, 89–106. [Google Scholar]
- Xue, J.L.; Fan, M.W.; Wang, S.Z.; Chen, X.M.; Li, Y.; Wang, L. A Clinical Study of 674 Patients with Oral Lichen Planus in China. J. Oral Pathol. Med. 2005, 34, 467–472. [Google Scholar] [CrossRef]
- Halawani, M. Hepatitis C Virus Genotypes among Patients with Lichen Planus in the Kingdom of Saudi Arabia. Int. J. Dermatol. 2014, 53, 171–177. [Google Scholar] [CrossRef]
- Adamo, D.; Calabria, E.; Coppola, N.; Lo Muzio, L.; Giuliani, M.; Bizzoca, M.E.; SIPMO. Psychological Profile and Unexpected Pain in Oral Lichen Planus: A Case–Control Multicenter Sipmo Studya. Oral Dis. 2022, 28, 398–414. [Google Scholar] [CrossRef]
- Aguirre-Urizar, J.M.; Alberdi-Navarro, J.; de Mendoza, I.L.I.; Marichalar-Mendia, X.; Martínez-Revilla, B.; Parra-Pérez, C.; Echebarria-Goicouria, M.Á. Clinicopathological and Prognostic Characterization of Oral Lichenoid Disease and Its Main Subtypes: A Series of 384 Cases. Med. Oral Patol. Oral Cir. Bucal. 2020, 25, e554. [Google Scholar]
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, Á.; Kerr, A.R.; Johnson, N.W. Oral Potentially Malignant Disorders: A Consensus Report from an International Seminar on Nomenclature and Classification, Convened by the Who Collaborating Centre for Oral Cancer. Oral Dis. 2021, 27, 1862–1880. [Google Scholar] [PubMed]
- Van Der Meij, E.H.; Van Der Waal, I. Lack of Clinicopathologic Correlation in the Diagnosis of Oral Lichen Planus Based on the Presently Available Diagnostic Criteria and Suggestions for Modifications. J. Oral Pathol. Med. 2003, 32, 507–512. [Google Scholar]
- Aghbari, S.M.H.; Abushouk, A.I.; Attia, A.; Elmaraezy, A.; Menshawy, A.; Ahmed, M.S.; Elsaadany, B.A.; Ahmed, E.M. Malignant Transformation of Oral Lichen Planus and Oral Lichenoid Lesions: A Meta-Analysis of 20095 Patient Data. Oral Oncol. 2017, 68, 92–102. [Google Scholar]
- Müller, S. Oral Lichenoid Lesions: Distinguishing the Benign from the Deadly. Mod. Pathol. 2017, 30, S54–S67. [Google Scholar] [CrossRef]
- Fitzpatrick, S.G.; Honda, K.S.; Sattar, A.; Hirsch, S.A. Histologic Lichenoid Features in Oral Dysplasia and Squamous Cell Carcinoma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 511–520. [Google Scholar] [CrossRef]
- Schlosser, B.J. Lichen Planus and Lichenoid Reactions of the Oral Mucosa. Dermatol. Ther. 2010, 23, 251–267. [Google Scholar]
- Rock, L.; Laronde, D.; Lin, I.; Rosin, M.; Chan, B.; Shariati, B.; Zhang, L. Dysplasia Should Not Be Ignored in Lichenoid Mucositis. J. Dent. Res. 2018, 97, 767–772. [Google Scholar] [CrossRef]
- Lin, I.; Laronde, D.M.; Zhang, L.; Rosin, M.P.; Yim, I.; Rock, L.D. Basement Membrane Degeneration Is Common in Lichenoid Mucositis with Dysplasia. Can. J. Dent. Hyg. 2021, 55, 9. [Google Scholar]
