
Effect of a Real-Time Audio Ventilation Feedback Device on the Survival Rate and Outcomes of Patients with Out-of-Hospital Cardiac Arrest: A Prospective Randomized Controlled Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
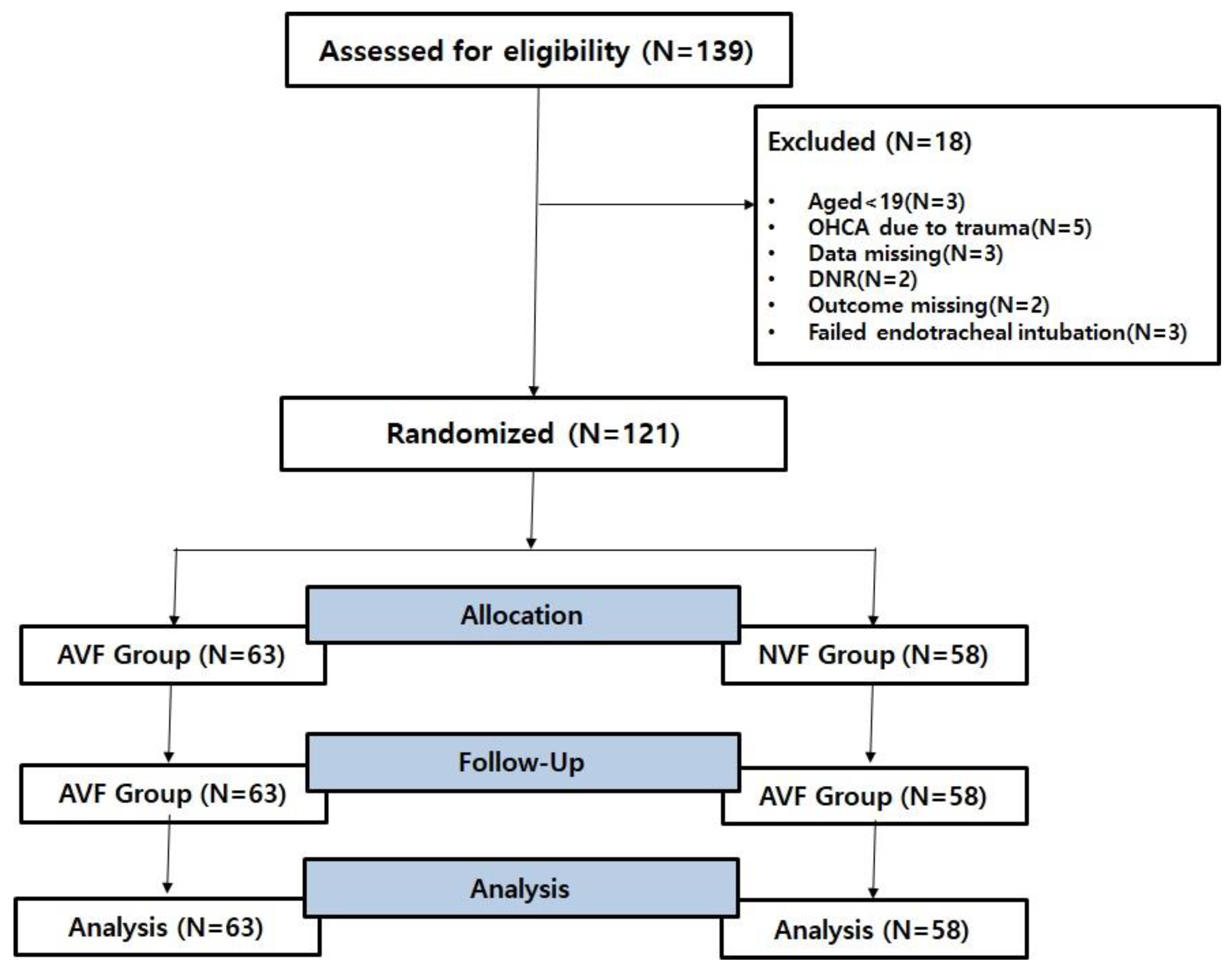
2.2. Selection of Participants and Data Collection
2.3. Sample Size Calculation
2.4. Outcomes
2.5. Data Analysis
2.6. Equipment
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Effect of AVF Device on the Prognosis of Patients with Out-of-Hospital Cardiac Arrest
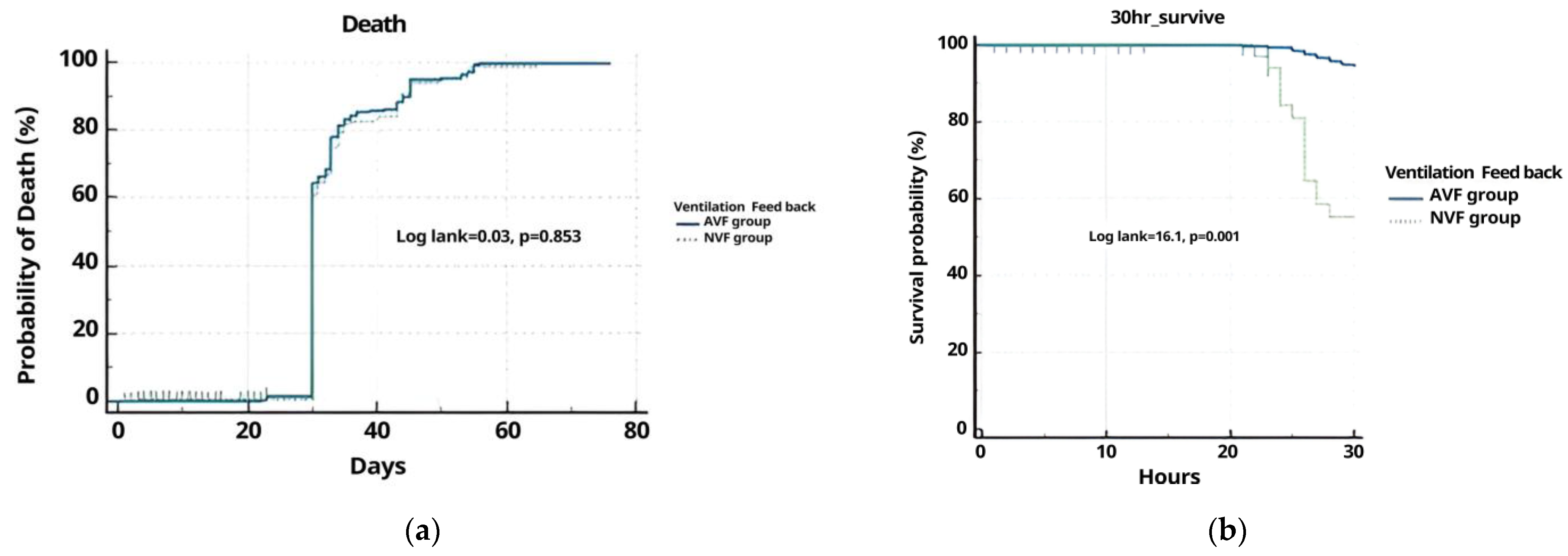
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nolan, J.P. High-quality cardiopulmonary resuscitation. Curr. Opin. Crit. Care 2014, 20, 227–233. [Google Scholar] [CrossRef]
- Song, F.; Sun, S.; Ristagno, G.; Yu, T.; Shan, Y.; Chung, S.P.; Weil, M.H.; Tang, W. Delayed high-quality CPR does not improve outcomes. Resuscitation 2011, 82, S52–S55. [Google Scholar] [CrossRef]
- Sugiyama, A.; Duval, S.; Nakamura, Y.; Yoshihara, K.; Yannopoulos, D. Impedance threshold device combined with high-quality cardiopulmonary resuscitation improves survival with favorable neurological function after witnessed out-of-hospital cardiac arrest. Circ. J. 2016, 80, 2124–2132. [Google Scholar] [CrossRef]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142, S366–S468. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.; Aiello, S.; Govender, K.; Shaw, B.; Tseng, B.; Dawad, Z.; McAulay, M.; Wilkinson, N. The impact of a ventilation timing light on CPR Quality: A randomized crossover study. Resusc. Plus 2023, 14, 100404. [Google Scholar] [CrossRef]
- Hon, K.L.; Cheung, S.T.; Tan, Y.W.; Leung, K.K.Y.; Ho, A.; Chan, H.B.; Qian, S.Y. Are we compressing and ventilating effectively during cardiopulmonary resuscitation? Curr. Pediatr. Rev. 2023. [Google Scholar] [CrossRef] [PubMed]
- Aoki, T.; Wong, V.; Endo, Y.; Hayashida, K.; Takegawa, R.; Shoaib, M.; Miyara, S.J.; Choudhary, R.C.; Yin, T.; Saeki, K.; et al. Insufficient oxygen inhalation during cardiopulmonary resuscitation induces early changes in hemodynamics followed by late and unfavorable systemic responses in post-cardiac arrest rats. Faseb J. 2023, 37, e23001. [Google Scholar] [CrossRef]
