
The Role of Adipose Tissue Mesenchymal Stem Cells in Colonic Anastomosis Healing in Inflammatory Bowel Disease: Experimental Study in Rats

 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Experimental Design
2.3. Adipose Tissue-Derived Mesenchymal Stromal Cells
2.4. Colitis Protocol
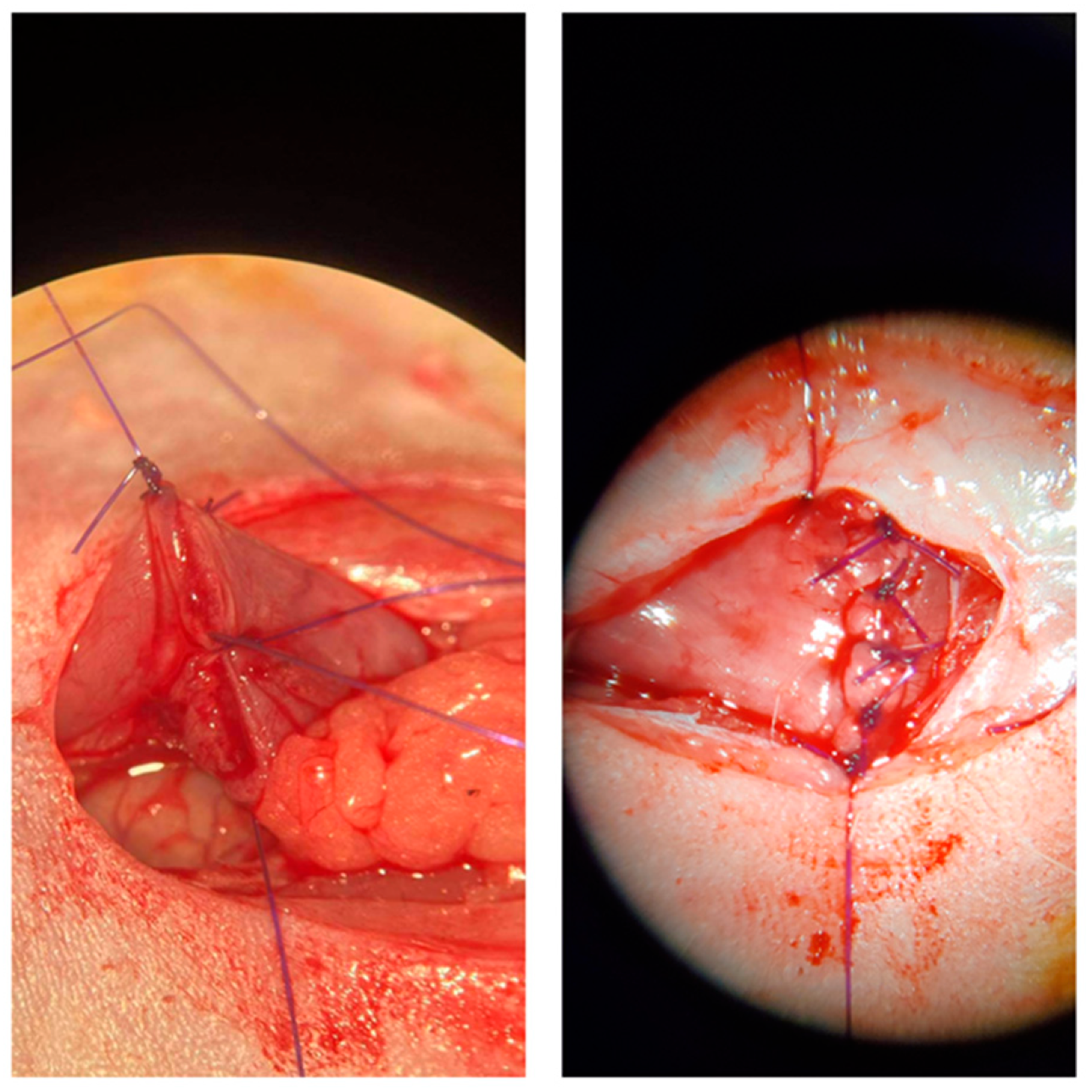
2.5. Operative Procedure
2.6. Macroscopic Assessment
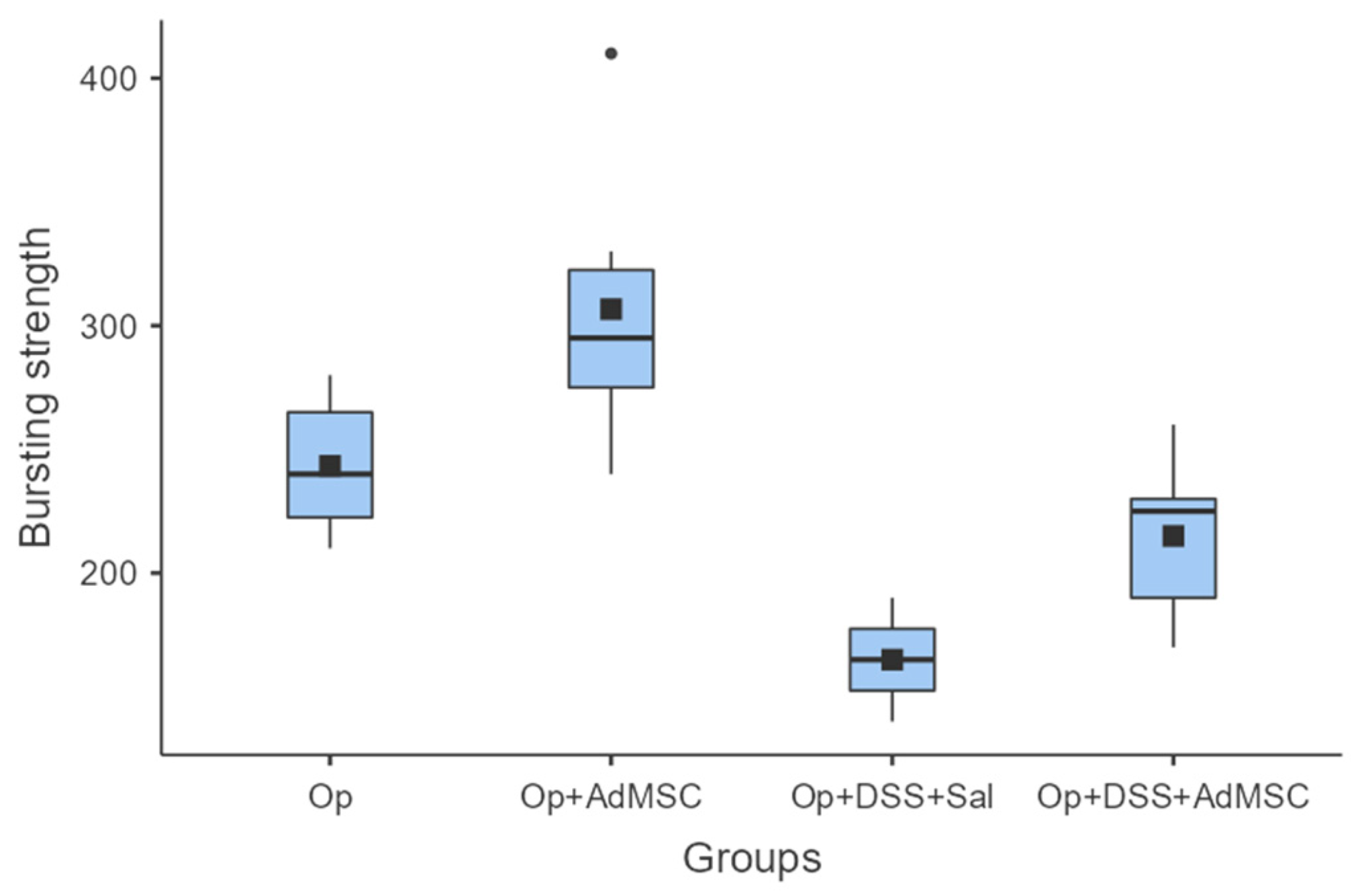
2.7. Bursting Pressure
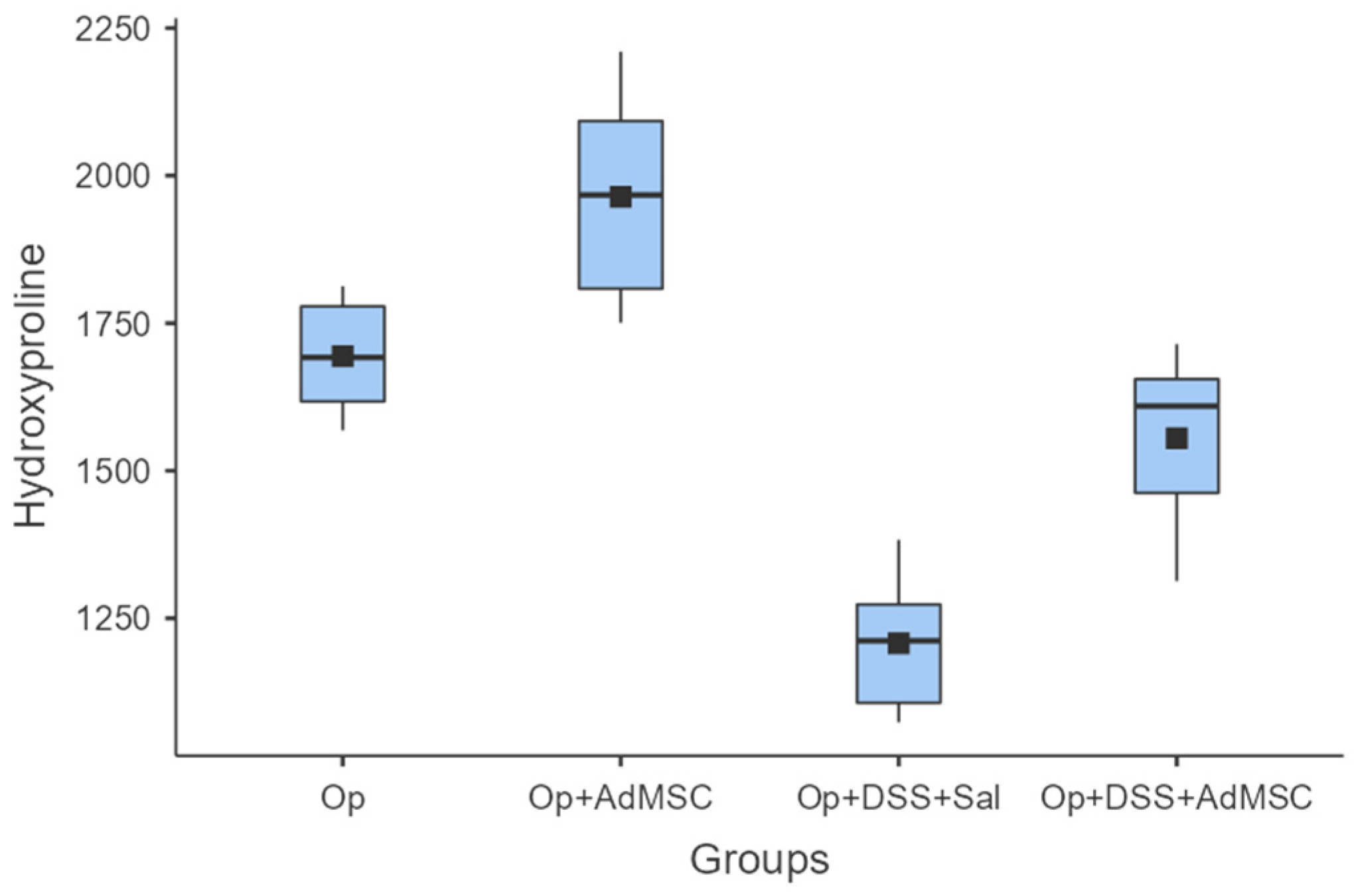
2.8. Hydroxyproline
2.9. Real Time-Polymerase Chain Reaction
2.10. Statistical Analysis
3. Results
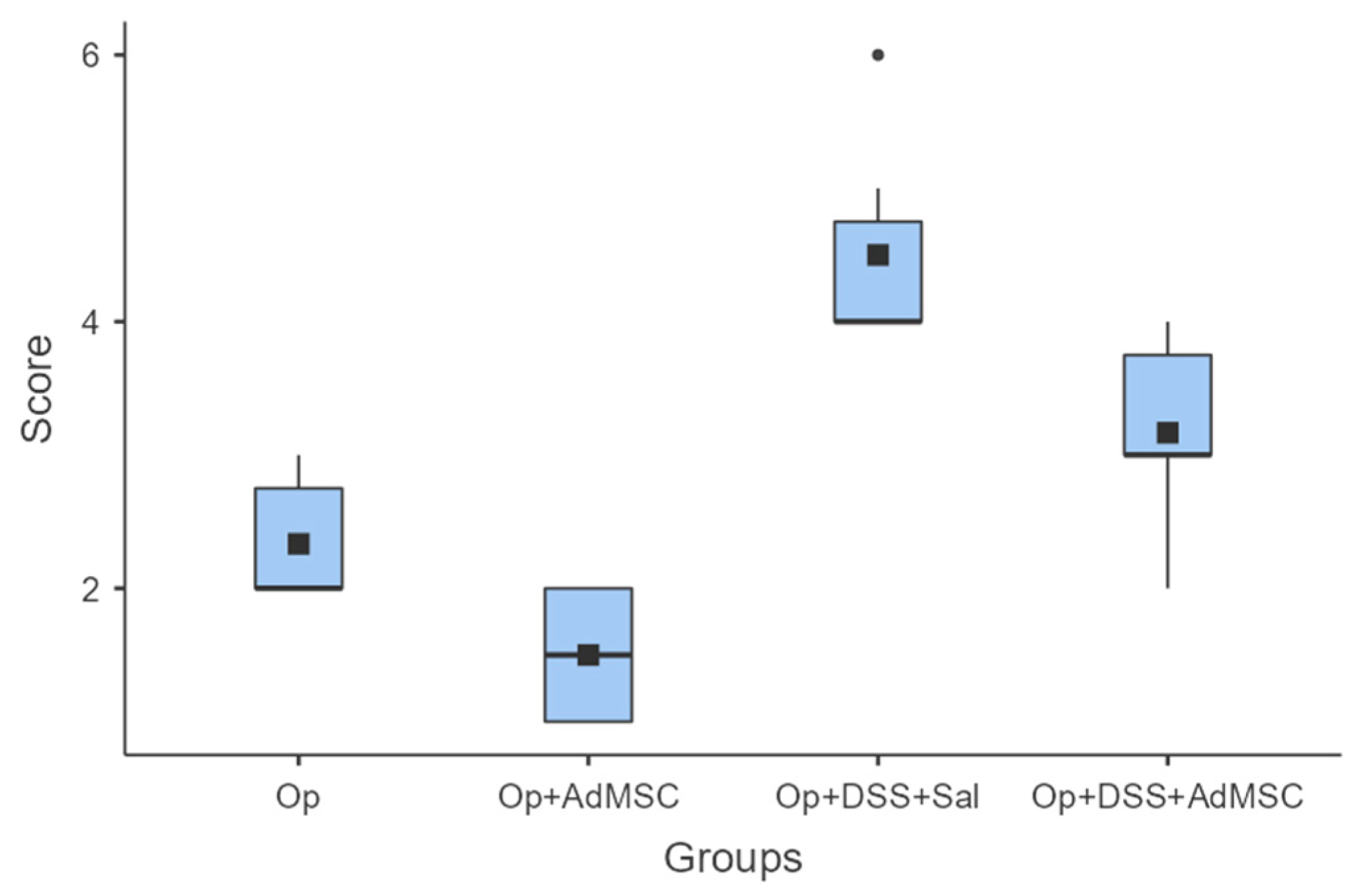
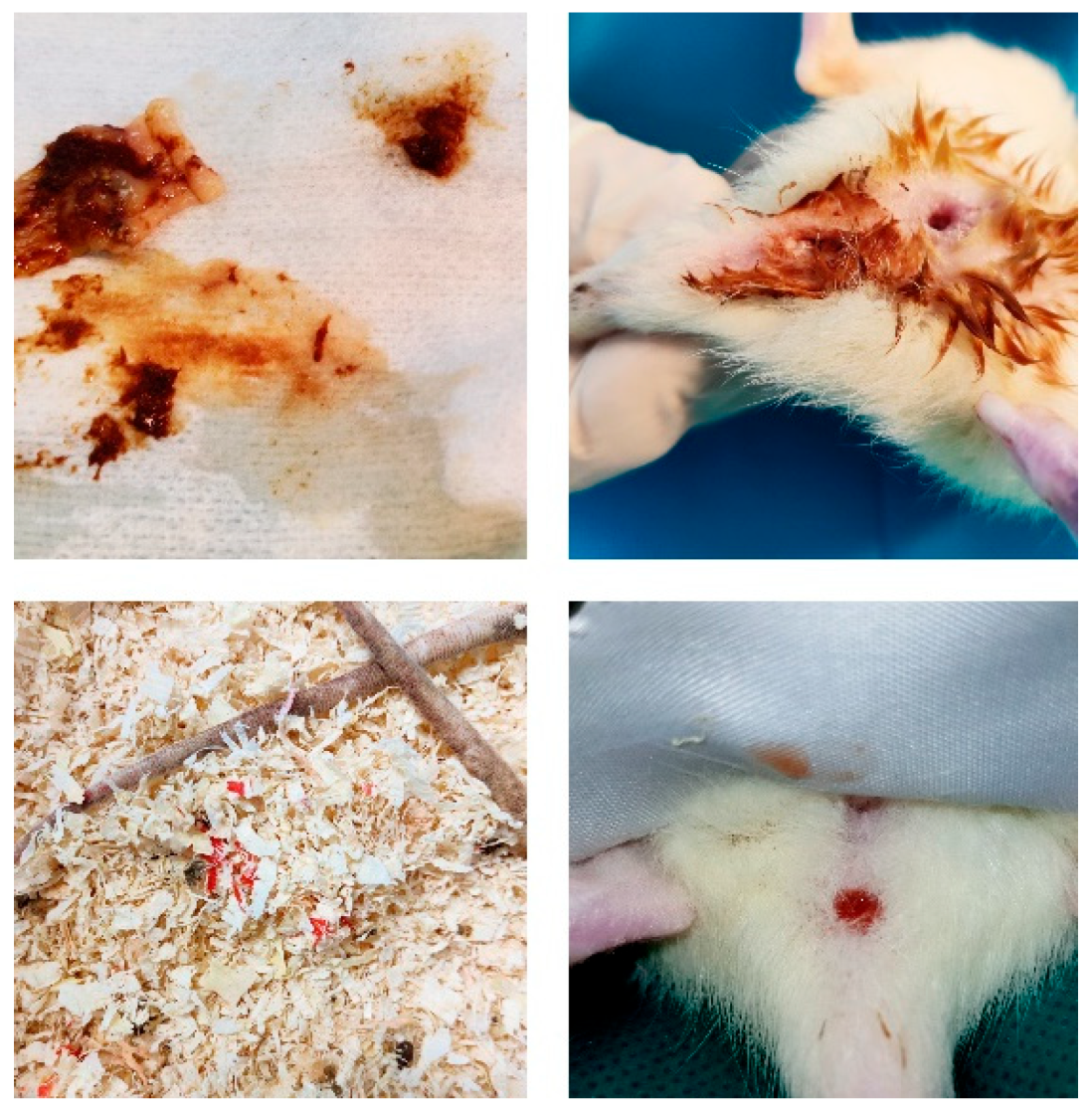
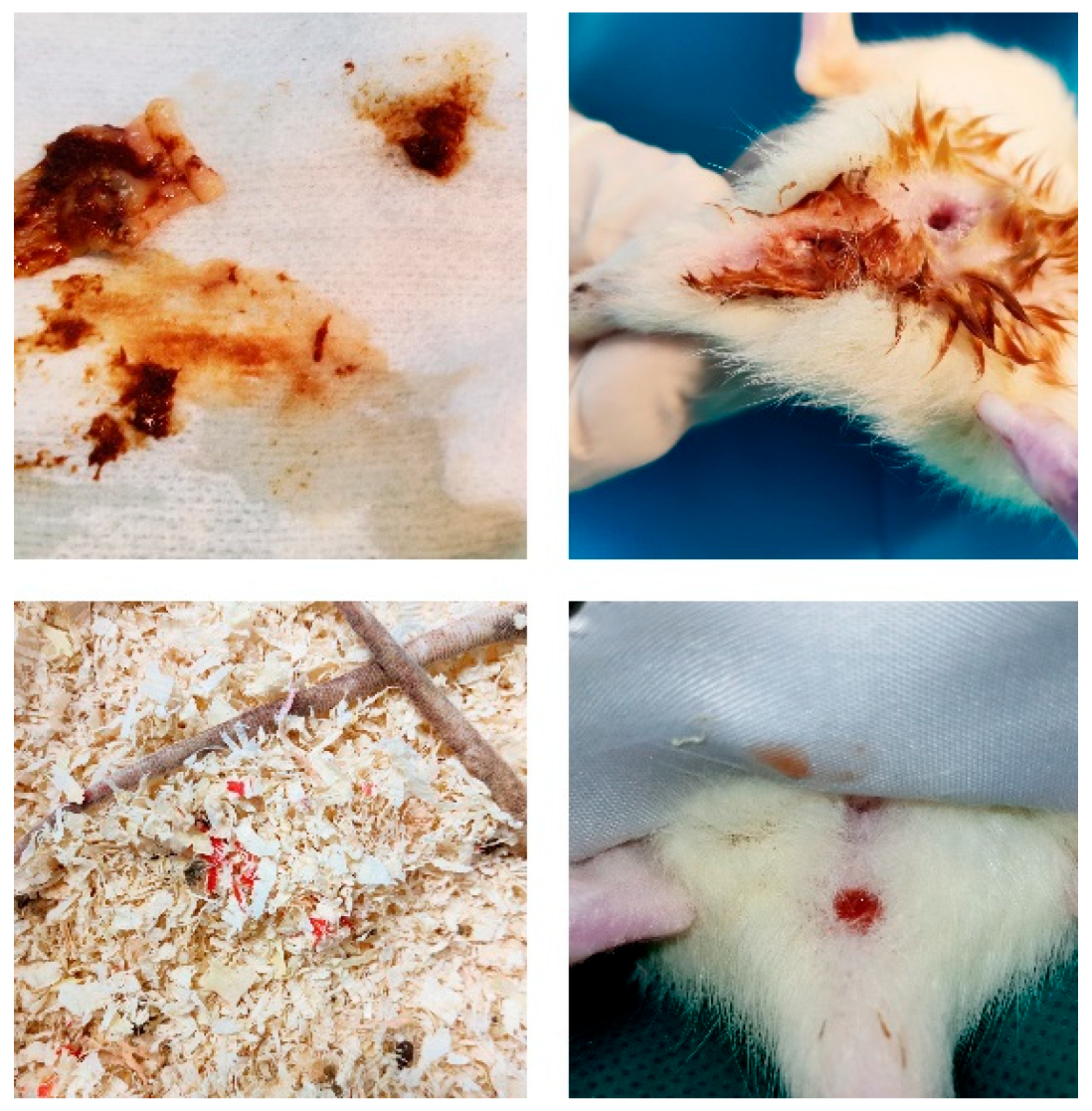
3.1. AdMSCs Macroscopically Attenuate Intra-Abdominal Complications
3.2. Bursting Strength Is Significantly Higher in Groups with AdMSC
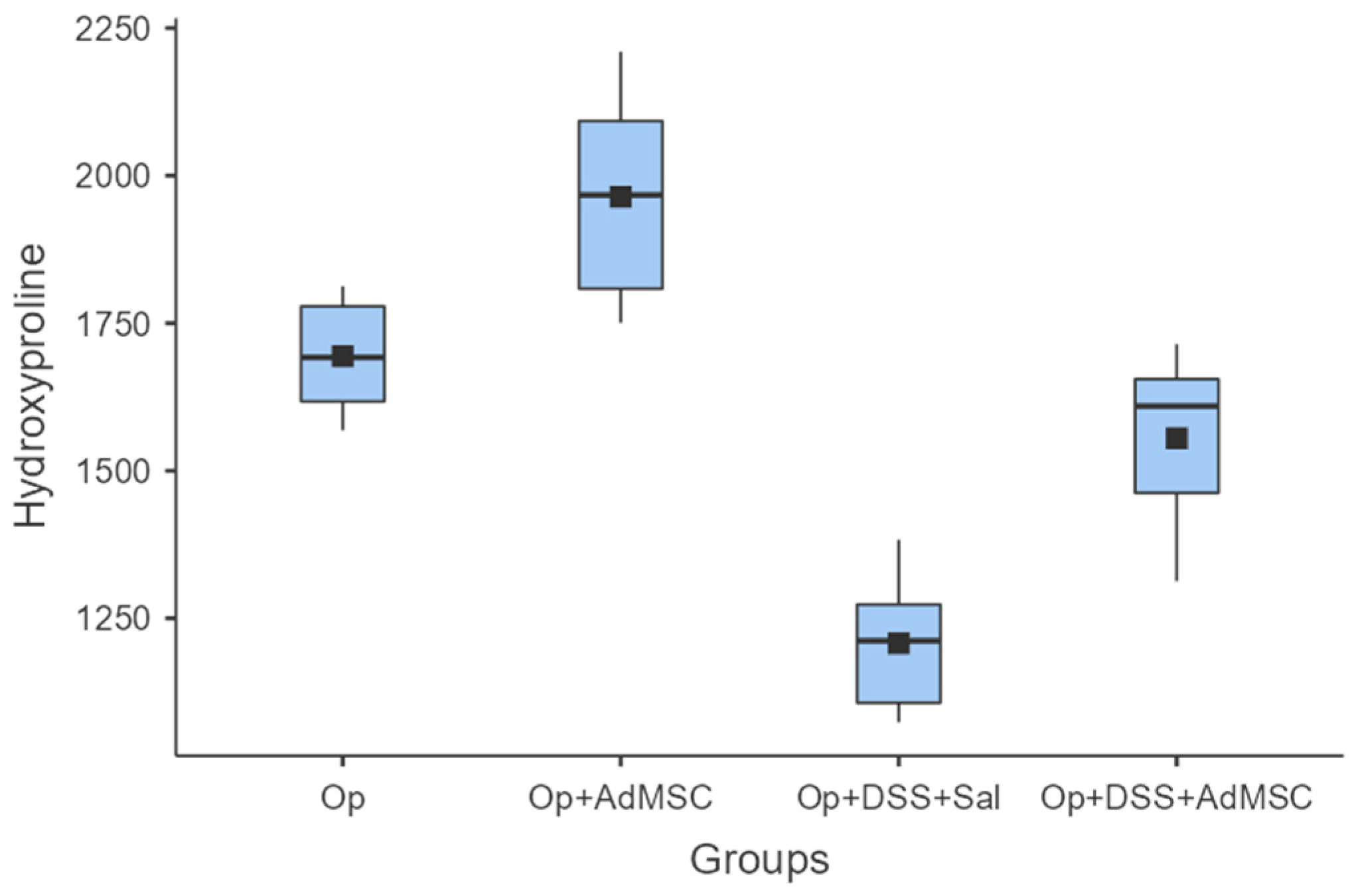
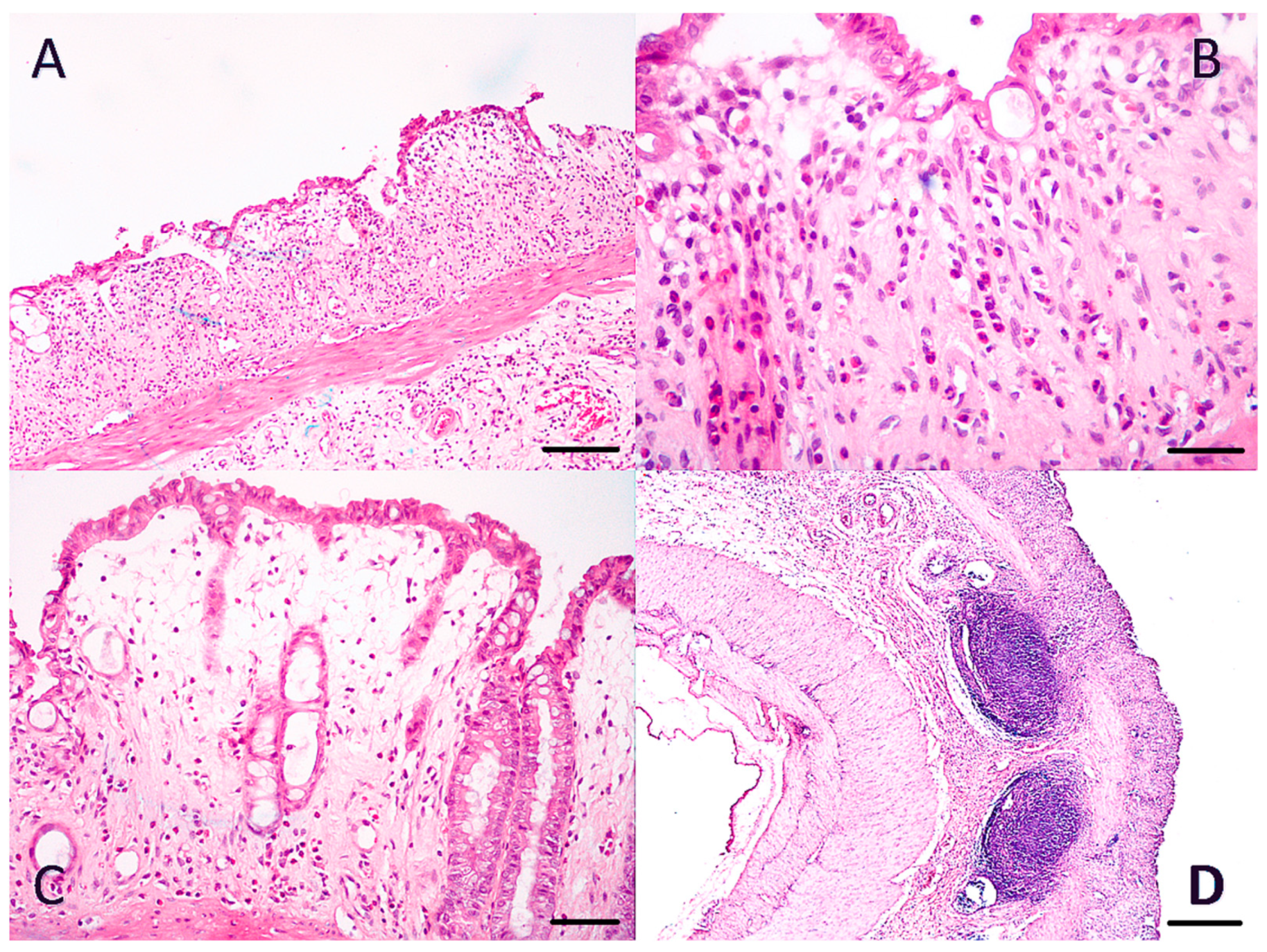
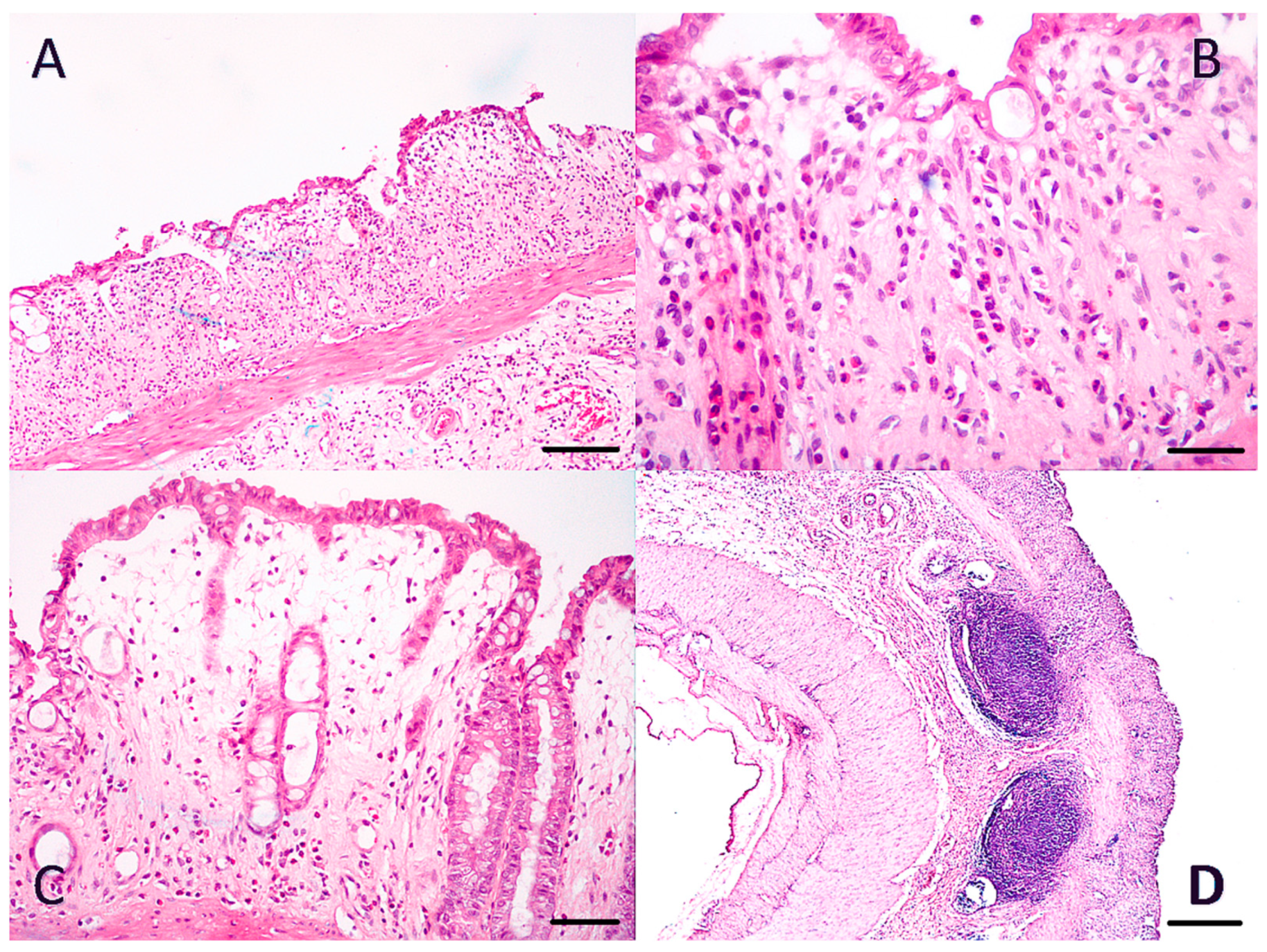
3.3. Anastomoses with AdMSCs Had More Collagen Deposition
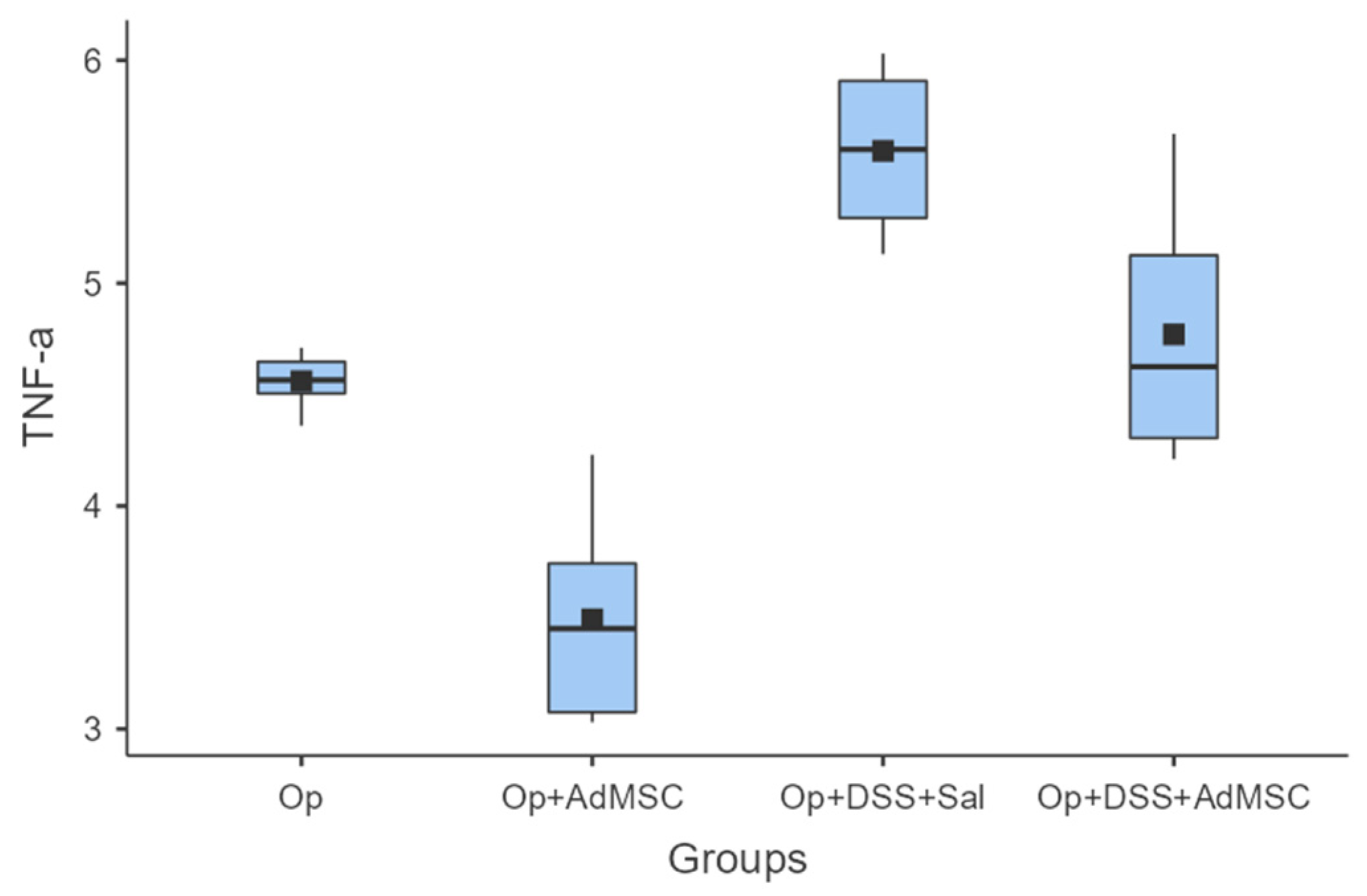
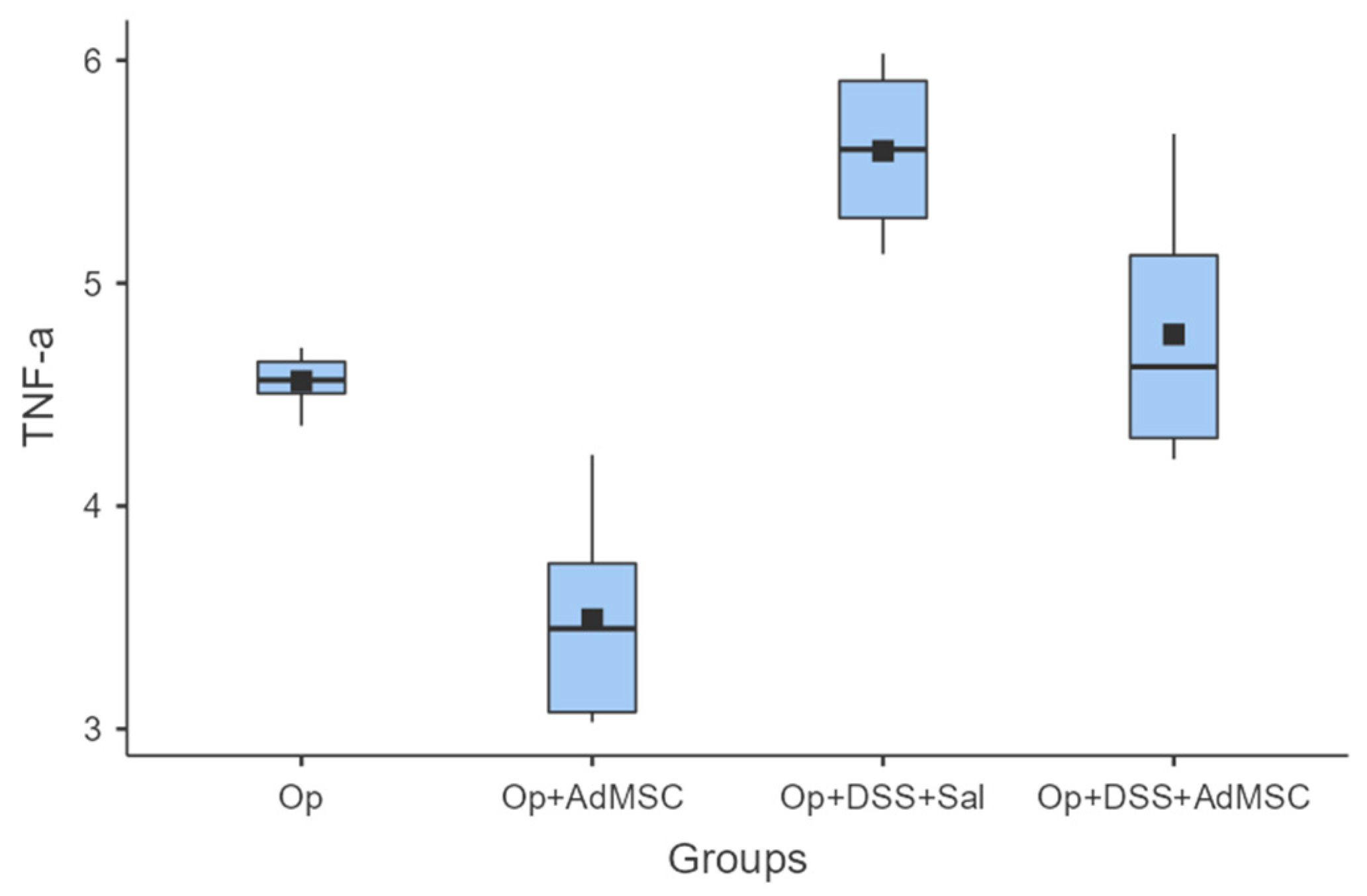
3.4. Pro-Inflammatory Cytokine Expression Is Downregulated in Groups That Received AdMSC
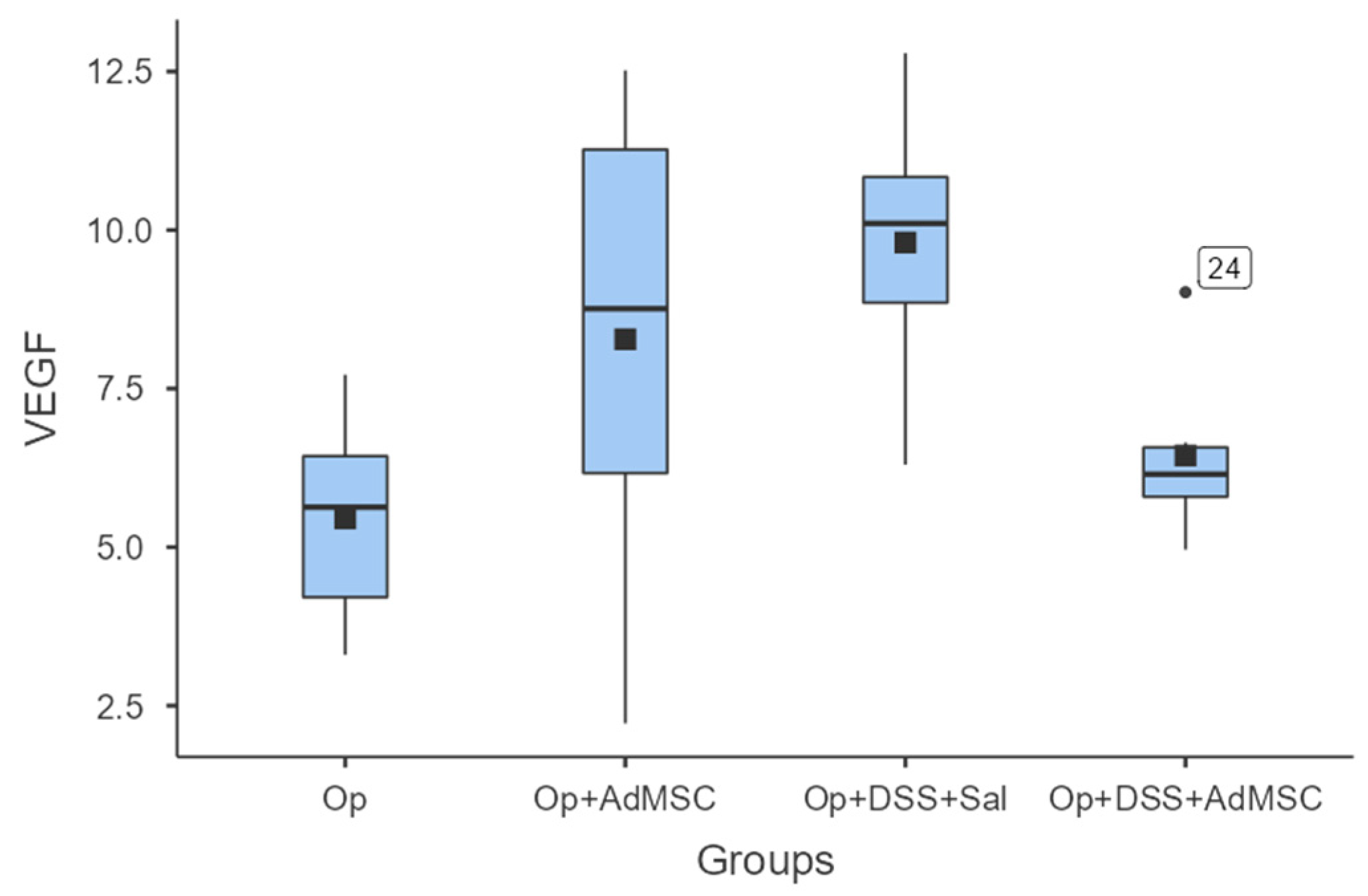
3.5. No Difference in Neo-Vascularization of the Anastomosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Solution |
|---|---|
| 1 | Citric acid buffer pH = 6.5 |
| 2 | 50% k-propanol |
| 3 | Chloramine-T, 0.056 M |
| 4 | NaOH 10.125 N |
| 5 | Ehrlich 1 M reagent |
| 6 | Acetic acid 0.5N |
| 7 | Collagen standard solution 1 mg/mL |
| Ascending Primer (5′–3′) | Descending Primer (5′–3′) | |
|---|---|---|
| TNF-a | TACTGAACTTCGG GGTGATCGGTCC | CAGCCTTGTCCCT TGAAGAGAACC |
| IL-6 | CAAGAGACTT CCAGCCAGTTG | TTGCCGAGTAGAC CTCATAGTGACC |
| VEGF | CGCCTTGGCT TGTCACATC | GTCGGAGAGC AACGTCACTA |
| GAPDH | ACCACAGTC CATGCCATCAC | TCCACCACC CTGTTGCTGTA |


Appendix B
| Groups | Mean | Median | SD | Min | Max |
|---|---|---|---|---|---|
| A Op | 2.33 | 2 | 0.516 | 2 | 3 |
| B Op + AdMSC | 1.50 | 1.5 | 0.548 | 1 | 2 |
| C Op + DSS + Sal | 4.50 | 4 | 0.837 | 4 | 6 |
| D Op + DSS + AdMSC | 3.17 | 3 | 0.753 | 2 | 4 |
| Groups | Mean | Median | SD | Min | Max |
|---|---|---|---|---|---|
| A Op | 243 | 240 | 28.0 | 210 | 280 |
| B Op + AdMSC | 307 | 295 | 58.9 | 240 | 410 |
| C Op + DSS + Sal | 165 | 165 | 18.7 | 140 | 190 |
| D Op + DSS + AdMSC | 215 | 225 | 33.9 | 170 | 260 |
| Groups | Mean | Median | SD | Min | Max |
|---|---|---|---|---|---|
| A Op | 1694 | 1692 | 103 | 1568 | 1813 |
| B Op + AdMSC | 1964 | 1967 | 186 | 1751 | 2210 |
| C Op + DSS + Sal | 1208 | 1212 | 120 | 1074 | 1383 |
| D Op + DSS + AdMSC | 1555 | 1609 | 155 | 1313 | 1715 |
| Groups | Mean | Median | SD | Min | Max |
