
Antenatal, Intrapartum and Postpartum Interventions for Preventing Postpartum Urinary and Faecal Incontinence: An Umbrella Overview of Cochrane Systematic Reviews


Abstract
:1. Introduction
What Is the Issue
2. Materials and Methods
2.1. Objectives
2.2. Criteria for Inclusion
2.3. Participants
2.4. Interventions
2.5. Outcomes of Interest
2.6. Search Strategy
2.7. Data Collection and Analysis
2.7.1. Selection of Reviews
2.7.2. Data Extraction and Management
- review title and authors;
- date that the review was last assessed as up-to-date;
- number of included trials;
- number of participants in the trials and their characteristics;
- quality of the included trials (as reported by the review authors);
- interventions pertinent to this overview;
- all predetermined outcomes pertinent to this overview.
- number of studies and participants contributing data relevant to this overview;
- the summary intervention effects: risk ratios (RR) or odds ratios (OR) with 95% confidence intervals (CI);
- data needed to evaluate the quality of evidence regarding the intervention’s impact.
2.7.3. Assessment of Methodological Quality of Included Reviews
Quality of Included Reviews
Methodological Quality
- High
- Moderate
- Low
- Critically low
Risk of Bias
- Study eligibility criteria;
- Identification and selection of studies;
- Data collection and study appraisal;
- Synthesis and findings.
Quality of Included Studies within Reviews
Quality of Evidence in Included Reviews
- Study limitations: internal validity of the evidence;
- Inconsistency: discrepancy or fluctuation in the effect measurements across studies;
- Indirectness: extent of disparities among populations;
- Imprecision (random error): the level of confidence in the effect estimate to make informed decisions;
- Publication bias: the degree to which studies with certain results are selectively published.
- High: additional research is highly improbable to alter our level of confidence in the effect estimate;
- Moderate: additional studies are likely to substantially influence our level of confidence in the effect estimate and could potentially lead to revisions in the estimate;
- Low: further research is highly likely to significantly impact our confidence in the effect estimate and is likely to change the estimate;
- Very low: the effect estimate is highly uncertain.
Data Synthesis
