
Effects of an App-Based Mindfulness Intervention during Pregnancy on the Infant’s Prenatal Androgen Exposure: A Randomized Controlled Pilot Trial

 , , , , ,
, , , , ,  ,
,  , and
, and
Abstract
1. Introduction
Aims of the Study
2. Materials and Methods
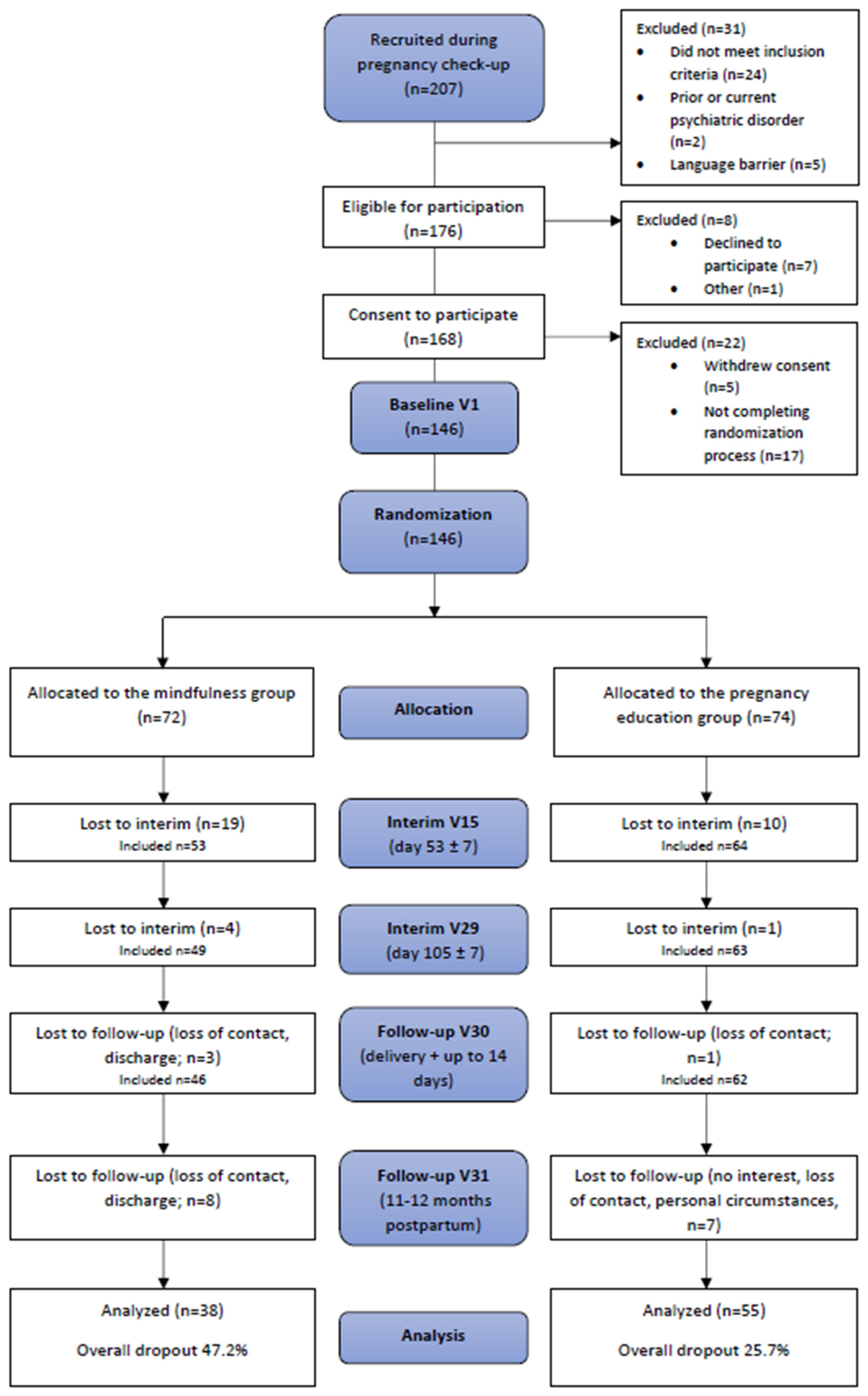
2.1. Study Cohort and Intervention
2.2. Markers of Prenatal Androgen Exposure
2.2.1. Second-to-Fourth Digit Length Ratio (2D:4D)
2.2.2. Anogenital Distance
2.3. Maternal Behavioral Phenotyping
2.4. Statistical Analyses
2.4.1. Markers of Prenatal Androgen Exposure
2.4.2. Maternal Behavioral Phenotyping
2.4.3. Dropout Analyses
3. Results
3.1. Sociodemographic Characteristics
3.2. Intervention Effects on Second-to-Fourth Digit Length Ratio (2D:4D) and Anogenital Distance
3.3. Intervention Effects on the Mothers’ Stress, Anxiety, Depressiveness, and Mindfulness Levels
3.3.1. Stress Scores (PSS-10)
3.3.2. Anxiety Scores (PRAQ-R2)
3.3.3. Depressiveness Scores (EPDS)
3.3.4. Mindfulness Scores (MAAS)
3.3.5. Mindfulness Scores (FFMQ-D)
4. Discussion
4.1. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Dropout Analyses

{kind=link}
| Predicted Outcome | Predictor(s) | OR | 95% CI | p | Model Parameters |
|---|---|---|---|---|---|
| Model 1 | |||||
| Data at V31 available | Group allocation Previous experience | 0.33 0.57 | 0.15–0.70 0.26–1.12 | 0.005 0.137 | χ2 = 12.01, df = 2, p = 0.002 Nagelkerke’s R2 = 0.11 |
| Model 2 | |||||
| Data at V31 available | Group allocation | 0.39 | 0.19–0.77 | 0.007 | χ2 = 7.40, df = 1, p = 0.006 Nagelkerke’s R2 = 0.06 |
Appendix B
| Questionnaire | Measurement Timepoint | Mindfulness Group | Pregnancy Education Group | |||
|---|---|---|---|---|---|---|
| N | Adjusted means (95% CI) | N | Adjusted means (95% CI) | Adjusted Difference (95% CI) | ||
| PSS-10 | −0.87 (−2.43; 0.70) | |||||
| V15 | 46 | 13.60 (12.25; 15.00) | 51 | 12.80 (11.44; 14.10) | ||
| V29 | 42 | 13.70 (12.31; 15.10) | 50 | 12.80 (11.51; 14.20) | ||
| V30 | 38 | 12.90 (11.45; 14.30) | 46 | 12.00 (10.66; 13.40) | ||
| V31 | 33 | 12.10 (10.68; 13.60) | 47 | 11.30 (9.92; 12.60) | ||
| EPDS | −0.02 (−1.11; 1.06) | |||||
| V15 | 47 | 5.58 (4.65; 6.52) | 59 | 5.56 (4.70; 6.42) | ||
| V29 | 45 | 5.68 (4.74; 6.63) | 56 | 5.66 (4.79; 6.53) | ||
| V30 | 37 | 5.15 (4.17; 6.14) | 52 | 5.13 (4.23; 6.03) | ||
| V31 | 35 | 5.52 (4.52; 6.51) | 52 | 5.50 (4.60; 6.40) | ||
| FFMQ-D | −2.52 (−7.13; 2.08) | |||||
| V15 | 8 | 138.00 (132.00; 144.00) | 15 | 136.00 (130.00; 141.00) | ||
| V29 | 41 | 141.00 (138.00; 145.00) | 49 | 139.00 (136.00; 142.00) | ||
| MAAS | 0.12 (−0.07; 0.31) | |||||
| V15 | 45 | 4.26 (4.10; 4.42) | 51 | 4.38 (4.23; 4.54) | ||
| V29 | 42 | 4.37 (4.20; 4.53) | 50 | 4.49 (4.33; 4.65) | ||
| V30 | 37 | 4.39 (4.22; 4.56) | 44 | 4.51 (4.35; 4.68) | ||
| V31 | 34 | 4.41 (4.24; 4.58) | 50 | 5.53 (4.37; 4.69) | ||
References
- Phoenix, C.H.; Goy, R.W.; Gerall, A.A.; Young, W.C. Organizing action of prenatally administered testosterone propionate on the tissues mediating mating behavior in the female guinea pig. Endocrinology 1959, 65, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.C.Z.; Steadman, C.J.; Lee, T.M.; Padmanabhan, V.; Lehman, M.N.; Coolen, L.M. Sex differences and effects of prenatal exposure to excess testosterone on ventral tegmental area dopamine neurons in adult sheep. Eur. J. Neurosci. 2015, 41, 1157–1166. [Google Scholar] [CrossRef] [PubMed]
- Huber, S.E.; Zoicas, I.; Reichel, M.; Mühle, C.; Büttner, C.; Ekici, A.B.; Eulenburg, V.; Lenz, B.; Kornhuber, J.; Müller, C.P. Prenatal androgen receptor activation determines adult alcohol and water drinking in a sex-specific way. Addict. Biol. 2018, 23, 904–920. [Google Scholar] [CrossRef]