|---|---|---|---|---|---|
| A Op | 7.60 | 7.63 | 0.831 | 6.55 | 8.77 |
| B Op + AdMSC | 6.20 | 6.34 | 0.626 | 5.36 | 7.08 |
| C Op + DSS + Sal | 9.61 | 9.59 | 0.925 | 8.59 | 10.73 |
| D Op + DSS + AdMSC | 8.33 | 8.45 | 0.919 | 7.11 | 9.30 |
| Groups | Mean | Median | SD | Min | Max |
|---|---|---|---|---|---|
| A Op | 4.56 | 4.56 | 0.126 | 4.36 | 4.71 |
| B Op + AdMSC | 3.49 | 3.45 | 0.485 | 3.03 | 4.23 |
| C Op + DSS + Sal | 5.59 | 5.60 | 0.381 | 5.13 | 6.03 |
| D Op + DSS + AdMSC | 4.77 | 4.63 | 0.584 | 4.21 | 5.67 |
| Groups | Mean | Median | SD | Min | Max |
|---|---|---|---|---|---|
| A Op | 5.45 | 5.63 | 1.67 | 3.30 | 7.72 |
| B Op + AdMSC | 8.28 | 8.76 | 3.91 | 2.22 | 12.52 |
| C Op + DSS + Sal | 8.94 | 8.89 | 2.62 | 5.30 | 12.79 |
| D Op + DSS + AdMSC | 6.10 | 6.14 | 2.03 | 3.84 | 9.54 |
References
- Ananthakrishnan, A.N. Epidemiology and Risk Factors for IBD. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 205. [Google Scholar] [CrossRef] [PubMed]
- Burisch, J.; Munkholm, P. The Epidemiology of Inflammatory Bowel Disease. Scand. J. Gastroenterol. 2015, 50, 942–951. [Google Scholar] [CrossRef] [PubMed]
- Kamat, N.; Ganesh Pai, C.; Surulivel Rajan, M.; Kamath, A. Cost of Illness in Inflammatory Bowel Disease. Dig. Dis. Sci. 2017, 62, 2318–2326. [Google Scholar] [CrossRef]
- Malik, T.A. Inflammatory Bowel Disease. Surg. Clin. N. Am. 2015, 95, 1105–1122. [Google Scholar] [CrossRef] [PubMed]
- Tekkis, P.P.; Purkayastha, S.; Lanitis, S.; Athanasiou, T.; Heriot, A.G.; Orchard, T.R.; Nicholls, R.J.; Darzi, A.W. A Comparison of Segmental vs Subtotal/Total Colectomy for Colonic Crohn’s Disease: A Meta-Analysis. Color. Dis. 2006, 8, 82–90. [Google Scholar] [CrossRef]
- Gallo, G.; Kotze, P.G.; Spinelli, A. Surgery in Ulcerative Colitis: When? How? Best Pract. Res. Clin. Gastroenterol. 2018, 32–33, 71–78. [Google Scholar] [CrossRef]
- Forbes, G.M. Mesenchymal Stromal Cell Therapy in Crohn’s Disease. Dig. Dis. 2017, 35, 115–122. [Google Scholar] [CrossRef]
- Yuan, Y.; Ni, S.; Zhuge, A.; Li, L.; Li, B. Adipose-Derived Mesenchymal Stem Cells Reprogram M1 Macrophage Metabolism via PHD2/HIF-1α Pathway in Colitis Mice. Front. Immunol. 2022, 13, 859806. [Google Scholar] [CrossRef]
- Ko, J.Z.-H.; Johnson, S.; Dave, M. Efficacy and Safety of Mesenchymal Stem/Stromal Cell Therapy for Inflammatory Bowel Diseases: An Up-to-Date Systematic Review. Biomolecules 2021, 11, 82. [Google Scholar] [CrossRef]
- Hu, Q.; Lyon, C.J.; Fletcher, J.K.; Tang, W.; Wan, M.; Hu, T.Y. Extracellular Vesicle Activities Regulating Macrophage- and Tissue-Mediated Injury and Repair Responses. Acta Pharm. Sin. B 2021, 11, 1493–1512. [Google Scholar] [CrossRef]
