
Association between Antidepressants and Dementia Risk in Older Adults with Depression: A Systematic Review and Meta-Analysis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategies
2.2. Article Selection
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Data Analysis
3. Results
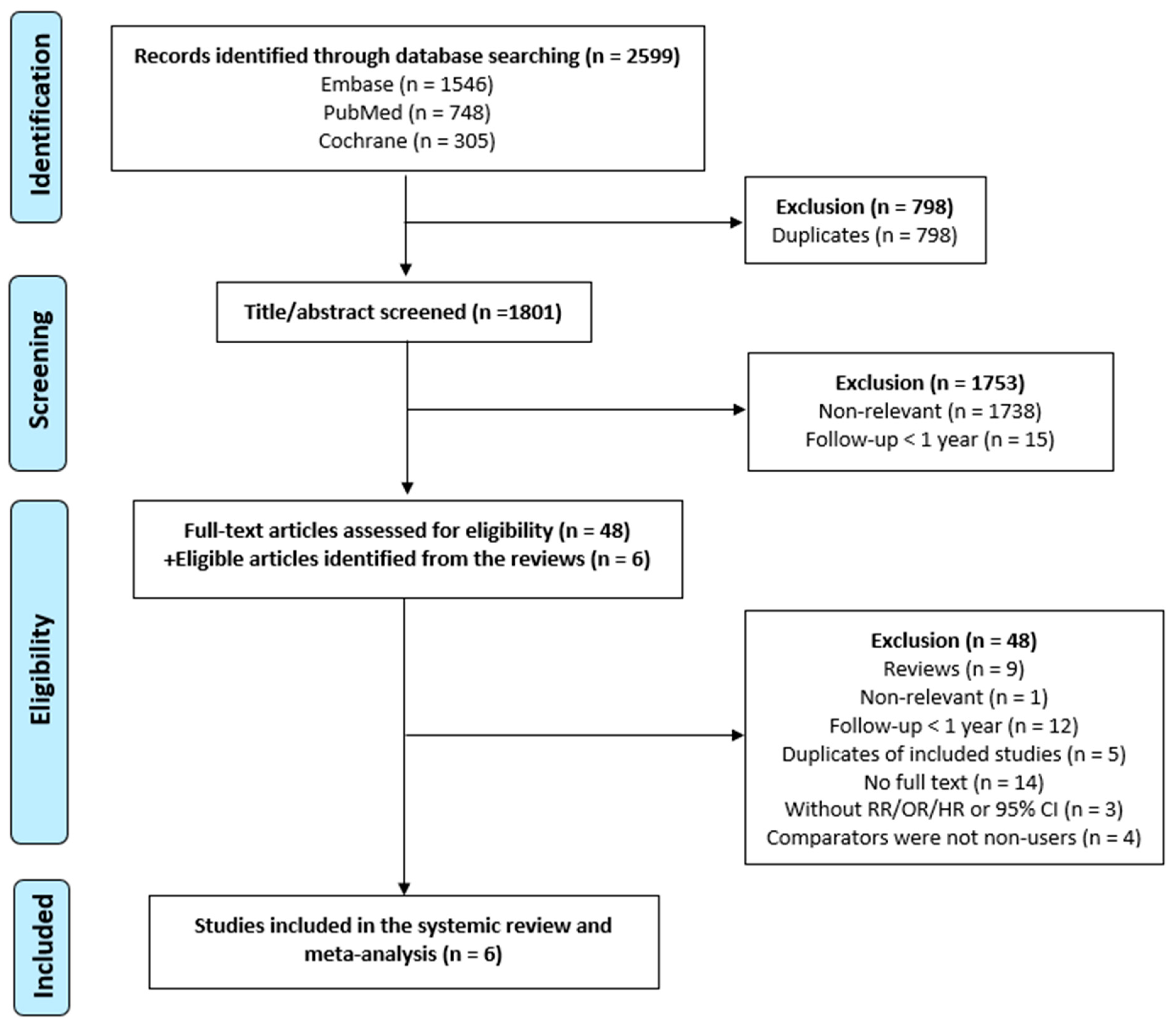
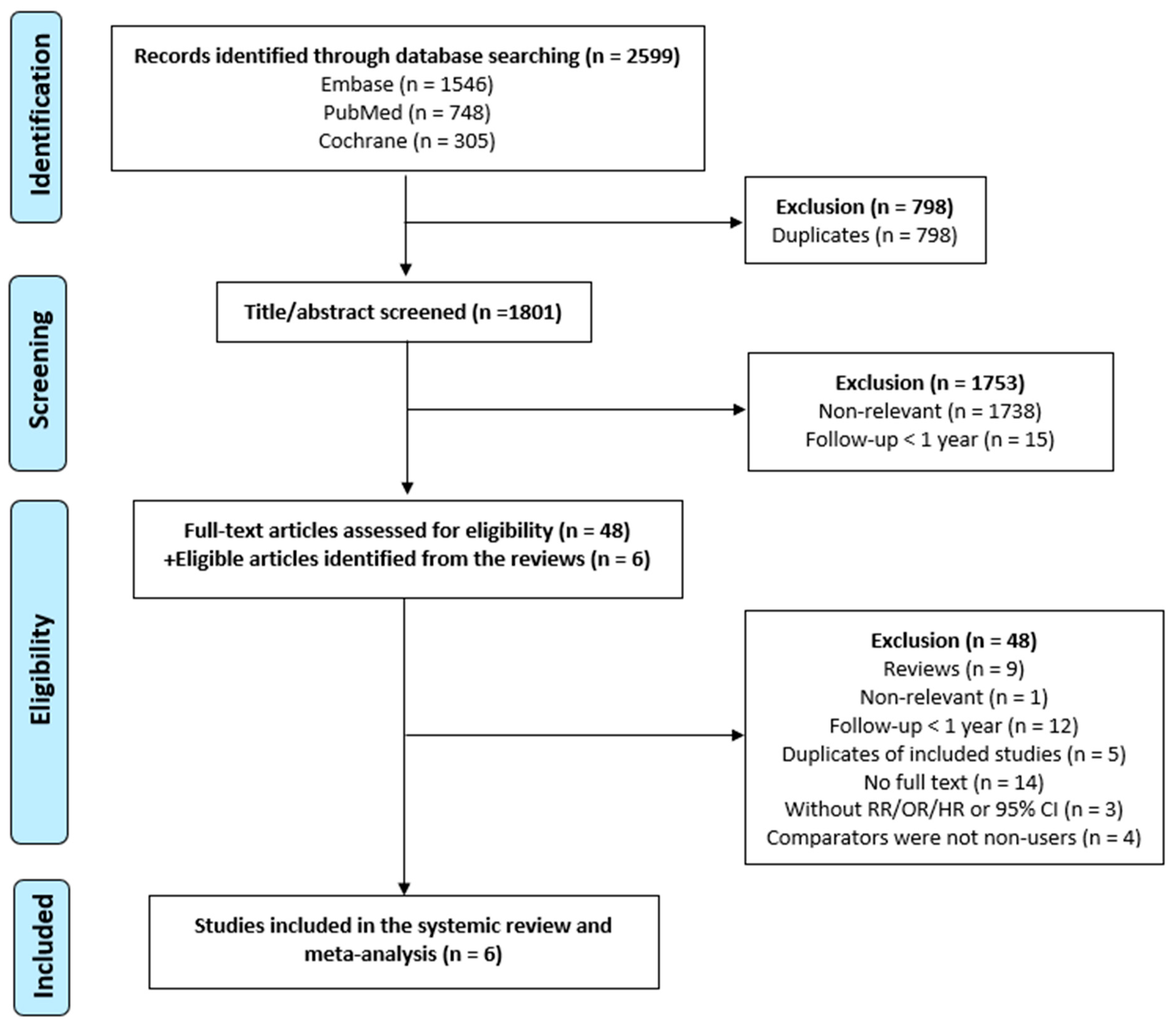
3.1. Literature Search
3.2. Study Characteristics
3.3. Summary of the Included Studies
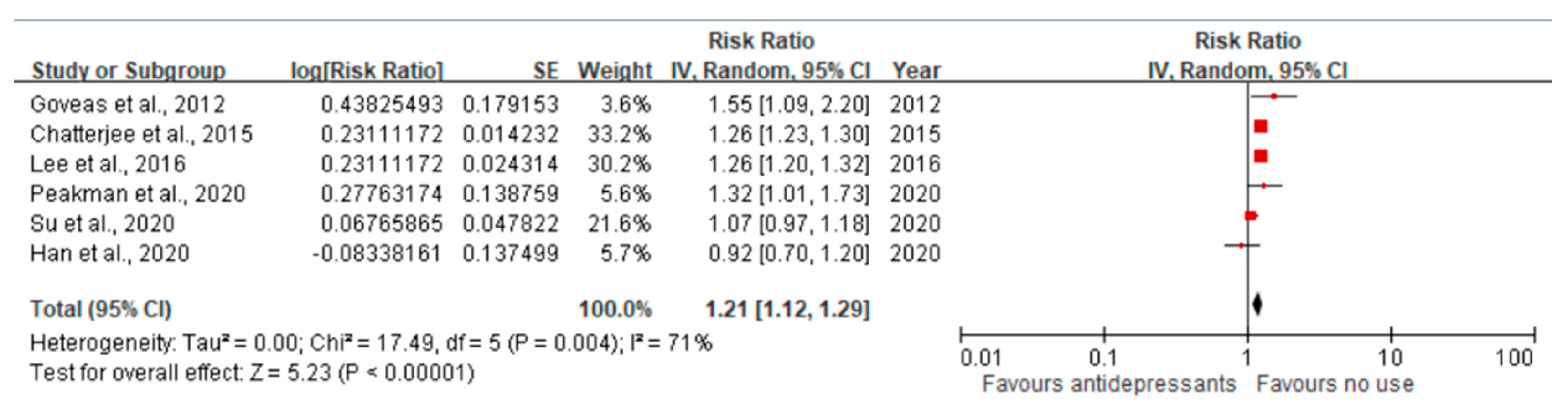
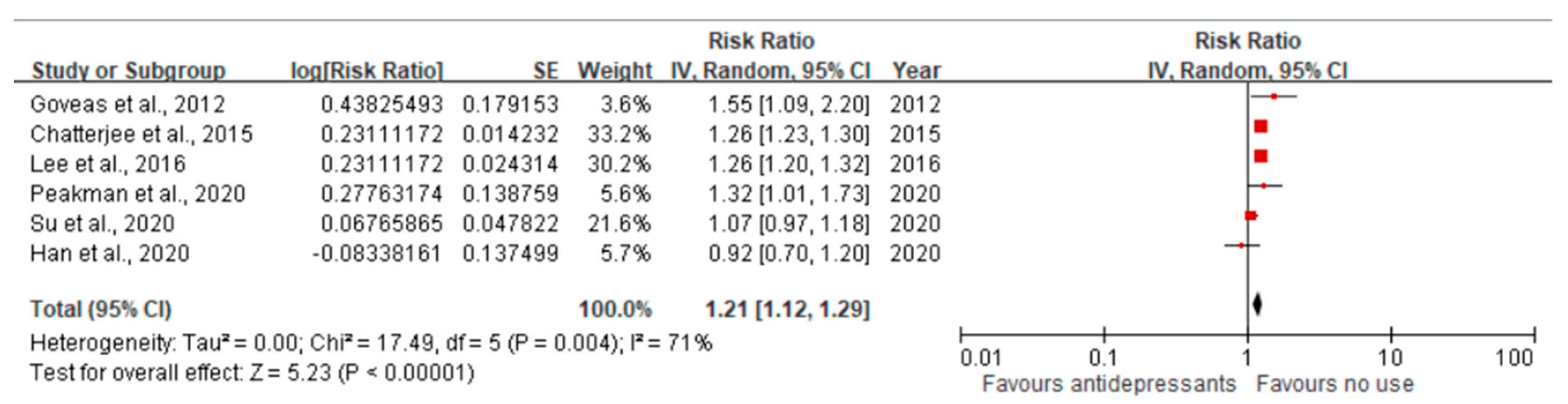
3.4. Meta-Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Emmady, P.D.; Schoo, C.; Tadi, P. Major neurocognitive disorder (dementia). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Plassman, B.L.; Langa, K.M.; Fisher, G.G.; Heeringa, S.G.; Weir, D.R.; Ofstedal, M.B.; Burke, J.R.; Hurd, M.D.; Potter, G.G.; Rodgers, W.L.; et al. Prevalence of dementia in the United States: The aging, demographics, and memory study. Neuroepidemiology 2007, 29, 125–132. [Google Scholar] [CrossRef]
- Wang, Y.-C.; Tai, P.-A.; Poly, T.N.; Islam, M.M.; Yang, H.-C.; Wu, C.-C.; Li, Y.-C.J. Increased Risk of Dementia in Patients with Antidepressants: A Meta-Analysis of Observational Studies. Behav. Neurol. 2018, 2018, 5315098. [Google Scholar] [CrossRef]
- Skaria, A.P. The economic and societal burden of Alzheimer disease: Managed care considerations. Am. J. Manag. Care 2022, 28, S188–S196. [Google Scholar] [PubMed]
- Nichols, E.; Steinmetz, J.D.; Vollset, S.E.; Fukutaki, K.; Chalek, J.; Abd-Allah, F.; Abdoli, A.; Abualhasan, A.; Abu-Gharbieh, E.; Akram, T.T. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Bains, N.; Abdijadid, S.; Miller, J.L. Major depressive disorder (nursing). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Hasin, D.S.; Sarvet, A.L.; Meyers, J.L.; Saha, T.D.; Ruan, W.J.; Stohl, M.; Grant, B.F. Epidemiology of Adult DSM-5 Major Depressive Disorder and Its Specifiers in the United States. JAMA Psychiatry 2018, 75, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Santomauro, D.F.; Herrera, A.M.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation (IHME). GBD Compare Data Visualization; IHME, University of Washington: Seattle, WA, USA, 2020; Available online: http://vizhub.healthdata.org/gbd-compare (accessed on 8 April 2022).
- Morimoto, S.S.; Kanellopoulos, D.; Alexopoulos, G.S. Cognitive Impairment in Depressed Older Adults: Implications for Prognosis and Treatment. Psychiatr. Ann. 2014, 44, 138–142. [Google Scholar] [CrossRef]
- Barnes, D.E.; Yaffe, K.; Byers, A.L.; McCormick, M.; Schaefer, C.; Whitmer, R.A. Midlife vs late-life depressive symptoms and risk of dementia: Differential effects for Alzheimer disease and vascular dementia. Arch. Gen. Psychiatry 2012, 69, 493–498. [Google Scholar] [PubMed]
- Baumgart, M.; Snyder, H.M.; Carrillo, M.C.; Fazio, S.; Kim, H.; Johns, H. Summary of the evidence on modifiable risk factors for cognitive decline and dementia: A population-based perspective. Alzheimer’s Dement. 2015, 11, 718–726. [Google Scholar] [CrossRef]
- Cerejeira, J.; Lagarto, L.; Mukaetova-Ladinska, E. Behavioral and psychological symptoms of dementia. Front. Neurol. 2012, 3, 73. [Google Scholar] [CrossRef]
- Zubenko, G.S.; Zubenko, W.N.; McPherson, S.; Spoor, E.; Marin, D.B.; Farlow, M.R.; Smith, G.E.; Geda, Y.E.; Cummings, J.L.; Petersen, R.C. A collaborative study of the emergence and clinical features of the major depressive syndrome of Alzheimer’s disease. Am. J. Psychiatry 2003, 160, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Wolf, N.J.; Hopko, D.R. Psychosocial and pharmacological interventions for depressed adults in primary care: A critical review. Clin. Psychol. Rev. 2008, 28, 131–161. [Google Scholar] [CrossRef]