- McCarthy, M.M.; Arnold, A.P.; Ball, G.F.; Blaustein, J.D.; De Vries, G.J. Sex differences in the brain: The not so inconvenient truth. J. Neurosci. 2012, 32, 2241–2247. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.V.; Ashwin, E.; Auyeung, B.; Chakrabarti, B.; Lai, M.C.; Taylor, K.; Hackett, G.; Bullmore, E.T.; Baron-Cohen, S. Fetal programming effects of testosterone on the reward system and behavioral approach tendencies in humans. Biol. Psychiatry 2012, 72, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.V.; Ashwin, E.; Auyeung, B.; Chakrabarti, B.; Taylor, K.; Hackett, G.; Bullmore, E.T.; Baron-Cohen, S. Fetal testosterone influences sexually dimorphic gray matter in the human brain. J. Neurosci. 2012, 32, 674–680. [Google Scholar] [CrossRef]
- Berenbaum, S.A.; Bryk, K.K.; Nowak, N.; Quigley, C.A.; Moffat, S. Fingers as a marker of prenatal androgen exposure. Endocrinology 2009, 150, 5119–5124. [Google Scholar] [CrossRef]
- Manning, J.; Kilduff, L.; Cook, C.; Crewther, B.; Fink, B. Digit ratio (2D:4D): A biomarker for prenatal sex steroids and adult sex steroids in challenge situations. Front. Endocrinol. 2014, 5, 9. [Google Scholar] [CrossRef]
- Zheng, Z.; Cohn, M.J. Developmental basis of sexually dimorphic digit ratios. Proc. Natl. Acad. Sci. USA 2011, 108, 16289–16294. [Google Scholar] [CrossRef]
- Talarovičová, A.; Kršková, L.; Blažeková, J. Testosterone enhancement during pregnancy influences the 2D:4D ratio and open field motor activity of rat siblings in adulthood. Horm. Behav. 2009, 55, 235–239. [Google Scholar] [CrossRef]
- Hönekopp, J.; Watson, S. Meta-analysis of digit ratio 2D:4D shows greater sex difference in the right hand. Am. J. Hum. Biol. 2010, 22, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Lutchmaya, S.; Baron-Cohen, S.; Raggatt, P.; Knickmeyer, R.; Manning, J.T. 2nd to 4th digit ratios, fetal testosterone and estradiol. Early Hum. Dev. 2004, 77, 23–28. [Google Scholar] [CrossRef]
- Ventura, T.; Gomes, M.C.; Pita, A.; Neto, M.T.; Taylor, A. Digit ratio (2D:4D) in newborns: Influences of prenatal testosterone and maternal environment. Early Hum. Dev. 2013, 89, 107–112. [Google Scholar] [CrossRef] [PubMed]
- van Anders, S.M.; Vernon, P.A.; Wilbur, C.J. Finger-length ratios show evidence of prenatal hormone-transfer between opposite-sex twins. Horm. Behav. 2006, 49, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Voracek, M.; Dressler, S.G. Digit ratio (2D:4D) in twins: Heritability estimates and evidence for a masculinized trait expression in women from opposite-sex pairs. Psychol. Rep. 2007, 100, 115–126. [Google Scholar] [CrossRef]
- Richards, G.; Browne, W.V.; Aydin, E.; Constantinescu, M.; Nave, G.; Kim, M.S.; Watson, S.J. Digit ratio (2D:4D) and congenital adrenal hyperplasia (CAH): Systematic literature review and meta-analysis. Horm. Behav. 2020, 126, 104867. [Google Scholar] [CrossRef]
- Chang, S.; Skakkebæk, A.; Trolle, C.; Bojesen, A.; Hertz, J.M.; Cohen, A.; Hougaard, D.M.; Wallentin, M.; Pedersen, A.D.; Østergaard, J.R.; et al. Anthropometry in Klinefelter syndrome--multifactorial influences due to CAG length, testosterone treatment and possibly intrauterine hypogonadism. J. Clin. Endocrinol. Metab. 2015, 100, E508–E517. [Google Scholar] [CrossRef]
- Manning, J.T.; Kilduff, L.P.; Trivers, R. Digit ratio (2D:4D) in Klinefelter’s syndrome. Andrology 2013, 1, 94–99. [Google Scholar] [CrossRef]
- van Hemmen, J.; Cohen-Kettenis, P.T.; Steensma, T.D.; Veltman, D.J.; Bakker, J. Do sex differences in CEOAEs and 2D:4D ratios reflect androgen exposure? A study in women with complete androgen insensitivity syndrome. Biol. Sex Differ. 2017, 8, 11. [Google Scholar] [CrossRef]
- Malas, M.A.; Dogan, S.; Evcil, E.H.; Desdicioglu, K. Fetal development of the hand, digits and digit ratio (2D:4D). Early Hum. Dev. 2006, 82, 469–475. [Google Scholar] [CrossRef]
