

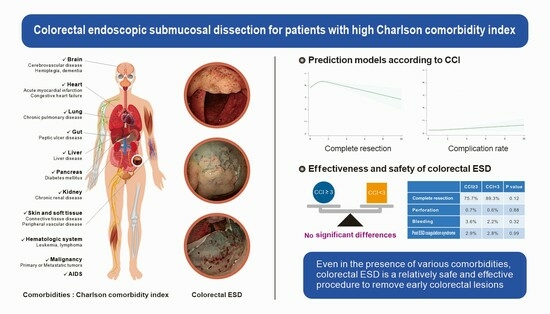
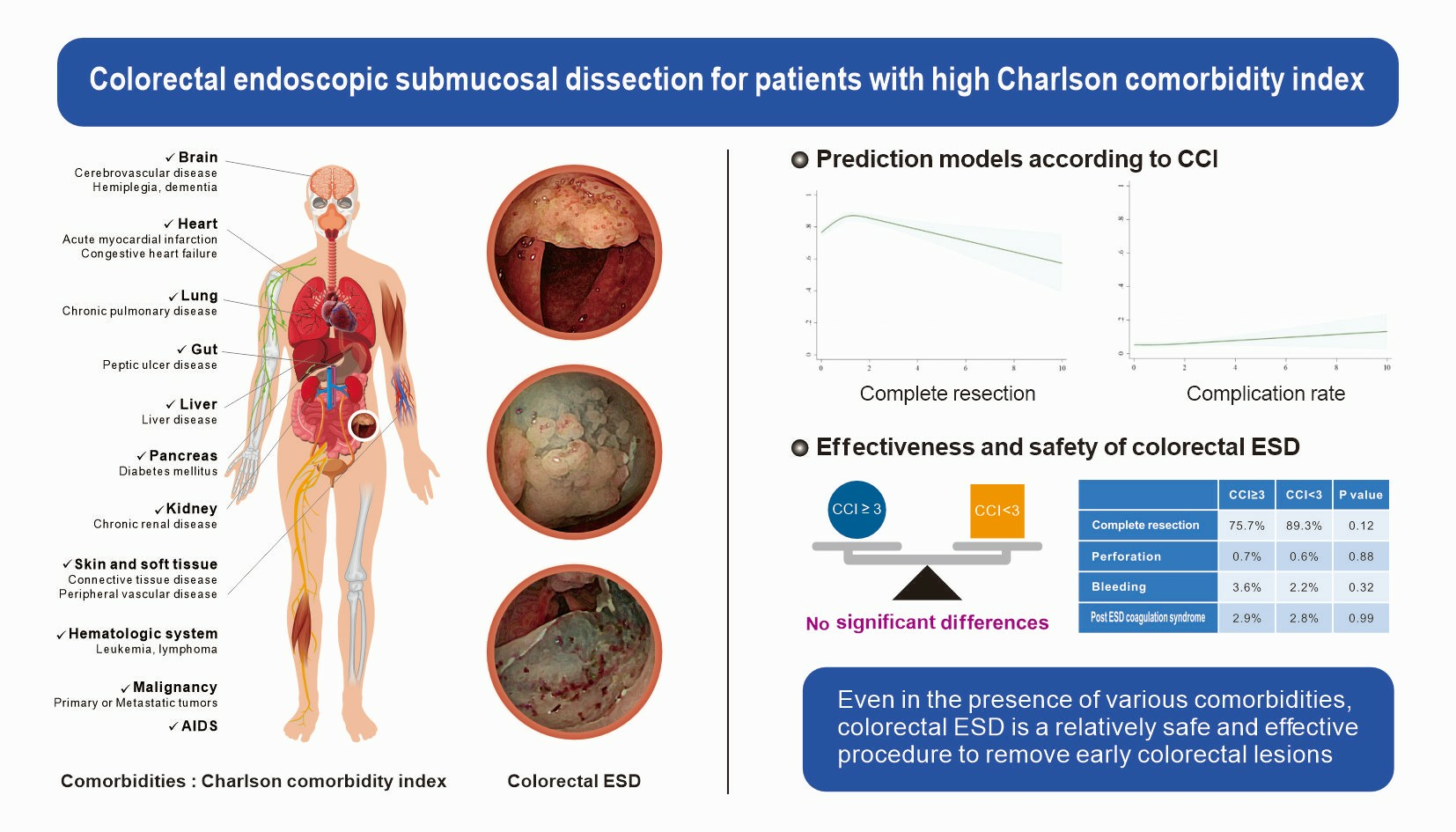
Effectiveness and Safety of Endoscopic Submucosal Dissection for Colorectal Neoplasm in Patients with High Charlson Comorbidity Index Score: A HASID Multicenter Study
 , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Patients
2.2. Data Collection and Outcomes
2.3. Statistical Analysis
3. Results
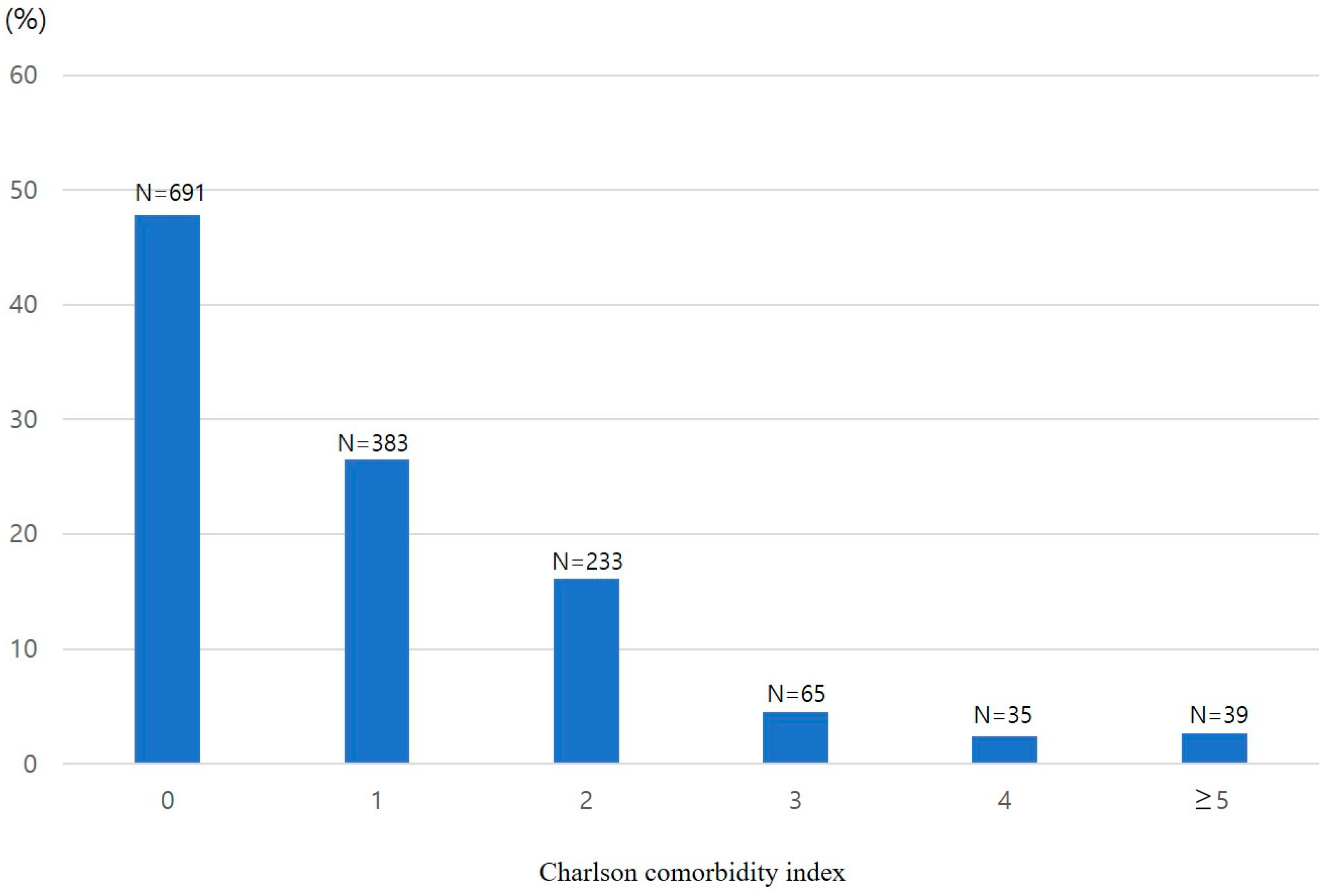
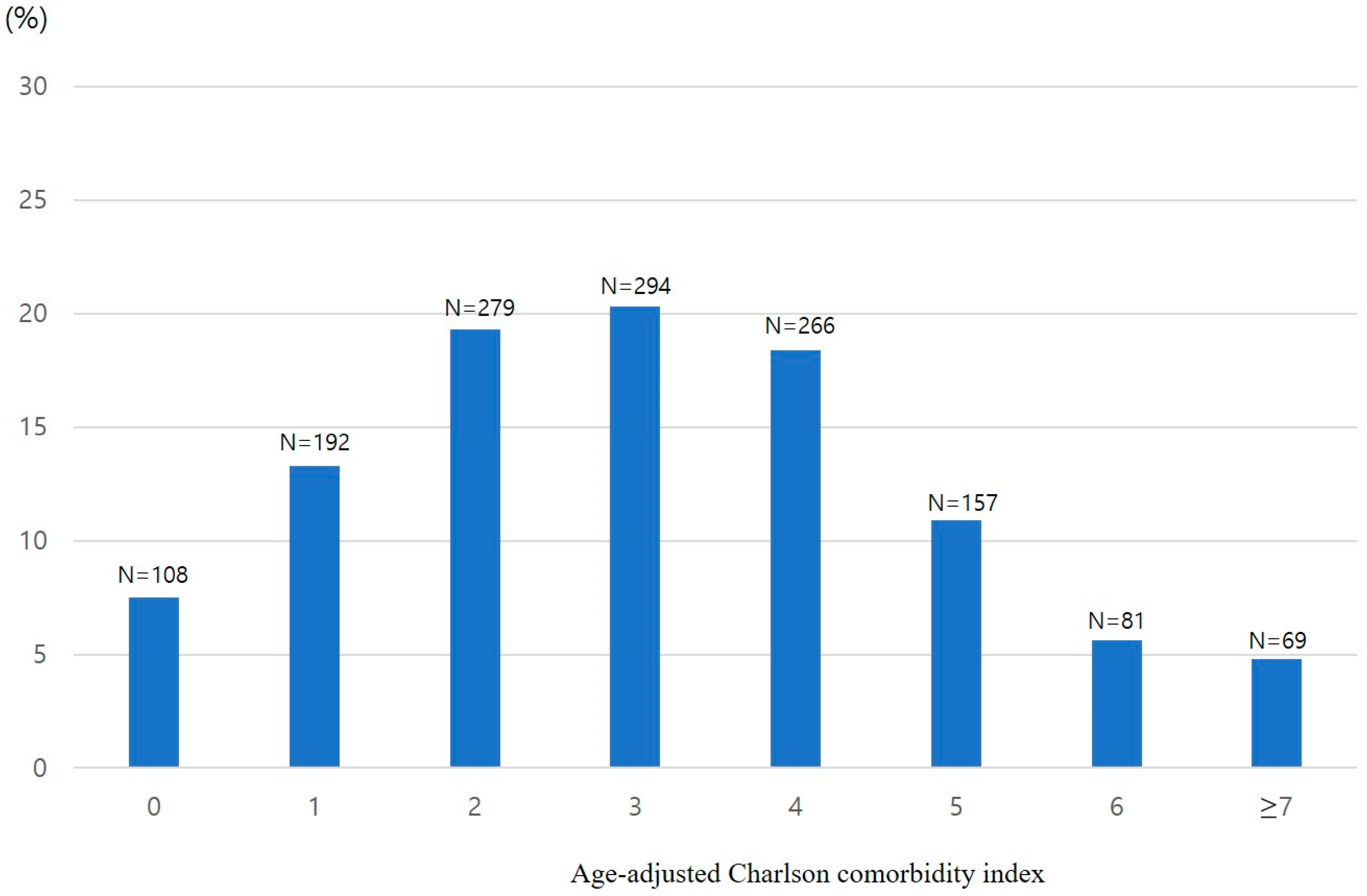
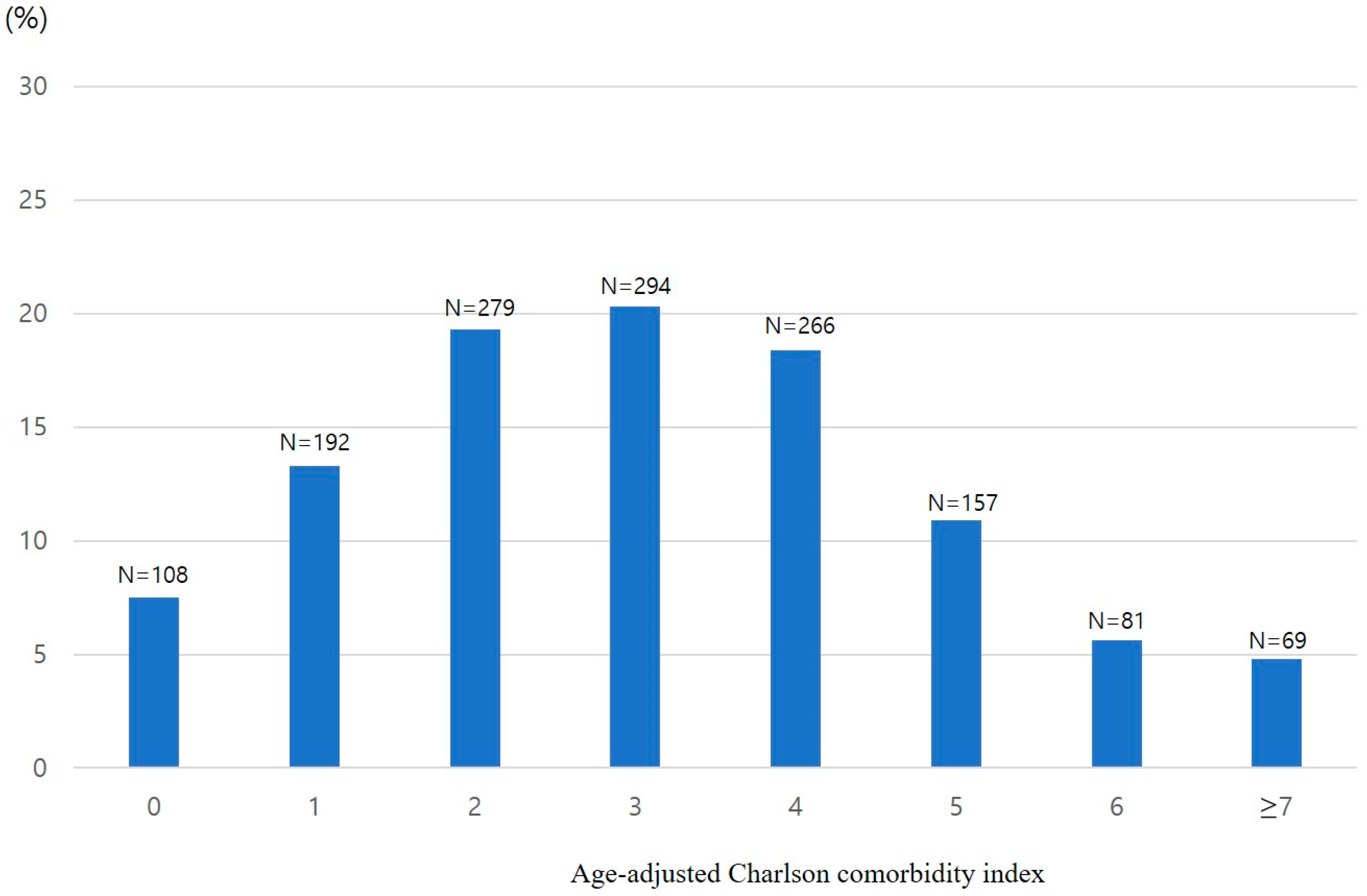
3.1. Patients and Comorbidities
3.2. Procedures
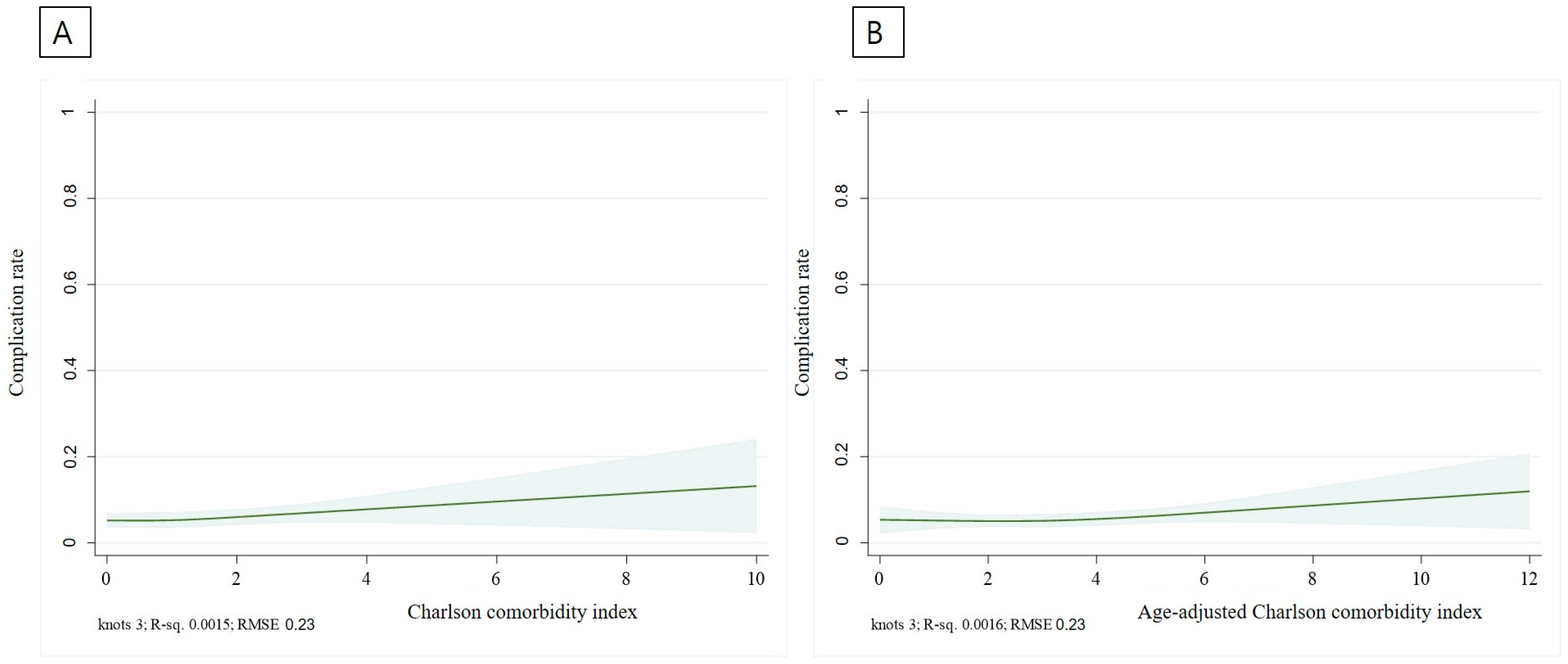
3.3. Treatment Outcome and Complications
3.4. Long-Term Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Jullumstrø, E.; Wibe, A.; Lydersen, S.; Edna, T.H. Colon cancer incidence, presentation, treatment and outcomes over 25 years. Color. Dis. 2011, 13, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Otake, Y.; Sakamoto, T.; Nakajima, T.; Yamada, M.; Haruyama, S.; So, E.; Abe, S.; Matsuda, T. Indications for and technical aspects of colorectal endoscopic submucosal dissection. Gut Liver 2013, 7, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.W.; Byeon, J.S. Endoscopic diagnosis and treatment of early colorectal cancer. Intest. Res. 2022, 20, 281–290. [Google Scholar] [CrossRef]
- Park, C.H.; Yang, D.H.; Kim, J.W.; Kim, J.H.; Kim, J.H.; Min, Y.W.; Lee, S.H.; Bae, J.H.; Chung, H.; Choi, K.D.; et al. Clinical practice guideline for endoscopic resection of early gastrointestinal cancer. Intest. Res. 2021, 19, 127–157. [Google Scholar] [CrossRef]
