
Safety and Effectiveness of Intensive Treatments Administered Outside the Intensive Care Unit to Hematological Critically Ill Patients: An Intensive Care without Walls Trial

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Data Collection
2.4. Statistical Analysis
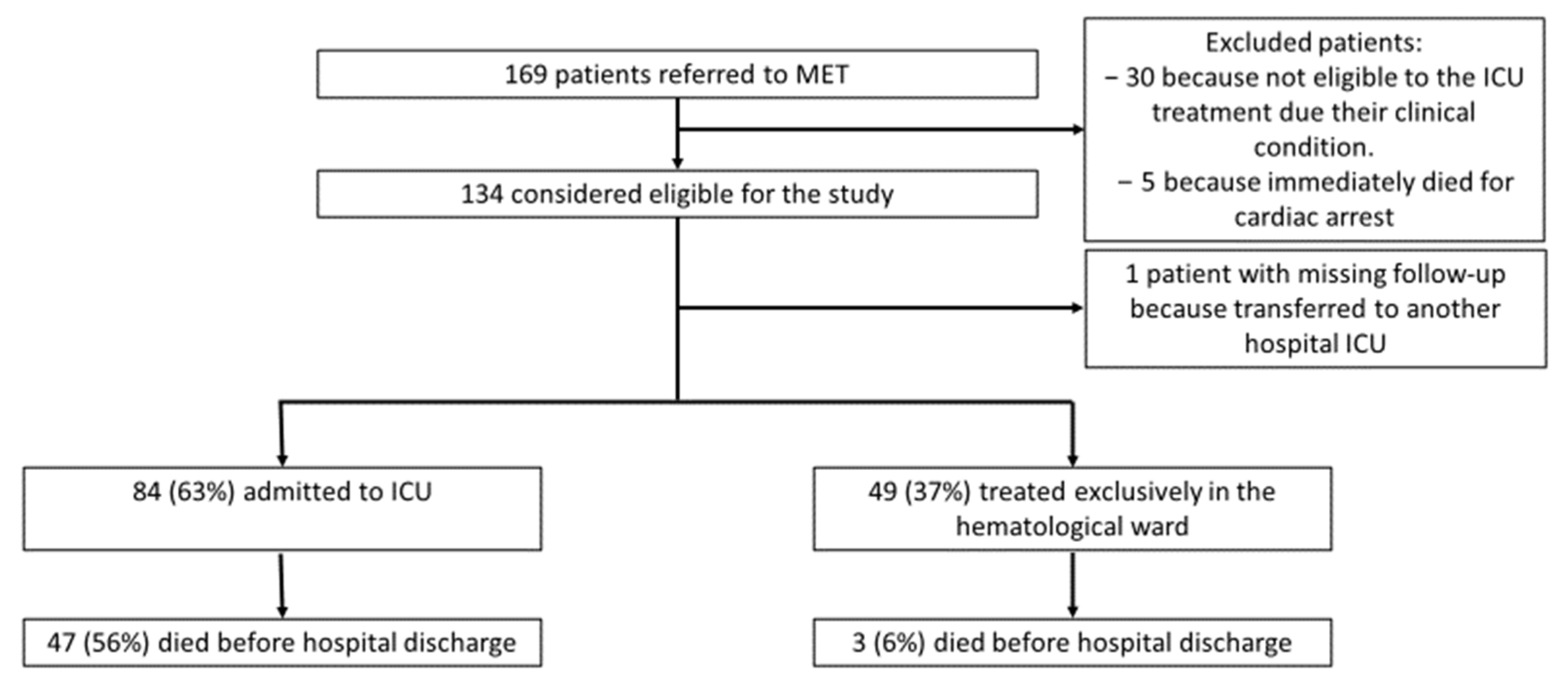
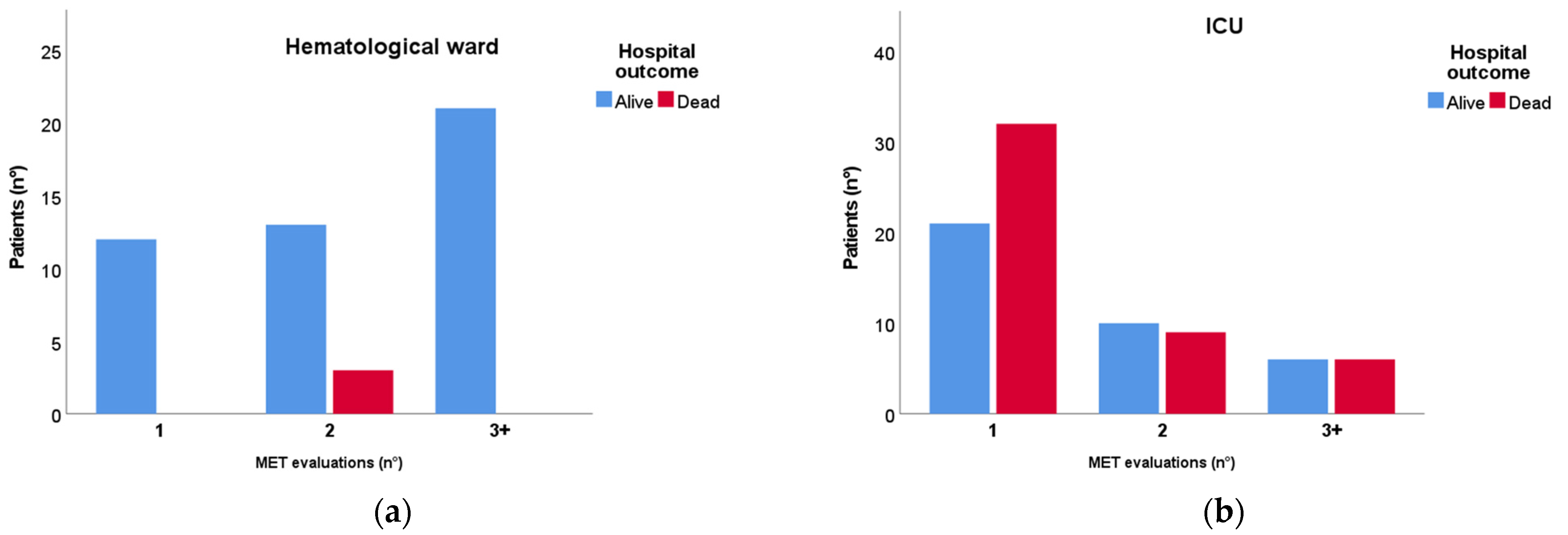
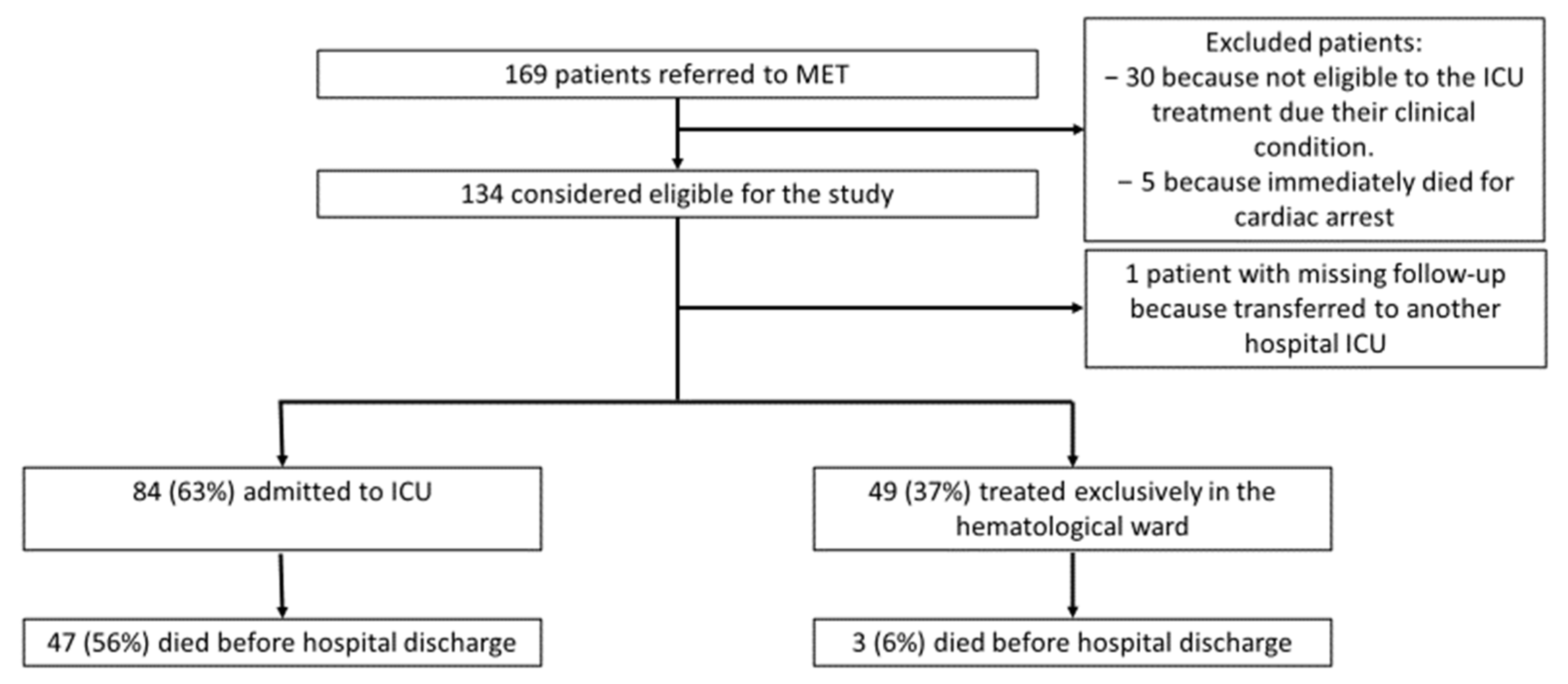
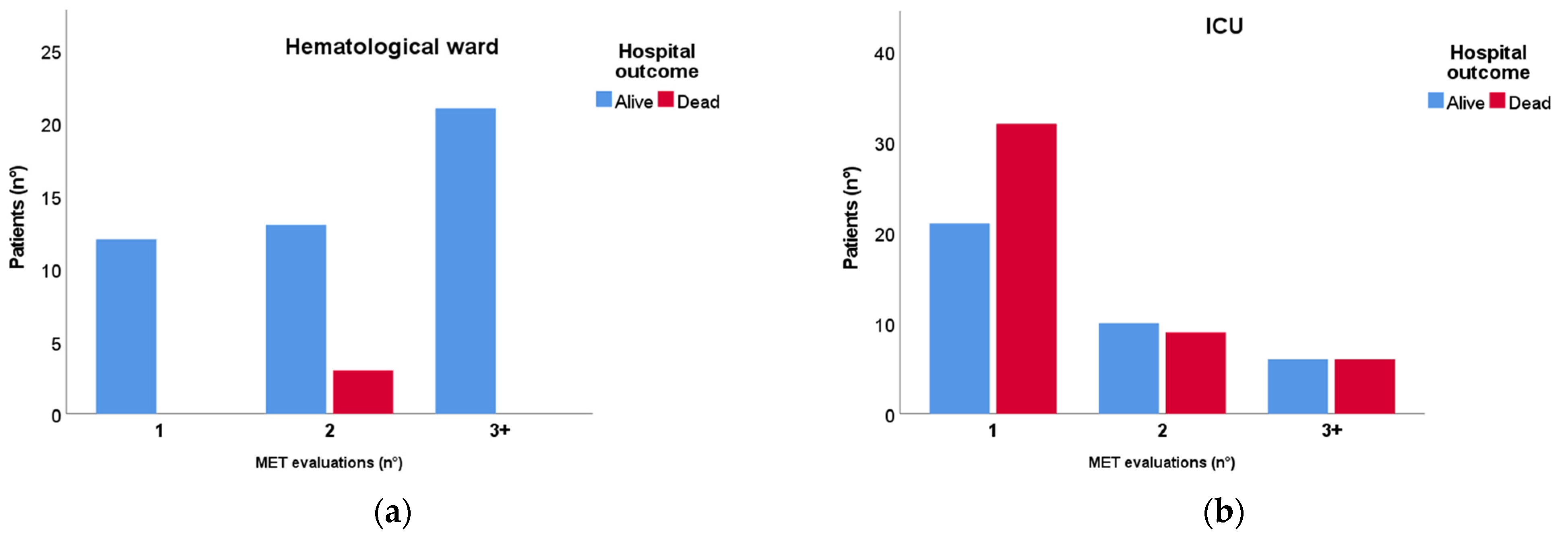
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Darmon, M.; Bourmaud, A.; Georges, Q.; Soares, M.; Jeon, K.; Oeyen, S.; Rhee, C.K.; Gruber, P.; Ostermann, M.; Hill, Q.A.; et al. Changes in critically ill cancer patients’ short-term outcome over the last decades: Results of systematic review with meta-analysis on individual data. Intensive Care Med. 2019, 45, 977–987. [Google Scholar] [CrossRef] [PubMed]
- Azoulay, E.; Mokart, D.; Pène, F.; Lambert, J.; Kouatchet, A.; Mayaux, J.; Vincent, F.; Nyunga, M.; Bruneel, F.; Laisne, L.-M.; et al. Outcomes of critically ill patients with hematologic malignancies: Prospective multicenter data from France and Belgium—A groupe de recherche respiratoire en réanimation onco-hématologique study. J. Clin. Oncol. 2013, 31, 2810–2818. [Google Scholar] [CrossRef] [PubMed]
- Denardo, S.J.; Oye, R.K.; Bellamy, P.E. Efficacy of intensive care for bone marrow transplant patients with respiratory failure. Crit. Care Med. 1989, 17, 4–6. [Google Scholar] [CrossRef]
- Kiehl, M.G.; Beutel, G.; Böll, B.; Buchheidt, D.; Forkert, R.; Fuhrmann, V.; Knöbl, P.; Kochanek, M.; Kroschinsky, F.; La Rosée, P.; et al. Consensus statement for cancer patients requiring intensive care support. Ann. Hematol. 2018, 97, 1271–1282. [Google Scholar] [CrossRef]