- Gómez-Ferrer, M.; Amaro-Prellezo, E.; Dorronsoro, A.; Sánchez-Sánchez, R.; Vicente, Á.; Cosín-Roger, J.; Barrachina, M.D.; Baquero, M.C.; Valencia, J.; Sepúlveda, P. HIF-Overexpression and Pro-Inflammatory Priming in Human Mesenchymal Stromal Cells Improves the Healing Properties of Extracellular Vesicles in Experimental Crohn’s Disease. Int. J. Mol. Sci. 2021, 22, 11269. [Google Scholar] [CrossRef]
- Arabpour, M.; Saghazadeh, A.; Rezaei, N. Anti-Inflammatory and M2 Macrophage Polarization-Promoting Effect of Mesenchymal Stem Cell-Derived Exosomes. Int. Immunopharmacol. 2021, 97, 107823. [Google Scholar] [CrossRef]
- Song, W.-J.; Li, Q.; Ryu, M.-O.; Ahn, J.-O.; Bhang, D.H.; Jung, Y.C.; Youn, H.-Y. TSG-6 Released from Intraperitoneally Injected Canine Adipose Tissue-Derived Mesenchymal Stem Cells Ameliorate Inflammatory Bowel Disease by Inducing M2 Macrophage Switch in Mice. Stem Cell Res. Ther. 2018, 9, 91. [Google Scholar] [CrossRef] [PubMed]
- Park, H.J.; Kim, J.; Saima, F.T.; Rhee, K.-J.; Hwang, S.; Kim, M.Y.; Baik, S.K.; Eom, Y.W.; Kim, H.-S. Adipose-Derived Stem Cells Ameliorate Colitis by Suppression of Inflammasome Formation and Regulation of M1-Macrophage Population through Prostaglandin E2. Biochem. Biophys. Res. Commun. 2018, 498, 988–995. [Google Scholar] [CrossRef]
- Luz-Crawford, P.; Djouad, F.; Toupet, K.; Bony, C.; Franquesa, M.; Hoogduijn, M.J.; Jorgensen, C.; Noël, D. Mesenchymal Stem Cell-Derived Interleukin 1 Receptor Antagonist Promotes Macrophage Polarization and Inhibits B Cell Differentiation. Stem Cells 2016, 34, 483–492. [Google Scholar] [CrossRef]
- Abumaree, M.H.; Al Jumah, M.A.; Kalionis, B.; Jawdat, D.; Al Khaldi, A.; Abomaray, F.M.; Fatani, A.S.; Chamley, L.W.; Knawy, B.A. Human Placental Mesenchymal Stem Cells (pMSCs) Play a Role as Immune Suppressive Cells by Shifting Macrophage Differentiation from Inflammatory M1 to Anti-Inflammatory M2 Macrophages. Stem Cell Rev. Rep. 2013, 9, 620–641. [Google Scholar] [CrossRef]
- Wang, S.; Lei, B.; Zhang, E.; Gong, P.; Gu, J.; He, L.; Han, L.; Yuan, Z. Targeted Therapy for Inflammatory Diseases with Mesenchymal Stem Cells and Their Derived Exosomes: From Basic to Clinics. Int. J. Nanomed. 2022, 17, 1757–1781. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Xue, H.; Tan, J.; Liu, P.; Qiao, C.; Pang, C.; Zhang, L. Bone Marrow Mesenchymal Stem Cells-Derived Exosomes Containing miR-539-5p Inhibit Pyroptosis through NLRP3/Caspase-1 Signalling to Alleviate Inflammatory Bowel Disease. Inflamm. Res. 2022, 71, 833–846. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.; Odenthal, M.; Fries, J.W.U. Exosomes as miRNA Carriers: Formation-Function-Future. Int. J. Mol. Sci. 2016, 17, 2028. [Google Scholar] [CrossRef]