- Ferlitsch, M.; Moss, A.; Hassan, C.; Bhandari, P.; Dumonceau, J.M.; Paspatis, G.; Jover, R.; Langner, C.; Bronzwaer, M.; Nalankilli, K.; et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2017, 49, 270–297. [Google Scholar] [CrossRef]
- Yoshida, N.; Naito, Y.; Sakai, K.; Sumida, Y.; Kanemasa, K.; Inoue, K.; Morimoto, Y.; Konishi, H.; Wakabayashi, N.; Kokura, S.; et al. Outcome of endoscopic submucosal dissection for colorectal tumors in elderly people. Int. J. Color. Dis. 2010, 25, 455–461. [Google Scholar] [CrossRef]
- Takahashi, Y.; Mizuno, K.I.; Takahashi, K.; Sato, H.; Hashimoto, S.; Takeuchi, M.; Kobayashi, M.; Yokoyama, J.; Sato, Y.; Terai, S. Long-term outcomes of colorectal endoscopic submucosal dissection in elderly patients. Int. J. Color. Dis. 2017, 32, 567–573. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Wellejus Albertsen, L.; Heide-Jørgensen, U.; Schmidt, S.A.J.; Grey, C.; Jackson, R.; Sørensen, H.T.; Schmidt, M. The DANish Comorbidity Index for Acute Myocardial Infarction (DANCAMI): Development, Validation and Comparison with Existing Comorbidity Indices. Clin. Epidemiol. 2020, 12, 1299–1311. [Google Scholar] [CrossRef]
- Jepsen, P.; Vilstrup, H.; Andersen, P.K.; Lash, T.L.; Sørensen, H.T. Comorbidity and survival of Danish cirrhosis patients: A nationwide population-based cohort study. Hepatology 2008, 48, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Kastner, C.; Armitage, J.; Kimble, A.; Rawal, J.; Carter, P.G.; Venn, S. The Charlson comorbidity score: A superior comorbidity assessment tool for the prostate cancer multidisciplinary meeting. Prostate Cancer Prostatic Dis. 2006, 9, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Tuty Kuswardhani, R.A.; Henrina, J.; Pranata, R.; Anthonius Lim, M.; Lawrensia, S.; Suastika, K. Charlson comorbidity index and a composite of poor outcomes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2020, 14, 2103–2109. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Koseki, Y.; Hikage, M.; Fujiya, K.; Kamiya, S.; Tanizawa, Y.; Bando, E.; Terashima, M. Utility of a modified age-adjusted Charlson Comorbidity Index in predicting cause-specific survival among patients with gastric cancer. Eur. J. Surg. Oncol. 2021, 47, 2010–2015. [Google Scholar] [CrossRef]
- Tian, Y.; Jian, Z.; Xu, B.; Liu, H. Age-adjusted Charlson comorbidity index score as predictor of survival of patients with digestive system cancer who have undergone surgical resection. Oncotarget 2017, 8, 79453–79461. [Google Scholar] [CrossRef]
- Marventano, S.; Grosso, G.; Mistretta, A.; Bogusz-Czerniewicz, M.; Ferranti, R.; Nolfo, F.; Giorgianni, G.; Rametta, S.; Drago, F.; Basile, F.; et al. Evaluation of four comorbidity indices and Charlson comorbidity index adjustment for colorectal cancer patients. Int. J. Color. Dis. 2014, 29, 1159–1169. [Google Scholar] [CrossRef]
- Zhang, N.; Lin, Q.; Jiang, H.; Zhu, H. Age-adjusted Charlson Comorbidity Index as effective predictor for in-hospital mortality of patients with cardiac arrest: A retrospective study. BMC Emerg. Med. 2023, 23, 7. [Google Scholar] [CrossRef]
- Endoscopic Classification Review Group. Update on the paris classification of superficial neoplastic lesions in the digestive tract. Endoscopy 2005, 37, 570–578. [Google Scholar] [CrossRef]
- Eisen, G.M.; Baron, T.H.; Dominitz, J.A.; Faigel, D.O.; Goldstein, J.L.; Johanson, J.F.; Mallery, J.S.; Raddawi, H.M.; Vargo, J.J., 2nd; Waring, J.P.; et al. Guideline on the management of anticoagulation and antiplatelet therapy for endoscopic procedures. Gastrointest. Endosc. 2002, 55, 775–779. [Google Scholar] [CrossRef]