- Meert, A.-P.; Wittnebel, S.; Holbrechts, S.; Toffart, A.-C.; Lafitte, J.-J.; Piagnerelli, M.; Lemaitre, F.; Peyrony, O.; Calvel, L.; Lemaitre, J.; et al. Critically ill cancer patient’s resuscitation: A Belgian/French societies’ consensus conference. Intensive Care Med. 2021, 47, 1063–1077. [Google Scholar] [CrossRef] [PubMed]
- Taheri, L.; Anandanadesan, R.; de Lavallade, H.; Pagkalidou, E.; Pagliuca, A.; Mufti, G.; Auzinger, G.; Metaxa, V. The role of a critical care outreach service in the management of patients with haematological malignancy. J. Intensive Care Soc. 2019, 20, 327–334. [Google Scholar] [CrossRef]
- Rhodes, A.; Ferdinande, P.; Flaatten, H.; Guidet, B.; Metnitz, P.G.; Moreno, R.P. The variability of critical care bed numbers in Europe. Intensive Care Med. 2012, 38, 1647–1653. [Google Scholar] [CrossRef]
- Song, J.-U.; Suh, G.Y.; Park, H.Y.; Lim, S.Y.; Han, S.G.; Kang, Y.R.; Kwon, O.J.; Woo, S.; Jeon, K. Early intervention on the outcomes in critically ill cancer patients admitted to intensive care units. Intensive Care Med. 2012, 38, 1505–1513. [Google Scholar] [CrossRef]
- Bauer, J.; Brüggmann, D.; Klingelhöfer, D.; Maier, W.; Schwettmann, L.; Weiss, D.J.; Groneberg, D.A. Access to intensive care in 14 European countries: A spatial analysis of intensive care need and capacity in the light of COVID-19. Intensive Care Med. 2020, 46, 2026–2034. [Google Scholar] [CrossRef]
