

A Multi-Color Flow Cytometric Assay for Quantifying Dinutuximab Binding to Neuroblastoma Cells in Tumor, Bone Marrow, and Blood
Abstract
1. Introduction
2. Materials and Methods
2.1. Antibodies
2.2. Cell Culture
2.3. Seeding of Neuroblastoma Cell Lines into Human Blood
2.4. Flow Cytometric Evaluation of Neuroblastoma Detection and GD2 Expression
2.5. Preparation of Patient Samples
2.6. Staining of Neuroblastoma Patient Samples
3. Results
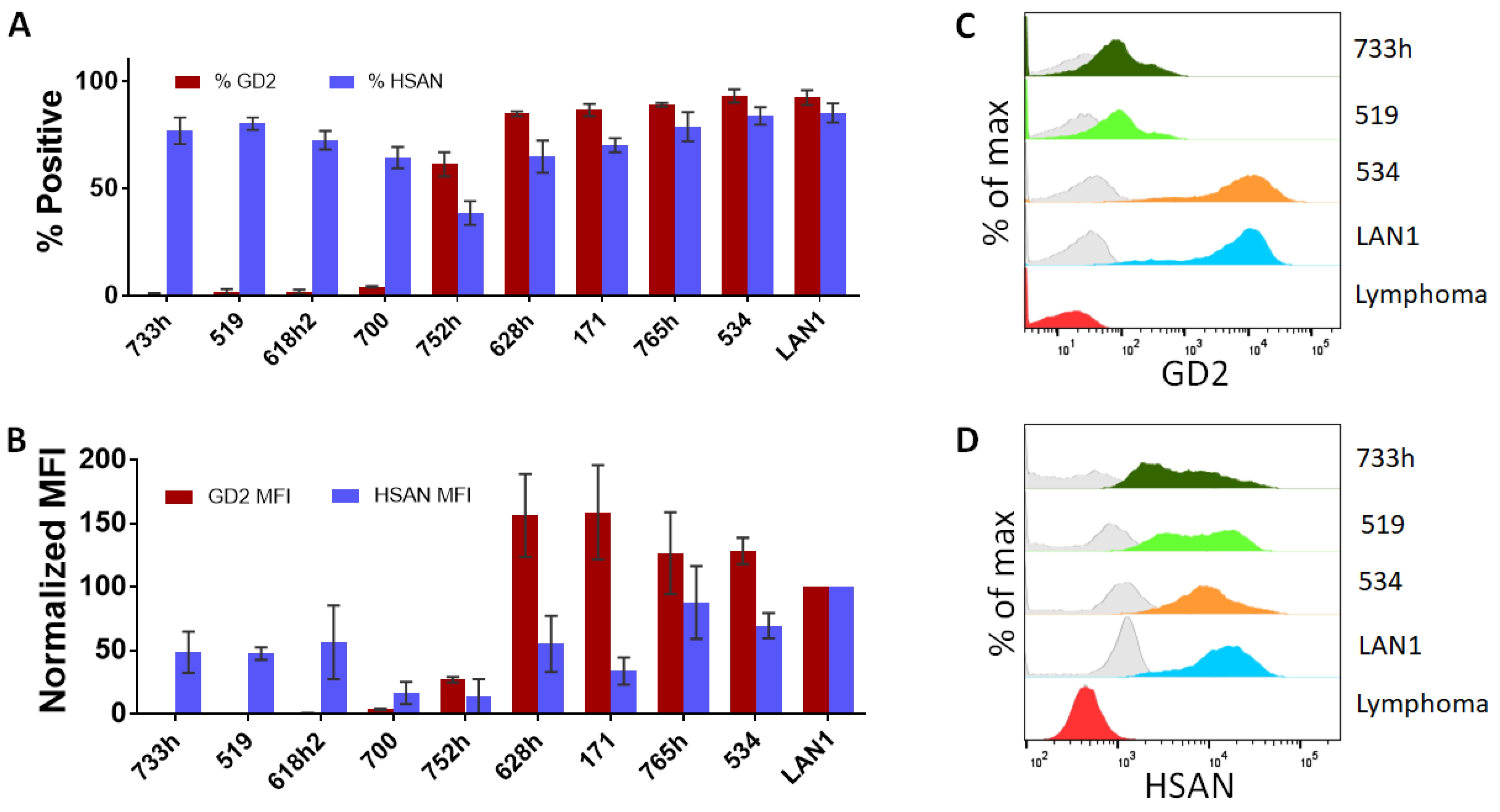
3.1. Evaluation of Surface Markers on Neuroblastoma Cell Lines
3.2. Validation of Detection of Neuroblastoma Cells from a Mixed Population
3.3. Quantification of GD2 Surface Expression from Neuroblastoma Cells in a Mixed Population
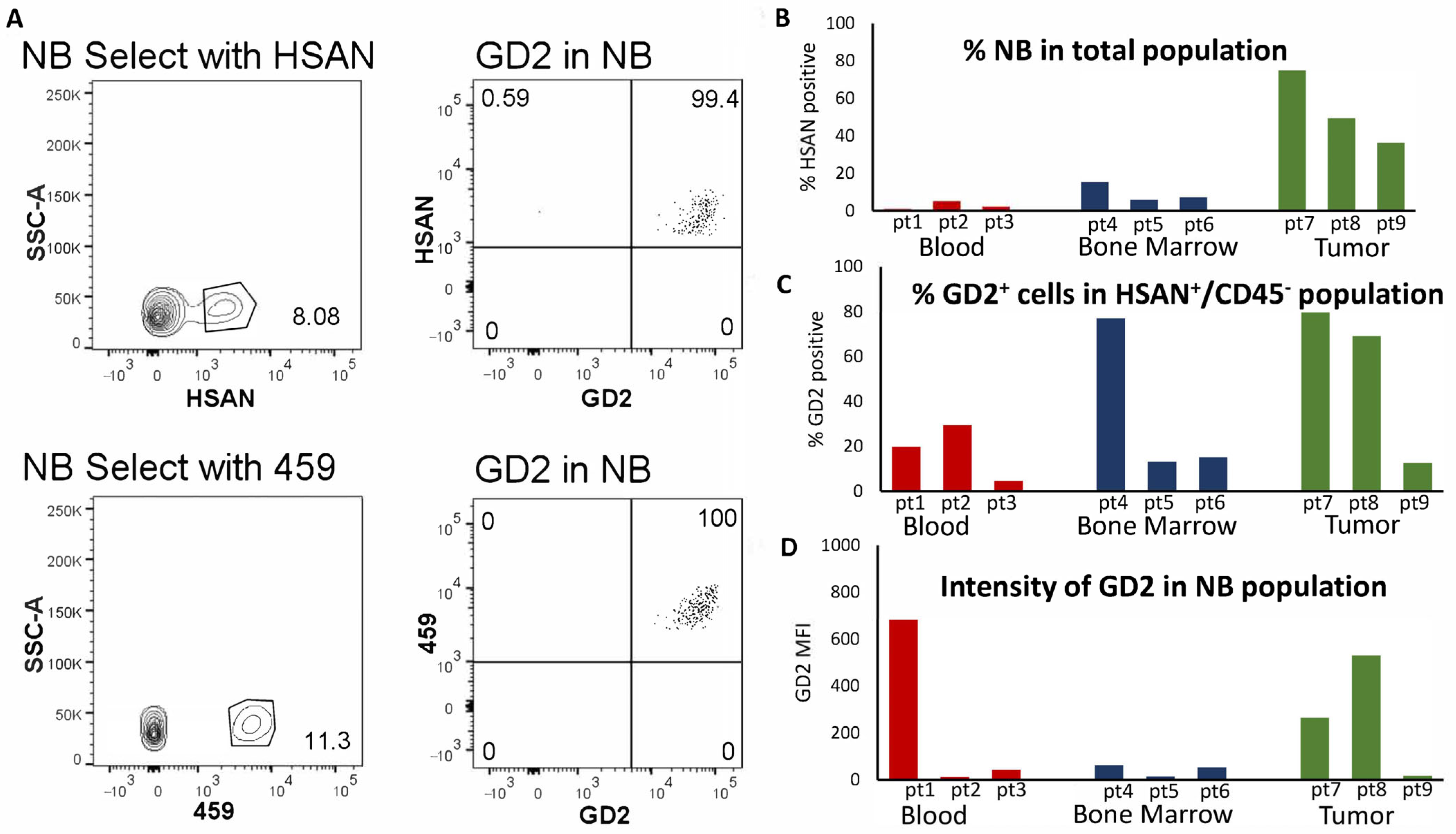
3.4. Identification of Neuroblastoma Cell Lines from Patient Blood, Bone Marrow, and Tumor Samples
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dobrenkov, K.; Cheung, N.K. GD2-targeted immunotherapy and radioimmunotherapy. Semin. Oncol. 2014, 41, 589–612. [Google Scholar] [CrossRef] [PubMed]