- Butovskaya, M.; Burkova, V.; Apalkova, Y.; Dronova, D.; Rostovtseva, V.; Karelin, D.; Mkrtchyan, R.; Negasheva, M.; Batsevich, V. Sex, population origin, age and average digit length as predictors of digit ratio in three large world populations. Sci. Rep. 2021, 11, 8157. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, M.H.; Ellison, P.T.; Lieberman, D.E.; Demerath, E.; Towne, B. The development of sex differences in digital formula from infancy in the Fels Longitudinal Study. Proc. Biol. Sci. 2005, 272, 1473–1479. [Google Scholar] [CrossRef] [PubMed]
- Lenz, B.; Gerhardt, S.; Boroumand-Jazi, R.; Eichler, A.; Buchholz, V.N.; Fasching, P.A.; Kornhuber, J.; Banaschewski, T.; Flor, H.; Guldner, S.; et al. Sex-specific association between prenatal androgenization (second-to-fourth digit length ratio) and frontal brain volumes in adolescents. Eur. Arch. Psychiatry Clin. Neurosci. 2023, 273, 1243–1254. [Google Scholar] [CrossRef]
- Eichler, A.; Kaufmann, F.; Titzmann, A.; Fasching, P.A.; Beckmann, M.W.; Gerlach, J.; Kratz, O.; Moll, G.H.; Buchholz, V.N.; Kornhuber, J.; et al. 2D:4D biomarker reliability and validity in a within-subject pregnancy-childhood-adolescence cohort. Early Hum. Dev. 2023, 181, 105776. [Google Scholar] [CrossRef]
- Hönekopp, J.; Bartholdt, L.; Beier, L.; Liebert, A. Second to fourth digit length ratio (2D:4D) and adult sex hormone levels: New data and a meta-analytic review. Psychoneuroendocrinology 2007, 32, 313–321. [Google Scholar] [CrossRef]
- Swift-Gallant, A.; Johnson, B.A.; Di Rita, V.; Breedlove, S.M. Through a glass, darkly: Human digit ratios reflect prenatal androgens, imperfectly. Horm. Behav. 2020, 120, 104686. [Google Scholar] [CrossRef] [PubMed]
- Knickmeyer, R.C.; Woolson, S.; Hamer, R.M.; Konneker, T.; Gilmore, J.H. 2D:4D ratios in the first 2 years of life: Stability and relation to testosterone exposure and sensitivity. Horm. Behav. 2011, 60, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.I.; Hines, M. Interpreting digit ratio (2D:4D)-behavior correlations: 2D:4D sex difference, stability, and behavioral correlates and their replicability in young children. Horm. Behav. 2016, 78, 86–94. [Google Scholar] [CrossRef]
- Thankamony, A.; Pasterski, V.; Ong, K.K.; Acerini, C.L.; Hughes, I.A. Anogenital distance as a marker of androgen exposure in humans. Andrology 2016, 4, 616–625. [Google Scholar] [CrossRef]
- McIntyre, B.S.; Barlow, N.J.; Foster, P.M. Androgen-mediated development in male rat offspring exposed to flutamide in utero: Permanence and correlation of early postnatal changes in anogenital distance and nipple retention with malformations in androgen-dependent tissues. Toxicol. Sci. 2001, 62, 236–249. [Google Scholar] [CrossRef]
- Callegari, C.; Everett, S.; Ross, M.; Brasel, J.A. Anogenital ratio: Measure of fetal virilization in premature and full-term newborn infants. J. Pediatr. 1987, 111, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Yeh, S.; Tsai, M.Y.; Xu, Q.; Mu, X.M.; Lardy, H.; Huang, K.E.; Lin, H.; Yeh, S.D.; Altuwaijri, S.; Zhou, X.; et al. Generation and characterization of androgen receptor knockout (ARKO) mice: An in vivo model for the study of androgen functions in selective tissues. Proc. Natl. Acad. Sci. USA 2002, 99, 13498–13503. [Google Scholar] [CrossRef] [PubMed]
- Hönekopp, J.; Watson, S. Meta-analysis of the relationship between digit-ratio 2D:4D and aggression. Pers. Individ. Dif. 2011, 51, 381–386. [Google Scholar] [CrossRef]
- Körner, L.M.; Pause, B.M.; Meinlschmidt, G.; Tegethoff, M.; Fröhlich, S.; Kozlowski, P.; Rivet, N.; Jamey, C.; Reix, N.; Kintz, P.; et al. Prenatal testosterone exposure is associated with delay of gratification and attention problems/overactive behavior in 3-year-old boys. Psychoneuroendocrinology 2019, 104, 49–54. [Google Scholar] [CrossRef]