- Tanaka, S.; Kashida, H.; Saito, Y.; Yahagi, N.; Yamano, H.; Saito, S.; Hisabe, T.; Yao, T.; Watanabe, M.; Yoshida, M.; et al. Japan Gastroenterological Endoscopy Society guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig. Endosc. 2020, 32, 219–239. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kim, S.Y.; Lee, J. Prognosis and risk factors of electrocoagulation syndrome after endoscopic submucosal dissection in the colon and rectum. Large cohort study. Surg. Endosc. 2022, 36, 6243–6249. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, Y.; Takeuchi, Y.; Iwatsubo, T.; Kato, M.; Hamada, K.; Tonai, Y.; Matsuura, N.; Kanesaka, T.; Yamashina, T.; Arao, M.; et al. Line-assisted complete closure for a large mucosal defect after colorectal endoscopic submucosal dissection decreased post-electrocoagulation syndrome. Dig. Endosc. 2018, 30, 633–641. [Google Scholar] [CrossRef] [PubMed]
- St-Louis, E.; Iqbal, S.; Feldman, L.S.; Sudarshan, M.; Deckelbaum, D.L.; Razek, T.S.; Khwaja, K. Using the age-adjusted Charlson comorbidity index to predict outcomes in emergency general surgery. J. Trauma Acute Care Surg. 2015, 78, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Iwai, N.; Dohi, O.; Naito, Y.; Inada, Y.; Fukui, A.; Takayama, S.; Ogita, K.; Terasaki, K.; Nakano, T.; Ueda, T.; et al. Impact of the Charlson comorbidity index and prognostic nutritional index on prognosis in patients with early gastric cancer after endoscopic submucosal dissection. Dig. Endosc. 