
Multimodal Imaging of Cancer Therapy-Related Cardiac Dysfunction in Breast Cancer—A State-of-the-Art Review


Abstract
:1. Introduction
1.1. Cardiotoxicity
1.2. HER2 Agents
1.3. Tyrosine Kinase Inhibitors
1.4. Anthracyclines
1.5. Alkylating Agents
1.6. Radiotherapy
1.7. Multimodal Imaging
1.8. Echocardiography
1.9. Magnetic Resonance Imaging
1.10. Cardiac Computed Tomography
1.11. Nuclear Imaging
1.12. Cardiac Biomarkers
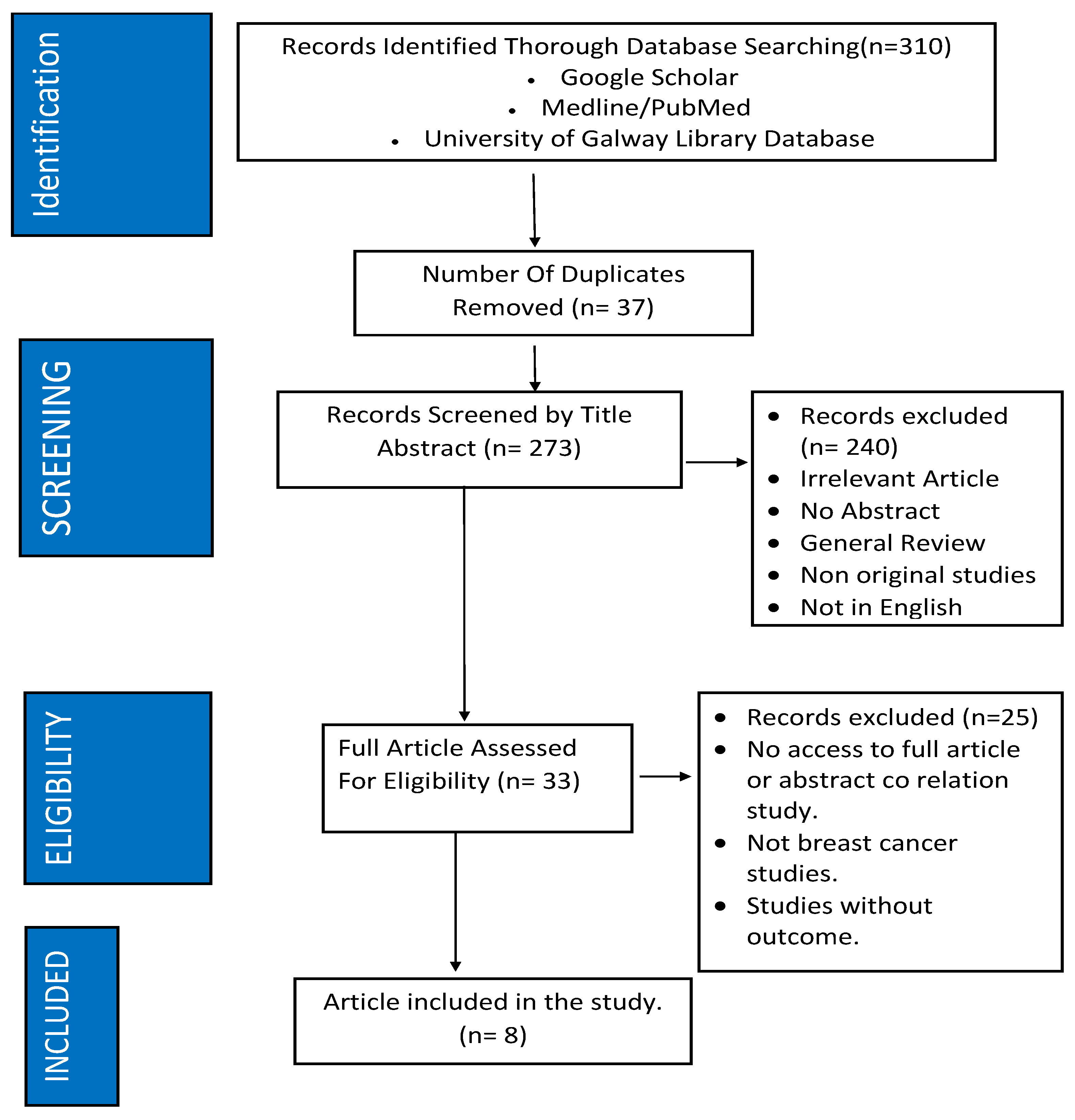
2. Materials and Methods
3. Results
4. Discussion
Gaps in the Literature
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Plana, J.C.; Galderisi, M.; Barac, A.; Ewer, M.S.; Ky, B.; Scherrer-Crosbie, M.; Ganame, J.; Sebag, I.A.; Agler, D.A.; Badano, L.P.; et al. Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2014, 27, 911–939. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Cardinale, D.; Dent, S.; Criscitiello, C.; Aseyev, O.; Lenihan, D.; Cipolla, C.M. Cardiotoxicity of anticancer treatments: Epidemiology, detection, and management. CA Cancer J. Clin. 2016, 66, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Seidman, A.; Hudis, C.; Pierri, M.K.; Shak, S.; Paton, V.; Ashby, M.; Murphy, M.; Stewart, S.J.; Keefe, D. Cardiac dysfunction in the trastuzumab clinical trials experience. J. Clin. Oncol. 2002, 20, 1215–1221. [Google Scholar] [CrossRef] [PubMed]
- Ewer, M.S.; Ewer, S.M. Cardiotoxicity of anticancer treatments. Nat. Rev. Cardiol. 2015, 12, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Mohan, N.; Shen, Y.; Endo, Y.; ElZarrad, M.K.; Wu, W.J. Trastuzumab, but Not Pertuzumab, Dysregulates HER2 Signaling to Mediate Inhibition of Autophagy and Increase in Reactive Oxygen Species Production in Human Cardiomyocytes. Mol. Cancer Ther. 2016, 15, 1321–1331. [Google Scholar] [CrossRef]
- Udagawa, C.; Nakamura, H.; Ohnishi, H.; Tamura, K.; Shimoi, T.; Yoshida, M.; Yoshida, T.; Totoki, Y.; Shibata, T.; Zembutsu, H. Whole exome sequencing to identify genetic markers for trastuzumab-induced cardiotoxicity. Cancer Sci. 2018, 109, 446–452. [Google Scholar] [CrossRef]
- Pituskin, E.; Mackey, J.R.; Koshman, S.; Jassal, D.; Pitz, M.; Haykowsky, M.J.; Pagano, J.J.; Chow, K.; Thompson, R.B.; Vos, L.J.; et al. Multidisciplinary approach to novel therapies in cardio-oncology research (MANTICORE 101–Breast): A randomized trial for the prevention of trastuzumab-associated cardiotoxicity. J. Clin. Oncol. 2017, 35, 870–877. [Google Scholar] [CrossRef]
- Buzdar, A.U.; Ibrahim, N.K.; Francis, D.; Booser, D.J.; Thomas, E.S.; Theriault, R.L.; Pusztai, L.; Green, M.C.; Arun, B.K.; Giordano, S.H.; et al. Significantly higher pathologic complete remission rate after neoadjuvant therapy with trastuzumab, paclitaxel, and epirubicin chemotherapy: Results of a randomized trial in human epidermal growth factor receptor 2–positive operable breast cancer. J. Clin. Oncol. 2005, 23, 3676–3685. [Google Scholar] [CrossRef]
- Bowles, E.J.A.; Wellman, R.; Feigelson, H.S.; Onitilo, A.A.; Freedman, A.N.; Delate, T.; Allen, L.A.; Nekhlyudov, L.; Goddard, K.A.B.; Davis, R.L.; et al. Risk of heart failure in breast cancer patients after anthracycline and trastuzumab treatment: A Retrospective Cohort Study. JNCI J. Natl. Cancer Inst. 2012, 104, 1293–1305. [Google Scholar] [CrossRef]
- Perez, E.A.; Suman, V.J.; Davidson, N.E.; Sledge, G.W.; Kaufman, P.A.; Hudis, C.A.; Martino, S.; Gralow, J.R.; Dakhil, S.R.; Ingle, J.N.; et al. Cardiac safety analysis of doxorubicin and cyclophosphamide followed by paclitaxel with or without trastuzumab in the north central cancer treatment group N9831 adjuvant breast cancer trial. J. Clin. Oncol. 2008, 26, 1231–1238. [Google Scholar] [CrossRef]