- Martel, M.M.; Gobrogge, K.L.; Breedlove, S.M.; Nigg, J.T. Masculinized finger-length ratios of boys, but not girls, are associated with attention-deficit/hyperactivity disorder. Behav. Neurosci. 2008, 122, 273–281. [Google Scholar] [CrossRef]
- Hönekopp, J. Digit ratio 2D:4D in relation to autism spectrum disorders, empathizing, and systemizing: A quantitative review. Autism. Res. 2012, 5, 221–230. [Google Scholar] [CrossRef]
- Rodríguez-Ramos, A.; Moriana, J.A.; García-Torres, F.; Ruiz-Rubio, M. Emotional stability is related to 2D:4D and social desirability in women: Possible implications on subjective well-being and psychopathology. PLoS ONE 2021, 16, e0248368. [Google Scholar] [CrossRef]
- Siegmann, E.M.; Bouna-Pyrrou, P.; Lenz, B.; Kornhuber, J. Digit ratio (2D:4D) in relation to substance and computer use: A meta-analysis. J. Neural. Transm. 2019, 126, 623–636. [Google Scholar] [CrossRef]
- Han, C.; Bae, H.; Lee, Y.-S.; Won, S.-D.; Kim, D.J. The ratio of 2nd to 4th digit length in Korean alcohol-dependent patients. Clin. Psychopharmacol. Neurosci. 2016, 14, 148–152. [Google Scholar] [CrossRef][Green Version]
- Canan, F.; Karaca, S.; Düzgün, M.; Erdem, A.M.; Karaçaylı, E.; Topan, N.B.; Lee, S.K.; Zhai, Z.W.; Kuloğlu, M.; Potenza, M.N. The relationship between second-to-fourth digit (2D:4D) ratios and problematic and pathological Internet use among Turkish university students. J. Behav. Addict. 2017, 6, 30–41. [Google Scholar] [CrossRef]
- Canan, F.; Tegin, C.; Gecici, O. The second to fourth digit (2D:4D) ratios, smoking, and problem drinking in a young adult university student sample. Neurol. Psychiatry Brain Res. 2019, 32, 63–67. [Google Scholar] [CrossRef]
- Kim, Y.J.; Roh, D.; Lee, S.K.; Canan, F.; Potenza, M.N. Factors statistically predicting at-risk/problematic internet use in a sample of young adolescent boys and girls in South Korea. Front. Psychiatry 2018, 9, 351. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; Brand, M.; Mies, J.; Lachmann, B.; Sariyska, R.Y.; Montag, C. The 2D:4D marker and different forms of internet use disorder. Front. Psychiatry 2017, 8, 213. [Google Scholar] [CrossRef] [PubMed]
- Lenz, B.; Mühle, C.; Braun, B.; Weinland, C.; Bouna-Pyrrou, P.; Behrens, J.; Kubis, S.; Mikolaiczik, K.; Muschler, M.R.; Saigali, S.; et al. Prenatal and adult androgen activities in alcohol dependence. Acta Psychiatr. Scand. 2017, 136, 96–107. [Google Scholar] [CrossRef]
- Lenz, B.; Thiem, D.; Bouna-Pyrrou, P.; Mühle, C.; Stoessel, C.; Betz, P.; Kornhuber, J. Low digit ratio (2D:4D) in male suicide victims. J. Neural. Transm. 2016, 123, 1499–1503. [Google Scholar] [CrossRef][Green Version]
- Lenz, B.; Kornhuber, J. Cross-national gender variations of digit ratio (2D:4D) correlate with life expectancy, suicide rate, and other causes of death. J. Neural. Transm. 2018, 125, 239–246. [Google Scholar] [CrossRef]
- Siegmann, E.M.; Müller, T.; Dziadeck, I.; Mühle, C.; Lenz, B.; Kornhuber, J. Digit ratio (2D:4D) and transgender identity: New original data and a meta-analysis. Sci. Rep. 2020, 10, 19326. [Google Scholar] [CrossRef]
- Gorka, A.X.; Norman, R.E.; Radtke, S.R.; Carre, J.M.; Hariri, A.R. Anterior cingulate cortex gray matter volume mediates an association between 2D:4D ratio and trait aggression in women but not men. Psychoneuroendocrinology 2015, 56, 148–156. [Google Scholar] [CrossRef]
- Rizwan, S.; Manning, J.T.; Brabin, B.J. Maternal smoking during pregnancy and possible effects of in utero testosterone: Evidence from the 2D:4D finger length ratio. Early Hum. Dev. 2007, 83, 87–90. [Google Scholar] [CrossRef]
- Lilley, T.; Laaksonen, T.; Huitu, O.; Helle, S. Maternal corticosterone but not testosterone level is associated with the ratio of second-to-fourth digit length (2D:4D) in field vole offspring (Microtus agrestis). Physiol. Behav. 2010, 99, 433–437. [Google Scholar] [CrossRef]
