
Bariatric Surgery Outcomes in Patients with Chronic Kidney Disease
 , , , , , , ,
, , , , , , ,  , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Clinical and Laboratory Measures
2.2. Metabolic and Kidney-Related Outcomes following BS
2.3. Hospitalization, Surgical Complications and Mortality
2.4. Statistical Analyses
3. Results
3.1. Subjects’ Characteristics
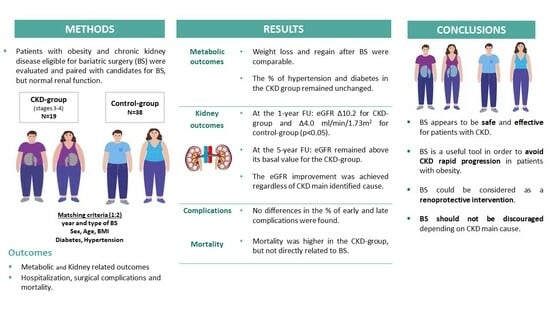
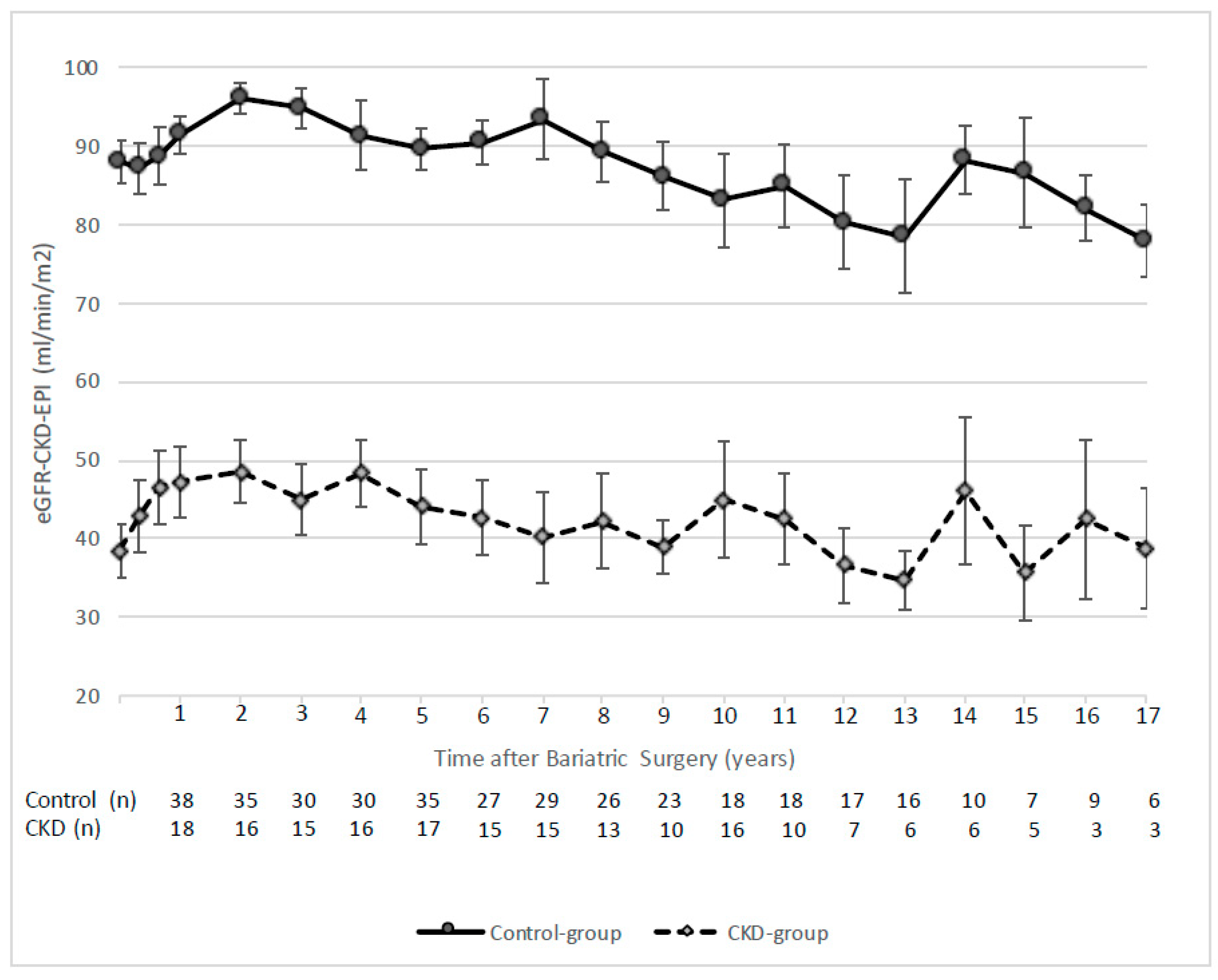
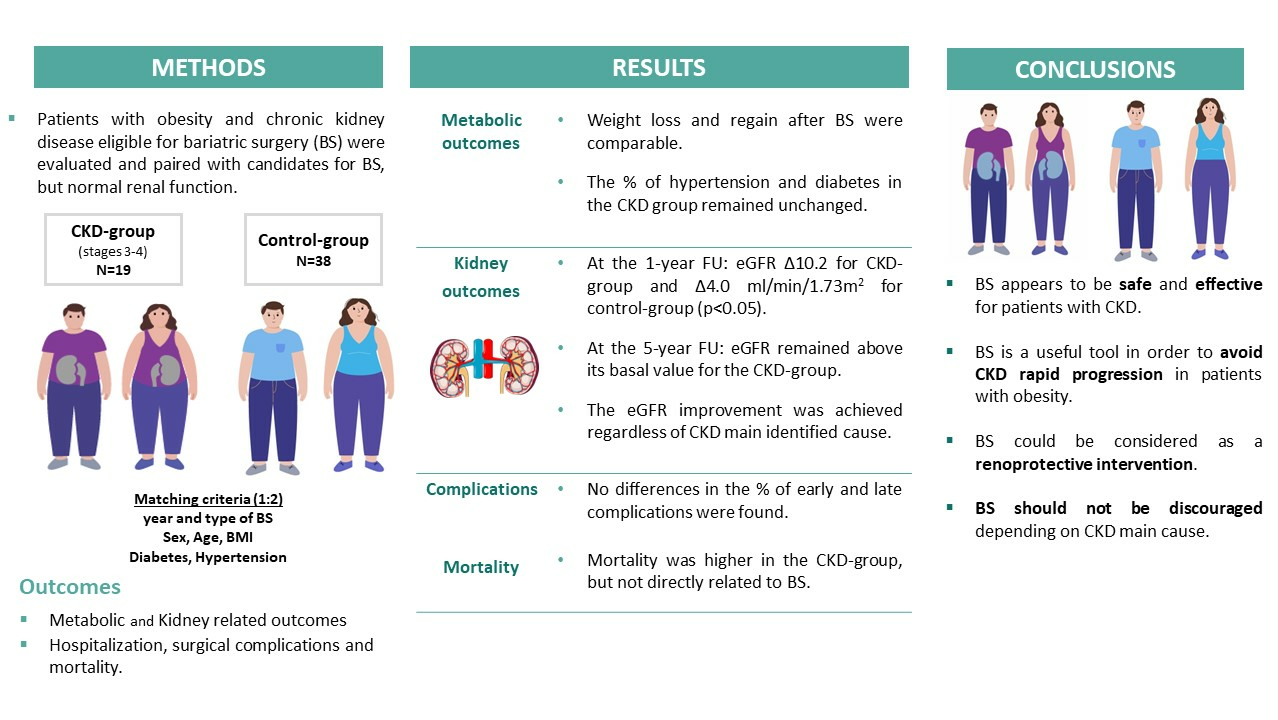
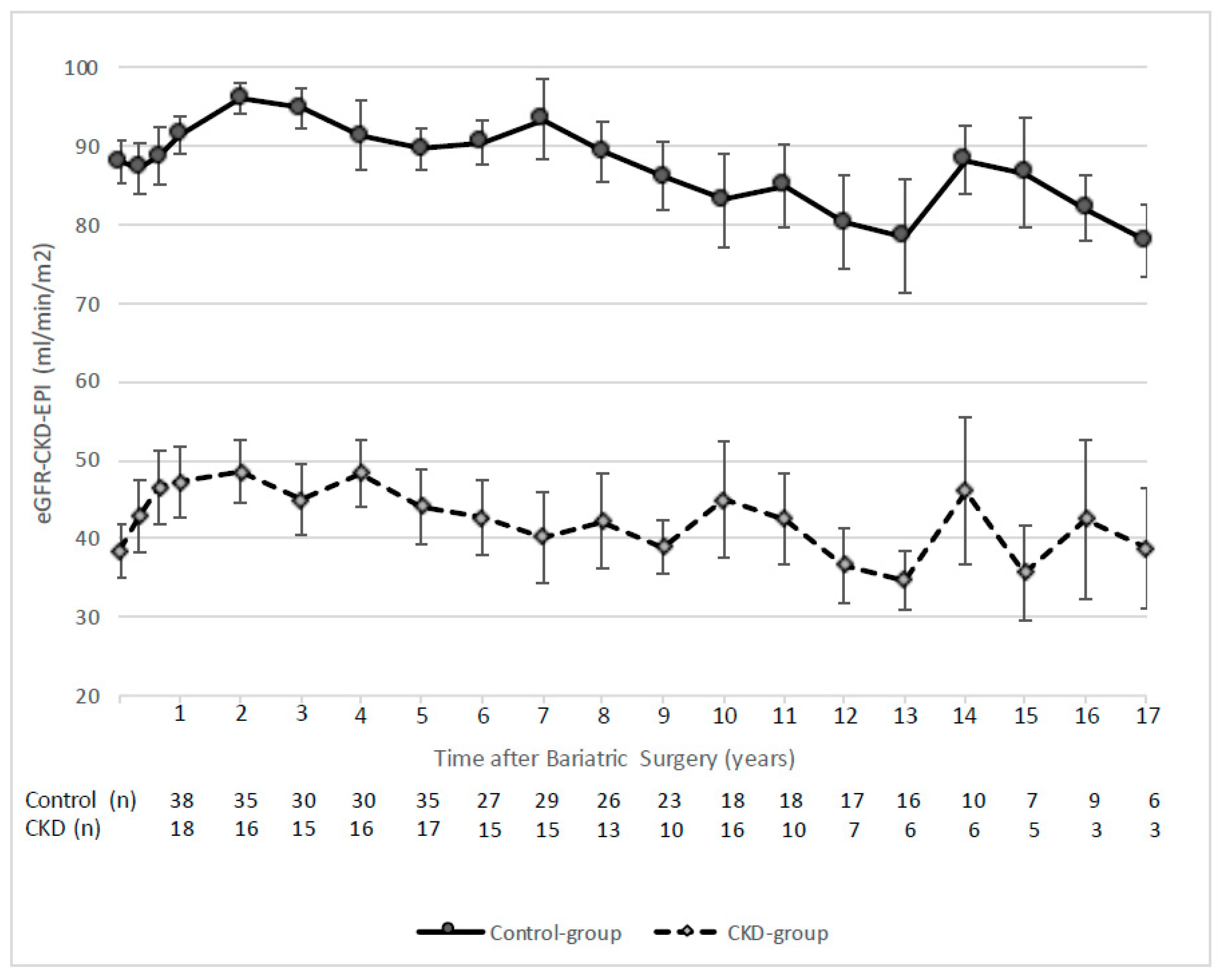
3.2. Metabolic and Kidney Related Outcomes
3.3. Post-Operative Complications and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Y.; Chen, X.; Song, Y.; Caballero, B.; Cheskin, L.J. Association between obesity and kidney disease: A systematic review and meta-analysis. Kidney Int. 2008, 73, 19–33. [Google Scholar] [CrossRef] [PubMed]
- Praga, M.; Morales, E. The Fatty Kidney: Obesity and Renal Disease. Nephron 2017, 136, 273–276. [Google Scholar] [CrossRef] [PubMed]
- Navarro Díaz, M. Consequences of morbid obesity on the kidney. Where are we going? Clin. Kidney J. 2016, 9, 782. [Google Scholar] [CrossRef]
- Nelson, R.G.; Grams, M.E.; Ballew, S.H.; Sang, Y.; Azizi, F.; Chadban, S.J.; Chaker, L.; Dunning, S.C.; Fox, C.; Hirakawa, Y.; et al. Development of Risk Prediction Equations for Incident Chronic Kidney Disease. JAMA-J. Am. Med. Assoc. 2019, 322, 2104–2114. [Google Scholar] [CrossRef]
- Turgeon, N.A.; Perez, S.; Mondestin, M.; Scott Davis, S.; Lin, E.; Tata, S.; Kirk, A.D.; Larsen, C.P.; Pearson, T.C.; Sweeney, J.F. The Impact of Renal Function on Outcomes of Bariatric Surgery. J. Am. Soc. Nephrol. 2012, 23, 885–894. [Google Scholar] [CrossRef]
- GBD Chronic Kidney Disease Collaboration. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [PubMed]
- Sjöström, L.; Lindroos, A.-K.; Peltonen, M.; Torgerson, J.; Bouchard, C.; Carlsson, B.; Dahlgren, S.; Larsson, B.; Narbro, K.; Sjöström, C.D.; et al. Lifestyle, Diabetes, and Cardiovascular Risk Factors 10 Years after Bariatric Surgery. N. Engl. J. Med. 2004, 351, 2683–2693. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, C.N.; Goss, L.E.; Almehmi, A.; Grams, J.M.; Corey, B.L. Bariatric surgery is associated with renal function improvement. Surg. Endosc. 2017, 32, 276–281. [Google Scholar] [CrossRef]
- Friedman, A.N.; Cohen, R.V. Bariatric surgery as a renoprotective intervention. Curr. Opin. Nephrol. Hypertens. 2019, 28, 537–544. [Google Scholar] [CrossRef]
- Afshinnia, F.; Wilt, T.J.; Duval, S.; Esmaeili, A.; Ibrahim, H.N. Weight loss and proteinuria: Systematic review of clinical trials and comparative cohorts. Nephrol. Dial. Transplant. 2010, 25, 1173–1183. [Google Scholar] [CrossRef]