- Alves, M.G.O.; Almeida, J.D.; Balducci, I.; Cabral, L.A.G. Oral Lichen Planus: A Retrospective Study of 110 Brazilian Patients. BMC Res. Notes 2010, 3, 157. [Google Scholar]
- Radochová, V.; Dřízhal, I.; Slezák, R.A. Retrospective Study of 171 Patients with Oral Lichen Planus in the East Bohemia-Czech Republic–Single Center Experience. J. Clin. Exp. Dent. 2014, 6, e556. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Fenoll, A.; Sánchez-Siles, M.; López-Jornet, P.; Camacho-Alonso, F.; Salazar-Sánchez, N. A Retrospective Clinicopathological Study of 550 Patients with Oral Lichen Planus in South-Eastern Spain. J. Oral Pathol. Med. 2010, 39, 491–496. [Google Scholar] [CrossRef]
- Thongprasom, K.; Youngnak-Piboonratanakit, P.; Pongsiriwet, S.; Laothumthut, T.; Kanjanabud, P.; Rutchakitprakarn, L. A Multicenter Study of Oral Lichen Planus in Thai Patients. J. Investig. Clin. Dent. 2010, 1, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Ingafou, M.; Leao, J.; Porter, S.; Scully, C. Oral Lichen Planus: A Retrospective Study of 690 British Patients. Oral Dis. 2006, 12, 463–468. [Google Scholar] [CrossRef] [PubMed]
- Salem, G. Oral Lichen Planus among 4277 Patients from Gizan, Saudi Arabia. Community Dent. Oral Epidemiol. 1989, 17, 322–324. [Google Scholar] [CrossRef]
- Almazrooa, S.; Alhelo, A.F.; Mansour, G.; Alhamed, S.; Alfarabi, S.; Akeel, S.K.; Alhindi, N.; Alsulaimani, L.; Alamri, M.; Mawardi, H.H.; et al. Characterization of Oral Lichen Planus in a Subset of Patients: A Single-Center Experience. Saudi J. Oral Sci. 2020, 7, 199–205. [Google Scholar] [CrossRef]
- Casparis, S.; Borm, J.M.; Tektas, S.; Kamarachev, J.; Locher, M.C.; Damerau, G.; Stadlinger, B. Oral Lichen Planus (Olp), Oral Lichenoid Lesions (Oll), Oral Dysplasia, and Oral Cancer: Retrospective Analysis of Clinicopathological Data from 2002–2011. Oral Maxillofac. Surg. 2015, 19, 149–156. [Google Scholar] [CrossRef]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- González-Moles, M.Á.; Ramos-García, P. Oral Lichen Planus and Related Lesions. What Should We Accept Based on the Available Evidence? Oral Dis. 2022, 29, 2624–2637. [Google Scholar] [CrossRef]
- The World Bank. World Development Indicators: Population Dynamics; World Bank Group: Washington, DC, USA, 2015. [Google Scholar]
- Cascone, M.; Celentano, A.; Adamo, D.; Leuci, S.; Ruoppo, E.; Mignogna, M.D. Oral Lichen Planus in Childhood: A Case Series. Int. J. Dermatol. 2017, 56, 641–652. [Google Scholar] [CrossRef]
- Merhy, R.; Sarkis, A.; Assaf, J.; Afiouni, R.; Zeinaty, P.; Kechichian, E.; Tomb, R.; Helou, J. Pediatric Lichen Planus: A Systematic Review of 985 Published Cases. Int. J. Dermatol. 2022, 61, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Otero Rey, E.M.; Yáñez-Busto, A.; Rosa Henriques, I.F.; López-López, J.; Blanco-Carrión, A. Lichen Planus and Diabetes Mellitus: Systematic Review and Meta-Analysis. Oral Dis. 2019, 25, 1253–1264. [Google Scholar] [CrossRef] [PubMed]