- We summarized the main results of the included reviews by organizing by intervention topic.
- Effective interventions: the review provided strong evidence supporting their effectiveness;
- Potentially effective interventions: the review provided reasonable evidence supporting their effectiveness;
- Ineffective interventions: the review provided strong evidence showing they are not effective;
- Probably ineffective interventions: the review provided reasonable evidence suggesting they are not effective;
- No conclusion possible: the review had limited or very uncertain evidence.
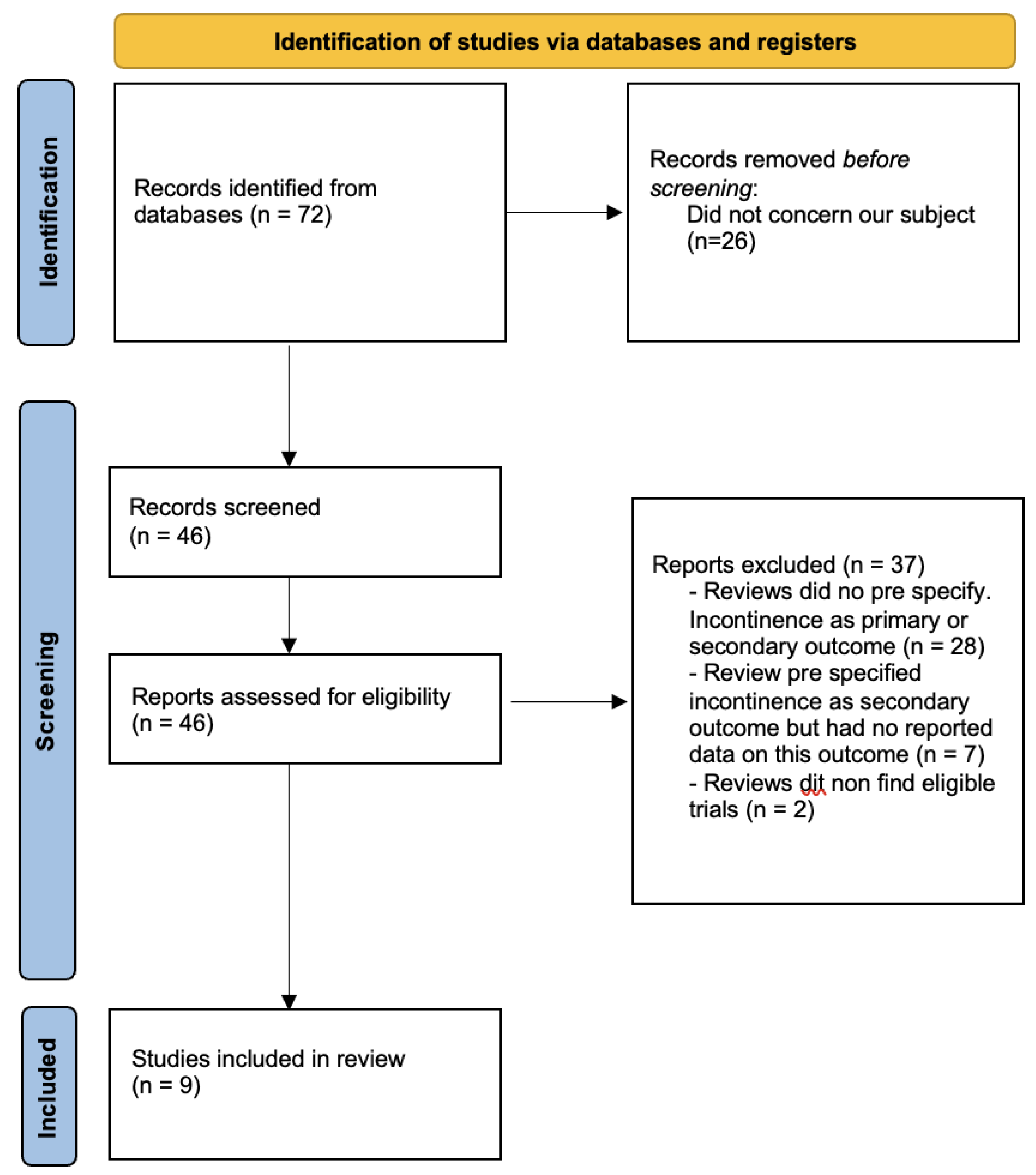
3. Results
- Three evaluated vaginal delivery versus caesarean delivery:
- One compared instruments (forceps and vacuum) for assisted delivery [8].
- One evaluated the effects of antenatal perineal massage [9].
- One evaluated the effects of antenatal or postnatal pelvic floor muscle training [10].
- One compared performing episiotomy only if needed versus routine episiotomy [11].
- Two evaluated the repair of perineal tears:
3.1. Methodological Quality of Included Reviews
- All reviews indicated the components of PICO;
- All reviews predetermined their study design;
- All reviews pre-specified which study design will be included, but only four explain why they choose this design;
- All reviews used a comprehensive search strategy;
- All reviews reported that study selection and data extraction were conducted independently by different people;
- All reviews presented lists of studies that were excluded;
- All reviews provided detailed characteristics of the studies that were included;
- All reviews used an appropriate and satisfactory method for evaluating the risk of bias in the included studies;
- Eight reviews used appropriate methods for the statistical combination of results and assessment of the potential impact of risk of bias on the results of the meta-analysis. The last review conducted no meta-analysis because only one trial was included [12];
- All the reviews took into account the risk of bias in individual studies when interpreting the results;
- All the reviews provided a satisfactory explanation for the heterogeneity observed in the results;
- None of the reviews carried out an adequate investigation of publication bias;
- Only one review did not report any potential sources of conflict of interest [11].