- Li, K.; Zou, J.; Ye, Z.; Di, J.; Han, X.; Zhang, H.; Liu, W.; Ren, Q.; Zhang, P. Effects of bariatric surgery on renal function in obese patients: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0163907. [Google Scholar] [CrossRef] [PubMed]
- Shulman, A.; Andersson-Assarsson, J.C.; Sjöström, C.D.; Jacobson, P.; Taube, M.; Sjöholm, K.; le Roux, C.W.; Peltonen, M.; Carlsson, L.M.S.; Svensson, P.A. Remission and progression of pre-existing micro- and macroalbuminuria over 15 years after bariatric surgery in Swedish Obese Subjects study. Int. J. Obes. 2020, 45, 535–546. [Google Scholar] [CrossRef]
- Amor, A.; Jiménez, A.; Moizé, V.; Ibarzabal, A.; Flores, L.; Lacy, A.M.; Vidal, J. Weight loss independently predicts urinary albumin excretion normalization in morbidly obese type 2 diabetic patients undergoing bariatric surgery. Surg. Endosc. 2013, 27, 2046–2051. [Google Scholar] [CrossRef]
- Kassam, A.F.; Mirza, A.; Kim, Y.; Hanseman, D.; Woodle, E.S.; Quillin, R.C.; Johnson, B.L.; Govil, A.; Cardi, M.; Schauer, D.P.; et al. Long-term outcomes in patients with obesity and renal disease after sleeve gastrectomy. Am. J. Transplant. 2020, 20, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Imam, T.H.; Fischer, H.; Jing, B.; Burchette, R.; Henry, S.; DeRose, S.F.; Coleman, K.J. Estimated GFR Before and After Bariatric Surgery in CKD. Am. J. Kidney Dis. 2017, 69, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.W.; Goodman, H.R.; Gersin, K.; Cardi, M.; Austin, J.; Goel, S.; Safdar, S.; Huang, S.; Woodle, E.S. Gastric bypass in morbidly obese patients with chronic renal failure and kidney transplant. Transplantation 2004, 78, 469–474. [Google Scholar] [CrossRef]
- Al-Bahri, S.; Fakhry, T.K.; Gonzalvo, J.P.; Murr, M.M. Bariatric Surgery as a Bridge to Renal Transplantation in Patients with End-Stage Renal Disease. Obes. Surg. 2017, 13, 336–2955. [Google Scholar] [CrossRef]
- Lin, M.Y.C.; Tavakol, M.M.; Sarin, A.; Amirkiai, S.M.; Rogers, S.J.; Carter, J.T.; Posselt, A.M. Laparoscopic sleeve gastrectomy is safe and efficacious for pretransplant candidates. Surg. Obes. Relat. Dis. 2013, 9, 653–658. [Google Scholar] [CrossRef]
- Montgomery, J.R.; Waits, S.A.; Dimick, J.B.; Telem, D.A. Risks of Bariatric Surgery among Patients with End-stage Renal Disease. JAMA Surg. 2019, 154, 1160–1162. [Google Scholar] [CrossRef]
- Gheith, O.; Al-Otaibi, T.; Halim, M.A.; Mahmoud, T.; Mosaad, A.; Yagan, J.; Zakaria, Z.; Rida, S.; Nair, P.; Hassan, R. Bariatric Surgery in Renal Transplant Patients. Exp. Clin. Transplant. 2017, 15, 164–169. [Google Scholar] [CrossRef]
- MacLaughlin, H.L.; Hall, W.L.; Patel, A.G.; MacDougall, I.C. Laparoscopic sleeve gastrectomy is a novel and effective treatment for obesity in patients with chronic kidney disease. Obes. Surg. 2012, 22, 119–123. [Google Scholar] [CrossRef]