- Al-Hashimi, I.; Schifter, M.; Lockhart, P.B.; Wray, D.; Brennan, M.; Migliorati, C.A.; van der Waal, I. Oral Lichen Planus and Oral Lichenoid Lesions: Diagnostic and Therapeutic Considerations. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2007, 103, S25.e1–S25.e12. [Google Scholar] [CrossRef]
- Kim, H.J.; Yang, G.S.; Greenspan, J.D.; Downton, K.D.; Griffith, K.A.; Renn, C.L.; Dorsey, S.G. Racial and Ethnic Differences in Experimental Pain Sensitivity: Systematic Review and Meta-Analysis. Pain 2017, 158, 194–211. [Google Scholar] [CrossRef] [PubMed]
- López-Pintor, R.M.; Diniz-Freitas, M.; Ramesh, S.S.K.; Valdéz, J.A.; Bissonnette, C.; Dan, H.; Brennan, M.T.; Burkhart, N.W.; Greenberg, M.S.; Farag, A.; et al. World Workshop on Oral Medicine Viii: Development of a Core Outcome Set for Oral Lichen Planus: A Consensus Study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2023, 135, 772–780. [Google Scholar] [CrossRef]
- González-Moles, M.; Ruiz-Ávila, I.; González-Ruiz, L.; Ayén, A.; Gil-Montoya, J.A.; Ramos-García, P. Malignant Transformation Risk of Oral Lichen Planus: A Systematic Review and Comprehensive Meta-Analysis. Oral Oncol. 2019, 96, 121–130. [Google Scholar] [CrossRef]
- Jaber, M.A.; Elameen, E.M. Long-Term Follow-up of Oral Epithelial Dysplasia: A Hospital Based Cross-Sectional Study. J. Dent. Sci. 2021, 16, 304–310. [Google Scholar] [CrossRef]
- Bombeccari, G.P.; Guzzi, G.; Tettamanti, M.; Giannì, A.B.; Baj, A.; Pallotti, F.; Spadari, F. Oral Lichen Planus and Malignant Transformation: A Longitudinal Cohort Study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2011, 112, 328–334. [Google Scholar] [CrossRef]
- Gandolfo, S.; Richiardi, L.; Carrozzo, M.; Broccoletti, R.; Carbone, M.; Pagano, M.; Vestita, C.; Rosso, S.; Merletti, F. Risk of Oral Squamous Cell Carcinoma in 402 Patients with Oral Lichen Planus: A Follow-up Study in an Italian Population. Oral Oncol. 2004, 40, 77–83. [Google Scholar] [CrossRef]
- Guan, G.; Mei, L.; Polonowita, A.; Hussaini, H.; Seo, B.; Rich, A.M. Malignant Transformation in Oral Lichen Planus and Lichenoid Lesions: A 14-Year Longitudinal Retrospective Cohort Study of 829 Patients in New Zealand. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 411–418. [Google Scholar] [CrossRef]
- Kaomongkolgit, R.; Daroonpan, P.; Tantanapornkul, W.; Palasuk, J. Clinical Profile of 102 Patients with Oral Lichen Planus in Thailand. J. Clin. Exp. Dent. 2019, 11, e625. [Google Scholar] [CrossRef]
- Kaplan, I.; Ventura-Sharabi, Y.; Gal, G.; Calderon, S.; Anavi, Y. The Dynamics of Oral Lichen Planus: A Retrospective Clinicopathological Study. Head Neck Pathol. 2012, 6, 178–183. [Google Scholar] [CrossRef]