- Ewer, M.S.; Vooletich, M.T.; Durand, J.-B.; Woods, M.L.; Davis, J.R.; Valero, V.; Lenihan, D.J. Reversibility of trastuzumab-related cardiotoxicity: New insights based on clinical course and response to medical treatment. J. Clin. Oncol. 2005, 23, 7820–7826. [Google Scholar] [CrossRef] [PubMed]
- Chu, T.F.; A Rupnick, M.; Kerkela, R.; Dallabrida, S.M.; Zurakowski, D.; Nguyen, L.; Woulfe, K.; Pravda, E.; Cassiola, F.; Desai, J.; et al. Cardiotoxicity associated with tyrosine kinase inhibitor sunitinib. Lancet 2007, 370, 2011–2019. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Qadir, H.; Ethier, J.-L.; Lee, D.S.; Thavendiranathan, P.; Amir, E.; Cardio-Oncology Outcomes Research Team. Cardiovascular toxicity of angiogenesis inhibitors in treatment of malignancy: A systematic review and meta-analysis. Cancer Treat. Rev. 2017, 53, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Moslehi, J.J.; Salem, J.-E.; A Sosman, J.; Lebrun-Vignes, B.; Johnson, D.B. Increased reporting of fatal immune checkpoint inhibitor-associated myocarditis. Lancet 2018, 391, 933. [Google Scholar] [CrossRef] [PubMed]
- Maitland, M.L.; Bakris, G.L.; Black, H.R.; Chen, H.X.; Durand, J.-B.; Elliott, W.J.; Ivy, S.P.; Leier, C.V.; Lindenfeld, J.; Liu, G.; et al. Initial assessment, surveillance, and management of blood pressure in patients receiving vascular endothelial growth factor signaling pathway inhibitors. JNCI J. Natl. Cancer Inst. 2010, 102, 596–604. [Google Scholar] [CrossRef]
- Barber, M.C.; Mauro, M.J.; Moslehi, J. Cardiovascular care of patients with chronic myeloid leukemia (CML) on tyrosine kinase inhibitor (TKI) therapy. Hematology 2017, 2017, 110–114. [Google Scholar] [CrossRef]
- Moslehi, J.J. Cardiovascular Toxic Effects of Targeted Cancer Therapies. N. Engl. J. Med. 2016, 375, 1457–1467. [Google Scholar] [CrossRef]
- Cardinale, D.; Iacopo, F.; Cipolla, C.M. Cardiotoxicity of Anthracyclines. Front. Cardiovasc. Med. 2020, 7, 26. [Google Scholar] [CrossRef]
- Curigliano, G.; Cardinale, D.; Suter, T.; Plataniotis, G.; de Azambuja, E.; Sandri, M.T.; Criscitiello, C.; Goldhirsch, A.; Cipolla, C.; Roila, F. Cardiovascular toxicity induced by chemotherapy, targeted agents and radiotherapy: ESMO Clinical Practice Guidelines. Ann. Oncol. 2012, 23 (Suppl. S7), vii155–vii166. [Google Scholar] [CrossRef]
- Takemura, G.; Fujiwara, H. Doxorubicin-induced cardiomyopathy from the cardiotoxic mechanisms to management. Prog. Cardiovasc. Dis. 2007, 49, 330–352. [Google Scholar] [CrossRef]
- Petrykey, K.; Andelfinger, G.U.; Laverdière, C.; Sinnett, D.; Krajinovic, M. Genetic factors in anthracycline-induced cardiotoxicity in patients treated for pediatric cancer. Expert Opin. Drug Metab. Toxicol. 2020, 16, 865–883. [Google Scholar] [CrossRef] [PubMed]
- Jeyaprakash, P.; Sangha, S.; Ellenberger, K.; Sivapathan, S.; Pathan, F.; Negishi, K. Cardiotoxic Effect of Modern Anthracycline Dosing on Left Ventricular Ejection Fraction: A Systematic Review and Meta-Analysis of Placebo Arms From Randomized Controlled Trials. J. Am. Heart Assoc. 2021, 10, e018802. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, K.; Zhang, J.; Honbo, N.; Karliner, J.S. Doxorubicin cardiomyopathy. Cardiology 2018, 139, 253–258. [Google Scholar] [CrossRef] [PubMed]