- Nazha, B.; Inal, C.; Owonikoko, T.K. Disialoganglioside GD2 Expression in Solid Tumors and Role as a Target for Cancer Therapy. Front. Oncol. 2020, 10, 1000. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.L.; Gilman, A.L.; Ozkaynak, M.F.; London, W.B.; Kreissman, S.G.; Chen, H.X.; Smith, M.; Anderson, B.; Villablanca, J.G.; Matthay, K.K.; et al. Anti-GD2 antibody with GM-CSF, interleukin-2, and isotretinoin for neuroblastoma. N. Engl. J. Med. 2010, 363, 1324–1334. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N.K.; Neely, J.E.; Landmeier, B.; Nelson, D.; Miraldi, F. Targeting of ganglioside GD2 monoclonal antibody to neuroblastoma. J. Nucl. Med. 1987, 28, 1577–1583. [Google Scholar] [PubMed]
- Dhillon, S. Dinutuximab: First global approval. Drugs 2015, 75, 923–927. [Google Scholar] [CrossRef]
- Ladenstein, R.; Weixler, S.; Baykan, B.; Bleeke, M.; Kunert, R.; Katinger, D.; Pribill, I.; Glander, P.; Bauer, S.; Pistoia, V.; et al. Ch14.18 antibody produced in CHO cells in relapsed or refractory Stage 4 neuroblastoma patients: A SIOPEN Phase 1 study. MAbs 2013, 5, 801–809. [Google Scholar] [CrossRef]
- Siebert, N.; Troschke-Meurer, S.; Marx, M.; Zumpe, M.; Ehlert, K.; Valteau-Couanet, D.; Luksch, R.; Manzitti, C.; Garaventa, A.; Gray, J.; et al. Impact of HACA on Immunomodulation and Pain Following Ch14.18/CHO Long-Term Infusion with Interleukin-2: A SIOPEN Phase 2 trial. Adv. Neuroblastoma Res. 2018, 26. Available online: https://www.anrmeeting.org/anr2018-abstracts/meetings-2018_abstracts.php (accessed on 20 August 2023).
- Lode, B.; Ceylan, K.; Jahns, L.; Ehlert, K.; Troschke-Meurer, S.; Siebert, N.; Lode, H. Inflammatory Response and Treatment Tolerance of Long-Term Infusion of The Anti-GD2 Antibody Ch14.18/CHO in Combination with Interleukin-2 in High-Risk Neuroblastoma. Adv. Neuroblastoma Res. 2018, 57. Available online: https://www.anrmeeting.org/anr2018-abstracts/meetings-2018_abstracts.php (accessed on 20 August 2023).