- Merrell, J.G.; Scott, A.C.; Stambro, R.; Boukai, A.; Cooper, D.D. Improved simulated ventilation with a novel tidal volume and peak inspiratory pressure controlling bag valve mask: A pilot study. Resusc. Plus 2023, 13, 100350. [Google Scholar] [CrossRef]
- Orlob, S.; Wittig, J.; Hobisch, C.; Auinger, D.; Honnef, G.; Fellinger, T.; Ristl, R.; Schindler, O.; Metnitz, P.; Feigl, G.; et al. Reliability of mechanical ventilation during continuous chest compressions: A crossover study of transport ventilators in a human cadaver model of CPR. Scand. J. Trauma Resusc. Emerg. Med. 2021, 29, 102. [Google Scholar] [CrossRef]
- Lyngby, R.M.; Clark, L.; Kjoelbye, J.S.; Oelrich, R.M.; Silver, A.; Christensen, H.C.; Barfod, C.; Lippert, F.; Nikoletou, D.; Quinn, T.; et al. Higher resuscitation guideline adherence in paramedics with use of real-time ventilation feedback during simulated out-of-hospital cardiac arrest: A randomised controlled trial. Resusc. Plus 2021, 5, 100082. [Google Scholar] [CrossRef] [PubMed]
- Abella, B.S.; Alvarado, J.P.; Myklebust, H.; Edelson, D.P.; Barry, A.; O’Hearn, N.; Hoek, T.L.V.; Becker, L.B. Quality of cardiopulmonary resuscitation during in-hospital cardiac arrest. JAMA 2005, 293, 305–310. [Google Scholar] [CrossRef]
- You, K.M.; Lee, C.; Kwon, W.Y.; Lee, J.C.; Suh, G.J.; Kim, K.S.; Park, M.J.; Kim, S. Real-time tidal volume feedback guides optimal ventilation during simulated CPR. Am. J. Emerg. Med. 2017, 35, 292–298. [Google Scholar] [CrossRef]
- Pirrallo, R.G.; Aufderheide, T.P.; Provo, T.A.; Lurie, K.G. Effect of an inspiratory impedance threshold device on hemodynamics during conventional manual cardiopulmonary resuscitation. Resuscitation 2005, 66, 13–20. [Google Scholar] [CrossRef]
- Thayne, R.C.; Thomas, D.C.; Neville, J.D.; Van Dellen, A. Use of an impedance threshold device improves short-term outcomes following out-of-hospital cardiac arrest. Resuscitation 2005, 67, 103–108. [Google Scholar] [CrossRef]
- Lurie, K.G.; Zielinski, T.; McKnite, S.; Aufderheide, T.; Voelckel, W. Use of an inspiratory impedance valve improves neurologically intact survival in a porcine model of ventricular fibrillation. Circulation 2002, 105, 124–129. [Google Scholar] [CrossRef]