- Yang, S.; Liang, X.; Song, J.; Li, C.; Liu, A.; Luo, Y.; Ma, H.; Tan, Y.; Zhang, X. A Novel Therapeutic Approach for Inflammatory Bowel Disease by Exosomes Derived from Human Umbilical Cord Mesenchymal Stem Cells to Repair Intestinal Barrier via TSG-6. Stem Cell Res. Ther. 2021, 12, 315. [Google Scholar] [CrossRef]
- Shen, Z.; Huang, W.; Liu, J.; Tian, J.; Wang, S.; Rui, K. Effects of Mesenchymal Stem Cell-Derived Exosomes on Autoimmune Diseases. Front. Immunol. 2021, 12, 749192. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Liang, Z.; Wang, F.; Zhou, C.; Zheng, X.; Hu, T.; He, X.; Wu, X.; Lan, P. Exosomes from Mesenchymal Stromal Cells Reduce Murine Colonic Inflammation via a Macrophage-Dependent Mechanism. JCI Insight 2019, 4, e131273. [Google Scholar] [CrossRef]
- Wang, G.; Yuan, J.; Cai, X.; Xu, Z.; Wang, J.; Ocansey, D.K.W.; Yan, Y.; Qian, H.; Zhang, X.; Xu, W.; et al. HucMSC-exosomes Carrying miR-326 Inhibit Neddylation to Relieve Inflammatory Bowel Disease in Mice. Clin. Transl. Med. 2020, 10, e113. [Google Scholar] [CrossRef]
- Sun, Z.; Shi, K.; Yang, S.; Liu, J.; Zhou, Q.; Wang, G.; Song, J.; Li, Z.; Zhang, Z.; Yuan, W. Effect of Exosomal miRNA on Cancer Biology and Clinical Applications. Mol. Cancer 2018, 17, 147. [Google Scholar] [CrossRef] [PubMed]
- Heidari, M.; Pouya, S.; Baghaei, K.; Aghdaei, H.A.; Namaki, S.; Zali, M.R.; Hashemi, S.M. The Immunomodulatory Effects of Adipose-derived Mesenchymal Stem Cells and Mesenchymal Stem Cells-conditioned Medium in Chronic Colitis. J. Cell. Physiol. 2018, 233, 8754–8766. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Zhang, Z.; Yuan, J.; Ocansey, D.K.W.; Tu, Q.; Zhang, X.; Qian, H.; Xu, W.; Qiu, W.; Mao, F. hucMSC-Derived Exosomes Attenuate Colitis by Regulating Macrophage Pyroptosis via the miR-378a-5p/NLRP3 Axis. Stem Cell Res. Ther. 2021, 12, 416. [Google Scholar] [CrossRef]
- Cao, Y.; Ding, Z.; Han, C.; Shi, H.; Cui, L.; Lin, R. Efficacy of Mesenchymal Stromal Cells for Fistula Treatment of Crohn’s Disease: A Systematic Review and Meta-Analysis. Dig. Dis. Sci. 2017, 62, 851–860. [Google Scholar] [CrossRef]
- Garcia-Olmo, D.; Garcia-Arranz, M.; Herreros, D. Expanded Adipose-Derived Stem Cells for the Treatment of Complex Perianal Fistula Including Crohn’s Disease. Expert Opin. Biol. Ther. 2008, 8, 1417–1423. [Google Scholar] [CrossRef]
- Ciccocioppo, R.; Gallia, A.; Sgarella, A.; Kruzliak, P.; Gobbi, P.G.; Corazza, G.R. Long-Term Follow-Up of Crohn Disease Fistulas After Local Injections of Bone Marrow-Derived Mesenchymal Stem Cells. Mayo Clin. Proc. 2015, 90, 747–755. [Google Scholar] [CrossRef]