2018, 30, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Nakajo, K.; Abe, S.; Oda, I.; Ishihara, R.; Tanaka, M.; Yoshio, T.; Katada, C.; Yano, T. Impact of the Charlson Comorbidity Index on the treatment strategy and survival in elderly patients after non-curative endoscopic submucosal dissection for esophageal squamous cell carcinoma: A multicenter retrospective study. J. Gastroenterol. 2019, 54, 871–880. [Google Scholar] [CrossRef]
- Croxford, R. Restricted Cubic Spline Regression: A Brief Introduction; Paper 5621-2016; Institute for Clinical Evaluative Sciences: Toronto, ON, Canada, 2016. [Google Scholar]
- Lim, J.H.; Kim, S.G.; Kim, J.W.; Choi, Y.J.; Kwon, J.; Kim, J.Y.; Lee, Y.B.; Choi, J.; Im, J.P.; Kim, J.S.; et al. Do antiplatelets increase the risk of bleeding after endoscopic submucosal dissection of gastric neoplasms? Gastrointest. Endosc. 2012, 75, 719–727. [Google Scholar] [CrossRef]
- Ono, S.; Fujishiro, M.; Niimi, K.; Goto, O.; Kodashima, S.; Yamamichi, N.; Omata, M. Technical feasibility of endoscopic submucosal dissection for early gastric cancer in patients taking anti-coagulants or antiplatelet agents. Dig. Liver Dis. 2009, 41, 725–728. [Google Scholar] [CrossRef]
- Kim, S.; Kim, D.H.; Park, S.Y.; Park, C.H.; Kim, H.S.; Choi, S.K.; Rew, J.S. Association between Charlson comorbidity index and complications of endoscopic resection of gastric neoplasms in elderly patients. BMC Gastroenterol. 2020, 20, 213. [Google Scholar] [CrossRef]
- Kinjo, K.; Matsui, T.; Hisabe, T.; Ishihara, H.; Kojima, T.; Chuman, K.; Yasukawa, S.; Beppu, T.; Koga, A.; Ishikawa, S.; et al. Risk factors for severity of colonic diverticular hemorrhage. Intest. Res. 2018, 16, 458–466. [Google Scholar] [CrossRef]