- Biard, L.; Darmon, M.; Lemiale, V.; Mokart, D.; Chevret, S.; Azoulay, E.; Resche-Rigon, M. Center Effects in Hospital Mortality of Critically Ill Patients with Hematologic Malignancies. Crit. Care Med. 2019, 47, 809–816. [Google Scholar] [CrossRef]
- Guidelines for intensive care unit admission, discharge, and triage. Task Force of the American College of Critical Care Medicine, Society of Critical Care Medicine. Crit. Care Med. 1999, 27, 633–638. [Google Scholar]
- Blanch, L.; Abillama, F.F.; Amin, P.; Christian, M.; Joynt, G.M.; Myburgh, J.; Nates, J.L.; Pelosi, P.; Sprung, C.; Topeli, A.; et al. Triage decisions for ICU admission: Report from the Task Force of the World Federation of Societies of Intensive and Critical Care Medicine. J. Crit. Care 2016, 36, 301–305. [Google Scholar] [CrossRef]
- Ramos, J.G.R.; Perondi, B.; Dias, R.D.; Miranda, L.C.; Cohen, C.; Carvalho, C.R.R.; Velasco, I.T.; Forte, D.N. Development of an algorithm to aid triage decisions for intensive care unit admission: A clinical vignette and retrospective cohort study. Crit. Care 2016, 20, 81. [Google Scholar] [CrossRef]
- Hillman, K.M. Critical care without walls. Curr. Opin. Crit. Care 2002, 8, 594–599. [Google Scholar] [CrossRef]
- Austin, C.A.; Hanzaker, C.B.; Stafford, R.M.; Mayer, C.; Culp, L.R.; Lin, F.-C.; Chang, L. Utilization of rapid response resources and outcomes in a comprehensive cancer center. Crit. Care Med. 2014, 42, 905–909. [Google Scholar] [CrossRef] [PubMed]
- Jung, B.; Daurat, A.; De Jong, A.; Chanques, G.; Mahul, M.; Monnin, M.; Molinari, N.; Jaber, S. Rapid response team and hospital mortality in hospitalized patients. Intensive Care Med. 2016, 42, 494–504. [Google Scholar] [CrossRef] [PubMed]