- Van Dalen, E.C.; van der Pal, H.J.; Kok, W.E.; Caron, H.N.; Kremer, L.C. Clinical heart failure in a cohort of children treated with anthracyclines: A long-term follow-up study. Eur. J. Cancer 2016, 54, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Tapio, S. Pathology and biology of radiation-induced cardiac disease. J. Radiat. Res. 2016, 57, 439–448. [Google Scholar] [CrossRef]
- Darby, S.C.; Ewertz, M.; McGale, P.; Bennet, A.M.; Blom-Goldman, U.; Brønnum, D.; Correa, C.; Cutter, D.; Gagliardi, G.; Gigante, B.; et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. N. Engl. J. Med. 2013, 368, 987–998. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS): Developed by the task force on cardio-oncology of the European Society of Cardiology (ESC). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Negishi, K.; Negishi, T.; Hare, J.L.; Haluska, B.A.; Plana, J.C.; Marwick, T.H. Independent and incremental value of deformation indices for prediction of trastuzumab-induced cardiotoxicity. J. Am. Soc. Echocardiogr. 2013, 26, 493–498. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Poulin, F.; Lim, K.-D.; Plana, J.C.; Woo, A.; Marwick, T.H. Use of myocardial strain imaging by echocardiography for the early detection of cardiotoxicity in patients during and after cancer chemotherapy: A systematic review. J. Am. Coll. Cardiol. 2013, 63, 2751–2768. [Google Scholar] [CrossRef]
- Sawaya, H.; Sebag, I.A.; Plana, J.C.; Januzzi, J.L.; Ky, B.; Cohen, V.; Gosavi, S.; Carver, J.R.; Wiegers, S.E.; Martin, R.P.; et al. Early detection and prediction of cardiotoxicity in chemotherapy-treated patients. Am. J. Cardiol. 2011, 107, 1375–1380. [Google Scholar] [CrossRef]
- Cardinale, D.; Colombo, A.; Sandri, M.T.; Lamantia, G.; Colombo, N.; Civelli, M.; Martinelli, G.; Veglia, F.; Fiorentini, C.; Cipolla, C.M.; et al. Prevention of high-dose chemotherapy-induced cardiotoxicity in high-risk patients by angiotensin-converting enzyme inhibition. Circulation. Circulation 2006, 114, 2474–2481. [Google Scholar] [CrossRef] [PubMed]
- Jurcut, R.; Wildiers, H.; Ganame, J.; D’hooge, J.; Paridaens, R.; Voigt, J.-U. Detection and monitoring of cardiotoxicity—What does modern cardiology offer? Support. Care Cancer 2008, 16, 437–445. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Negishi, T.; Somerset, E.; Negishi, K.; Penicka, M.; Lemieux, J.; Aakhus, S.; Miyazaki, S.; Shirazi, M.; Galderisi, M.; et al. Strain-Guided Management of Potentially Cardiotoxic Cancer Therapy. J. Am. Coll. Cardiol. 2021, 77, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Thavendiranathan, P.; Grant, A.D.; Negishi, T.; Plana, J.C.; Popović, Z.B.; Marwick, T.H. Reproducibility of echocardiographic techniques for sequential assessment of left ventricular ejection fraction and volumes: Application to patients undergoing cancer chemotherapy. J. Am. Coll. Cardiol. 2013, 61, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Čelutkienė, J.; Pudil, R.; López-Fernández, T.; Grapsa, J.; Nihoyannopoulos, P.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; Tocchetti, C.G.; von Haehling, S.; et al. Role of cardiovascular imaging in cancer patients receiving cardiotoxic therapies: A position statement on behalf of the Heart Failure Association (HFA), the European Association of Cardiovascular Imaging (EACVI) and the Cardio-Oncology Council of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2020, 22, 1504–1524. [Google Scholar] [CrossRef]