3.2. Effects of Interventions
3.3. Probably Ineffective Interventions: Moderate-Quality Evidence
3.4. Probably Effective Interventions: Moderate-Quality Evidence
4. Discussion
4.1. Summary of Main Results
- When performing an endo-anal ultrasound after childbirth and prior to repairing any perineal tears (moderate-quality evidence);
- When using a vacuum instead of forceps for instrumented vaginal deliveries (moderate-quality evidence);
- When pelvic floor muscle training is performed postpartum (moderate-quality evidence).
4.2. Overall Completeness and Applicability of Evidence
4.3. Quality of the Evidence
4.4. Potential Biases in the Overview Procedure
4.5. Consensus and Disparities with Other Studies
- Some recommendations included that routine episiotomy does not prevent severe perineal trauma [10];
- A vaginal delivery with vacuum resulted in less damage to the perineum than the forceps [7];
- The systematic search of obstetrical anal sphincter injury is necessary after vaginal delivery to adapt the repair [12];
- Antenatal pelvic floor muscle training seems to be beneficial to prevent incontinence postpartum [9];
- Caesarean delivery could be beneficial to prevent incontinence post-partum compared to vaginal delivery [4].
5. Authors’ Conclusions
5.1. Implications for Practice
5.2. Implications for Research
- A shortage of primary research exists, with few long-term, follow-up studies on women involving randomized trials of antenatal, intrapartum and postpartum interventions.
- Insufficient reporting on urinary and faecal incontinence by randomized trials.
- Insufficient reporting on incontinence postpartum by relevant Cochrane reviews (probably because it was not predefined as an outcome).
- The absence of a Cochrane review evaluating potentially relevant interventions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Ongoing Reviews
| Review Citation | Overview of Pre-Specified Outcomes in the Protocol |
| Aasheim et al. | Secondary outcomes included
|
| Dodd et al. | Secondary outcomes included
|
| Elharmeel et al. | Secondary outcomes included
|
| Gupta et al. | Secondary outcomes included
|
| Hofmeyr et al. | Secondary outcomes included
|
| Torvaldsen et al. | Secondary outcomes included
|
| Zhou F et al. | Secondary outcomes
|
|
Appendix B. Reviews Awaiting Further Classification
| Review Citation | Overview of Pre-Specified Outcomes in Review with No Outcome Data | Main Conclusion of Review |
| Farrar et al. | Primary outcome included
| No included trials. “No completed trials that met the inclusion criteria of the review were identified”. |
| Hofmeyr et al. | Secondary outcomes included
| No included trials. “We found no randomized or quasi-randomized trials of symphysiotomy for either inclusion or exclusion”. |
Appendix C. AMSTAR 2 Criteria
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
References
- Pollock, M.; Fernandes, R.M.; Becker, L.A.; Pieper, D.; Hartling LChapter, V. Overviews of Reviews. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.4 (Updated August 2023); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Available online: https://training.cochrane.org/handbook/current/chapter-v.2023 (accessed on 6 September 2023).