- Parnia, S.; Yang, J.; Nguyen, R.; Ahn, A.; Zhu, J.; Inigo-Santiago, L. Cerebral oximetry during cardiac arrest: A multicenter study of neurologic outcomes and survival. Crit. Care Med. 2016, 44, 1663–1674. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Taccone, F.S.; He, X. Harmful effects of hyperoxia in postcardiac arrest, sepsis, traumatic brain injury, or stroke: The importance of individualized oxygen therapy in critically ill patients. Can. Respir. J. 2017, 2017, 2834956. [Google Scholar] [CrossRef]
- Bellomo, R.; Bailey, M.; Eastwood, G.M.; Nichol, A.; Pilcher, D.; Hart, G.K.; Reade, M.C.; Egi, M.; Cooper, J.D.; Group SoOiCC. Arterial hyperoxia and in-hospital mortality after resuscitation from cardiac arrest. Crit. Care 2011, 15, R90. [Google Scholar] [CrossRef]
- Rasooly, D.; Peloso, G.M. Two-Sample Multivariable Mendelian Randomization Analysis Using R. Curr. Protoc. 2021, 1, e335. [Google Scholar] [CrossRef]
- Sielski, J.; Kaziród-Wolski, K.; Siudak, Z. Out-of-hospital cardiac arrest: Data from the National Registry of Invasive Cardiology Procedures (ORPKI) in a long-term survival analysis of patients with acute coronary syndromes in a Polish region. Kardiol. Pol. 2020, 78, 412–419. [Google Scholar] [CrossRef]
- Merchant, R.M.; Topjian, A.A.; Panchal, A.R.; Cheng, A.; Aziz, K.; Berg, K.M.; Lavonas, E.J.; Magid, D.J.; Basic, A. Advanced Life Support PB. Part 1: Executive summary: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2020, 142, S337–S357. [Google Scholar] [CrossRef]
- Pemberton, K.; Franklin, R.C.; Bosley, E.; Watt, K. Pre-hospital predictors of long-term survival from out-of-hospital cardiac arrest. Australas. Emerg. Care 2023, 26, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Sielski, J.; Kaziród-Wolski, K.; Solnica, M.; Data, M.; Kukla, D.; Woźnica, K.; Sadowski, M. Age-related differences in the prehospital management of 2500 patients with sudden cardiac arrest. Arch. Med. Sci. 2021. [Google Scholar] [CrossRef]