- Sawaya, H.; Sebag, I.A.; Plana, J.C.; Januzzi, J.L.; Ky, B.; Tan, T.C.; Cohen, V.; Banchs, J.; Carver, J.R.; Wiegers, S.E.; et al. Assessment of echocardiography and biomarkers for the extended prediction of cardiotoxicity in patients treated with anthracyclines, taxanes, and trastuzumab. Circ Cardiovasc Imaging. Circ. Cardiovasc. Imaging 2012, 5, 596–603. [Google Scholar] [CrossRef]
- Venturelli, F.; Masetti, R.; Fabi, M.; Rondelli, R.; Martoni, A.; Prete, A.; Bonvicini, M.; Pession, A. Tissue Doppler Imaging for anthracycline cardiotoxicity monitoring in pediatric patients with cancer. Cardiooncology 2018, 4, 6–8. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef]
- Negishi, K.; Negishi, T.; Agler, D.A.; Plana, J.C.; Marwick, T.H. Role of temporal resolution in selection of the appropriate strain technique for evaluation of subclinical myocardial dysfunction. Echocardiography. Echocardiography 2012, 29, 334–339. [Google Scholar] [CrossRef]
- Jordan, J.H.; Todd, R.M.; Vasu, S.; Hundley, W.G. Cardiovascular Magnetic Resonance in the Oncology Patient. JACC Cardiovasc. Imaging 2018, 11, 1150–1172. [Google Scholar] [CrossRef]
- Schelbert, E.B.; Piehler, K.M.; Zareba, K.M.; Moon, J.C.; Ugander, M.; Messroghli, D.R.; Valeti, U.S.; Chang, C.H.; Shroff, S.G.; Diez, J.; et al. Myocardial Fibrosis Quantified by Extracellular Volume Is Associated with Subsequent Hospitalization for Heart Failure, Death, or Both Across the Spectrum of Ejection Fraction and Heart Failure Stage. J. Am. Heart Assoc. 2015, 4, e002613. [Google Scholar] [CrossRef] [PubMed]
- Neilan, T.G.; Coelho-Filho, O.R.; Pena-Herrera, D.; Shah, R.V.; Jerosch-Herold, M.; Francis, S.A.; Moslehi, J.; Kwong, R.Y. Left ventricular mass in patients with a cardiomyopathy after treatment with anthracyclines. Am. J. Cardiol. 2012, 110, 1679–1686. [Google Scholar] [CrossRef] [PubMed]
- Tham, E.B.; Haykowsky, M.J.; Chow, K.; Spavor, M.; Kaneko, S.; Khoo, N.S.; Pagano, J.J.; Mackie, A.S.; Thompson, R.B. Diffuse myocardial fibrosis by T1-mapping in children with subclinical anthracycline cardiotoxicity: Relationship to exercise capacity, cumulative dose and remodeling. J. Cardiovasc. Magn. Reson. 2013, 15, 48. [Google Scholar] [CrossRef] [PubMed]
- Neilan, T.G.; Rothenberg, M.L.; Amiri-Kordestani, L.; Sullivan, R.J.; Steingart, R.M.; Gregory, W.; Hariharan, S.; Hammad, T.A.; Lindenfeld, J.; Murphy, M.J.; et al. Myocarditis Associated with Immune Checkpoint Inhibitors: An Expert Consensus on Data Gaps and a Call to Action. Oncol. 2018, 23, 874–878. [Google Scholar] [CrossRef]
- Lewis, A.J.M.; Burrage, M.K.; Ferreira, V.M. Cardiovascular magnetic resonance imaging for inflammatory heart diseases. Cardiovasc. Diagn. Ther. 2020, 10, 598–609. [Google Scholar] [CrossRef]
- Pontone, G.; Rossi, A.; Guglielmo, M.; Dweck, M.R.; Gaemperli, O.; Nieman, K.; Pugliese, F.; Maurovich-Horvat, P.; Gimelli, A.; Cosyns, B.; et al. Clinical applications of cardiac computed tomography: A consensus paper of the European Association of Cardiovascular Imaging—Part I. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 299–314. [Google Scholar] [CrossRef]
- Giusca, S.; Schütz, M.; Kronbach, F.; Wolf, D.; Nunninger, P.; Korosoglou, G. Coronary Computer Tomography Angiography in 2021—Acquisition Protocols, Tips and Tricks and Heading beyond the Possible. Diagnostics 2021, 11, 1072. [Google Scholar] [CrossRef]
- Egashira, K.; Sueta, D.; Kidoh, M.; Tomiguchi, M.; Oda, S.; Usuku, H.; Hidaka, K.; Goto-Yamaguchi, L.; Sueta, A.; Komorita, T.; et al. Cardiac computed tomography-derived myocardial tissue characterization after anthracycline treatment. ESC Heart Fail. 2022, 9, 1792–1800. [Google Scholar] [CrossRef]
