
Hyperphagia, Growth, and Puberty in Children with Angelman Syndrome

 , , , , and
, , , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics at Most Recent Visit
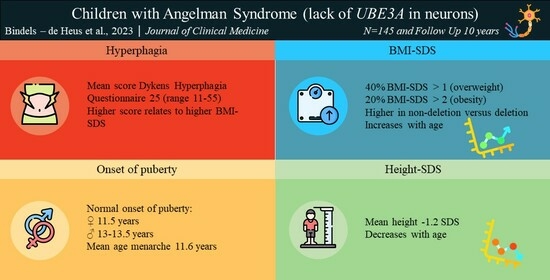
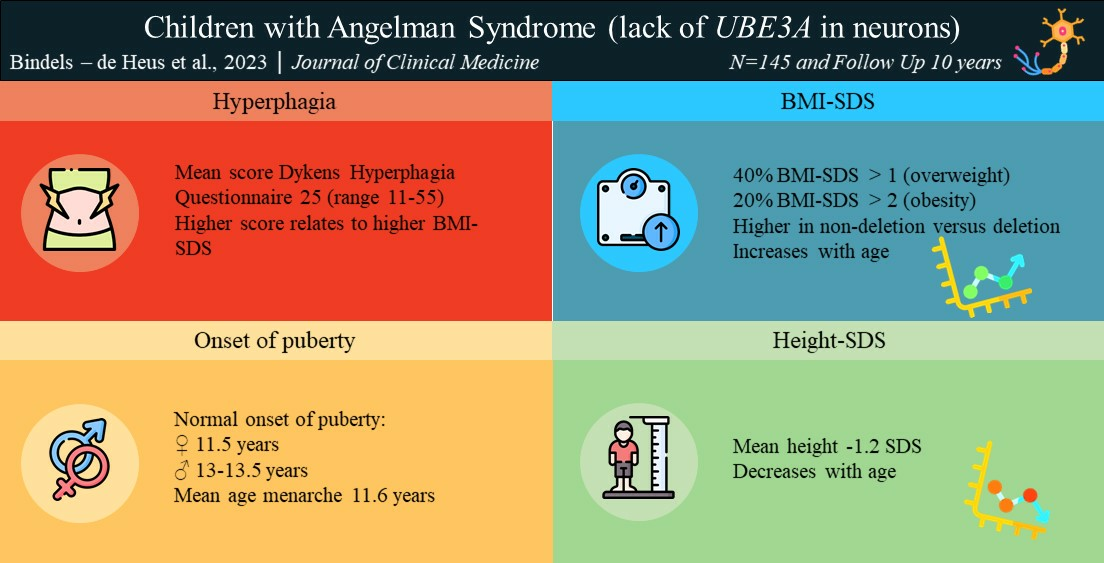
3.2. Hyperphagia
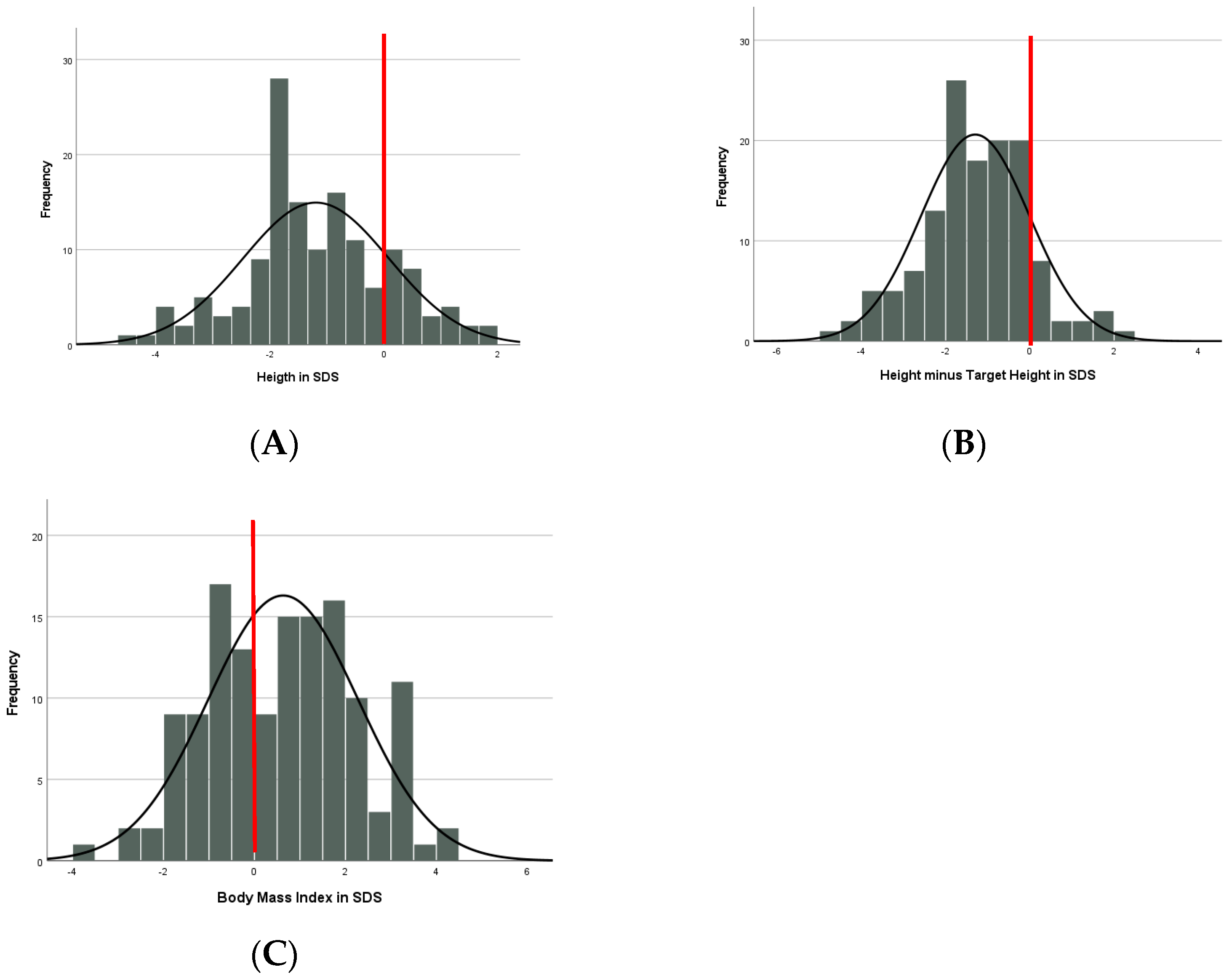