- Cohen, R.V.; Pereira, T.V.; Aboud, C.M.; Petry, T.B.Z.; Lopes Correa, J.L.; Schiavon, C.A.; Pompílio, C.E.; Pechy, F.N.Q.; Da Costa Silva, A.C.C.; De Melo, F.L.G.; et al. Effect of Gastric Bypass vs. Best Medical Treatment on Early-Stage Chronic Kidney Disease in Patients with Type 2 Diabetes and Obesity: A Randomized Clinical Trial. JAMA Surg. 2020, 155, e200420. [Google Scholar] [CrossRef] [PubMed]
- Khajeh, E.; Aminizadeh, E.; Dooghaie Moghadam, A.; Sabetkish, N.; Abbasi Dezfouli, S.; Morath, C.; Zeier, M.; Nickel, F.; Billeter, A.T.; Müller-Stich, B.P.; et al. Bariatric surgery in patients with obesity and end-stage renal disease. Surg. Obes. Relat. Dis. 2023, 19, 858–871. [Google Scholar] [CrossRef] [PubMed]
- Thakar, C.V.; Kharat, V.; Blanck, S.; Leonard, A.C. Acute kidney injury after gastric bypass surgery. Clin. J. Am. Soc. Nephrol. 2007, 2, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Weingarten, T.N.; Gurrieri, C.; McCaffrey, J.M.; Ricter, S.J.; Hilgeman, M.L.; Schroeder, D.R.; Kendrick, M.L.; Greene, E.L.; Sprung, J. Acute kidney injury following bariatric surgery. Obes. Surg. 2013, 23, 64–70. [Google Scholar] [CrossRef]
- Abdullah, H.R.; Tan, T.P.; Vaez, M.; Deb, C.; Farag, N.; Jackson, T.D.; Wong, D.T. Predictors of Perioperative Acute Kidney Injury in Obese Patients Undergoing Laparoscopic Bariatric Surgery: A Single-Centre Retrospective Cohort Study. Obes. Surg. 2016, 26, 1493–1499. [Google Scholar] [CrossRef]
- Fried, M.; Yumuk, V.; Oppert, J.M.; Scopinaro, N.; Torres, A.; Weiner, R.; Yashkov, Y.; Frühbeck, G. Interdisciplinary European guidelines on metabolic and bariatric surgery. Obes. Surg. 2014, 24, 42–55. [Google Scholar] [CrossRef]
- Jiménez, A.; Ibarzabal, A.; Moizé, V.; Pané, A.; Andreu, A.; Molero, J.; de Hollanda, A.; Flores, L.; Ortega, E.; Lacy, A.; et al. Ten-year outcomes after Roux-en-Y gastric bypass and sleeve gastrectomy: An observational nonrandomized cohort study. Surg. Obes. Relat. Dis. 2019, 15, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46, S19–S40. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Brethauer, S.A.; Kim, J.; El Chaar, M.; Papasavas, P.; Eisenberg, D.; Rogers, A.; Ballem, N.; Kligman, M.; Kothari, S. Standardized outcomes reporting in metabolic and bariatric surgery. Surg. Obes. Relat. Dis. 2015, 11, 489–506. [Google Scholar] [CrossRef] [PubMed]
- King, W.C.; Hinerman, A.S.; Belle, S.H.; Wahed, A.S.; Courcoulas, A.P. Comparison of the Performance of Common Measures of Weight Regain after Bariatric Surgery for Association with Clinical Outcomes. JAMA-J. Am. Med. Assoc. 2018, 320, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- Riddle, M.C.; Cefalu, W.T.; Evans, P.H.; Gerstein, H.C.; Nauck, M.A.; Oh, W.K.; Rothberg, A.E.; le Roux, C.W.; Rubino, F.; Schauer, P.; et al. Consensus Report: Definition and Interpretation of Remission in Type 2 Diabetes. Diabetes Care 2021, 44, 2438–2444. [Google Scholar] [CrossRef]