- Hessulf, F.; Bhatt, D.L.; Engdahl, J.; Lundgren, P.; Omerovic, E.; Rawshani, A.; Helleryd, E.; Dworeck, C.; Friberg, H.; Redfors, B.; et al. Predicting survival and neurological outcome in out-of-hospital cardiac arrest using machine learning: The SCARS model. EBioMedicine 2023, 89, 104464. [Google Scholar] [CrossRef] [PubMed]
- LA Via, L.; Astuto, M.; Bignami, E.G.; Busalacchi, D.; Dezio, V.; Girardis, M.; Lanzafame, B.; Ristagno, G.; Pelosi, P.; Sanfilippo, F. The effects of exposure to severe hyperoxemia on neurological outcome and mortality after cardiac arrest. Minerva Anestesiol. 2022, 88, 853–863. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Badenes, R.; Battaglini, D.; Ball, L.; Sanfilippo, F.; Brunetti, I. Oxygen targets and 6-month outcome after out of hospital cardiac arrest: A pre-planned sub-analysis of the targeted hypothermia versus targeted normothermia after Out-of-Hospital Cardiac Arrest (TTM2) trial. Crit. Care 2022, 26, 323. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (N = 121) | AVF Group (N = 63) | NVF Group (N = 58) | p-Value |
|---|---|---|---|---|
| Age (years) | 70.36 ± 15.68 | 68.87 ± 15.01 | 70.98 ± 15.94 | 0.213 |
| Gender | ||||
| Male | 68 (56.1) | 37 (58.3) | 31 (53.4) | 0.051 |
| Female | 53 (43.9) | 24 (41.7) | 27 (46.6) | 0.111 |
| Arrest location | 0.101 | |||
| Public area | 73 (60.3) | 43 (68.2) | 30 (51.7) | 0.012 |
| Non-public area | 48 (39.7) | 20 (31.8) | 28 (48.3) | 0.042 |
| Apply TTM | 51 (42.1) | 29 (46.0) | 22 (37.9) | 0.123 |
| Time to CPR by bystander (min) | 9.4 ± 3.43 | 6.5 ± 2.11 | 6.9 ± 2.88 | 0.981 |
| CPR duration (min) | 34.1 ± 11.23 | 39.4 ± 12.89 | 37.2 ± 10.21 | 0.126 |
| Time from collapse to visit ED | ||||
| Witness collapse, yes | 31 (25.6) | 17 (26.9) | 14 (24.1) | 0.323 |
| Bystander CPR, yes | 13 (10.7) | 7 (11.1) | 6 (10.3) | 0.332 |
| ROSC within 30 min | 69 (57.0) | 43 (68.2) | 26 (44.8)) | 0.031 |
| ROSC (%) yes | 58 (47.9) | 35 (55.5) | 21 (36.2) | 0.041 |
| Outcome | ||||
| Survival in 80 days | 49 (40.4) | 21 (33.3) | 13 (22.4) | 0.232 |
| Survival at 30 h | 59 (48.7) | 31 (49.2) | 27 (46.5) | 0.001 |
| Survival discharge | 12 (9.9) | 6 (4.9) | 5 (8.6) | 0.543 |
| Death | 67 (55.3) | 31 (49.2) | 34 (58.6) | 0.654 |
| Survival good outcome (CPC 1–2) | 13 (10.7) | 7 (11.1) | 6 (10.3) | 0.766 |