- Kailayangiri, S.; Altvater, B.; Meltzer, J.; Pscherer, S.; Luecke, A.; Dierkes, C.; Titze, U.; Leuchte, K.; Landmeier, S.; Hotfilder, M.; et al. The ganglioside antigen G(D2) is surface-expressed in Ewing sarcoma and allows for MHC-independent immune targeting. Br. J. Cancer 2012, 106, 1123–1133. [Google Scholar] [CrossRef]
- Cheung, N.K.; Cheung, I.Y.; Kushner, B.H.; Ostrovnaya, I.; Chamberlain, E.; Kramer, K.; Modak, S. Murine anti-GD2 monoclonal antibody 3F8 combined with granulocyte-macrophage colony-stimulating factor and 13-cis-retinoic acid in high-risk patients with stage 4 neuroblastoma in first remission. J. Clin. Oncol. 2012, 30, 3264–3270. [Google Scholar] [CrossRef]
- Kushner, B.H.; Kramer, K.; Cheung, N.K. Phase II trial of the anti-G(D2) monoclonal antibody 3F8 and granulocyte-macrophage colony-stimulating factor for neuroblastoma. J. Clin. Oncol. 2001, 19, 4189–4194. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.; Cheung, N.K. Engineering anti-GD2 monoclonal antibodies for cancer immunotherapy. FEBS Lett. 2014, 588, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N.K.; Guo, H.; Hu, J.; Tassev, D.V.; Cheung, I.Y. Humanizing murine IgG3 anti-GD2 antibody m3F8 substantially improves antibody-dependent cell-mediated cytotoxicity while retaining targeting in vivo. Oncoimmunology 2012, 1, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Bradford, D.; Singh, H.; Donoghue, M. FDA regulatory considerations for the review of drugs intended to treat pediatric cancers and rare tumors. Curr. Opin. Pediatr. 2023, 35, 48–54. [Google Scholar] [CrossRef]
- Yamane, B.H.; Hank, J.A.; Albertini, M.R.; Sondel, P.M. The development of antibody-IL-2 based immunotherapy with hu14.18-IL2 (EMD-273063) in melanoma and neuroblastoma. Expert Opin. Investig. Drugs 2009, 18, 991–1000. [Google Scholar] [CrossRef]
- Shusterman, S.; London, W.B.; Gillies, S.D.; Hank, J.A.; Voss, S.D.; Seeger, R.C.; Reynolds, C.P.; Kimball, J.; Albertini, M.R.; Wagner, B.; et al. Antitumor activity of hu14.18-IL2 in patients with relapsed/refractory neuroblastoma: A Children’s Oncology Group (COG) phase II study. J. Clin. Oncol. 2010, 28, 4969–4975. [Google Scholar] [CrossRef]
- Federico, S.M.; McCarville, M.B.; Shulkin, B.L.; Sondel, P.M.; Hank, J.A.; Hutson, P.; Meagher, M.; Shafer, A.; Ng, C.Y.; Leung, W.; et al. A Pilot Trial of Humanized Anti-GD2 Monoclonal Antibody (hu14.18K322A) with Chemotherapy and Natural Killer Cells in Children with Recurrent/Refractory Neuroblastoma. Clin. Cancer Res. 2017, 23, 6441–6449. [Google Scholar] [CrossRef]
- Sorkin, L.S.; Otto, M.; Baldwin, W.M., 3rd; Vail, E.; Gillies, S.D.; Handgretinger, R.; Barfield, R.C.; Ming Yu, H.; Yu, A.L. Anti-GD(2) with an FC point mutation reduces complement fixation and decreases antibody-induced allodynia. Pain 2010, 149, 135–142. [Google Scholar] [CrossRef]
- Mody, R.; Naranjo, A.; Van Ryn, C.; Yu, A.L.; London, W.B.; Shulkin, B.L.; Parisi, M.T.; Servaes, S.E.; Diccianni, M.B.; Sondel, P.M.; et al. Irinotecan-temozolomide with temsirolimus or dinutuximab in children with refractory or relapsed neuroblastoma (COG ANBL1221): An open-label, randomised, phase 2 trial. Lancet Oncol. 2017, 18, 946–957. [Google Scholar] [CrossRef]
- Markham, A. Naxitamab: First Approval. Drugs 2021, 81, 291–296. [Google Scholar] [CrossRef]