- Barrett, E.S.; Parlett, L.E.; Sathyanarayana, S.; Liu, F.; Redmon, J.B.; Wang, C.; Swan, S.H. Prenatal exposure to stressful life events is associated with masculinized anogenital distance (AGD) in female infants. Physiol. Behav. 2013, 114–115, 14–20. [Google Scholar] [CrossRef]
- Barrett, E.S.; Swan, S.H. Stress and androgen activity during fetal development. Endocrinology 2015, 156, 3435–3441. [Google Scholar] [CrossRef] [PubMed]
- Fowler, P.A.; Bhattacharya, S.; Flannigan, S.; Drake, A.J.; O’Shaughnessy, P.J. Maternal cigarette smoking and effects on androgen action in male offspring: Unexpected effects on second-trimester anogenital distance. J. Clin. Endocrinol. Metab. 2011, 96, E1502–E1506. [Google Scholar] [CrossRef] [PubMed]
- García-Villarino, M.; Fernández-Iglesias, R.; Riaño-Galán, I.; Rodríguez-Dehli, C.; Babarro, I.; Fernández-Somoano, A.; Tardón, A. Prenatal exposure to cigarette smoke and anogenital distance at 4 years in the INMA-Asturias cohort. Int. J. Environ. Res. Public Health 2021, 18, 4774. [Google Scholar] [CrossRef] [PubMed]
- Kızılay, D.O.; Aydin, C.; Aygün, A.P.; Tuhan, H.U.; Olukman, O. Prenatal smoke exposure is associated with increased anogenital distance in female infants: A prospective case-control study. J. Pediatr. Endocrinol. Metab. 2021, 34, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Lenz, B.; Eichler, A.; Schwenke, E.; Buchholz, V.N.; Hartwig, C.; Moll, G.H.; Reich, K.; Mühle, C.; Volz, B.; Titzmann, A.; et al. Mindfulness-based stress reduction in pregnancy: An app-based programme to improve the health of mothers and children (MINDFUL/PMI study). Geburtshilfe Frauenheilkd. 2018, 78, 1283–1291. [Google Scholar] [CrossRef]
- Agius, A.; Xuereb, R.B.; Carrick-Sen, D.; Sultana, R.; Rankin, J. The co-existence of depression, anxiety and post-traumatic stress symptoms in the perinatal period: A systematic review. Midwifery 2016, 36, 70–79. [Google Scholar] [CrossRef] [PubMed]
- O’Hara, M.W.; Wisner, K.L. Perinatal mental illness: Definition, description and aetiology. Best Pract. Res. Clin. Obs. Gynaecol. 2014, 28, 3–12. [Google Scholar] [CrossRef]
- Fairbrother, N.; Young, A.H.; Janssen, P.; Antony, M.M.; Tucker, E. Depression and anxiety during the perinatal period. BMC Psychiatry 2015, 15, 206. [Google Scholar] [CrossRef]
- Stone, S.L.; Diop, H.; Declercq, E.; Cabral, H.J.; Fox, M.P.; Wise, L.A. Stressful events during pregnancy and postpartum depressive symptoms. J. Womens Health 2015, 24, 384–393. [Google Scholar] [CrossRef]
- Lilliecreutz, C.; Laren, J.; Sydsjo, G.; Josefsson, A. Effect of maternal stress during pregnancy on the risk for preterm birth. BMC Pregnancy Childbirth 2016, 16, 5. [Google Scholar] [CrossRef] [PubMed]
- Baibazarova, E.; van de Beek, C.; Cohen-Kettenis, P.T.; Buitelaar, J.; Shelton, K.H.; van Goozen, S.H. Influence of prenatal maternal stress, maternal plasma cortisol and cortisol in the amniotic fluid on birth outcomes and child temperament at 3 months. Psychoneuroendocrinology 2013, 38, 907–915. [Google Scholar] [CrossRef] [PubMed]
- Davis, E.P.; Glynn, L.M.; Schetter, C.D.; Hobel, C.; Chicz-Demet, A.; Sandman, C.A. Prenatal exposure to maternal depression and cortisol influences infant temperament. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 737–746. [Google Scholar] [CrossRef]
- Nolvi, S.; Karlsson, L.; Bridgett, D.J.; Korja, R.; Huizink, A.C.; Kataja, E.L.; Karlsson, H. Maternal prenatal stress and infant emotional reactivity six months postpartum. J. Affect Disord. 2016, 199, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Stein, A.; Pearson, R.M.; Goodman, S.H.; Rapa, E.; Rahman, A.; McCallum, M.; Howard, L.M.; Pariante, C.M. Effects of perinatal mental disorders on the fetus and child. Lancet 2014, 384, 1800–1819. [Google Scholar] [CrossRef]