- Dudas, R.; Malouf, R.; McCleery, J.; Dening, T. Antidepressants for treating depression in dementia. Cochrane Database Syst. Rev. 2018, 8, CD003944. [Google Scholar] [CrossRef] [PubMed]
- Mur, J.; Russ, T.C.; Cox, S.R.; Marioni, R.E.; Muniz-Terrera, G. Association between anticholinergic burden and dementia in UK Biobank. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2022, 8, e12290. [Google Scholar] [CrossRef] [PubMed]
- Panel, A.G.S.B.C.U.E.; Fick, D.M.; Semla, T.P.; Steinman, M.; Beizer, J.; Brandt, N.; Dombrowski, R.; DuBeau, C.E.; Pezzullo, L.; Epplin, J.J. American Geriatrics Society 2019 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar]
- Wiese, B.S. Geriatric depression: The use of antidepressants in the elderly. BC Med. J. 2011, 53, 341–347. [Google Scholar]
- Bishop, M.M.; Fixen, D.R.; Linnebur, S.A.; Pearson, S.M. Cognitive effects of vortioxetine in older adults: A systematic review. Ther. Adv. Psychopharmacol. 2021, 11, 20451253211026796. [Google Scholar] [CrossRef]
- Doraiswamy, P.M.; Krishnan, K.R.R.; Oxman, T.; Jenkyn, L.R.; Coffey, D.J.; Burt, T.; Clary, C.M. Does Antidepressant Therapy Improve Cognition in Elderly Depressed Patients? J. Gerontol. Ser. A 2003, 58, M1137–M1144. [Google Scholar] [CrossRef]
- Ferguson, J.M.; Wesnes, K.A.; Schwartz, G.E. Reboxetine versus paroxetine versus placebo: Effects on cognitive functioning in depressed patients. Int. Clin. Psychopharmacol. 2003, 18, 9–14. [Google Scholar]
- Geretsegger, C.; Böhmer, F.; Ludwig, M. Paroxetine in the elderly depressed patient: Randomized comparison with fluoxetine of efficacy, cognitive and behavioural effects. Int. Clin. Psychopharmacol. 1994, 9, 25–29. [Google Scholar] [CrossRef]