- Soh, H.; Chun, J.; Hong, S.W.; Park, S.; Lee, Y.B.; Lee, H.J.; Cho, E.J.; Lee, J.H.; Yu, S.J.; Im, J.P.; et al. Child-Pugh B or C Cirrhosis Increases the Risk for Bleeding Following Colonoscopic Polypectomy. Gut Liver 2020, 14, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Goto, O.; Fujishiro, M.; Kodashima, S.; Ono, S.; Niimi, K.; Yamamichi, N.; Omata, M. Feasibility of endoscopic submucosal dissection for patients with chronic renal failure on hemodialysis. Dig. Endosc. 2010, 22, 45–48. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | ||
|---|---|---|
| Comorbidities, variable of CCI, n (%) | Weighting | |
| Acute myocardial infarction | 1 | 65 (4.5) |
| Congestive heart failure | 1 | 22 (1.5) |
| Peripheral vascular disease | 1 | 7 (0.5) |
| Cerebrovascular disease | 1 | 44 (3.0) |
| Dementia | 1 | 16 (1.1) |
| Connective tissue disease | 1 | 5 (0.3) |
| Chronic pulmonary disease | 1 | 15 (1.0) |
| Peptic ulcer | 1 | 2 (0.1) |
| Mild liver disease | 1 | 40 (2.8) |
| Moderate to severe liver disease | 3 | 11 (0.8) |
| Diabetes without end organ damage | 1 | 284 (19.6) |
| Diabetes with end organ damage | 2 | 22 (1.5) |
| Hemiplegia | 2 | 2 (0.1) |
| Moderate to severe renal disease | 2 | 25 (1.7) |
| Any solid tumor without metastasis | 2 | 140 (9.7) |
| Leukemia | 2 | 1 (0.1) |
| Lymphoma | 2 | 3 (0.2) |
| Metastatic solid tumor | 6 | 4 (0.3) |
| Acquired immunodeficiency syndrome | 6 | 0 |
| CCI, mean ± SD | 0.98 ± 1.34 | |
| Age-adjusted CCI, mean ± SD | 3.13 ± 1.96 |
| All Patients (n = 1446) | CCI ≥ 3 (n = 140) | CCI < 3 (n = 1306) | p-Value | |
|---|---|---|---|---|
| Age, years | 65.3 ± 11.2 | 70.6 ± 8.8 | 64.7 ± 11.2 | <0.01 |