- De Jong, A.; Jung, B.; Daurat, A.; Chanques, G.; Mahul, M.; Monnin, M.; Molinari, N.; Jaber, S. Effect of rapid response systems on hospital mortality: A systematic review and meta-analysis. Intensive Care Med. 2016, 42, 615–617. [Google Scholar] [CrossRef]
- Park, J.; Lee, Y.J.; Hong, S.-B.; Jeon, K.; Moon, J.Y.; Kim, J.S.; Kang, B.J.; Ahn, J.-J.; Lee, D.-H.; Park, J.; et al. The association between hospital length of stay before rapid response system activation and clinical outcomes: A retrospective multicenter cohort study. Respir. Res. 2021, 22, 60. [Google Scholar] [CrossRef]
- Lee, J.; Shin, Y.; Choi, E.; Choi, S.; Son, J.; Jung, Y.K.; Hong, S.-B. Impact of hospitalization duration before medical emergency team activation: A retrospective cohort study. PLoS ONE 2021, 16, e0247066. [Google Scholar] [CrossRef] [PubMed]
- Bouteloup, M.; Perinel, S.; Bourmaud, A.; Azoulay, E.; Mokart, D.; Darmon, M. Outcomes in adult critically ill cancer patients with and without neutropenia: A systematic review and meta-analysis of the Groupe de Recherche en Réanimation Respiratoire du patient d’Onco-Hématologie (GRRR-OH). Oncotarget 2017, 8, 1860–1870. [Google Scholar] [CrossRef] [PubMed]
- Doukhan, L.; Bisbal, M.; Chow-Chine, L.; Sannini, A.; Brun, J.P.; Cambon, S.; Duong, L.N.; Faucher, M.; Mokart, D. Respiratory events in ward are associated with later intensive care unit (ICU) admission and hospital mortality in onco-hematology patients not admitted to ICU after a first request. PLoS ONE 2017, 12, e0181808. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.K.; Kang, J.Y.; Kim, Y.H.; Kim, J.W.; Yoon, H.K.; Kim, S.C.; Kwon, S.S.; Kim, Y.K.; Kim, K.H.; Moon, H.S.; et al. Risk factors for acute respiratory distress syndrome during neutropenia recovery in patients with hematologic malignancies. Crit. Care 2009, 13, R173. [Google Scholar] [CrossRef] [PubMed]
- Squadrone, V.; Massaia, M.; Bruno, B.; Marmont, F.; Falda, M.; Bagna, C.; Bertone, S.; Filippini, C.; Slutsky, A.S.; Vitolo, U.; et al. Early CPAP prevents evolution of acute lung injury in patients with hematologic malignancy. Intensive Care Med. 2010, 36, 1666–1674. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| N = 133 (%) | |
| Hematological diagnosis | |
| - Non-Hodgkin Lymphoma | 38 (29) |
| - Acute myeloid leukemia | 36 (27) |
| - Multiple Myeloma | 17 (13) |
| - Acute lymphocytic leukemia | 16 (12) |
| - Chronic lymphocytic leukemia | 5 (4) |
| - Myelodysplasia | 5 (4) |
| - Bone marrow aplasia | 4 (3) |
| - Hodgkin Lymphoma | 3 (2) |
| - Others | 9 (7) |
| Disease state | |
| - Onset | 55 (42) |
| - Complete remission | 41 (31) |
| - Relapse < 1 year | 5 (4) |
| - Relapse > 1 year | 19 (14) |
| - Refractory disease | 12 (9) |
| - Unknown | 1 (1) |
| Bone marrow transplant | |
| - Autologous | 5 (4) |
| - Allogenic | 30 (23) |
| Graft-vs.-host disease | |
| - Acute | 16 (12) |
| - Chronic | 2 (2) |
| Neutropenia * | 46 (35) |
| Ongoing chemotherapy | 76 (57) |
| Pharmacological immunosuppression | 62 (47) |
| Alive (N = 83) | Dead (N = 50) | p-Value | |
|---|---|---|---|
| Age—Years | 56 ± 13 | 58 ± 12 | 0.395 |
| Sex—Female no. (%) | 32 (39) | 19 (38) | 0.949 |