- Docherty, N.G.; le Roux, C.W. Bariatric surgery for the treatment of chronic kidney disease in obesity and type 2 diabetes mellitus. Nat. Rev. Nephrol. 2020, 16, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Raveendran, L.; Lovrics, O.; Tian, C.; Khondker, A.; Koyle, M.A.; Farcas, M.; Doumouras, A.G.; Hong, D. The role of bariatric surgery on kidney transplantation: A systematic review and meta-analysis. Can. Urol. Assoc. J. 2021, 15, E553–E562. [Google Scholar] [CrossRef] [PubMed]
- Morales, E.; Porrini, E.; Martin-Taboada, M.; Luis-Lima, S.; Vila-Bedmar, R.; de Pablos, I.G.; Gómez, P.; Rodríguez, E.; Torres, L.; Lanzón, B.; et al. Renoprotective role of bariatric surgery in patients with established chronic kidney disease. Clin. Kidney J. 2021, 14, 2037–2046. [Google Scholar] [CrossRef]
- Friedman, A.N.; Moe, S.; Fadel, W.F.; Inman, M.; Mattar, S.G.; Shihabi, Z.; Quinney, S.K.; Cheng, Y.L.; Elli, E.F.; de Hollanda, A.; et al. Outcomes of Bariatric Surgery after Solid Organ Transplantation. Obes. Surg. 2017, 27, 4899–4904. [Google Scholar] [CrossRef]
- Huang, H.; Lu, J.; Dai, X.; Li, Z.; Zhu, L.; Zhu, S.; Wu, L. Improvement of Renal Function After Bariatric Surgery: A Systematic Review and Meta-analysis. Obes. Surg. 2021, 31, 4470–4484. [Google Scholar] [CrossRef]
- Sandino, J.; Martín-Taboada, M.; Medina-Gómez, G.; Vila-Bedmar, R.; Morales, E. Novel Insights in the Physiopathology and Management of Obesity-Related Kidney Disease. Nutrients 2022, 14, 3937. [Google Scholar] [CrossRef]
- Official Journal of the International Society of Nephrology KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Available online: www.publicationethics.org (accessed on 1 December 2020).
- Syn, N.L.; Cummings, D.E.; Wang, L.Z.; Lin, D.J.; Zhao, J.J.; Loh, M.; Koh, Z.J.; Chew, C.A.; Loo, Y.E.; Tai, B.C.; et al. Association of metabolic-bariatric surgery with long-term survival in adults with and without diabetes: A one-stage meta-analysis of matched cohort and prospective controlled studies with 174,772 participants. Lancet 2021, 397, 1830–1841. [Google Scholar] [CrossRef]
- Aminian, A.; Zajichek, A.; Arterburn, D.E.; Wolski, K.E.; Brethauer, S.A.; Schauer, P.R.; Kattan, M.W.; Nissen, S.E. Association of Metabolic Surgery with Major Adverse Cardiovascular Outcomes in Patients with Type 2 Diabetes and Obesity. JAMA-J. Am. Med. Assoc. 2019, 322, 1271–1282. [Google Scholar] [CrossRef] [PubMed]