- Gargett, T.; Yu, W.; Dotti, G.; Yvon, E.S.; Christo, S.N.; Hayball, J.D.; Lewis, I.D.; Brenner, M.K.; Brown, M.P. GD2-specific CAR T Cells Undergo Potent Activation and Deletion Following Antigen Encounter but can be Protected From Activation-induced Cell Death by PD-1 Blockade. Mol. Ther. 2016, 24, 1135–1149. [Google Scholar] [CrossRef] [PubMed]
- Del Bufalo, F.; De Angelis, B.; Caruana, I.; Del Baldo, G.; De Ioris, M.A.; Serra, A.; Mastronuzzi, A.; Cefalo, M.G.; Pagliara, D.; Amicucci, M.; et al. GD2-CART01 for Relapsed or Refractory High-Risk Neuroblastoma. N. Engl. J. Med. 2023, 388, 1284–1295. [Google Scholar] [CrossRef] [PubMed]
- Schumacher-Kuckelkorn, R.; Volland, R.; Gradehandt, A.; Hero, B.; Simon, T.; Berthold, F. Lack of immunocytological GD2 expression on neuroblastoma cells in bone marrow at diagnosis, during treatment, and at recurrence. Pediatr. Blood Cancer 2017, 64, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Terzic, T.; Cordeau, M.; Herblot, S.; Teira, P.; Cournoyer, S.; Beaunoyer, M.; Peuchmaur, M.; Duval, M.; Sartelet, H. Expression of Disialoganglioside (GD2) in Neuroblastic Tumors: A Prognostic Value for Patients Treated With Anti-GD2 Immunotherapy. Pediatr. Dev. Pathol. 2018, 21, 355–362. [Google Scholar] [CrossRef]
- Keyel, M.; Davidson, H.; Nguyen, T.; Reynolds, C.P. Association of Anti-Tumor Activity in Neuroblastoma Patient-Derived Xenografts with Levels of GD2 Expression. Adv. Neuroblastoma Res. 2018, 101. Available online: https://www.anrmeeting.org/anr2018-abstracts/meetings-2018_abstracts.php (accessed on 20 August 2023).
- Keyel, M.E.; Reynolds, C.P. Spotlight on dinutuximab in the treatment of high-risk neuroblastoma: Development and place in therapy. Biologics 2019, 13, 1–12. [Google Scholar] [CrossRef]
- Kushner, B.H.; Cheung, N.K. GM-CSF enhances 3F8 monoclonal antibody-dependent cellular cytotoxicity against human melanoma and neuroblastoma. Blood 1989, 73, 1936–1941. [Google Scholar] [CrossRef]
- Sivori, S.; Parolini, S.; Marcenaro, E.; Castriconi, R.; Pende, D.; Millo, R.; Moretta, A. Involvement of natural cytotoxicity receptors in human natural killer cell-mediated lysis of neuroblastoma and glioblastoma cell lines. J. Neuroimmunol. 2000, 107, 220–225. [Google Scholar] [CrossRef]
- Tarek, N.; Le Luduec, J.B.; Gallagher, M.M.; Zheng, J.; Venstrom, J.M.; Chamberlain, E.; Modak, S.; Heller, G.; Dupont, B.; Cheung, N.K.; et al. Unlicensed NK cells target neuroblastoma following anti-GD2 antibody treatment. J. Clin. Investig. 2012, 122, 3260–3270. [Google Scholar] [CrossRef]
- Asgharzadeh, S.; Salo, J.A.; Ji, L.; Oberthuer, A.; Fischer, M.; Berthold, F.; Hadjidaniel, M.; Liu, C.W.; Metelitsa, L.S.; Pique-Regi, R.; et al. Clinical significance of tumor-associated inflammatory cells in metastatic neuroblastoma. J. Clin. Oncol. 2012, 30, 3525–3532. [Google Scholar] [CrossRef]
- Chen, R.L.; Reynolds, C.P.; Seeger, R.C. Neutrophils are cytotoxic and growth-inhibiting for neuroblastoma cells with an anti-GD2 antibody but, without cytotoxicity, can be growth-stimulating. Cancer Immunol. Immunother. 2000, 48, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Nysom, K.; Morad, A.G.; Rafael, M.S.; Zier, J.; Marachelian, A.; Watt, T.; Morgenstern, D.A. Pain mitigation and management strategies for anti-GD2 infusions: An expert consensus. Pediatr. Blood Cancer 2023, 70, e30217. [Google Scholar] [CrossRef] [PubMed]