| Days of hospitalization before MET evaluation | 3 (0; 13) | 10 (0; 23) | 0.032 * |
| Days between critical illness symptoms and MET evaluation—median (IQR) | 0 (0; 1) | 0 (0; 1) | 0.509 |
| CCI | 5.3 ± 2.4 | 5.0 ± 2.0 | 0.407 |
| SOFA score † | 5.9 ± 2.5 | 8.0 ± 2.6 | <0.001 * |
| MEWS † | 3.8 ± 2.2 | 4.9 ± 2.3 | 0.007 * |
| ECOG performance status—median (IQR) | 0 (0; 1) | 0 (0; 1) | 0.163 |
| PaO2/FiO2—mmHg † | 241 ± 115 | 212 ± 113 | 0.201 |
| Amine support—no. (%) † | 7 (8) | 5 (10) | 0.760 |
| Neutropenia £—no. (%) | 30 (36) | 16 (32) | 0.626 |
| Pharmacological immunosuppression—no. (%) | 35 (54) | 27 (42) | 0.185 |
| Sepsis—no. (%) | 30 (36) | 28 (56) | 0.025 * |
| ICU admission—no. (%) | 37 (45) | 47 (94) | <0.001 * |
| Immediately Admitted to ICU (N = 53) | 2 or More MET Evaluations (N = 68) | p-Value | |
|---|---|---|---|
| Respiratory rate >30 bpm †—no. (%) | 19 (36) | 19 (28) | 0.042 * |
| Heart rate >130 bpm †—no. (%) | 13 (25) | 8 (12) | <0.001 * |
| Systolic blood pressure <70 mmHg †—no. (%) | 15 (28) | 1 (2) | <0.001 * |
| Mental status alteration †—no. (%) | 12 (23) | 4 (6) | 0.010 * |
| SOFA score † | 7.9 ± 2.9 | 6.0 ± 2.2 | <0.001 * |
| MEWS † | 5.6 ± 2.5 | 3.5 ± 1.6 | <0.001 * |
| PaO2/FiO2—mmHg † | 213 ± 126 | 239 ± 108 | 0.252 |
| Neutropenia—no. (%) | 41 (77) | 38 (56) | 0.014 * |
| Pharmacological immunosuppression—no. (%) | 23 (43) | 32 (47) | 0.688 |