- Boñar-Alvarez, P.; Sayáns, M.P.; Garcia-Garcia, A.; Chamorro-Petronacci, C.; Gándara-Vila, P.; Luces-González, R.; Suárez-Peñaranda, J.M. Correlation between Clinical and Pathological Features of Oral Lichen Planus: A Retrospective Observational Study. Medicine 2019, 98, 8. [Google Scholar] [CrossRef]
- Al-Mohaya, M.A.; Al-Harthi, F.; Arfin, M.; Al-Asmari, A. Tnf-A, Tnf-Β and Il-10 Gene Polymorphism and Association with Oral Lichen Planus Risk in Saudi Patients. J. Appl. Oral Sci. 2015, 23, 295–301. [Google Scholar] [CrossRef]
- Escudier, M.; Ahmed, N.; Shirlaw, P.; Setterfield, J.; Tappuni, A.; Black, M.; Challacombe, S. A Scoring System for Mucosal Disease Severity with Special Reference to Oral Lichen Planus. Br. J. Dermatol. 2007, 157, 765–770. [Google Scholar] [CrossRef] [PubMed]
- Alsoghier, A. Integrating Oral Medicine within Saudi Arabia’s Healthcare Systems. Saudi J. Health Syst. Res. 2022, 2, 42–44. [Google Scholar] [CrossRef]
- Adeoye, J.; Koohi-Moghadam, M.; Choi, S.-W.; Zheng, L.-W.; Lo, A.W.I.; Tsang, R.K.-Y.; Chow, V.L.Y.; Akinshipo, A.; Thomson, P.; Su, Y.-X. Predicting Oral Cancer Risk in Patients with Oral Leukoplakia and Oral Lichenoid Mucositis Using Machine Learning. J. Big Data 2023, 10, 39. [Google Scholar] [CrossRef]

{kind=link}
| Clinical Characteristics | Category | Number (%) |
|---|---|---|
| Associated symptoms | Asymptomatic | 104 (74%) |
| Burning sensation | 15 (10%) | |
| Pain | 19 (13%) | |
| Cutaneous pruritus | 1 (0.7%) | |
| Nausea and vomiting | 1 (0.7%) | |
| Consistency | Soft | 62 (44%) |
| Firm | 9 (6%) | |
| Not recorded | 69 (49%) | |
| Site | Buccal mucosa and sulcus | 79 (56%) |
| Ginigva and alveolar mucosa | 21 (15%) | |
| Tongue | 20 (14%) | |
| Lateral tongue | 12 (8%) | |
| Dorsal tongue | 4 (2%) | |
| Ventral tongue | 2 (1%) | |
| Lips and labial mucosa | 10 (7%) | |
| Hard and soft palate | 7 (5%) | |
| The floor of the mouth | 2 (1%) | |
| Type of Biopsy | Incisional | 135 (96%) |
| Excisional | 5 (3%) | |
| Management | Corticosteroid alone or combined with immunosuppressants | 22 (15%) |
| Not required or recorded 1 | 117 (83%) |
| Findings | Number (%) of Records Showing this Finding | |
|---|---|---|
| Yes | No | |
| Band-like inflammatory cells | 140 (100%) | 0 (0%) |
| Epithelial hyperkeratosis 1 | 138 (99%) | 2 (1%) |
| Atrophic 2 | 124 (88%) | 15 (10%) |
| Basal cell degeneration | 124 (88%) | 16 (11%) |
| Squamatisation | 122 (87%) | 18 (12%) |
| Thickening of basement membrane | 102 (72%) | 38 (27%) |
| Fibrin deposit 3 | 100 (71%) | 40 (28%) |
| Civatte bodies | 85 (60%) | 55 (39%) |
| Melanin incontinence | 82 (58%) | 58 (41%) |
| Saw tooth rete ridges | 63 (45%) | 77 (55%) |
| Hypergranulosis | 57 (40%) | 83 (59%) |
| Artificial cleft formation | 53 (37%) | 87 (62%) |