- Cassano, G.B.; Puca, F.; Scapicchio, P.L.; Trabucchi, M. Paroxetine and fluoxetine effects on mood and cognitive functions in depressed nondemented elderly patients. J. Clin. Psychiatry 2002, 63, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Nyth, A.L.; Gottfries, C.G.; Lyby, K.; Smedegaard-Andersen, L.; Gylding-Sabroe, J.; Kristensen, M.; Refsum, H.E.; Ofsti, E.; Eriksson, S.; Syversen, S. A controlled multicenter clinical study of citalopram and placebo in elderly depressed patients with and without concomitant dementia. Acta Psychiatr. Scand. 1992, 86, 138–145. [Google Scholar] [CrossRef]
- Raskin, J.; Wiltse, C.G.; Siegal, A.; Sheikh, J.; Xu, J.; Dinkel, J.J.; Rotz, B.T.; Mohs, R.C. Efficacy of duloxetine on cognition, depression, and pain in elderly patients with major depressive disorder: An 8-week, double-blind, placebo-controlled trial. Am. J. Psychiatry 2007, 164, 900–909. [Google Scholar] [CrossRef] [PubMed]
- Heser, K.; Luck, T.; Röhr, S.; Wiese, B.; Kaduszkiewicz, H.; Oey, A.; Bickel, H.; Mösch, E.; Weyerer, S.; Werle, J.; et al. Potentially inappropriate medication: Association between the use of antidepressant drugs and the subsequent risk for dementia. J. Affect. Disord. 2018, 226, 28–35. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group*. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Schiavo, J.H. PROSPERO: An international register of systematic review protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Limaye, D.; Limaye, V.; Pitani, R.S.; Fortwengel, G.; Sydymanov, A.; Otzipka, C.; Ziesenis, P. Development of a quantitative scoring method for STROBE checklist. Acta Pol. Pharm. Drug Res. 2018, 75, 1095–1106. [Google Scholar] [CrossRef]
- Stare, J.; Maucort-Boulch, D. Odds ratio, hazard ratio and relative risk. Adv. Methodol. Stat. 2016, 13, 59–67. [Google Scholar] [CrossRef]