- Everson, M.; Sukcharoen, K.; Milner, Q. Contrast-associated acute kidney injury. BJA Educ. 2020, 20, 417–423. [Google Scholar] [CrossRef]
- D’Amore, C.; Gargiulo, P.; Paolillo, S.; Pellegrino, A.M.; Formisano, T.; Mariniello, A.; Della Ratta, G.; Iardino, E.; D’Amato, M.; La Mura, L.; et al. Nuclear imaging in detection and monitoring of cardiotoxicity. World J. Radiol. 2014, 6, 486–492. [Google Scholar] [CrossRef]
- Sarocchi, M.; Bauckneht, M.; Arboscello, E.; Capitanio, S.; Marini, C.; Morbelli, S.; Miglino, M.; Congiu, A.G.; Ghigliotti, G.; Balbi, M.; et al. An increase in myocardial 18-fluorodeoxyglucose uptake is associated with left ventricular ejection fraction decline in Hodgkin lymphoma patients treated with anthracycline. J. Transl. Med. 2018, 16, 295. [Google Scholar] [CrossRef] [PubMed]
- Pudil, R.; Mueller, C.; Čelutkienė, J.; Henriksen, P.A.; Lenihan, D.; Dent, S.; Barac, A.; Stanway, S.; Moslehi, J.; Suter, T.M.; et al. Role of serum biomarkers in cancer patients receiving cardiotoxic cancer therapies: A position statement from the Cardio-Oncology Study Group of the Heart Failure Association and the Cardio-Oncology Council of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1966–1983. [Google Scholar] [CrossRef] [PubMed]
- Onitilo, A.A.; Engel, J.M.; Stankowski, R.V.; Liang, H.; Berg, R.L.; Doi, S.A.R. High-sensitivity C-reactive protein (hs-CRP) as a biomarker for trastuzumab-induced cardiotoxicity in HER2-positive early-stage breast cancer: A pilot study. Breast Cancer Res. Treat. 2012, 134, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.F.; Manrique, C.; Pun, S.; Liu, J.E.; Mara, E.; Fleisher, M.; Patil, S.; Jones, L.W.; Steingart, R.M.; Hudis, C.A.; et al. Cardiac Safety of Paclitaxel Plus Trastuzumab and Pertuzumab in Patients with HER2-Positive Metastatic Breast Cancer. Oncologist 2016, 21, 418–424. [Google Scholar] [CrossRef]
- Grela-Wojewoda, A.; Püsküllüoğlu, M.; Sas-Korczyńska, B.; Zemełka, T.; Pacholczak-Madej, R.; Wysocki, W.M.; Wojewoda, T.; Adamczyk, A.; Lompart, J.; Korman, M.; et al. Biomarkers of Trastuzumab-Induced Cardiac Toxicity in HER2- Positive Breast Cancer Patient Population. Cancers 2022, 14, 3353. [Google Scholar] [CrossRef]
- Lopez, J.S.; Penas, R.D.L.; De Avila, L.; De Julian, M.; Arnal, M.; Duenas, E.M.-D.; Olmos, S.; Lopez-Rodriguez, A.; Munarriz, J.; Peset, A.; et al. Prospective evaluation of echocardiography and serum biomarkers as predictors of cardiotoxicity in patients with breast cancer treated with anthracyclines, taxanes, with/without trastuzumab. J. Clin. Oncol. 2014, 32, e20686. [Google Scholar] [CrossRef]
- Michel, L.; Mincu, R.I.; Mahabadi, A.A.; Settelmeier, S.; Al-Rashid, F.; Rassaf, T.; Totzeck, M. Troponins and brain natriuretic peptides for the prediction of cardiotoxicity in cancer patients: A meta-analysis. Eur. J. Heart Fail. 2020, 22, 350–361. [Google Scholar] [CrossRef]
- Wolff, R.F.; Moons, K.G.; Riley, R.; Whiting, P.F.; Westwood, M.; Collins, G.S.; Reitsma, J.B.; Kleijnen, J.; Mallett, S.; for the PROBAST Group. PROBAST: A Tool to Assess the Risk of Bias and Applicability of Prediction Model Studies. Ann. Intern. Med. 2019, 170, 51–58. [Google Scholar] [CrossRef]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. BMJ 2015, 350, g7594. [Google Scholar] [CrossRef]