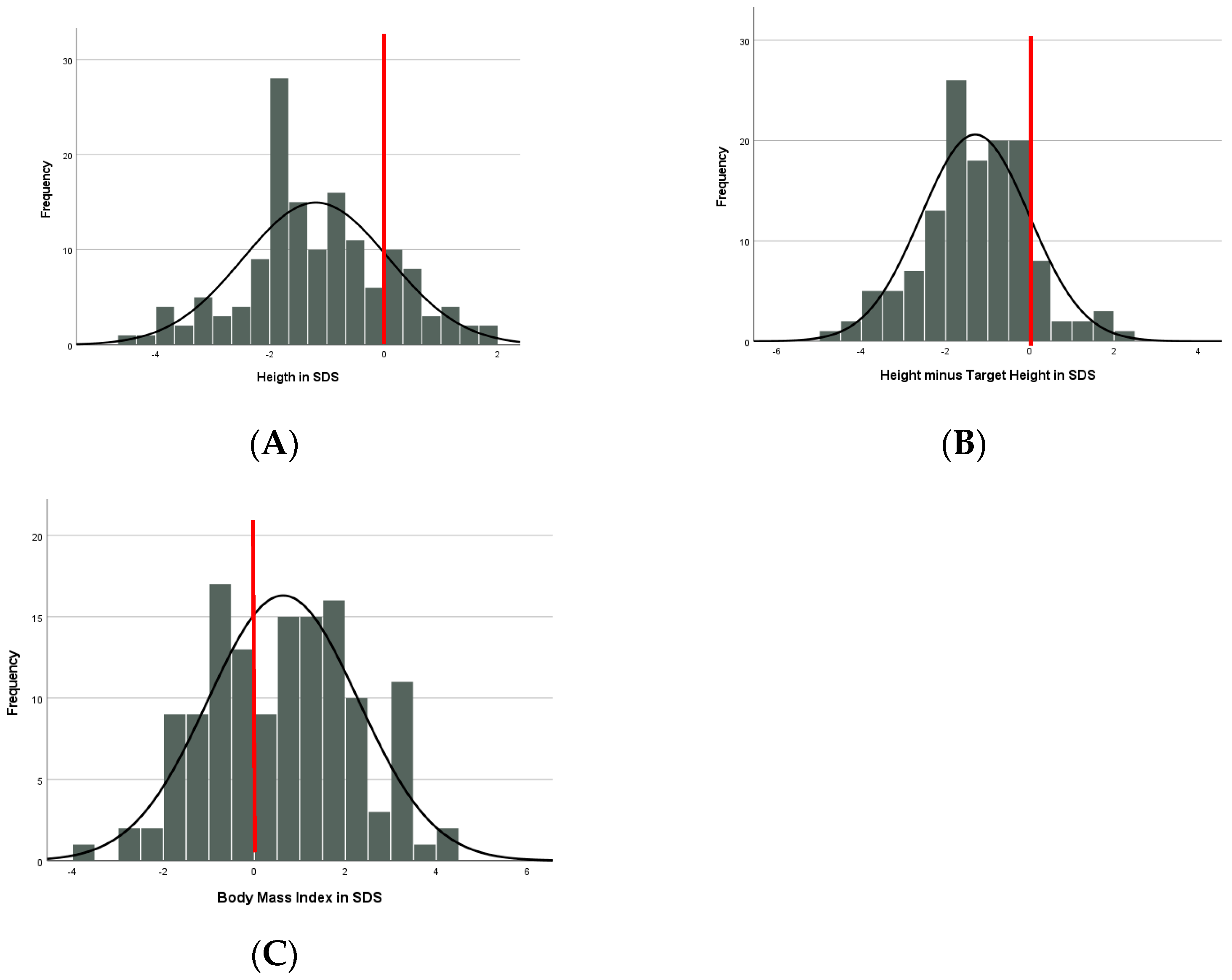
3.3. Growth: Cross-Sectional Results
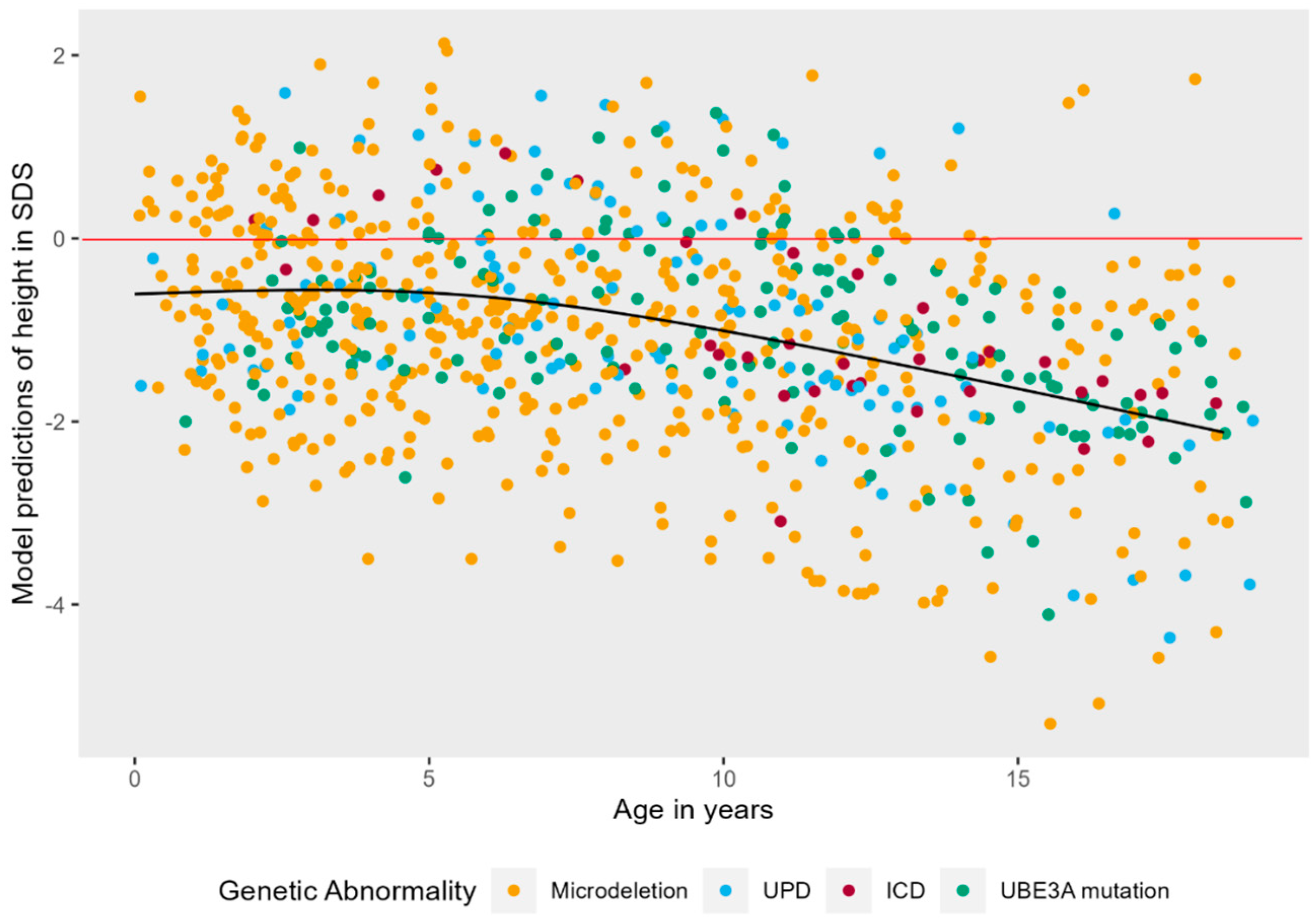