- Viera, A.J. Odds ratios and risk ratios: What’s the difference and why does it matter? South. Med. J. 2008, 101, 730–734. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Goveas, J.S.; Hogan, P.E.; Kotchen, J.M.; Smoller, J.W.; Denburg, N.L.; Manson, J.E.; Tummala, A.; Mysiw, W.J.; Ockene, J.K.; Woods, N.F. Depressive symptoms, antidepressant use, and future cognitive health in postmenopausal women: The Women’s Health Initiative Memory Study. Int. Psychogeriatr. 2012, 24, 1252–1264. [Google Scholar] [CrossRef]
- Chatterjee, S.; Bali, V.; Carnahan, R.M.; Johnson, M.L.; Chen, H.; Aparasu, R.R. Anticholinergic medication use and risk of dementia among elderly nursing home residents with depression. Am. J. Geriatr. Psychiatry 2016, 24, 485–495. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.W.-S.; Lin, C.-L.; Sung, F.-C.; Liang, J.-A.; Kao, C.-H. Antidepressant treatment and risk of dementia: A population-based, retrospective case-control study. J. Clin. Psychiatry 2016, 77, 961. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Bonnett, T.; Brenowitz, W.D.; Teylan, M.A.; Besser, L.M.; Chen, Y.-C.; Chan, G.; Cao, K.-G.; Gao, Y.; Zhou, X.-H. Estimating associations between antidepressant use and incident mild cognitive impairment in older adults with depression. PLoS ONE 2020, 15, e0227924. [Google Scholar] [CrossRef] [PubMed]
- Peakman, G.; Karunatilake, N.; Seynaeve, M.; Perera, G.; Aarsland, D.; Stewart, R.; Mueller, C. Clinical factors associated with progression to dementia in people with late-life depression: A cohort study of patients in secondary care. BMJ Open 2020, 10, e035147. [Google Scholar] [CrossRef]
- Su, J.-A.; Chang, C.-C.; Yang, Y.-H.; Chen, K.-J.; Li, Y.-P.; Lin, C.-Y. Risk of incident dementia in late-life depression treated with antidepressants: A nationwide population cohort study. J. Psychopharmacol. 2020, 34, 1134–1142. [Google Scholar] [CrossRef]