- Kar, J.; Cohen, M.V.; McQuiston, S.A.; Malozzi, C.M. Can global longitudinal strain (GLS) with magnetic resonance prognosticate early cancer therapy-related cardiac dysfunction (CTRCD) in breast cancer patients, a prospective study? Magn. Reson. Imaging 2023, 97, 68–81. [Google Scholar] [CrossRef]
- Fallah-Rad, N.; Walker, J.R.; Wassef, A.; Lytwyn, M.; Bohonis, S.; Fang, T.; Tian, G.; Kirkpatrick, I.D.; Singal, P.K.; Krahn, M.; et al. The utility of cardiac biomarkers, tissue velocity and strain imaging, and cardiac magnetic resonance imaging in predicting early left ventricular dysfunction in patients with human epidermal growth factor receptor II-positive breast cancer treated with adjuvant trastuzumab therapy. J. Am. Coll. Cardiol. 2011, 57, 2263–2270. [Google Scholar] [CrossRef]
- Guglin, M.; Krischer, J.; Tamura, R.; Fink, A.; Bello-Matricaria, L.; McCaskill-Stevens, W.; Munster, P.N. Randomized Trial of Lisinopril Versus Carvedilol to Prevent Trastuzumab Cardiotoxicity in Patients with Breast Cancer. J. Am. Coll. Cardiol. 2019, 73, 2859–2868. [Google Scholar] [CrossRef]
- Henry, M.L.; Niu, J.; Zhang, N.; Giordano, S.H.; Chavez-MacGregor, M. Cardiotoxicity and Cardiac Monitoring Among Chemotherapy-Treated Breast Cancer Patients. JACC Cardiovasc. Imaging 2018, 11, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
- Houbois, C.P.; Nolan, M.; Somerset, E.; Shalmon, T.; Esmaeilzadeh, M.; Lamacie, M.M.; Amir, E.; Brezden-Masley, C.; Koch, C.A.; Thevakumaran, Y.; et al. Serial Cardiovascular Magnetic Resonance Strain Measurements to Identify Cardiotoxicity in Breast Cancer: Comparison with Echocardiography. JACC Cardiovasc. Imaging 2021, 14, 962–974. [Google Scholar] [CrossRef]
- Boekhout, A.H.; Gietema, J.A.; Kerklaan, B.M.; van Werkhoven, E.D.; Altena, R.; Honkoop, A.; Los, M.; Smit, W.M.; Nieboer, P.; Smorenburg, C.H.; et al. Angiotensin II–Receptor Inhibition with Candesartan to Prevent Trastuzumab-Related Cardiotoxic Effects in Patients with Early Breast Cancer: A Randomized Clinical Trial. JAMA Oncol. 2016, 2, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Terui, Y.; Sugimura, K.; Ota, H.; Tada, H.; Nochioka, K.; Sato, H.; Katsuta, Y.; Fujiwara, J.; Harada-Shoji, N.; Sato-Tadano, A.; et al. Usefulness of cardiac magnetic resonance for early detection of cancer therapeutics-related cardiac dysfunction in breast cancer patients. Int. J. Cardiol. 2023, 371, 472–479. [Google Scholar] [CrossRef]
- Yu, A.F.; Moskowitz, C.S.; Chuy, K.L.; Yang, J.; Dang, C.T.; Liu, J.E.; Oeffinger, K.C.; Steingart, R.M. Cardiotoxicity Surveillance and Risk of Heart Failure During HER2 Targeted Therapy. JACC CardioOncology 2020, 2, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Akrida, I.; Mulita, F. The clinical significance of HER2 expression in DCIS. Med. Oncol. 2022, 40, 16. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.-H.; Chen, H.H.W.; Tsai, Y.-S. Accelerated coronary calcium burden in breast cancer patients after radiotherapy: A comparison with age and race matched healthy women. Radiat. Oncol. 2021, 16, 210. [Google Scholar] [CrossRef] [PubMed]
- Dhir, V.; Yan, A.T.; Nisenbaum, R.; Sloninko, J.; Connelly, K.A.; Barfett, J.; Haq, R.; Kirpalani, A.; Chan, K.K.W.; Petrella, T.M.; et al. Assessment of left ventricular function by CMR versus MUGA scans in breast cancer patients receiving trastuzumab: A prospective observational study. Int. J. Cardiovasc. Imaging 2019, 35, 2085–2093. [Google Scholar] [CrossRef]

{kind=link}
| Categories | Data Extracted |
|---|---|
| Study Characteristics |
|
| Participant Characteristics |