| Female | 581 (40.2) | 41 (29.3) | 540 (41.3) | <0.01 |
| Tumor size, mm | ||||
| Long axis (mm) | 29.6 ± 12.3 | 29.3 ± 13.8 | 29.6 ± 12.1 | 0.77 |
| Short axis (mm) | 25.1 ± 10.3 | 25.3 ± 10.5 | 25.1 ± 10.3 | 0.77 |
| Tumor location | <0.01 | |||
| Right side | 486 (33.6) | 31 (22.1) | 455 (34.8) | |
| Left side | 322 (22.3) | 48 (34.3) | 274 (21.0) | |
| Rectum | 638 (44.1) | 61 (43.6) | 577 (44.2) | |
| Procedure time (min) | 47.4 ± 46.4 | 42.2 ± 36.6 | 47.9 ± 27.3 | 0.09 |
| Histology, n (%) | <0.01 | |||
| Adenoma | 774 (53.5) | 31 (22.1) | 455 (34.8) | |
| Intramucosal cancer | 300 (20.7) | 48 (34.3) | 274 (21.0) | |
| Invasive cancer | 372 (25.7) | 61 (43.6) | 577 (44.2) | |
| Medication, n (%) | ||||
| Aspirin | 127 (8.8) | 35 (25.0) | 92 (7.0) | <0.01 |
| Clopidogrel | 50 (3.5) | 15 (10.7) | 35 (2.7) | <0.01 |
| Antithrombotics | 14 (1.0) | 3 (2.1) | 11 (0.8) | 0.14 |
| Sedation, n (%) | 1018 (70.4) | 81 (57.9) | 937 (71.7) | <0.01 |
| Midazolam | 942 (65.1) | 78 (55.7) | 864 (66.2) | |
| Propofol | 5 (0.3) | 0 | 5 (0.4) | |
| Midazolam and Propofol | 71 (4.9) | 3 (2.1) | 68 (5.2) |
| Total (n = 1446) | CCI ≥ 3 (n = 140) | CCI < 3 (n = 1306) | p-Value | |
|---|---|---|---|---|
| En bloc resection | 1292 (89.3) | 126 (90.0) | 1166 (89.3) | 0.79 |
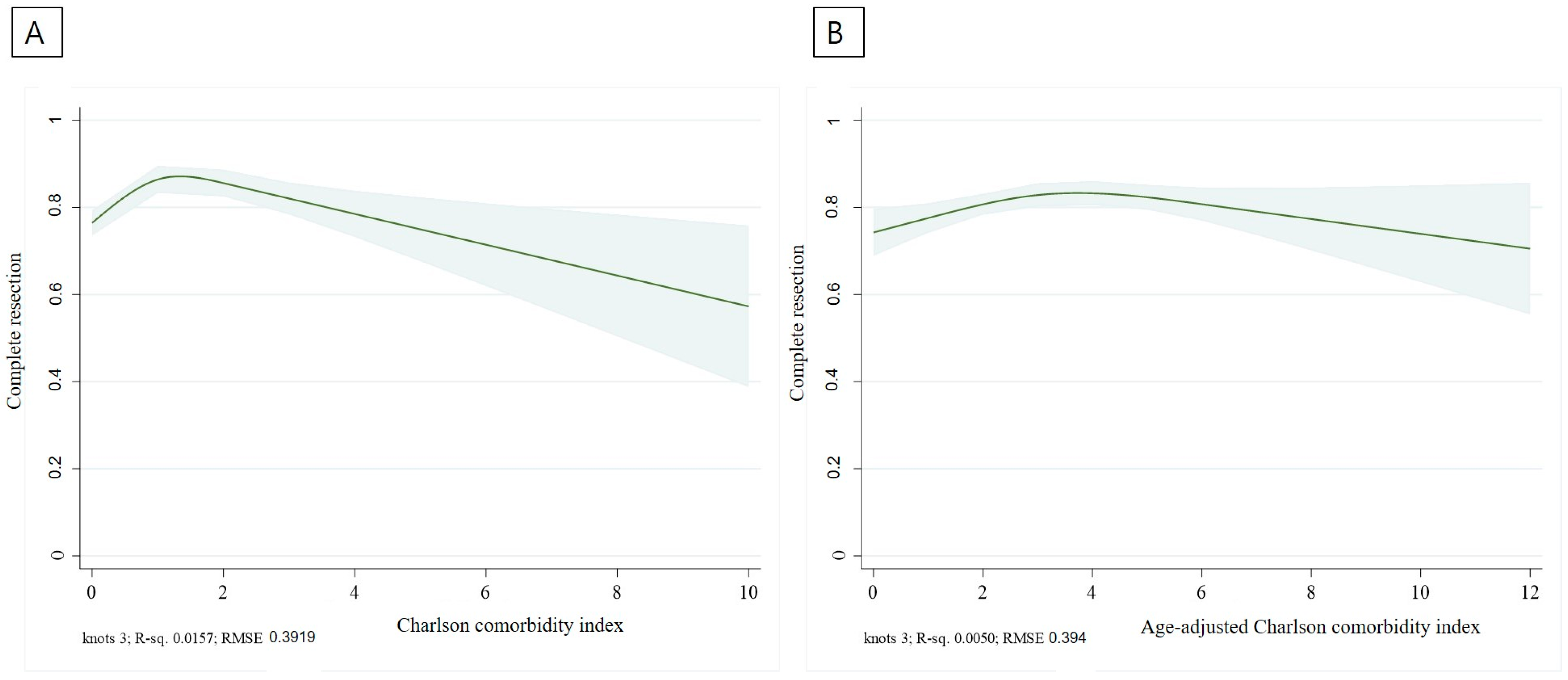
| Complete resection | 1167 (80.7) | 106 (75.7) | 1061 (81.2) | 0.12 |
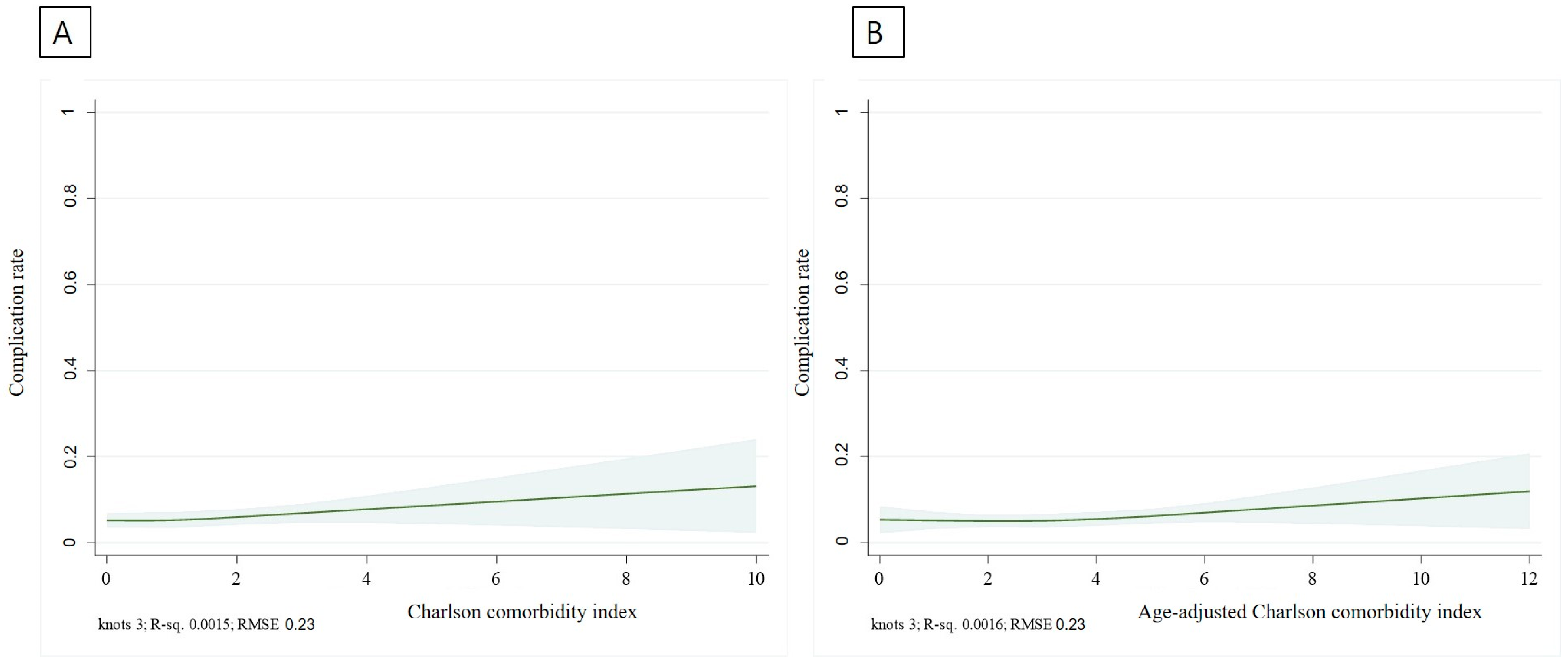
| Procedural complication | ||||
| perforation | 9 (0.6) | 1 (0.7) | 8 (0.6) | 0.88 |
| bleeding | 34 (2.4) | 5 (3.6) | 29 (2.2) | 0.32 |
| PECS | 41 (2.8) | 4 (2.9) | 37 (2.8) | 0.99 |
| Sedative complications | ||||
| Hypotension | 1 (0.1) | 0 | 1 (0.1) | 0.74 |