- Dafsari, F.S.; Jessen, F. Depression—An underrecognized target for prevention of dementia in Alzheimer’s disease. Transl. Psychiatry 2020, 10, 160. [Google Scholar] [CrossRef]
- Cassano, T.; Calcagnini, S.; Carbone, A.; Bukke, V.N.; Orkisz, S.; Villani, R.; Romano, A.; Avolio, C.; Gaetani, S. Pharmacological treatment of depression in Alzheimer’s disease: A challenging task. Front. Pharmacol. 2019, 10, 1067. [Google Scholar] [CrossRef]
- Keefe, R.S.; McClintock, S.M.; Roth, R.M.; Doraiswamy, P.M.; Tiger, S.; Madhoo, M. Cognitive effects of pharmacotherapy for major depressive disorder: A systematic review. J. Clin. Psychiatry 2014, 75, 3169. [Google Scholar] [CrossRef]
- Caruso, G.; Grasso, M.; Fidilio, A.; Torrisi, S.A.; Musso, N.; Geraci, F.; Tropea, M.R.; Privitera, A.; Tascedda, F.; Puzzo, D.; et al. Antioxidant Activity of Fluoxetine and Vortioxetine in a Non-Transgenic Animal Model of Alzheimer’s Disease. Front. Pharmacol. 2021, 12, 809541. [Google Scholar] [CrossRef] [PubMed]
- Alboni, S.; Benatti, C.; Colliva, C.; Radighieri, G.; Blom, J.M.C.; Brunello, N.; Tascedda, F. Vortioxetine Prevents Lipopolysaccharide-Induced Memory Impairment Without Inhibiting the Initial Inflammatory Cascade. Front. Pharmacol. 2020, 11, 603979. [Google Scholar] [CrossRef] [PubMed]
- Torrisi, S.A.; Geraci, F.; Tropea, M.R.; Grasso, M.; Caruso, G.; Fidilio, A.; Musso, N.; Sanfilippo, G.; Tascedda, F.; Palmeri, A.; et al. Fluoxetine and Vortioxetine Reverse Depressive-Like Phenotype and Memory Deficits Induced by Aβ(1-42) Oligomers in Mice: A Key Role of Transforming Growth Factor-β1. Front. Pharmacol. 2019, 10, 693. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Author, Year | Exposure | Comparison | Follow-Up (Years) | Adjusted RR (95% CI) |