|
| Intervention and Character Details |
|
| Outcome Measures |
|
| Results |
|
| Author(s) | Source of Data | No. of Subjects | Imaging Technique | Treatment |
|---|---|---|---|---|
| Boekhout et al., 2016 | Type of study: Randomized clinical trial Place of study: The Netherlands Years of study: 2011–2015 | 206 | TTE, MUGA | Trastuzumab |
| Fallah-Rad et al., 2011 | Type of study: Observational study Place of study: Canada Years of study: 2011 | 42 | Strain Imaging, CMR | Trastuzumab |
| Guglin et al., 2019 | Type of study: Randomized controlled trial. Place of study: USA Years of study: 2019 | 468 | TTE, MUGA | Trastuzumab Lisinopril Carvedilol Phosphate-Extended Release |
| Henry et al., 2018 | Type of study: Observational study Place of study: USA Years of study: 2018 | 16,456 | TTE, MUGA, CMR | Trastuzumab |
| Houbois et al., 2021 | Type of study: Prospective observational study Place of study: Denmark Years of study: 2014–2018 | 125 | CMR, Echo | Trastuzumab Anthracyclines |
| Kar et al., 2023 | Type of study: Prospective study Place of study: USA Years of study: 2023 | 32 | Stimulated Echoes (DENSE) MRI, TTE, GLS | Trastuzumab Doxorubicin Cyclophosphamide Taxol Carboplatin Pertuzumab |
| Terui et al., 2023 | Type of study: Prospective observational study Place of study: Japan Years of study: 2016–2021 | 83 | CMR, TTE | Trastuzumab Anthracyclines |
| Yu et al., 2020 | Type of study: Prospective observational study Place of study: Japan Years of study: 2016–2021 | 53 | TTE, MUGA, CMR | Trastuzumab |
| Study | Title | Imaging Technique | Main Study Outcomes |
|---|---|---|---|
| Boekhout et al., 2016 | Angiotensin-2 Reception Inhibition with Candesartan to prevent Trastuzumab-related Cardiotoxic events in patients with early Breast Cancer | TTE, MUGA | At least 1 of the 2 primary cardiac end points was manifested by 36/206 cases. There were 3.8% more cardiac events in the candesartan group than in the placebo group. The 2-year cumulative incidence of cardiac events was 0.28 (95% CI, 0.13–0.40) in the candesartan group and 0.16 (95% CI, 0.08–0.22) in the placebo group (p = 0.56). Candesartan did not affect changes in NT-pro-BNP and HS-TnT values, and these biomarkers were not associated with significant changes in LVEF |
| Fallah-Rad et al., 2011 | The Utility of Cardiac Biomarkers, Tissue Velocity, Strain Imaging, and Cardiac MRI in predicting early LV Dysfunction in patients with HER2-positive Breast Cancer treated with adjuvant Trastuzumab therapy | TTE, MRI | Ten (24%) women developed trastuzumab-induced CM. Decreased LVEF at 12-month follow-up: by TTE from 61% +/− 9 to 49% +/− 4, and by CMR: from 66% +/− 5% to 47 +/− 4% |
| Guglin et al., 2019 | Randomized Trial of Lisinopril vs. Carvedilol to prevent Trastuzumab Cardiotoxicity in patients with Breast Cancer | TTE, MUGA | CTRCD in 32% of patients on placebo, 29% on carvedilol (Anthracycline group HR 0.49 (p = 0.009), non-anthracycline HR 1.05 (p = 0.559)), 30% on lisinopril (Anthracycline group HR 0.53 (p = 0.015), and non-anthracycline group HR 1.17 (p = 0.689)) |
| Henry et al., 2018 | Cardiotoxicity and Cardiac Monitoring among Chemotherapy-treated Breast Cancer Patients | TTE, MUGA, MRI | A total of 692 patients (4.2%) developed HF after chemotherapy: 2.1% (<35 years old), 2.9% (36–49 years old), 3.5% (50–64 years old), and 8.3% (>65 years old) |