- Brown, J.; Alwan, N.A.; West, J.; Brown, S.; McKinlay, C.J.; Farrar, D.; Crowther, C.A. Lifestyle interventions for the treatment of women with gestational diabetes. Cochrane Database Syst. Rev. 2017, 5, CD011970. [Google Scholar] [CrossRef] [PubMed]
- Glazener, C.M.; MacArthur, C.; Hagen, S.; Elders, A.; Lancashire, R.; Herbison, G.P.; Wilson, P.D.; ProLong Study Group. Twelve-year follow-up of conservative management of postnatal urinary and faecal incontinence and prolapse outcomes: Randomised controlled trial. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Bols, E.M.J.; Hendriks, E.J.M.; Berghmans, B.C.M.; Baeten, C.G.M.I.; Nijhuis, J.G.; de Bie, R.A. A systematic review of etiological factors for postpartum fecal incontinence. Acta Obstet. Gynecol. Scand. 2010, 89, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.L.; Furner, S.E.; Westercamp, M.; Farquhar, C. Cesarean delivery for the prevention of anal incontinence. Cochrane Database Syst. Rev. 2010, 2. [Google Scholar] [CrossRef] [PubMed]
- Hofmeyr, G.J.; Hannah, M.; Lawrie, T.A. Planned caesarean section for term breech delivery. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Hofmeyr, G.; Barrett, J.; Crowther, C. Planned caesarean section for women with a twin pregnancy. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, F.; Hofmeyr, G.J.; Menon, V. Choice of instruments for assisted vaginal delivery. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef] [PubMed]
- Beckmann, M.M.; Stock, O.M. Antenatal perineal massage for reducing perineal trauma. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Woodley, S.J.; Lawrenson, P.; Boyle, R.; Cody, J.D.; Mørkved, S.; Kernohan, A.; Hay-Smith, E.J.C. Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst. Rev. 2020, 5. [Google Scholar] [CrossRef]
- Jiang, H.; Qian, X.; Carroli, G.; Garner, P. Selective versus routine use of episiotomy for vaginal birth. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K.A.; Grivell, R.M. Use of endoanal ultrasound for reducing the risk of complications related to anal sphincter injury after vaginal birth. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Fernando, R.J.; Sultan, A.H.; Kettle, C.; Thakar, R. Methods of repair for obstetric anal sphincter injury. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Harvey, L.A. Summaries of Cochrane Systematic Reviews: Making high-quality evidence accessible. Spinal Cord 2018, 56, 185. [Google Scholar] [CrossRef] [PubMed]
- King, J. Are there adverse outcomes for child health and development following caesarean section delivery? Can we justify using elective caesarean section to prevent obstetric pelvic floor damage? Int. Urogynecol. J. 2021, 32, 1963–1969. [Google Scholar] [CrossRef] [PubMed]
- Driusso, P.; Beleza, A.C.S.; Mira, D.M.; de Oliveira Sato, T.; de Carvalho Cavalli, R.; Ferreira, C.H.J.; de Fátima Carreira Moreira, R. Are there differences in short-term pelvic floor muscle function after cesarean section or vaginal delivery in primiparous women? A systematic review with meta-analysis. Int. Urogynecol. J. 2020, 31, 1497–1506. [Google Scholar] [CrossRef] [PubMed]
- Jurczuk, M.; Bidwell, P.; Gurol-Urganci, I.; van der Meulen, J.; Sevdalis, N.; Silverton, L.; Thakar, R. The OASI care bundle quality improvement project: Lessons learned and future direction. Int. Urogynecol. J. 2021, 32, 1989–1995. [Google Scholar] [CrossRef] [PubMed]
- Bidwell, P.; Sevdalis, N.; Silverton, L.; Harris, J.; Gurol-Urganci, I.; Hellyer, A.; Freeman, R.; van der Meulen, J.; Thakar, R. Women’s experiences of the OASI Care Bundle; a package of care to reduce severe perineal trauma. Int. Urogynecol. J. 2021, 32, 1807–1816. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Review ID | Reason for Exclusion |
|---|---|
| Kettle et al. | No outcome focused on incontinence |
| Hodnett et al. | No outcome focused on incontinence |
| O’Kelly et al. | No outcome focused on incontinence |