- Jain, N.; Sattar, S.; Inglott, S.; Burchill, S.; Fisher, J.; Serban, A.M.; Thomas, R.; Connor, C.; Ghara, N.; Chowdhury, T.; et al. Flow cytometry of bone marrow aspirates from neuroblastoma patients is a highly sensitive technique for quantification of low-level neuroblastoma. F1000Research 2021, 10, 947. [Google Scholar] [CrossRef] [PubMed]
- Furlanetto, G.; Spagnol, F.; Alegretti, A.P.; Farias, M.G.; Soares, V.J.; Daudt, L.E.; Loss, J.F.; Scroferneker, M.L.; Michalowski, M.B. Flow cytometry as a diagnostic tool in neuroblastoma. J. Immunol. Methods 2021, 498, 113135. [Google Scholar] [CrossRef] [PubMed]
- Manenq, C.; Lesesve, J.F.; Dreumont, N.; Massin, F.; Salignac, S.; Mansuy, L.; Chastagner, P.; Latger-Cannard, V.; Broseus, J. Combined use of multiparametric flow cytometry and cytomorphology to enhance detection of neuroblastoma metastatic cells in bone marrow. Int. J. Lab. Hematol. 2020, 42, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.G.; Reynolds, C.P. Monoclonal antibody recognizing a human neuroblastoma-associated antigen. Diagn. Clin. Immunol. 1987, 5, 209–220. [Google Scholar] [PubMed]
- Moss, T.J.; Reynolds, C.P.; Sather, H.N.; Romansky, S.G.; Hammond, G.D.; Seeger, R.C. Prognostic value of immunocytologic detection of bone marrow metastases in neuroblastoma. N. Engl. J. Med. 1991, 324, 219–226. [Google Scholar] [CrossRef]
- Reynolds, C.P.; Seeger, R.C.; Vo, D.D.; Black, A.T.; Wells, J.; Ugelstad, J. Model system for removing neuroblastoma cells from bone marrow using monoclonal antibodies and magnetic immunobeads. Cancer Res. 1986, 46, 5882–5886. [Google Scholar]
- Gabay, C.; Ben-Bassat, H.; Schlesinger, M.; Laskov, R. Somatic mutations and intraclonal variations in the rearranged Vkappa genes of B-non-Hodgkin’s lymphoma cell lines. Eur. J. Haematol. 1999, 63, 180–191. [Google Scholar] [CrossRef]
- Baruch, M.; Hochberg, M.; Gabay, C.; Ben-Bassat, H.; Shlomai, Z.; Laskov, R. Molecular characterization of an unusual non-Hodgkin’s B-lymphoma cell line (“Farage”) lacking the ability to produce immunoglobulin polypeptide chains. Leuk. Lymphoma 1996, 21, 485–495. [Google Scholar] [CrossRef]
- Koneru, B.; Farooqi, A.; Nguyen, T.H.; Chen, W.H.; Hindle, A.; Eslinger, C.; Makena, M.R.; Burrow, T.A.; Wilson, J.; Smith, A.; et al. ALT neuroblastoma chemoresistance due to telomere dysfunction-induced ATM activation is reversible with ATM inhibitor AZD0156. Sci. Transl. Med. 2021, 13, eabd5750. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.P.; Seeger, R.C.; Satake, N.; Monforte-Munoz, H.L.; Keshelava, N.; Bailey, H.H.; Reynolds, C.P. Buthionine sulfoximine and myeloablative concentrations of melphalan overcome resistance in a melphalan-resistant neuroblastoma cell line. J. Pediatr. Hematol. Oncol. 2001, 23, 500–505. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Seeger, R.C.; Rayner, S.A.; Banerjee, A.; Chung, H.; Laug, W.E.; Neustein, H.B.; Benedict, W.F. Morphology, growth, chromosomal pattern and fibrinolytic activity of two new human neuroblastoma cell lines. Cancer Res. 1977, 37, 1364–1371. [Google Scholar] [PubMed]
- Mujoo, K.; Cheresh, D.A.; Yang, H.M.; Reisfeld, R.A. Disialoganglioside GD2 on human neuroblastoma cells: Target antigen for monoclonal antibody-mediated cytolysis and suppression of tumor growth. Cancer Res. 1987, 47, 1098–1104. [Google Scholar]