| Houbois et al., 2021 | Serial Cardiovascular MR Strain Measurements to identify Cardiotoxicity in Breast Cancer | TTE, MRI | In total, 28% of patients developed CTRCD by CMR and 22% by 2DE. A 15% relative reduction in 2DE-GLS increased the CTRCD odds by 133% at subsequent follow-up, compared with 47%/50% by tagged-CMR GLS/GCS and 87% by FT-GCS |
| Kar et al., 2023 | Can GLS with MR prognosticate early CTRCD in Breast Cancer Patients? A Prospective Study | TTE, MRI | GLS worsened from baseline to the 3- and 6-month follow-ups (−19.1 ± 2.1%, −16.0 ± 3.1%, −16.1 ± 3.0%; p < 0.001). Univariable Cox regression showed the 3-month GLS significantly associated as an agonist (hazard ratio [HR]-per-SD: 2.1; 95% CI: 1.4–3.1; p < 0.001) and LVEF as a protector (HR-per-SD: 0.8; 95% CI: 0.7–0.9; p = 0.001) for CTRCD occurrence. Bivariable regression showed the 3-month GLS (HR-per-SD: 2.0; 95% CI: 1.2–3.4; p = 0.01) as a CTRCD prognostic factor independent of other covariates, including LVEF (HR-per-SD: 1.0; 95% CI: 0.9–1.2; p = 0.9) |
| Terui et al., 2023 | Usefulness of Cardiac MR for early detection of CTRCD in Breast Cancer Patients | TTE, CMR | In total, 8.4% of subjects developed CTRCD. LVEF and GLS were significantly decreased after chemotherapy (LVEF, from 71.2 ± 4.4 to 67.6 ± 5.8%; GLS, from −27.9 ± 3.9 to −24.7 ± 3.5%, respectively, both p < 0.01). The native T1 value was also significantly elevated after chemotherapy (from 1283 ± 36 to 1308 ± 39 msec, p < 0.01) |
| Yu et al., 2020 | Cardiotoxicity Surveillance and risk of Heart Failure During HER2-targeted therapy | TTE, MUGA, MRI | In total, 14.7% of patients developed CTRCD. LVEF <55% on routine surveillance during HER2-targeted therapy indicates a risk of HF |
| 1 | Lack of standardization in the use of imaging modalities for cardiotoxicity assessment and in the protocol used during image acquisition. |
| 2 | There is a need for studies that evaluate the utility of multimodal imaging approaches for cardiotoxicity assessment. |
| 3 | Lack of standardization in the interpretation of imaging findings. |
| 4 | Lack of research on the cost-effectiveness of different imaging modalities for cardiotoxicity assessment. |
| 5 | Insufficient research into the long-term prognostic value of imaging modalities in assessing cardiotoxicity. |
| 6 | Evaluation of the utility of multimodality imaging approaches for cardiotoxicity assessment. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cronin, M.; Seher, M.; Arsang-Jang, S.; Lowery, A.; Kerin, M.; Wijns, W.; Soliman, O. Multimodal Imaging of Cancer Therapy-Related Cardiac Dysfunction in Breast Cancer—A State-of-the-Art Review. J. Clin. Med. 2023, 12, 6295. https://doi.org/10.3390/jcm12196295
Cronin M, Seher M, Arsang-Jang S, Lowery A, Kerin M, Wijns W, Soliman O. Multimodal Imaging of Cancer Therapy-Related Cardiac Dysfunction in Breast Cancer—A State-of-the-Art Review. Journal of Clinical Medicine. 2023; 12(19):6295. https://doi.org/10.3390/jcm12196295
Chicago/Turabian StyleCronin, Michael, Mehreen Seher, Shahram Arsang-Jang, Aoife Lowery, Michael Kerin, William Wijns, and Osama Soliman. 2023. "Multimodal Imaging of Cancer Therapy-Related Cardiac Dysfunction in Breast Cancer—A State-of-the-Art Review" Journal of Clinical Medicine 12, no. 19: 6295. https://doi.org/10.3390/jcm12196295
APA StyleCronin, M., Seher, M., Arsang-Jang, S., Lowery, A., Kerin, M., Wijns, W., & Soliman, O. (2023). Multimodal Imaging of Cancer Therapy-Related Cardiac Dysfunction in Breast Cancer—A State-of-the-Art Review. Journal of Clinical Medicine, 12(19), 6295. https://doi.org/10.3390/jcm12196295