- Talge, N.M.; Neal, C.; Glover, V. Early Stress, Translational Research and Prevention Science Network: Fetal and Neonatal Experience on Child and Adolescent Mental Health. Antenatal maternal stress and long-term effects on child neurodevelopment: How and why? J. Child. Psychol. Psychiatry 2007, 48, 245–261. [Google Scholar] [CrossRef]
- Bright, K.S.; Charrois, E.M.; Mughal, M.K.; Wajid, A.; McNeil, D.; Stuart, S.; Hayden, K.A.; Kingston, D. Interpersonal psychotherapy to reduce psychological distress in perinatal women: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 8421. [Google Scholar] [CrossRef]
- Shen, Q.; Huang, C.R.; Rong, L.; Ju, S.; Redding, S.R.; Ouyang, Y.Q.; Wang, R. Effects of needs-based education for prenatal anxiety in advanced multiparas: A randomized controlled trial. BMC Pregnancy Childbirth 2022, 22, 301. [Google Scholar] [CrossRef]
- Green, S.M.; Donegan, E.; McCabe, R.E.; Streiner, D.L.; Agako, A.; Frey, B.N. Cognitive behavioral therapy for perinatal anxiety: A randomized controlled trial. Aust. N. Z. J. Psychiatry 2020, 54, 423–432. [Google Scholar] [CrossRef]
- Loughnan, S.A.; Sie, A.; Hobbs, M.J.; Joubert, A.E.; Smith, J.; Haskelberg, H.; Mahoney, A.E.J.; Kladnitski, N.; Holt, C.J.; Milgrom, J.; et al. A randomized controlled trial of ‘MUMentum Pregnancy’: Internet-delivered cognitive behavioral therapy program for antenatal anxiety and depression. J. Affect. Disord. 2019, 243, 381–390. [Google Scholar] [CrossRef]
- Vakilian, K.; Zarei, F.; Majidi, A. Effect of Acceptance and Commitment Therapy (ACT) on anxiety and quality of life during pregnancy: A mental health clinical trial study. Iran Red Crescent Med. J. 2019, 21, e89489. [Google Scholar] [CrossRef]
- Waters, C.S.; Annear, B.; Flockhart, G.; Jones, I.; Simmonds, J.R.; Smith, S.; Traylor, C.; Williams, J.F. Acceptance and Commitment Therapy for perinatal mood and anxiety disorders: A feasibility and proof of concept study. Br. J. Clin. Psychol. 2020, 59, 461–479. [Google Scholar] [CrossRef] [PubMed]
- Mao, F.; Sun, Y.; Li, Y.; Cui, N.; Cao, F. Internet-delivered mindfulness-based interventions for mental health outcomes among perinatal women: A systematic review. Asian J. Psychiatr. 2023, 80, 103321. [Google Scholar] [CrossRef]
- Neo, H.S.; Tan, J.H.; Ang, W.H.D.; Lau, Y. Internet-delivered psychological interventions for reducing depressive, anxiety symptoms and fear of childbirth in pregnant women: A meta-analysis and meta-regression. J. Psychosom Res. 2022, 157, 110790. [Google Scholar] [CrossRef]
- Silang, K.A.; Sohal, P.R.; Bright, K.S.; Leason, J.; Roos, L.; Lebel, C.; Giesbrecht, G.F.; Tomfohr-Madsen, L.M. eHealth interventions for treatment and prevention of depression, anxiety, and insomnia during pregnancy: Systematic review and meta-analysis. JMIR Ment. Health 2022, 9, e31116. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, A.; Sparkes, E.; Duarte, R.V. Mindfulness-based interventions during pegnancy: A systematic review and meta-analysis. Mindfulness 2017, 8, 1421–1437. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Leng, L.L.; Yin, X.C.; Chan, C.L.W.; Ng, S.M. Antenatal mobile-delivered mindfulness-based intervention to reduce perinatal depression risk and improve obstetric and neonatal outcomes: A randomized controlled trial. J. Affect. Disord. 2023, 335, 216–227. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Wang, J.; Mao, F.; Wu, L.; Huang, Y.; Sun, J.; Cao, F. Effectiveness of digital guided self-help mindfulness training during pregnancy on maternal psychological distress and infant neuropsychological development: Randomized controlled trial. J. Med. Internet Res. 2023, 25, e41298. [Google Scholar] [CrossRef]
- Zhang, X.; Mao, F.; Li, Y.; Wang, J.; Wu, L.; Sun, J.; Cao, F. Effects of a maternal mindfulness intervention targeting prenatal psychological distress on infants’ meconium microbiota: A randomized controlled trial. Psychoneuroendocrinology 2022, 145, 105913. [Google Scholar] [CrossRef]