| Bonet et al. | No outcome focused on incontinence |
| Liabsuetrakul et al. | No outcome focused on incontinence |
| Buppasiri et al. | No outcome focused on incontinence |
| Nygaard et al. | No outcome focused on incontinence |
| Shepherd et al. | No outcome focused on incontinence |
| Lavender et al. | Not concerning perineal trauma in postpartum |
| McIntyre et al. | Not concerning perineal trauma in postpartum |
| Berghella et al. | Not concerning perineal trauma in postpartum |
| Bamigboye et al. | No outcome focused on incontinence |
| Sheperd et al. | Not concerning perineal trauma in postpartum |
| Simmons et al. | Not concerning perineal trauma in postpartum |
| Quijano et al. | Not concerning perineal trauma in postpartum |
| Kettle et al. | No outcome focused on incontinence |
| Bohren et al. | Not concerning perineal trauma in postpartum |
| Ciapponi et al. | Not concerning perineal trauma in postpartum |
| Amorim Adegboye | Not concerning perineal trauma in postpartum |
| Tieu et al. | Not concerning perineal trauma in postpartum |
| Lavender et al. | Not concerning perineal trauma in postpartum |
| Reveiz et al. | No outcome focused on incontinence |
| Brown et al. | Not concerning perineal trauma in postpartum |
| Ostaszkiewicz et al. | Not concerning perineal trauma in postpartum |
| Cluett et al. | No outcome focused on incontinence |
| Middleton et al. | No outcome focused on incontinence |
| Boulvain et al. | No outcome focused on incontinence |
| Horey et al. | Not concerning perineal trauma in postpartum |
| Balogun et al. | No outcome focused on incontinence |
| Turawa et al. | No outcome focused on incontinence |
| Lawrie et al. | Not concerning perineal trauma in postpartum |
| Brown et al. | Not concerning perineal trauma in postpartum |
| East et al. | No outcome focused on incontinence |
| Walker et al. | Not concerning perineal trauma in postpartum |
| Sandall et al. | Not concerning perineal trauma in postpartum |
| Cody et al. | Not concerning perineal trauma in postpartum |
| Wuytack et al. | No outcome focused on incontinence |
| Costley et al. | No outcome focused on incontinence |
| Abalos et al. | No outcome focused on incontinence |
| Maeda et al. | Not concerning perineal trauma in postpartum |
| Hay-Smith et al. | Not concerning perineal trauma in postpartum |
| Bietsy et al. | No outcome focused on incontinence |
| Hedayati et al. | No outcome focused on incontinence |
| Bonet et al. | No outcome focused on incontinence |
| Basevi et al. | Not concerning perineal trauma in postpartum |
| Downe et al. | No outcome focused on incontinence |
| Tieu et al. | Not concerning perineal trauma in postpartum |
| Dudley et al. | No outcome focused on incontinence |
| Maher et al. | Not concerning perineal trauma in postpartum |
| Baessler et al. | Not concerning perineal trauma in postpartum |
| Hay smith | No outcome focused on incontinence |
| Hedayati et al. | No outcome focused on incontinence |
| Majoko et al. | No outcome focused on incontinence |
| Herbison et al. | Not concerning perineal trauma in postpartum |
| Torvaldsen et al. | Secondary outcomes included Incidence of urinary incontinence postpartum Incidence of faecal incontinence postpartum No outcome data for these outcomes |
| Elharmeel et al. | Secondary outcomes included Urinary and faecal incontinence No outcome data for theses outcomes |
| Dodd et al. | Secondary outcomes included Symptoms related to pelvic floor damage No outcome data for this outcome |
| Gupta et al. | Secondary outcome included Urinary or faecal incontinence No outcome data for this outcome |
| Aasheim et al. | Secondary outcome included -Stress incontinence No outcome data for these outcomes |
| Zhou F et al. | Secondary outcomes Urinary incontinence Faecal incontinence No outcome data for these outcomes |
| Hofmeyr et al. | Secondary outcomes included Faecal incontinence Urinary incontinence No outcome data for these outcomes |