| Outcome | Adjust OR | |
|---|---|---|
| OR (95% CI) | p | |
| ROSC within 30 min | 0.56 (0.37–1.85) | 0.001 |
| Survival in 80 days | 0.66 (0.25–0.87) | 0.82 |
| Survival at 30 h | 0.53 (0.31–1.93) | 0.03 |
| Survival to hospital discharge | 0.84 (0.39–0.83) | 0.67 |
| Good neurologic outcome (CPC 1–2) | 0.68 (0.28–0.91) | 0.73 |
| Covariate | b | SE | Wald | OR (95% CI) | p |
|---|---|---|---|---|---|
| AVF group | 0.2121 | 0.0822 | 2.1021 | 0.7731–1.2439 | 0.0380 |
| NVF group | 0.3563 | 0.1952 | 3.3311 | 0.9740–2.0937 | 0.0675 |
| VF | HR | 95% CI | p |
|---|---|---|---|
| AVF group | 0.9769 | 0.4591–2.2825 | 0.3180 |
| NVF group | 1.0237 | 0.4381–2.1781 | 0.0675 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.D.; Jang, Y.D.; Kang, J.H.; Seo, Y.S.; Yoon, Y.S.; Kim, Y.W.; Jeong, W.B.; Ji, J.G. Effect of a Real-Time Audio Ventilation Feedback Device on the Survival Rate and Outcomes of Patients with Out-of-Hospital Cardiac Arrest: A Prospective Randomized Controlled Study. J. Clin. Med. 2023, 12, 6023. https://doi.org/10.3390/jcm12186023
Lee ED, Jang YD, Kang JH, Seo YS, Yoon YS, Kim YW, Jeong WB, Ji JG. Effect of a Real-Time Audio Ventilation Feedback Device on the Survival Rate and Outcomes of Patients with Out-of-Hospital Cardiac Arrest: A Prospective Randomized Controlled Study. Journal of Clinical Medicine. 2023; 12(18):6023. https://doi.org/10.3390/jcm12186023
Chicago/Turabian StyleLee, Eun Dong, Yun Deok Jang, Ji Hun Kang, Yong Song Seo, Yoo Sang Yoon, Yang Weon Kim, Woong Bin Jeong, and Jae Gu Ji. 2023. "Effect of a Real-Time Audio Ventilation Feedback Device on the Survival Rate and Outcomes of Patients with Out-of-Hospital Cardiac Arrest: A Prospective Randomized Controlled Study" Journal of Clinical Medicine 12, no. 18: 6023. https://doi.org/10.3390/jcm12186023
APA StyleLee, E. D., Jang, Y. D., Kang, J. H., Seo, Y. S., Yoon, Y. S., Kim, Y. W., Jeong, W. B., & Ji, J. G. (2023). Effect of a Real-Time Audio Ventilation Feedback Device on the Survival Rate and Outcomes of Patients with Out-of-Hospital Cardiac Arrest: A Prospective Randomized Controlled Study. Journal of Clinical Medicine, 12(18), 6023. https://doi.org/10.3390/jcm12186023