| Desaturation | 0 | 0 | 0 | |
| Use of antidote | 1 (0.1) | 0 | 1 (0.1) | 0.74 |
| Death | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.-H.; Jung, Y.-W.; Jin, B.-C.; Oh, H.-H.; Song, H.-Y.; Kim, S.-J.; Myung, D.-S.; Kim, S.-W.; Lee, J.; Seo, G.-S.; et al. Effectiveness and Safety of Endoscopic Submucosal Dissection for Colorectal Neoplasm in Patients with High Charlson Comorbidity Index Score: A HASID Multicenter Study. J. Clin. Med. 2023, 12, 6255. https://doi.org/10.3390/jcm12196255
Kim D-H, Jung Y-W, Jin B-C, Oh H-H, Song H-Y, Kim S-J, Myung D-S, Kim S-W, Lee J, Seo G-S, et al. Effectiveness and Safety of Endoscopic Submucosal Dissection for Colorectal Neoplasm in Patients with High Charlson Comorbidity Index Score: A HASID Multicenter Study. Journal of Clinical Medicine. 2023; 12(19):6255. https://doi.org/10.3390/jcm12196255
Chicago/Turabian StyleKim, Dong-Hyun, Yong-Wook Jung, Byung-Chul Jin, Hyung-Hoon Oh, Hyo-Yeop Song, Seong-Jung Kim, Dae-Seong Myung, Sang-Wook Kim, Jun Lee, Geom-Seog Seo, and et al. 2023. "Effectiveness and Safety of Endoscopic Submucosal Dissection for Colorectal Neoplasm in Patients with High Charlson Comorbidity Index Score: A HASID Multicenter Study" Journal of Clinical Medicine 12, no. 19: 6255. https://doi.org/10.3390/jcm12196255
APA StyleKim, D.-H., Jung, Y.-W., Jin, B.-C., Oh, H.-H., Song, H.-Y., Kim, S.-J., Myung, D.-S., Kim, S.-W., Lee, J., Seo, G.-S., Joo, Y.-E., & Kim, H.-S. (2023). Effectiveness and Safety of Endoscopic Submucosal Dissection for Colorectal Neoplasm in Patients with High Charlson Comorbidity Index Score: A HASID Multicenter Study. Journal of Clinical Medicine, 12(19), 6255. https://doi.org/10.3390/jcm12196255