- Klein, E.M.; Brähler, E.; Dreier, M.; Reinecke, L.; Müller, K.W.; Schmutzer, G.; Wölfling, K.; Beutel, M.E. The German version of the Perceived Stress Scale-psychometric characteristics in a representative German community sample. BMC Psychiatry 2016, 16, 159. [Google Scholar] [CrossRef]
- Michalak, J.; Heidenreich, T.; Ströhle, G.; Nachtigall, C. Die deutsche Version der Mindful Attention and Awareness Scale (MAAS) Psychometrische Befunde zu einem Achtsamkeitsfragebogen. Z. Für Klin. Psychol. Und Psychother. 2008, 37, 200–208. [Google Scholar] [CrossRef]
- Huizink, A.C.; Delforterie, M.J.; Scheinin, N.M.; Tolvanen, M.; Karlsson, L.; Karlsson, H. Adaption of pregnancy anxiety questionnaire-revised for all pregnant women regardless of parity: PRAQ-R2. Arch. Womens Ment. Health 2016, 19, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Bergant, A.M.; Nguyen, T.; Heim, K.; Ulmer, H.; Dapunt, O. German language version and validation of the Edinburgh postnatal depression scale. Dtsch. Med. Wochenschr. 1998, 123, 35–40. [Google Scholar] [CrossRef]
- Cox, J.L.; Chapman, G.; Murray, D.; Jones, P. Validation of the Edinburgh Postnatal Depression Scale (EPDS) in non-postnatal women. J. Affect. Disord. 1996, 39, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Michalak, J.; Zarbock, G.; Drews, M.; Otto, D.; Mertens, D.; Ströhle, G.; Schwinger, M.; Dahme, B.; Heidenreich, T. Erfassung von Achtsamkeit mit der deutschen Version des Five Facet Mindfulness Questionnaires (FFMQ-D). Z. Für Gesundheitspsychologie 2016, 24, 1–12. [Google Scholar] [CrossRef]
- R Core Team. A Language and Environment for Statistical Computing: R Foundation for Statistical Computing. 2022. Available online: https://www.R-project.org/ (accessed on 3 October 2022).
- Hulsbosch, L.P.; Potharst, E.S.; Schwabe, I.; Boekhorst, M.; Pop, V.J.M.; Nyklicek, I. Online mindfulness-based intervention for women with pregnancy distress: A randomized controlled trial. J. Affect. Disord. 2023, 332, 262–272. [Google Scholar] [CrossRef]
- Cuijpers, P.; Noma, H.; Karyotaki, E.; Cipriani, A.; Furukawa, T.A. Effectiveness and acceptability of cognitive behavior therapy delivery formats in adults with depression: A network meta-analysis. JAMA Psychiatry 2019, 76, 700–707. [Google Scholar] [CrossRef]
- Moshe, I.; Terhorst, Y.; Philippi, P.; Domhardt, M.; Cuijpers, P.; Cristea, I.; Pulkki-Råback, L.; Baumeister, H.; Sander, L.B. Digital interventions for the treatment of depression: A meta-analytic review. Psychol. Bull. 2021, 147, 749–786. [Google Scholar] [CrossRef]
- Van Dam, N.T.; van Vugt, M.K.; Vago, D.R.; Schmalzl, L.; Saron, C.D.; Olendzki, A.; Meissner, T.; Lazar, S.W.; Kerr, C.E.; Gorchov, J.; et al. Mind the hype: A critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspect. Psychol. Sci. 2018, 13, 36–61. [Google Scholar] [CrossRef]
- Heinz, A.; Kiefer, F.; Smolka, M.N.; Endrass, T.; Beste, C.; Beck, A.; Liu, S.; Genauck, A.; Romund, L.; Banaschewski, T.; et al. Addiction Research Consortium: Losing and regaining control over drug intake (ReCoDe)—From trajectories to mechanisms and interventions. Addict. Biol. 2020, 25, e12866. [Google Scholar] [CrossRef] [PubMed]

| Mindfulness Group (n = 72) | Pregnancy Education Group (n = 74) | |||||
|---|---|---|---|---|---|---|
| N | M ± SD (%) | N | M ± SD (%) | t, χ2 | p | |
| Maternal age (years) | 71 | 32.77 ± 4.39 | 74 | 32.73 ± 4.88 | 0.1 | 0.954 |
| Marital status | 5.6 | 0.127 | ||||
| Single | 19 | 27.9% | 20 | 30.3% | ||
| Married | 47 | 69.1% | 38 | 57.6% | ||
| Other | 2 | 2.9% | 8 | 12.1% | ||
| Maternal education | 0.0 | 1.0 | ||||
| >12 years | 30 | 44.1% | 29 | 43.9% | ||
| ≤12 years | 38 | 55.9% | 37 | 56.1% | ||
| Employment status at baseline | 5.4 | 0.124 | ||||