- Molendijk, I.; Bonsing, B.A.; Roelofs, H.; Peeters, K.C.M.J.; Wasser, M.N.J.M.; Dijkstra, G.; van der Woude, C.J.; Duijvestein, M.; Veenendaal, R.A.; Zwaginga, J.-J.; et al. Allogeneic Bone Marrow-Derived Mesenchymal Stromal Cells Promote Healing of Refractory Perianal Fistulas in Patients With Crohn’s Disease. Gastroenterology 2015, 149, 918–927.e6. [Google Scholar] [CrossRef]
- Duijvestein, M.; Vos, A.C.W.; Roelofs, H.; Wildenberg, M.E.; Wendrich, B.B.; Verspaget, H.W.; Kooy-Winkelaar, E.M.C.; Koning, F.; Zwaginga, J.J.; Fidder, H.H.; et al. Autologous Bone Marrow-Derived Mesenchymal Stromal Cell Treatment for Refractory Luminal Crohn’s Disease: Results of a Phase I Study. Gut 2010, 59, 1662–1669. [Google Scholar] [CrossRef] [PubMed]
- García-Olmo, D.; García-Arranz, M.; Herreros, D.; Pascual, I.; Peiro, C.; Rodríguez-Montes, J.A. A Phase I Clinical Trial of the Treatment of Crohn’s Fistula by Adipose Mesenchymal Stem Cell Transplantation. Dis. Colon Rectum 2005, 48, 1416–1423. [Google Scholar] [CrossRef]
- Dave, M.; Mehta, K.; Luther, J.; Baruah, A.; Dietz, A.B.; Faubion, W.A. Mesenchymal Stem Cell Therapy for Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Inflamm. Bowel Dis. 2015, 21, 2696–2707. [Google Scholar] [CrossRef]
- Van de Putte, D.; Demarquay, C.; Van Daele, E.; Moussa, L.; Vanhove, C.; Benderitter, M.; Ceelen, W.; Pattyn, P.; Mathieu, N. Adipose-Derived Mesenchymal Stromal Cells Improve the Healing of Colonic Anastomoses Following High Dose of Irradiation Through Anti-Inflammatory and Angiogenic Processes. Cell Transplant. 2017, 26, 1919–1930. [Google Scholar] [CrossRef] [PubMed]
- Pascual, I.; Fernández de Miguel, G.; García Arranz, M.; García-Olmo, D. Biosutures Improve Healing of Experimental Weak Colonic Anastomoses. Int. J. Color. Dis. 2010, 25, 1447–1451. [Google Scholar] [CrossRef] [PubMed]
- Adas, G.; Kemik, O.; Eryasar, B.; Okcu, A.; Adas, M.; Arikan, S.; Erman, G.; Kemik, A.S.; Kamali, G.; Dogan, Y.; et al. Treatment of Ischemic Colonic Anastomoses with Systemic Transplanted Bone Marrow Derived Mesenchymal Stem Cells. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 2275–2285. [Google Scholar]
- Adas, G.; Arikan, S.; Karatepe, O.; Kemik, O.; Ayhan, S.; Karaoz, E.; Kamali, G.; Eryasar, B.; Ustek, D. Mesenchymal Stem Cells Improve the Healing of Ischemic Colonic Anastomoses (Experimental Study). Langenbeck’s Arch. Surg. 2011, 396, 115–126. [Google Scholar] [CrossRef]
- Yoo, J.H.; Shin, J.H.; An, M.S.; Ha, T.K.; Kim, K.H.; Bae, K.B.; Kim, T.H.; Choi, C.S.; Hong, K.H.; Kim, J.; et al. Adipose-Tissue-Derived Stem Cells Enhance the Healing of Ischemic Colonic Anastomoses: An Experimental Study in Rats. J. Korean Soc. Coloproctol. 2012, 28, 132. [Google Scholar] [CrossRef]