- Mueller, B.M.; Romerdahl, C.A.; Gillies, S.D.; Reisfeld, R.A. Enhancement of antibody-dependent cytotoxicity with a chimeric anti-GD2 antibody. J. Immunol. 1990, 144, 1382–1386. [Google Scholar] [CrossRef]
- Berois, N.; Osinaga, E. Glycobiology of neuroblastoma: Impact on tumor behavior, prognosis, and therapeutic strategies. Front. Oncol. 2014, 4, 114. [Google Scholar] [CrossRef]
- Komada, Y.; Zhang, X.L.; Zhou, Y.W.; Inaba, H.; Deguchi, T.; Azuma, E.; Sakurai, M. Flow cytometric analysis of peripheral blood and bone marrow for tumor cells in patients with neuroblastoma. Cancer 1998, 82, 591–599. [Google Scholar] [CrossRef]
- Dondero, A.; Morini, M.; Cangelosi, D.; Mazzocco, K.; Serra, M.; Spaggiari, G.M.; Rotta, G.; Tondo, A.; Locatelli, F.; Castellano, A.; et al. Multiparametric flow cytometry highlights B7-H3 as a novel diagnostic/therapeutic target in GD2neg/low neuroblastoma variants. J. Immunother. Cancer 2021, 9, e002293. [Google Scholar] [CrossRef]
- Swerts, K.; De Moerloose, B.; Dhooge, C.; Brichard, B.; Benoit, Y.; Laureys, G.; Philippe, J. Detection of residual neuroblastoma cells in bone marrow: Comparison of flow cytometry with immunocytochemistry. Cytom. Part B Clin. Cytom. 2004, 61, 9–19. [Google Scholar] [CrossRef]
- Yu, A.L.; Gilman, A.L.; Ozkaynak, M.F.; Naranjo, A.; Diccianni, M.B.; Gan, J.; Hank, J.A.; Batova, A.; London, W.B.; Tenney, S.C.; et al. Long-Term Follow-up of a Phase III Study of ch14.18 (Dinutuximab) + Cytokine Immunotherapy in Children with High-Risk Neuroblastoma: COG Study ANBL0032. Clin. Cancer Res. 2021, 27, 2179–2189. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell Lines | Oxygen Condition | Phase of Therapy | Sample Type |
|---|---|---|---|
| COG-N-765h | 5% | DX | BM |
| COG-N-752h | 5% | PD | BM |
| COG-N-733h | 5% | DX | BM |
| COG-N-700 | 20% | DX | tumor |
| COG-N-628h [41] | 5% | DX | BM |
| COG-N-618h2 | 2% | PD | BM |
| COG-N-534 [41] | 20% | PD-PM | blood |
| COG-N-519 [41] | 20% | PD-PM | blood |
| CHLA-171 [42] | 20% | PD-PM | blood |
| LA-N-1 [43] | 20% | PD | BM |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keyel, M.E.; Furr, K.L.; Kang, M.H.; Reynolds, C.P. A Multi-Color Flow Cytometric Assay for Quantifying Dinutuximab Binding to Neuroblastoma Cells in Tumor, Bone Marrow, and Blood. J. Clin. Med. 2023, 12, 6223. https://doi.org/10.3390/jcm12196223
Keyel ME, Furr KL, Kang MH, Reynolds CP. A Multi-Color Flow Cytometric Assay for Quantifying Dinutuximab Binding to Neuroblastoma Cells in Tumor, Bone Marrow, and Blood. Journal of Clinical Medicine. 2023; 12(19):6223. https://doi.org/10.3390/jcm12196223
Chicago/Turabian StyleKeyel, Michelle E., Kathryn L. Furr, Min H. Kang, and C. Patrick Reynolds. 2023. "A Multi-Color Flow Cytometric Assay for Quantifying Dinutuximab Binding to Neuroblastoma Cells in Tumor, Bone Marrow, and Blood" Journal of Clinical Medicine 12, no. 19: 6223. https://doi.org/10.3390/jcm12196223
APA StyleKeyel, M. E., Furr, K. L., Kang, M. H., & Reynolds, C. P. (2023). A Multi-Color Flow Cytometric Assay for Quantifying Dinutuximab Binding to Neuroblastoma Cells in Tumor, Bone Marrow, and Blood. Journal of Clinical Medicine, 12(19), 6223. https://doi.org/10.3390/jcm12196223