- Sjöström, L.; Narbro, K.; Sjöström, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of Bariatric Surgery on Mortality in Swedish Obese Subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Bolignano, D.; Zoccali, C. Effects of weight loss on renal function in obese CKD patients: A systematic review. Nephrol. Dial. Transplant. 2013, 28 (Suppl. S4), iv82–iv98. [Google Scholar] [CrossRef] [PubMed]
- Abou-Mrad, R.M.; Abu-Alfa, A.K.; Ziyadeh, F.N. Effects of weight reduction regimens and bariatric surgery on chronic kidney disease in obese patients. Am. J. Physiol. Renal Physiol. 2013, 305, F613–F617. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, J.R.; Cohen, J.A.; Brown, C.S.; Sheetz, K.H.; Chao, G.F.; Waits, S.A.; Telem, D.A. Perioperative risks of bariatric surgery among patients with and without history of solid organ transplant. Am. J. Transplant. 2020, 20, 2530–2539. [Google Scholar] [CrossRef]
- Cohen, J.B.; Tewksbury, C.M.; Torres Landa, S.; Williams, N.N.; Dumon, K.R. National Postoperative Bariatric Surgery Outcomes in Patients with Chronic Kidney Disease and End-Stage Kidney Disease. Obes. Surg. 2019, 29, 975–982. [Google Scholar] [CrossRef]
- Ortiz, A.; Roger, M.; Jiménez, V.M.; Perez, J.C.R.; Furlano, M.; Atxer, L.S.; Zurro, D.G.; Casabona, C.M.R.; Gómez, C.G.; Bermúdez, P.P.; et al. RICORS2040: The need for collaborative research in chronic kidney disease. Clin. Kidney J. 2021, 15, 372–387. [Google Scholar] [CrossRef] [PubMed]
- Turin, T.C.; Tonelli, M.; Manns, B.J.; Ravani, P.; Ahmed, S.B.; Hemmelgarn, B.R. Chronic kidney disease and life expectancy. Nephrol. Dial. Transplant. 2012, 27, 3182–3186. [Google Scholar] [CrossRef]
- Gorostidi, M.; Sánchez-Martínez, M.; Ruilope, L.M.; Graciani, A.; de la Cruz, J.J.; Santamaría, R.; del Pino, M.D.; Guallar-Castillón, P.; de Álvaro, F.; Rodríguez-Artalejo, F.; et al. Chronic kidney disease in Spain: Prevalence and impact of accumulation of cardiovascular risk factors. Nefrologia 2018, 38, 606–615. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| CKD-Group (n = 19) | Control-Group (n = 38) | p-Value | |
|---|---|---|---|
| General clinical characteristics | |||
| Sex (female), n (%) | 12 (63.2) | 828 (73.7) | 0.413 |
| Age (years) | 54.9 (53.1–59.9) | 56.1 (53.9–58.8) | 0.509 |
| Weight (Kg) | 118.2 ± 18.4 | 122.8 ±18.9 | 0.381 |
| BMI (Kg/m2) | 46.2 ± 8.2 | 47.8 ± 6.1 | 0.398 |
| Renal function | |||
| Serum creatinine (mg/dL) | 1.50 (1.4–2.5) | 0.77 (0.7–0.9) | <0.001 |
| eGFR-CKD-EPI (mL/min/1.73 m2) | 38.4 ± 15.0 | 88.0 ± 16.3 | <0.001 |
| Comorbidities | |||
Hypertension, n (%)
| 17 (89.5) 10 (7–14) 2 (2–3) | 32 (84.2) 10 (6–15) 2 (1–2) | 0.590 0.768 0.003 |
Diabetes, n (%)
| 7 (36.8) 6 (4–16) 1 (0–1) | 12 (31.6) 8 (4–12) 1 (1–1.5) | 0.691 0.865 0.448 |
Dyslipemia, n (%)
| 16 (84.2) 11 (68.7) | 18 (47.4) 11 (61.1) | 0.008 0.642 |
| OSAHS, n (%) | 4 (21.1) | 16 (43.2) | 0.101 |