| Working (full/part-time) | 58 | 85.3% | 54 | 83.1% | ||
| Not working | 10 | 14.7% | 11 | 16.9% | ||
| Health insurance | 0.0 | 1.0 | ||||
| Public | 60 | 88.2% | 58 | 89.2% | ||
| Private/other | 8 | 11.8% | 7 | 10.8% | ||
| BMI (kg/m2) | 72 | 23.93 ± 4.32 | 74 | 24.38 ± 3.91 | 0.9 | 0.342 |
| Has previously practiced meditation | 2.4 | 0.123 | ||||
| Yes | 30 | 44.1% | 40 | 58.8% | ||
| No | 38 | 55.9% | 28 | 41.2% | ||
| Previous births | 1.7 | 0.189 | ||||
| 0 | 36 | 50.0% | 46 | 62.2% | ||
| 1 | 36 | 50.0% | 28 | 37.8% | ||
| Gestational age at enrollment (weeks) | 66 | 12.65 ± 1.48 | 61 | 12.56 ± 1.91 | 0.3 | 0.763 |
| Gestational age at birth (weeks) | 42 | 39.19 ± 1.57 | 50 | 38.82 ± 2.05 | 1.0 | 0.340 |
| Delivery mode | 0.8 | 0.364 | ||||
| Vaginal | 27 | 61.4% | 41 | 71.9% | ||
| Caesarian | 17 | 38.6% | 16 | 28.1% | ||
| PSS-10 score a | 72 | 15.97 ± 5.77 | 74 | 15.70 ± 5.43 | 0.3 | 0.772 |
| PRAQ-R2 score a | 66 | 23.77 ± 6.81 | 66 | 21.94 ± 5.48 | 2.0 | 0.160 |
| EPDS score a | 65 | 7.88 ± 5.12 | 65 | 6.71 ± 5.09 | 2.2 | 0.140 |
| FFMQ-D score a | 65 | 133.05 ± 17.27 | 58 | 135.41 ± 16.01 | −0.8 | 0.434 |
| MAAS score a | 72 | 4.17 ± 0.80 | 74 | 4.24 ± 0.68 | −0.6 | 0.539 |
| Infant’s sex | 0.0 | 0.951 | ||||
| Male | 23 | 50.0% | 28 | 47.5% | ||
| Female | 23 | 50.0% | 31 | 52.5% | ||
| Infant’s anogenital distance (cm) | 33 | 2.28 ± 0.83 | 40 | 2.13 ± 0.91 | 0.7 | 0.460 |
| Mothers’ A2D:4D | 32 | 0.97 ± 0.03 | 43 | 0.97 ± 0.03 | 0.3 | 0.742 |
| Mothers’ R2D:4D | 32 | 0.97 ± 0.03 | 44 | 0.97 ± 0.03 | 0.0 | 0.995 |
| Mothers’ L2D:4D | 32 | 0.97 ± 0.03 | 43 | 0.97 ± 0.03 | 0.4 | 0.681 |
| Infants’ A2D:4D | 22 | 0.92 ± 0.04 | 30 | 0.93 ± 0.03 | −0.4 | 0.689 |
| Infants’ R2D:4D | 26 | 0.92 ± 0.04 | 39 | 0.93 ± 0.04 | −0.9 | 0.373 |
| Infants’ L2D:4D | 29 | 0.92 ± 0.04 | 33 | 0.92 ± 0.05 | 0.1 | 0.888 |
| Group (Mindfulness versus Pregnancy Education) | Infant’s Sex | Age at Follow-Up | Mother’s 2D:4D | |
|---|---|---|---|---|
| A2D:4D | 0.003 | 0.001 | 0.005 | 0.141 |
| R2D:4D | 0.009 | 0.013 | 0.068 | 0.128 |
| L2D:4D | 0.00004 | 0.003 | 0.006 | 0.105 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siegmann, E.-M.; Eichler, A.; Buchholz, V.N.; Gerlach, J.; Pontones, C.A.; Titzmann, A.; Arnaud, N.; Consortium, I.-M.; Mühle, C.; Beckmann, M.W.; et al. Effects of an App-Based Mindfulness Intervention during Pregnancy on the Infant’s Prenatal Androgen Exposure: A Randomized Controlled Pilot Trial. J. Clin. Med. 2023, 12, 6142. https://doi.org/10.3390/jcm12196142
Siegmann E-M, Eichler A, Buchholz VN, Gerlach J, Pontones CA, Titzmann A, Arnaud N, Consortium I-M, Mühle C, Beckmann MW, et al. Effects of an App-Based Mindfulness Intervention during Pregnancy on the Infant’s Prenatal Androgen Exposure: A Randomized Controlled Pilot Trial. Journal of Clinical Medicine. 2023; 12(19):6142. https://doi.org/10.3390/jcm12196142
Chicago/Turabian StyleSiegmann, Eva-Maria, Anna Eichler, Verena Nadine Buchholz, Jennifer Gerlach, Constanza A. Pontones, Adriana Titzmann, Nicolas Arnaud, IMAC-Mind Consortium, Christiane Mühle, Matthias W. Beckmann, and et al. 2023. "Effects of an App-Based Mindfulness Intervention during Pregnancy on the Infant’s Prenatal Androgen Exposure: A Randomized Controlled Pilot Trial" Journal of Clinical Medicine 12, no. 19: 6142. https://doi.org/10.3390/jcm12196142
APA StyleSiegmann, E.-M., Eichler, A., Buchholz, V. N., Gerlach, J., Pontones, C. A., Titzmann, A., Arnaud, N., Consortium, I.-M., Mühle, C., Beckmann, M. W., Fasching, P. A., Kratz, O., Moll, G. H., Kornhuber, J., & Lenz, B. (2023). Effects of an App-Based Mindfulness Intervention during Pregnancy on the Infant’s Prenatal Androgen Exposure: A Randomized Controlled Pilot Trial. Journal of Clinical Medicine, 12(19), 6142. https://doi.org/10.3390/jcm12196142