|---|---|---|---|---|
| Goveas et al., 2012 [36] | ADs | no use | 7.6 | 1.55 (1.09–2.20) |
| Chatterjee et al., 2015 [37] | Anticholinergic ADs | no use | 3 | 1.26 (1.22–1.29) |
| Lee et al., 2016 [38] | TCAs | no use | 5 | 0.24 (0.22–0.27) |
| SSRIs | 2.48 (2.27–2.71) | |||
| MAOIs | 1.86 (1.47–2.36) | |||
| Heterocyclic ADs | 1.44 (1.32–1.57) | |||
| Other ADs | 2.05 (1.85–2.27) | |||
| Han et al., 2020 [39] | ADs | no use | 5 | 0.92 (0.70–1.20) |
| Peakman et al., 2020 [40] | ADs | no use | 2.7 | 1.32 (1.01–1.74) |
| Su et al., 2020 [41] | ADs | no use: cDDD < 28 | 8 | |
| cDDD 28-167 | 1.06 (0.91–1.23) | |||
| cDDD 168+ | 1.07 (0.95–1.20) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, G.H.-M.; Li, P.; Wang, Y.; Guo, J.; Wilson, D.L.; Lo-Ciganic, W.-H. Association between Antidepressants and Dementia Risk in Older Adults with Depression: A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 6342. https://doi.org/10.3390/jcm12196342
Wang GH-M, Li P, Wang Y, Guo J, Wilson DL, Lo-Ciganic W-H. Association between Antidepressants and Dementia Risk in Older Adults with Depression: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(19):6342. https://doi.org/10.3390/jcm12196342
Chicago/Turabian StyleWang, Grace Hsin-Min, Piaopiao Li, Yehua Wang, Jingchuan Guo, Debbie L. Wilson, and Wei-Hsuan Lo-Ciganic. 2023. "Association between Antidepressants and Dementia Risk in Older Adults with Depression: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 19: 6342. https://doi.org/10.3390/jcm12196342
APA StyleWang, G. H.-M., Li, P., Wang, Y., Guo, J., Wilson, D. L., & Lo-Ciganic, W.-H. (2023). Association between Antidepressants and Dementia Risk in Older Adults with Depression: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 12(19), 6342. https://doi.org/10.3390/jcm12196342