Heart disease, n (%)
| 3 (15.8) 2 (66.7) 1 (33.3) 0 (0) | 5 (13.2) 2 (40.0) 2 (40.0) 1 (20.0) | 0.787 0.465 0.850 0.408 |
| Laboratory results | |||
| Glucose (mg/dL), | 114 (92–124) | 101 (115–140) | 0.397 |
| Hemoglobin A1c (%) | 6.4 (5.5–6.8) | 5.9 (5.5–6.5) | 0.477 |
| Total cholesterol (mg/dL) | 204.5 ± 41.5 | 204.4 ± 34.7 | 0.988 |
| HDL-cholesterol (mg/dL) | 44 (39–54) | 47 (36–53) | 0.813 |
| LDL-cholesterol (mg/dL) | 122.3 ± 35.0 | 130.7 ± 29.7 | 0.358 |
| Triglycerides (mg/dL) | 168 (115–217) | 118 (90–171) | 0.077 |
| Type of bariatric surgery | |||
SG
| 13 (68.4) 90 (60–110) 6 (31.6) 102.5 (100–115) | 25 (65.7) 75 (60–85) 13 (34.2) 120 (87–130) | 0.843 0.413 0.843 0.597 |
| CKD-Group (n = 19) | p-Value † | Control-Group (n = 38) | p-Value † | p-Value †† | |||
|---|---|---|---|---|---|---|---|
| Baseline | 1 Year after Surgery ¶ | Baseline | 1 Year after Surgery | ||||
| General clinical characteristics | |||||||
| BMI (Kg/m2) | 46.0 ± 8.4 | 30.5 ± 4.6 | <0.001 | 47.8 ± 6.1 | 32.1 ± 4.6 | <0.001 | 0.810 |
| EWL (%) | --- | 76.6 ± 16.1 | --- | --- | 70.6 ± 15.8 | --- | 0.206 |
| TWL (%) | --- | 32.9 ± 6.2 | --- | --- | 32.8 ± 7.1 | --- | 0.970 |
| Renal function | |||||||
| Serum creatinine (mg/dL) | 1.5 (1.4–2.2) | 1.3 (1.1–1.9) | 0.001 | 0.8 (0.7–0.9) | 0.7 (0.7–0.8) | 0.037 | <0.001 |
| eGFR [CKD-EPI] (mL/min/1.73 m2) | 39.8 ± 14.1 | 49.8 ± 16.6 | <0.001 | 86.9 ± 16.3 | 91.4 ± 14.6 | 0.092 | 0.003 |
| Comorbidities | |||||||
Hypertension, n (%)
| 16 (88.9) 2 (2–3) | 14 (77.8) 2 (1–2) | 0.500 0.018 | 32 (84.2) 2 (1–2) | 17 (44.7) 1 (1–2) | <0.001 0.008 | 0.014 --- |
Diabetes, n (%)
| 7 (38.9) 2 (11.1) 1 (0–1) | 4 (22.2) 1 (5.5) 0 (0–0.5) | 0.250 1 0.157 | 12 (31.6) 6 (15.8) 1 (1.0–1.5) | 6 (15.8) 2 (5.3) 1 (1.0–1.0) | 0.031 0.125 0.157 | 0.764 0.363 --- |
| Dyslipemia, n (%) Statins use, n (%) | 16 (84.2) 11 (57.9) | 11 (57.9) 8 (42.1) | 0.125 0.453 | 18 (47.4) 11 (28.9) | 10 (26.3) 5 (13.2) | 0.008 0.031 | 0.681 0.670 |
| OSAHS, n (%) | 4 (22.2) | 1 (5.6) | 0.250 | 16 (43.2) | 6 (16.2) | 0.002 | 0.639 |
| Laboratory characteristics | |||||||
| Glucose (mg/dL) | 114 (94–124) | 91 (80–99) | 0.007 | 115 (101–140) | 88 (81–94) | <0.001 | 0.618 |
| Hemoglobin A1c (%) | 6.4 (5.6–6.8) | 5.6 (5.2–5.9) | 0.001 | 5.8 (5.5–6.3) | 5.2 (5.0–5.6) | <0.001 | 0.994 |
| Total cholesterol (mg/dL) | 206.4 ± 41.8 | 185.4 ± 39.6 | 0.017 | 203.3 ± 34.8 | 194.9 ± 37.5 | 0.126 | 0.196 |
| HDL-cholesterol (mg/dL) | 44 (39–54) | 51 (40–54) | 0.222 | 47 (36–51) | 53 (42–63) | <0.001 | 0.148 |
| LDL-cholesterol (mg/dL) | 124.6 ± 34.7 | 113.2 ± 39.4 | 0.119 | 130.8 ± 30.1 | 125.6 ± 31.4 | 0.252 | 0.443 |
| Triglycerides (mg/dL) | 172 (115–217) | 101 (74–139) | 0.001 | 118 (93–171) | 83 (66–108) | <0.001 | 0.581 |