| Acanthosis 1 | 33 (23%) | 106 (75%) |
| Ulcer | 23 (16%) | 117 (83%) |
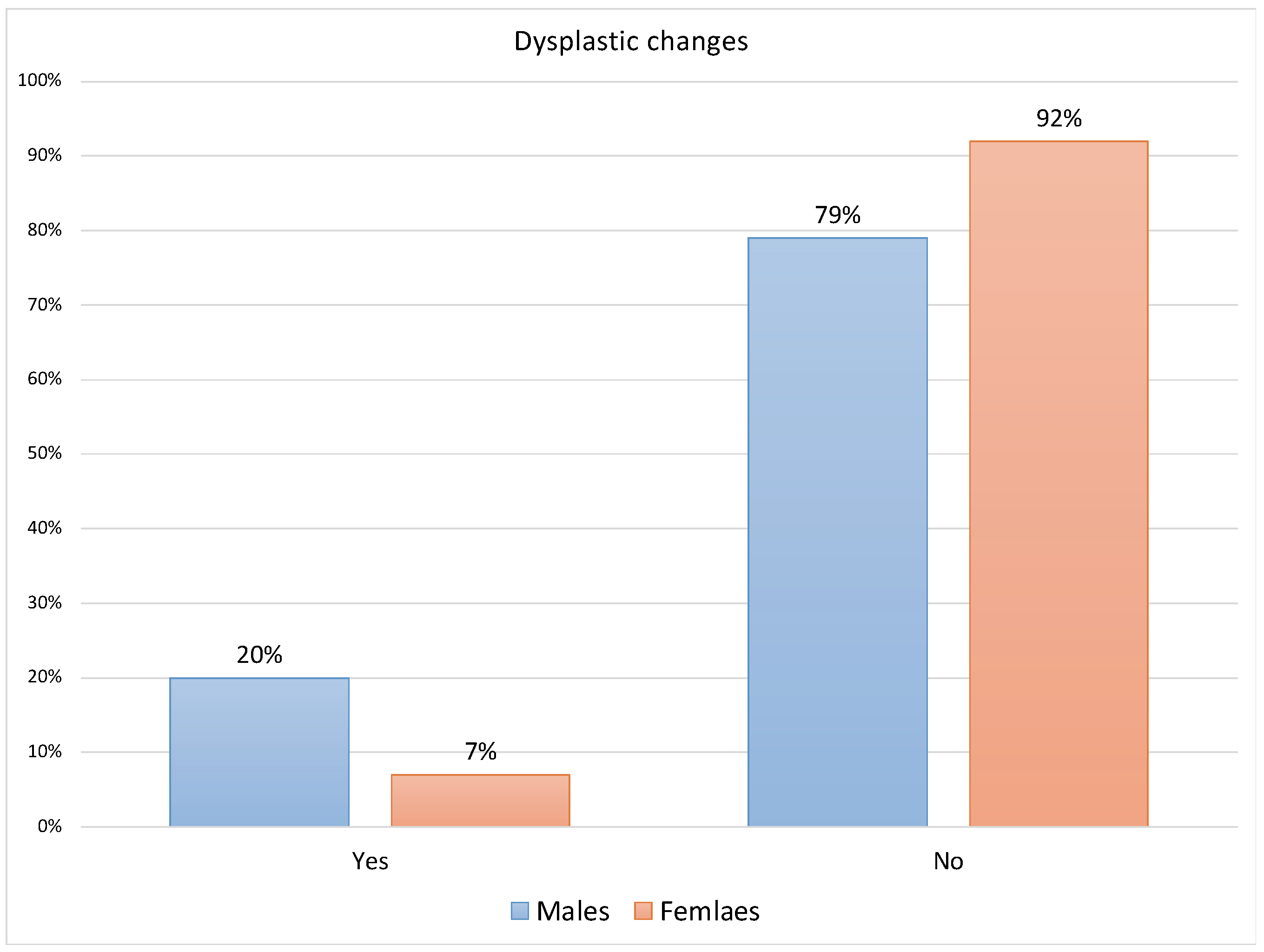
| Dysplastic changes | 18 (12%) | 122 (87%) |
| Medical History | Symptoms | p-Value | |
|---|---|---|---|
| Asymptomatic | Symptomatic | ||
| Diabetes millets | 15 (14.42%) | 12 (33.33%) | 0.0132 C* |
| Hypertension | 7 (6.73%) | 13 (36.11%) | < 0.001 C* |
| Hypothyroidism | 6 (5.77%) | 3 (8.33%) | 0.6944 F |
| Discoid lupus erythematous | 6 (5.77%) | 5 (13.89%) | 0.1502 F |
| Cutaneous lichen planus | 3 (2.88%) | 0 | 0.5692 F |
| Asthma | 2 (1.92%) | 1 (2.78%) | 0.9999 F |
| Cutaneous allergy | 2 (1.92%) | 0 | 0.9999 F |
| Breast cancer | 0 | 2 (5.56%) | 0.0648 F |
| Cardiac catheterization | 1 (0.96%) | 0 | 0.9999 F |
| Peptic ulcer | 1 (0.96%) | 0 | 0.9999 F |
| Sjogren’s syndrome | 1 (0.96%) | 0 | 0.9999 F |
| Psoriasis | 1 (0.96%) | 0 | 0.9999 F |
| Liver cirrhosis | 1 (0.96%) | 0 | 0.9999 F |
| Vitamin D deficiency | 1 (0.96%) | 0 | 0.9999 F |
| Fatigue | 1 (0.96%) | 0 | 0.9999 F |
| Depression | 1 (0.96%) | 1 (2.78%) | 0.4495 F |
| Inflammatory bowel disease | 1 (0.96%) | 0 | 0.9999 F |
| Osteoporosis | 1 (0.96%) | 1 (2.78%) | 0.4495 F |
| Coronary artery bypass surgery | 1 (0.96%) | 0 | 0.9999 F |
| Dry mouth | 0 | 1 (2.78%) | 0.2571 F |
| Rheumatoid arthritis | 0 | 1 (2.78%) | 0.2571 F |
| Variables | Age (Years) | p-Value | ||
|---|---|---|---|---|
| Mean (±SD) | Median (Min, Max) | |||
| Symptoms | Symptomatic | 53.64 (±13) | 56 (22, 79) | < 0.001 t* |
| Asymptomatic | 45.24 (±12) | 45 (22, 76) | ||
| Ulcer | No | 46.47 (±13) | 47.5 (22, 79) | 0.0149 t* |
| Yes | 54.2 (±11) | 52 (40, 75) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsoghier, A.; AlMadan, N.; Alali, M.; Alshagroud, R. Clinicohistological Characteristics of Patients with Oral Lichenoid Mucositis: A Retrospective Study for Dental Hospital Records. J. Clin. Med. 2023, 12, 6383. https://doi.org/10.3390/jcm12196383
Alsoghier A, AlMadan N, Alali M, Alshagroud R. Clinicohistological Characteristics of Patients with Oral Lichenoid Mucositis: A Retrospective Study for Dental Hospital Records. Journal of Clinical Medicine. 2023; 12(19):6383. https://doi.org/10.3390/jcm12196383
Chicago/Turabian StyleAlsoghier, Abdullah, Nasser AlMadan, Mohammed Alali, and Rana Alshagroud. 2023. "Clinicohistological Characteristics of Patients with Oral Lichenoid Mucositis: A Retrospective Study for Dental Hospital Records" Journal of Clinical Medicine 12, no. 19: 6383. https://doi.org/10.3390/jcm12196383
APA StyleAlsoghier, A., AlMadan, N., Alali, M., & Alshagroud, R. (2023). Clinicohistological Characteristics of Patients with Oral Lichenoid Mucositis: A Retrospective Study for Dental Hospital Records. Journal of Clinical Medicine, 12(19), 6383. https://doi.org/10.3390/jcm12196383