| Farrar et al. | Primary outcome included Anal incontinence Secondary outcome included Faecal incontinence Urinary incontinence No eligible trials identified |
| Hofmeyr et al. | Secondary outcomes included Urinary incontinence Flatus incontinence Faecal incontinence No studies included |
| Review ID | Date of Search | No. Included trials, Countries and Years of Publication No. Participants | Inclusion Criteria | Relevant Intervention and Comparison | Outcomes and Period of Evaluation |
|---|---|---|---|---|---|
| Caesarean delivery for the prevention of anal incontinence Nelson 2010 | July 2009 | 21 studies, 1 RCT and 20 non-randomized studies 31,698 women | Women with a history of pregnancy and delivery of a live infant, including breech presentations and twin pregnancies. | Caesarean delivery versus vaginal delivery | Anal incontinence as primary outcome |
| Choice of instruments for assisted vaginal delivery O’Mahony 2010 | 31 May 2010 | 32 RCTs 6597 women | Women in the second stage of labour due for instrumental vaginal delivery. |
| Urinary and faecal incontinence as secondary outcomes |
| Antenatal perineal massage for reducing perineal trauma Beckmann 2013 | 23 October 2012 | 4 RCTs 2497 women | Pregnant women who are planning vaginal birth. | Any method of perineal massage undertaken by women and/or her partner versus no massage. | Urinary and faecal incontinence as secondary outcomes |
| Methods of repair for obstetric anal sphincter injury Fernando 2013 | 30 September 2013 | 6 RCTs 588 women | Women who sustained OASIS and in whom the repair was performed in the immediate postpartum period (primary repair). | Overlap versus end- to-end technique. | Anal incontinence as primary outcome |
| Planned caesarean section for term breech delivery Hofmeyr 2015a | 31 March 2015 | 3 RCTs 2396 women | Women with breech presentation considered suitable for vaginal delivery. | Planned caesarean section compared with planned vaginal birth. | Urinary and faecal incontinence as secondary outcomes |
| Use of endoanal ultrasound for reducing the risk of complications related to anal sphincter injury after vaginal birth Walsh 2015 | 31 August 2015 | 1 RCT 752 women | Women after a vaginal birth, including spontaneous and assisted vaginal births. |
| Severe anal incontinence at ≥ six months as primary outcome |
| Planned caesarean section for women with a twin pregnancy Hofmeyr 2015b | 18 November 2015 | 2 RCTs 2864 women | Women with viable twin pregnancy considered suitable for vaginal birth. | Planned caesarean section compared with planned vaginal birth. | Urinary and faecal incontinence as secondary outcomes |
| Selective versus routine use of episiotomy for vaginal birth Jiang 2017 | 14 September 2016 | 12 RCTs 6177 women | Pregnant women having spontaneous or assisted vaginal births. | Performing episiotomy only if needed (’selective’ versus routine episiotomy). | Long-term effects including urinary incontinence and faecal incontinence as main outcomes |
| Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women Woodley 2020 | 7 August 2019 | 46 RCTs 10,382 women | Populations included women who, at randomization, were continent (PFMT for prevention) or incontinent (PFMT for treatment), and a mixed population of women who were one or the other (PFMT for prevention or treatment). | Antenatal PFMT versus no PFMT, usual care or other control condition for the postnatal PFMT versus no PFMT, usual care. | Urinary and faecal incontinence as primary outcomes |