| Non-HDL-cholesterol (mg/dL) | 161.8 ± 42.2 | 136.1 ± 42.6 | 0.005 | 157.8 ± 30.2 | 143.0 ± 32.3 | 0.002 | 0.219 |
| CKD-Group (n = 18) | p-Value † | Control-Group (n = 38) | p-Value † | p-Value †† | |||
|---|---|---|---|---|---|---|---|
| 1 Year after Surgery | 5 Years after Surgery ¶ | 1 Year after Surgery | 5 Years after Surgery ¶ | ||||
| General clinical characteristics | |||||||
| BMI (Kg/m2) | 30.4 ± 4.8 | 32.0 ± 5.2 | 0.177 | 32.6 ± 4.2 | 34.4 ± 4.1 | 0.001 | 0.840 |
| EWL (%) | --- | 68.1 ± 19.6 | --- | --- | 59.9 ± 14.3 | --- | 0.093 |
| TWL (%) | --- | 29.5 ± 10.6 | --- | --- | 28.2 ± 7.9 | --- | 0.983 |
| WR (%) | --- | 16.2 (6.3–28.2) | --- | --- | 19.7 (11.7–25.7) | --- | 0.439 |
| Renal function | |||||||
| Serum creatinine (mg/dL) * | 1.35 (1.13–1.9) | 1.50 (1.08–1.8) | 0.130 | 0.7 (0.7–0.8) | 0.70 (0.6–0.8) | 0.118 | 0.004 |
| eGFR [CKD-EPI] (mL/min/1.73 m2) * | 48.8 ± 16.5 | 44.4 ± 19.5 | 0.028 | 91.7 ± 14.9 | 90.0 ± 16.0 | 0.345 | 0.375 |
| Comorbidities | |||||||
Hypertension, n (%)
| 13 (76.5) 2 (2–3) | 14 (82.4) 2 (1–2) | 1 0.317 | 17 (45.9) 2 (1–3) | 19 (51.3) 1 (1–2) | 0.727 0.936 | 0.800 --- |
Diabetes, n (%)
| 4 (23.5) 1 (5.9) 0 (0–0.5) | 3 (17.6) 1 (5.9) 1 (0–1) | 1 1 --- | 6 (16.2) 2 (5.4) 1 (1–1) | 4 (10.8) 1 (5.3) 1 (0.5–1.5) | 0.5001 --- | 0.598 --- --- |
Dyslipemia, n (%)
| 11 (57.9) 8 (42.1) | 10 (52.6) 6 (31.6) | 1 0.625 | 10 (26.3) 5 (13.2) | 13 (34.2) 10 (26.3) | 0.375 0.125 | 0.314 0.506 |
| OSAHS, n (%) | 1 (5.9) | 1 (5.9) | 1 | 6 (16.2) | 4 (10.8) | 0.625 | 0.350 |
| Laboratory characteristics | |||||||
| Glucose (mg/dL) | 114 (94–124) | 96 (84–105) | 0.887 | 116 (102–143) | 90 (85–96) | 0.148 | 0.753 |
| Hemoglobin A1c (%) | 6.4 (5.6–6.8) | 5.9 (5.6–6.1) | 0.499 | 5.8 (5.5–6.2) | 5.5 (5.3–5.7) | 0.036 | 0.980 |
| Total cholesterol (mg/dL) | 186.4 ± 40.6 | 195.9 ± 40.7 | 0.157 | 194.7 ± 37.7 | 195.6 ± 35.9 | 0.910 | 0.440 |
| HDL-cholesterol (mg/dL) | 51 (45–54) | 55 (49–62) | 0.029 | 52 (42–61) | 57 (49–66) | 0.015 | 0.973 |
| LDL-cholesterol (mg/dL) | 117.4 ± 39.3 | 118.3 ± 38.0 | 0.873 | 125.9 ± 30.9 | 118.6 ± 30.6 | 0.199 | 0.353 |
| Triglycerides (mg/dL) | 94 (74–132) | 113 (66–135) | 0.435 | 80.5 (71–101) | 80.5 (70–112) | 0.831 | 0.376 |
| Non-HDL-cholesterol (mg/dL) | 136.5 ± 43.9 | 139.4 ± 43.1 | 0.637 | 143.9 ± 32.7 | 136.7 ± 32.6 | 0.231 | 0.279 |
| Obesity-CKD (n = 10) | Non-Obesity-CKD (n = 9) | p-Value | |
|---|---|---|---|
| General clinical characteristics | |||
| Sex (female), n (%) | 6 (60.0) | 6 (66.7) | 0.764 |
| Age (years) | 56.2 (54.0–61.1) | 54.6 (53.1–55.8) | 0.191 |
| Weight (Kg) | 112.7 (103.0–127.0) | 125.0 (108.0–127.7) | 0.567 |
| BMI (Kg/m2) | 46.2 (39.2–53.3) | 44.5 (39.4–47.5) | 0.683 |
| Comorbidities | |||
| Hypertension, n (%) | 8 (80.0) | 2 (20.0) | 0.156 |