- Morgan, A.; Zheng, A.; Linden, K.M.; Zhang, P.; Brown, S.A.; Carpenter, J.P.; Spitz, F.R.; Kwiatt, M.E. Locally Transplanted Adipose Stem Cells Reduce Anastomotic Leaks in Ischemic Colorectal Anastomoses: A Rat Model. Dis. Colon Rectum 2020, 63, 955–964. [Google Scholar] [CrossRef]
- Alvarenga, V.; da Silva, P.T.; Bonfá, N.D.; Pêgo, B.; Nanini, H.; Bernardazzi, C.; Madi, K.; Baetas da Cruz, W.; Castelo-Branco, M.T.; de Souza, H.S.P.; et al. Protective Effect of Adipose Tissue–Derived Mesenchymal Stromal Cells in an Experimental Model of High-Risk Colonic Anastomosis. Surgery 2019, 166, 914–925. [Google Scholar] [CrossRef]
- The ARRIVE Guidelines 2.0. Available online: https://arriveguidelines.org/arrive-guidelines (accessed on 23 July 2022).
- Perše, M.; Cerar, A. Dextran Sodium Sulphate Colitis Mouse Model: Traps and Tricks. J. Biomed. Biotechnol. 2012, 2012, 718617. [Google Scholar] [CrossRef] [PubMed]
- Perry, T.; Laffin, M.; Fedorak, R.N.; Thiesen, A.; Dicken, B.; Madsen, K.L. Ileocolic Resection Is Associated with Increased Susceptibility to Injury in a Murine Model of Colitis. PLoS ONE 2017, 12, e0184660. [Google Scholar] [CrossRef] [PubMed]
- Perry, T.; Borowiec, A.; Dicken, B.; Fedorak, R.; Madsen, K. Murine Ileocolic Bowel Resection with Primary Anastomosis. J. Vis. Exp. 2014, 92, e52106. [Google Scholar] [CrossRef]
- Karagergou, E.; Dionyssopoulos, A.; Karayannopoulou, M.; Psalla, D.; Theodoridis, A.; Demiri, E.; Koliakos, G. Adipose-Derived Stromal Vascular Fraction Aids Epithelialisation and Angiogenesis in an Animal Model. J. Wound Care 2018, 27, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Eichele, D.D.; Kharbanda, K.K. Dextran Sodium Sulfate Colitis Murine Model: An Indispensable Tool for Advancing Our Understanding of Inflammatory Bowel Diseases Pathogenesis. World J. Gastroenterol. 2017, 23, 6016–6029. [Google Scholar] [CrossRef]
- Bosmans, J.W.A.M.; Moossdorff, M.; Al-Taher, M.; van Beek, L.; Derikx, J.P.M.; Bouvy, N.D. International Consensus Statement Regarding the Use of Animal Models for Research on Anastomoses in the Lower Gastrointestinal Tract. Int. J. Color. Dis. 2016, 31, 1021–1030. [Google Scholar] [CrossRef]
- Pramateftakis, M.G.; Kanellos, D.; Mantzoros, I.; Despoudi, K.; Raptis, D.; Angelopoulos, S.; Koliakos, G.; Zaraboukas, T.; Lazaridis, C. Intraperitoneally Administered Irinotecan with 5-Fluorouracil Impair Wound Healing of Colonic Anastomoses in a Rat Model: An Experimental Study. Tech. Coloproctol. 2011, 15, 121–125. [Google Scholar] [CrossRef]
- Cihan, A.; Armutcu, F.; Uçan, B.H.; Acun, Z.; Numanoglu, V.K.; Gürel, A.; Ulukent, S.C. Comparison of the Measurement Methods of Bursting Pressure of Intestinal Anastomoses. Hepatogastroenterology 2003, 50 (Suppl. S2), ccxxxii–ccxxxiv. [Google Scholar]