| Components of PICO | A priori Design | Explanation for Selection of Studies | Search Strategy | Duplicate Selection and Extraction | Excluded Studies List | Characteristics of Included Studies | Assessment Risk of Bias | Report of Fundings | Appropriate Methods for Résults in Meta-analysis | Assessment of RoB on the Results of the Meta-analysis | Account for RoB when Discussing Results of the Review | Explanation for any Heterogeneity | Investigation of Publication Bias and Discuss Its likely Impact of the Results | Report of any Conflict of Interest | Total | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fernando et al., 2013 | + | + | + | +/− | + | + | + | + | − | + | + | + | + | − | + | High Quality |
| Woodley et al., 2020 | + | + | − | +/− | + | + | + | + | + | + | + | + | + | − | + | High Quality |
| Jiang et al., 2017 | + | + | − | +/− | + | + | + | + | + | + | + | + | + | − | − | High Quality |
| Walsh et al., 2015 | + | + | + | +/− | + | / | + | + | + | / | / | + | + | / | + | High Quality |
| Nelson et al., 2010 | + | + | + | +/− | + | + | + | + | − | + | + | + | + | − | + | High Quality |
| Hoffmeyr et al., 2015 | + | + | + | +/− | + | + | + | + | + | + | + | + | + | − | + | High Quality |
| Hoffmeyr et al., 2015 | + | + | + | +/− | + | + | + | + | + | + | + | + | + | − | + | High Quality |
| O’mahony et al., 2010 | + | + | − | +/− | + | + | +/− | + | − | + | + | + | + | − | + | High Quality |
| Beckmann et al., 2013 | + | + | − | +/− | + | + | + | + | − | + | + | + | + | − | + | High Quality |
| Study Eligibility Criteria | Identification and Selection of Studies | Data Collection and Study Appraisal | Synthesis and Findings | Overall Risk of Biais | |
|---|---|---|---|---|---|
| “Caesarean delivery for the prevention of anal incontinence” Nelson et al., 2010 | Low risk | Low risk | Low risk | Low risk | Low risk |
| “Choice of instruments for assisted vaginal delivery” O’Mahony et al., 2010 | Low risk | Low risk | Low risk | Low risk | Low risk |
| “Antenatal perineal massage for reducing perineal trauma” Beckmann et al., 2013 | Low risk | Low risk | Low risk | Low risk | Low risk |
| “Methods of repair for obstetric anal sphincter injury” Fernando 2013 | Low risk | Low risk | Low risk | Low risk | Low risk |
| “Planned caesarean section for term breech delivery” Hofmeyr et al., 2015 | Low risk | Low risk | Low risk | Low risk | Low risk |
| “Use of endoanal ultrasound for reducing the risk of complications related to anal sphincter injury after vaginal birth” Walsh 2015 | Low risk | Low risk | Low risk | Low risk | Low risk |
| “Planned caesarean section for women with a twin pregnancy” Hofmeyr et al., 2015 | Low risk | Low risk | Low risk | Low risk | Low risk |
| “Selective versus routine use of episiotomy for vaginal birth” Jiang 2017 | Low risk | Low risk | Low risk | Low risk | Low risk |
| “Pelvic floor muscle training for preventing and treating urinary and faecal incontinence in antenatal and postnatal women” Woodley 2020 | Low risk | Low risk | Low risk | Low risk | Low risk |
| Intervention and Comparison | Outcome | Reference | RR Urinary Incontinence | RR Faecal Incontinence | Quality of the Evidence (GRADE) | Comments |
|---|---|---|---|---|---|---|
| Clinical examination versus use of endoanal ultrasound prior to repairing perineal tears. | Reduction in severe anal incontinence at greater than 6 months postpartum. | Walsh et al. [12] | / | RR 0.48 (95% CI 0.24 to 0.97) | Moderate | The use of endoanal ultrasound prior to repairing any perineal tears may reduce severe anal incontinence compared with routine care. |
| Selective versus routine use of episiotomy. | Long-term effects: urinary or faecal incontinence. | Jiang et al. [11] | RR 0.98 (95% CI 0.67 to 1.44) | No reported data | Low | Did not demonstrate a clear difference in urinary incontinence between selective or routine episiotomy at six months or more, postpartum. |
| Assess the effects of PFMT for preventing or treating urinary and faecal incontinence in postnatal women. | Self-reported urinary or faecal incontinence. | Woodley et al. [10] | Early postnatal period: RR 0.38 (95% CI 0.17 to 0.83) Mid-postnatal period (three to six months): RR0.71 (95% CI 0.54 to 0.95) Late postnatal period (12 months): RR 1.20 (95% CI 0.65 to 2.21) | No reported data | Low to moderate | PFMT may reduce urinary incontinence in early and mid-postnatal periods, but no difference was provided in late postnatal period. |