| Sepsis—no. (%) | 28 (52) | 28 (41) | 0.202 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vergnano, B.; Signori, D.; Benini, A.; Calcinati, S.; Bettini, F.; Verga, L.; Borin, L.M.; Cavalca, F.; Gambacorti-Passerini, C.; Bellani, G.; et al. Safety and Effectiveness of Intensive Treatments Administered Outside the Intensive Care Unit to Hematological Critically Ill Patients: An Intensive Care without Walls Trial. J. Clin. Med. 2023, 12, 6281. https://doi.org/10.3390/jcm12196281
Vergnano B, Signori D, Benini A, Calcinati S, Bettini F, Verga L, Borin LM, Cavalca F, Gambacorti-Passerini C, Bellani G, et al. Safety and Effectiveness of Intensive Treatments Administered Outside the Intensive Care Unit to Hematological Critically Ill Patients: An Intensive Care without Walls Trial. Journal of Clinical Medicine. 2023; 12(19):6281. https://doi.org/10.3390/jcm12196281
Chicago/Turabian StyleVergnano, Beatrice, Davide Signori, Annalisa Benini, Serena Calcinati, Francesca Bettini, Luisa Verga, Lorenza Maria Borin, Fabrizio Cavalca, Carlo Gambacorti-Passerini, Giacomo Bellani, and et al. 2023. "Safety and Effectiveness of Intensive Treatments Administered Outside the Intensive Care Unit to Hematological Critically Ill Patients: An Intensive Care without Walls Trial" Journal of Clinical Medicine 12, no. 19: 6281. https://doi.org/10.3390/jcm12196281
APA StyleVergnano, B., Signori, D., Benini, A., Calcinati, S., Bettini, F., Verga, L., Borin, L. M., Cavalca, F., Gambacorti-Passerini, C., Bellani, G., & Foti, G. (2023). Safety and Effectiveness of Intensive Treatments Administered Outside the Intensive Care Unit to Hematological Critically Ill Patients: An Intensive Care without Walls Trial. Journal of Clinical Medicine, 12(19), 6281. https://doi.org/10.3390/jcm12196281