- Sukho, P.; Boersema, G.S.A.; Kops, N.; Lange, J.F.; Kirpensteijn, J.; Hesselink, J.W.; Bastiaansen-Jenniskens, Y.M.; Verseijden, F. Transplantation of Adipose Tissue-Derived Stem Cell Sheet to Reduce Leakage After Partial Colectomy in A Rat Model. J. Vis. Exp. 2018, 138, e57213. [Google Scholar] [CrossRef]
- Lourenssen, S.R.; Blennerhassett, M.G. M2 Macrophages and Phenotypic Modulation of Intestinal Smooth Muscle Cells Characterize Inflammatory Stricture Formation in Rats. Am. J. Pathol. 2020, 190, 1843–1858. [Google Scholar] [CrossRef]
- Duffield, J.S.; Lupher, M.; Thannickal, V.J.; Wynn, T.A. Host Responses in Tissue Repair and Fibrosis. Annu. Rev. Pathol. Mech. Dis. 2013, 8, 241–276. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.-H.; Huang, B.-S.; Horng, H.-C.; Yeh, C.-C.; Chen, Y.-J. Wound Healing. J. Chin. Med. Assoc. 2018, 81, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Biswas, S.K.; Galdiero, M.R.; Sica, A.; Locati, M. Macrophage Plasticity and Polarization in Tissue Repair and Remodelling. J. Pathol. 2013, 229, 176–185. [Google Scholar] [CrossRef]
- Mantovani, A.; Sica, A.; Locati, M. Macrophage Polarization Comes of Age. Immunity 2005, 23, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Davies, L.C.; Jenkins, S.J.; Allen, J.E.; Taylor, P.R. Tissue-Resident Macrophages. Nat. Immunol. 2013, 14, 986–995. [Google Scholar] [CrossRef]
- Hidalgo-Garcia, L.; Galvez, J.; Rodriguez-Cabezas, M.E.; Anderson, P.O. Can a Conversation Between Mesenchymal Stromal Cells and Macrophages Solve the Crisis in the Inflamed Intestine? Front. Pharmacol. 2018, 9, 179. [Google Scholar] [CrossRef]
- Gonzalez-Rey, E.; Anderson, P.; Gonzalez, M.A.; Rico, L.; Buscher, D.; Delgado, M. Human Adult Stem Cells Derived from Adipose Tissue Protect against Experimental Colitis and Sepsis. Gut 2009, 58, 929–939. [Google Scholar] [CrossRef]
- Tadauchi, A.; Narita, Y.; Kagami, H.; Niwa, Y.; Ueda, M.; Goto, H. Novel Cell-Based Therapeutic Strategy for Ischemic Colitis with Use of Bone Marrow-Derived Mononuclear Cells in Rats. Dis. Colon Rectum 2009, 52, 1443–1451. [Google Scholar] [CrossRef]
- Castelo-Branco, M.T.L.; Soares, I.D.P.; Lopes, D.V.; Buongusto, F.; Martinusso, C.A.; do Rosario, A.; Souza, S.A.L.; Gutfilen, B.; Fonseca, L.M.B.; Elia, C.; et al. Intraperitoneal but Not Intravenous Cryopreserved Mesenchymal Stromal Cells Home to the Inflamed Colon and Ameliorate Experimental Colitis. PLoS ONE 2012, 7, e33360. [Google Scholar] [CrossRef]
- Lee, R.H.; Pulin, A.A.; Seo, M.J.; Kota, D.J.; Ylostalo, J.; Larson, B.L.; Semprun-Prieto, L.; Delafontaine, P.; Prockop, D.J. Intravenous hMSCs Improve Myocardial Infarction in Mice Because Cells Embolized in Lung Are Activated to Secrete the Anti-Inflammatory Protein TSG-6. Cell Stem Cell 2009, 5, 54–63. [Google Scholar] [CrossRef]