| Overlap repair versus end-to-end repair following OASIS. | Anal incontinence symptoms | Fernando et al. [13] | / | Anal incontinence at: 6 weeks: RR 0.65 (95% CI 0.20 to 2.07) 3 months: RR 0.84 (95% CI 0.06 to 12.73) 6 months: RR 0.48 (95% CI 0.02 to 12.89) 12 months: RR 0.37 (95% CI 0.03 to 4.68) 24 months: RR 0.88 (95% CI 0.32 to 2.41) 36 months: RR 1.01 (95% CI 0.34 to 2.98) | Low | No statistically significant difference in anal incontinence between the 2 repair techniques. |
| Caesarean delivery (CD) in comparison to vaginal delivery (VD) to preserve anal continence. | Anal incontinence | Nelson et al. [5] | / | CD vs. VD: OR 0.93 (95% CI 0.77 to 1.13) | Moderate | No benefit for CD over VD on anal incontinence has been demonstrated. |
| Effect of antenatal digital perineal massage on the incidence of perineal trauma at birth and Subsequent morbidity | Secondary outcomes: urinary or faecal incontinence at 3 months postpartum. | Beckmann et al. [9] | RR 0.90 (95% CI 0.74 to 1.08) | RR 0.70 (95% CI 0.27 to 1.80) | Moderate | No difference was seen in urinary or faecal incontinence after antenatal digital perineal massage. |
| Evaluate different instruments in terms of achieving a vaginal birth and avoiding significant morbidity for mother. | Secondary outcome at long-term: urinary and faeal incontinence. | O’Mahony et al [8] | / | Vacuum vs. Forceps: RR 0.56 95% CI 0.61 to 0.84, one trial, and 130 women | Moderate | Flatus incontinence/altered continence seems more likely with forceps. |
| Assess the effects of planned caesarean section for singleton breech presentation at term on measures of pregnancy outcome. | Secondary outcomes: urinary and faecal incontinence at 3 months and 2 years post- partum. | Hofmeyr et al. [6] | -At 3 months: RR 0.62 (95% CI 0.41 to 0.93) -at 2 years: RR 1.14 (95% CI 0.81 to 1.61) | -At 3 months: RR 0.54 (95% RR 0.18 to 1.62) -At 2 years: RR 1.11, (95% CI 0.47 to 2.58) | Low | At 3 months, planned caesarean may reduce urinary incontinence, but no difference detected for faecal incontinence. At 2 years, no difference was detected. |
| To determine the short- and long-term effects on mothers and their babies of planned caesarean section for twin pregnancy. | Secondary outcomes: urinary and faecal incontinence. | Hofmeyr et al. [7] | RR 0.87 (95% CI 0.64 to 1.18) | RR 1.02 (95% CI 0.69 to 1.51) | Moderate | No difference detected. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sananès, J.; Pire, S.; Feki, A.; Boulvain, M.; Faltin, D.L. Antenatal, Intrapartum and Postpartum Interventions for Preventing Postpartum Urinary and Faecal Incontinence: An Umbrella Overview of Cochrane Systematic Reviews. J. Clin. Med. 2023, 12, 6037. https://doi.org/10.3390/jcm12186037
Sananès J, Pire S, Feki A, Boulvain M, Faltin DL. Antenatal, Intrapartum and Postpartum Interventions for Preventing Postpartum Urinary and Faecal Incontinence: An Umbrella Overview of Cochrane Systematic Reviews. Journal of Clinical Medicine. 2023; 12(18):6037. https://doi.org/10.3390/jcm12186037
Chicago/Turabian StyleSananès, Juliette, Sophie Pire, Anis Feki, Michel Boulvain, and Daniel L. Faltin. 2023. "Antenatal, Intrapartum and Postpartum Interventions for Preventing Postpartum Urinary and Faecal Incontinence: An Umbrella Overview of Cochrane Systematic Reviews" Journal of Clinical Medicine 12, no. 18: 6037. https://doi.org/10.3390/jcm12186037
APA StyleSananès, J., Pire, S., Feki, A., Boulvain, M., & Faltin, D. L. (2023). Antenatal, Intrapartum and Postpartum Interventions for Preventing Postpartum Urinary and Faecal Incontinence: An Umbrella Overview of Cochrane Systematic Reviews. Journal of Clinical Medicine, 12(18), 6037. https://doi.org/10.3390/jcm12186037