| Diabetes, n (%) | 5 (50.0) | 2 (22.2) | 0.210 |
| Dyslipemia, n (%) | 8 (80.0) | 8 (88.9) | 0.596 |
| OSAHS, n (%) | 1 (10.0) | 3 (33.3) | 0.213 |
| Heart disease, n (%) | 3 (30.0) | 0 (0.0) | 0.073 |
| Baseline renal function | |||
| Serum creatinine (mg/dL) | 1.4 (1.2–1.5) | 2.2 (1.8–2.6) | 0.018 |
| eGFR [CKD-EPI] (mL/min/1.73 m2) | 48.6 (39.2–52.6) | 28.6 (25.4–32.5) | 0.011 |
CKD stage, n (%)
| 9 (90.0) 1 (10.0) | 4 (44.4) 5 (55.6) | 0.033 |
| Mortality during follow-up | |||
Number of deaths, n (%)
| 3 (30.0) 1 1 1 0 | 2 (22.2) 0 1 0 1 | 0.701 |
| CKD Group (n = 19) | Control-Group (n = 38) | p-Value | |
|---|---|---|---|
| Hospitalization parameters | |||
| Length of stay (days) | 4.0 (2.9–6.2) | 3.8 (2.9–4.2) | 0.531 |
| Surgical time (min) | 95 (70–115) | 80 (67–110) | 0.525 |
| Post-operative complications | |||
| Early (<30 days) Major
| 4 (21.1) 1/4 (25.0) 1/4 (25.0) 1/4 (25.0) 1/4 (25.0) 0/4 (0.0) | 4 (10.5) 2/4 (50.0) 0/4 (0.0) 1/4 (25.0) 0/4 (0.0) 1/4 (25.0) | 0.281 |
| Late (>30 days) Major
| 3 (15.8) 1/3 (33.3) 1/3 (33.3) 0/3 (0.0) 0/3 (0.0) 1/3 (33.3) | 2 (5.3) 0/2 (0.0) 0/2 (0.0) 1/2 (50.0) 1/2 (50.0) 0/2 (0.0) | 0.185 |
Acute kidney injury
| 2 (10.5) 0/2 (0.0) | 0 (0.0) --- | 0.042 |
| Mortality during follow-up | |||
Number of deaths
| 5 (26.3) 1/5 (20.0) 2/5 (40.0) 1/5 (20.0) 1/5 (20.0) | 1 (2.6) 1/1 (100) --- --- --- | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pané, A.; Claro, M.; Molina-Andujar, A.; Olbeyra, R.; Romano-Andrioni, B.; Boswell, L.; Montagud-Marrahi, E.; Jiménez, A.; Ibarzabal, A.; Viaplana, J.; et al. Bariatric Surgery Outcomes in Patients with Chronic Kidney Disease. J. Clin. Med. 2023, 12, 6095. https://doi.org/10.3390/jcm12186095
Pané A, Claro M, Molina-Andujar A, Olbeyra R, Romano-Andrioni B, Boswell L, Montagud-Marrahi E, Jiménez A, Ibarzabal A, Viaplana J, et al. Bariatric Surgery Outcomes in Patients with Chronic Kidney Disease. Journal of Clinical Medicine. 2023; 12(18):6095. https://doi.org/10.3390/jcm12186095
Chicago/Turabian StylePané, Adriana, Maria Claro, Alicia Molina-Andujar, Romina Olbeyra, Bárbara Romano-Andrioni, Laura Boswell, Enrique Montagud-Marrahi, Amanda Jiménez, Ainitze Ibarzabal, Judith Viaplana, and et al. 2023. "Bariatric Surgery Outcomes in Patients with Chronic Kidney Disease" Journal of Clinical Medicine 12, no. 18: 6095. https://doi.org/10.3390/jcm12186095
APA StylePané, A., Claro, M., Molina-Andujar, A., Olbeyra, R., Romano-Andrioni, B., Boswell, L., Montagud-Marrahi, E., Jiménez, A., Ibarzabal, A., Viaplana, J., Ventura-Aguiar, P., Amor, A. J., Vidal, J., Flores, L., & de Hollanda, A. (2023). Bariatric Surgery Outcomes in Patients with Chronic Kidney Disease. Journal of Clinical Medicine, 12(18), 6095. https://doi.org/10.3390/jcm12186095