- Yu, W.; Zhou, H.; Feng, X.; Liang, X.; Wei, D.; Xia, T.; Yang, B.; Yan, L.; Zhao, X.; Liu, H. Mesenchymal Stem Cell Secretome-Loaded Fibrin Glue Improves the Healing of Intestinal Anastomosis. Front. Bioeng. Biotechnol. 2023, 11, 1103709. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-R.; Kim, J.-W.; Jun, H.-S.; Roh, J.Y.; Lee, H.-Y.; Hong, I.-S. Stem Cell Secretome and Its Effect on Cellular Mechanisms Relevant to Wound Healing. Mol. Ther. 2018, 26, 606–617. [Google Scholar] [CrossRef] [PubMed]
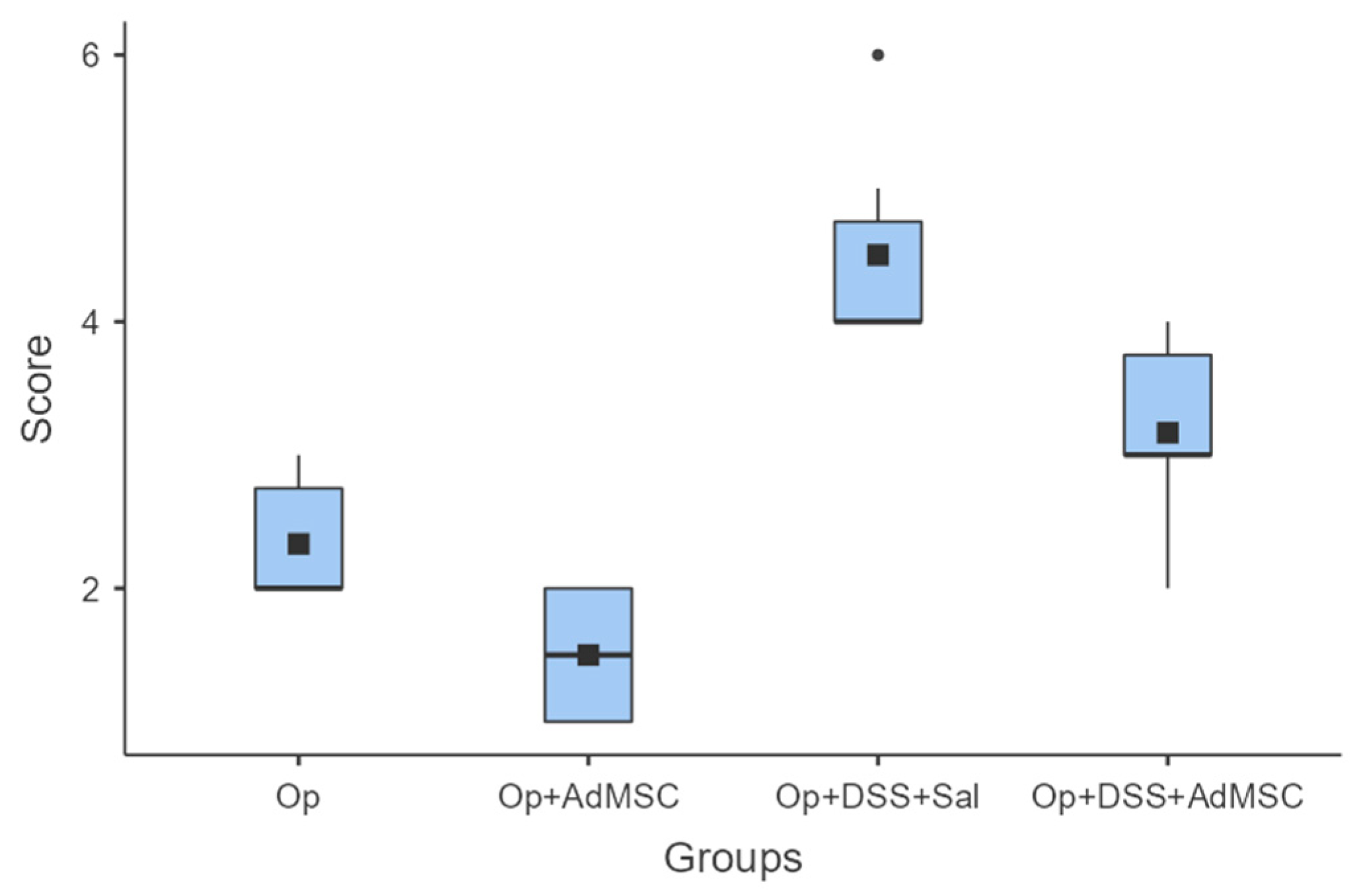


| Anastomotic Complication Score | |
|---|---|
| 0 | No adhesions or abnormalities |
| 1 | Adhesion to fat pad, clean anastomosis underneath |
| 2 | Adhesion to intestinal loop, abdominal wall or other organ |
| 3 | Anastomotic defect found underneath adhesion, no other abnormalities |
| 4 | Signs of possible contamination (e.g., small abscesses) |
| 5 | Clear anastomotic complication; free pus, obstruction, signs of peritonitis |
| 6 | Fecal peritonitis/Death due to peritonitis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ntampakis, G.; Pramateftakis, M.-G.; Ioannidis, O.; Bitsianis, S.; Christidis, P.; Symeonidis, S.; Koliakos, G.; Karakota, M.; Bekiari, C.; Tsakona, A.; et al. The Role of Adipose Tissue Mesenchymal Stem Cells in Colonic Anastomosis Healing in Inflammatory Bowel Disease: Experimental Study in Rats. J. Clin. Med. 2023, 12, 6336. https://doi.org/10.3390/jcm12196336
Ntampakis G, Pramateftakis M-G, Ioannidis O, Bitsianis S, Christidis P, Symeonidis S, Koliakos G, Karakota M, Bekiari C, Tsakona A, et al. The Role of Adipose Tissue Mesenchymal Stem Cells in Colonic Anastomosis Healing in Inflammatory Bowel Disease: Experimental Study in Rats. Journal of Clinical Medicine. 2023; 12(19):6336. https://doi.org/10.3390/jcm12196336
Chicago/Turabian StyleNtampakis, Georgios, Manousos-Georgios Pramateftakis, Orestis Ioannidis, Stefanos Bitsianis, Panagiotis Christidis, Savvas Symeonidis, Georgios Koliakos, Maria Karakota, Chrysanthi Bekiari, Anastasia Tsakona, and et al. 2023. "The Role of Adipose Tissue Mesenchymal Stem Cells in Colonic Anastomosis Healing in Inflammatory Bowel Disease: Experimental Study in Rats" Journal of Clinical Medicine 12, no. 19: 6336. https://doi.org/10.3390/jcm12196336
APA StyleNtampakis, G., Pramateftakis, M.-G., Ioannidis, O., Bitsianis, S., Christidis, P., Symeonidis, S., Koliakos, G., Karakota, M., Bekiari, C., Tsakona, A., Cheva, A., & Aggelopoulos, S. (2023). The Role of Adipose Tissue Mesenchymal Stem Cells in Colonic Anastomosis Healing in Inflammatory Bowel Disease: Experimental Study in Rats. Journal of Clinical Medicine, 12(19), 6336. https://doi.org/10.3390/jcm12196336