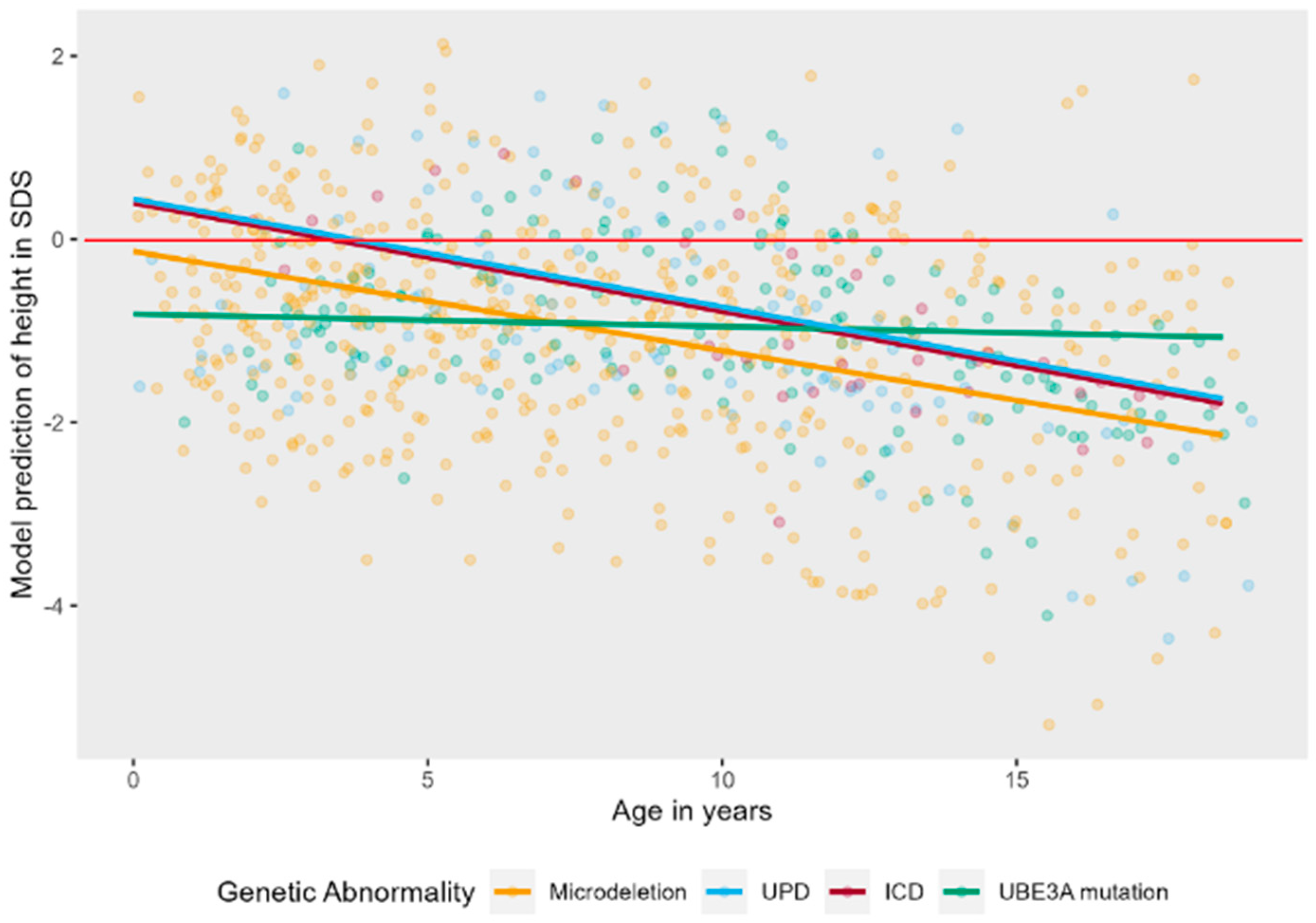
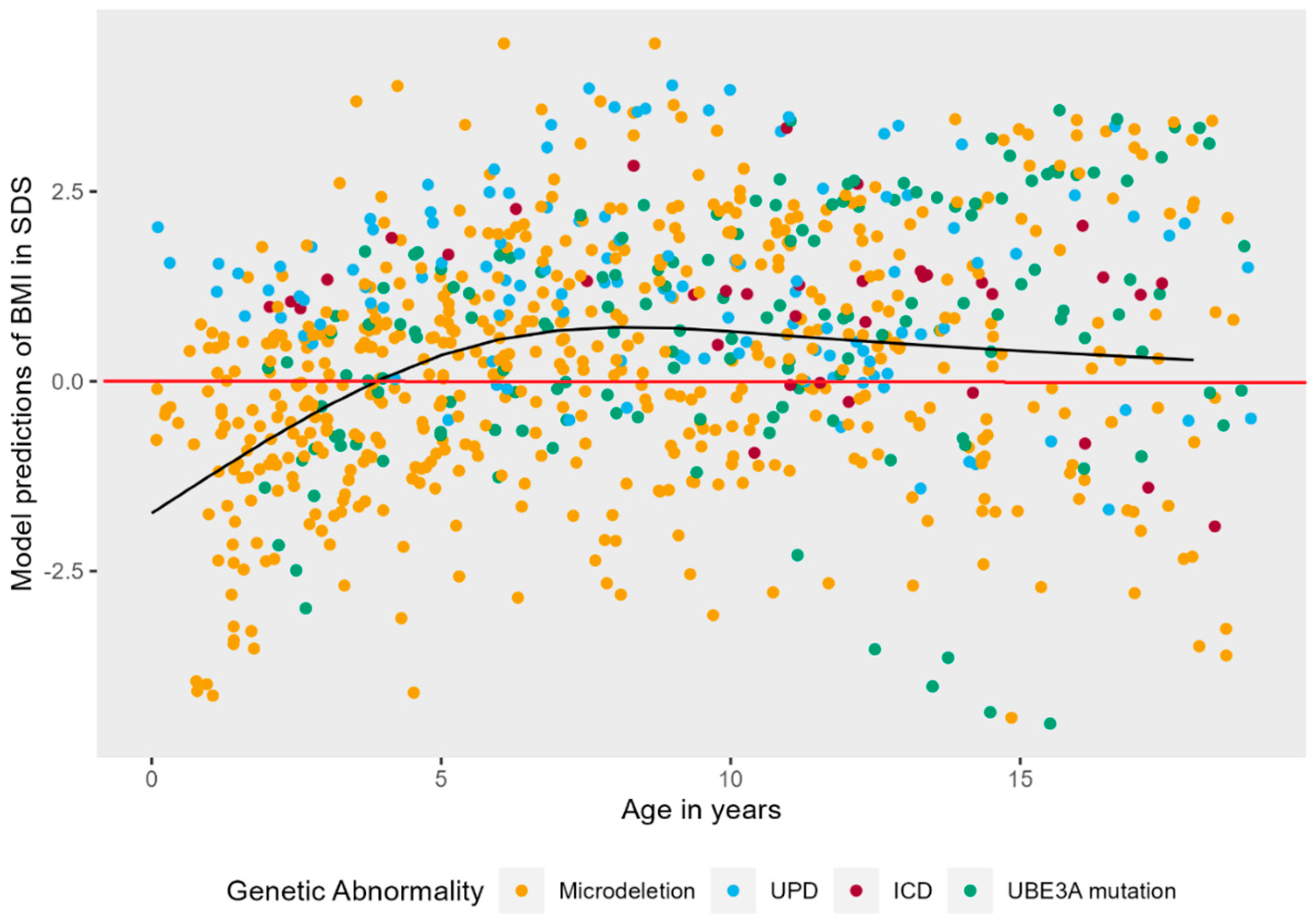
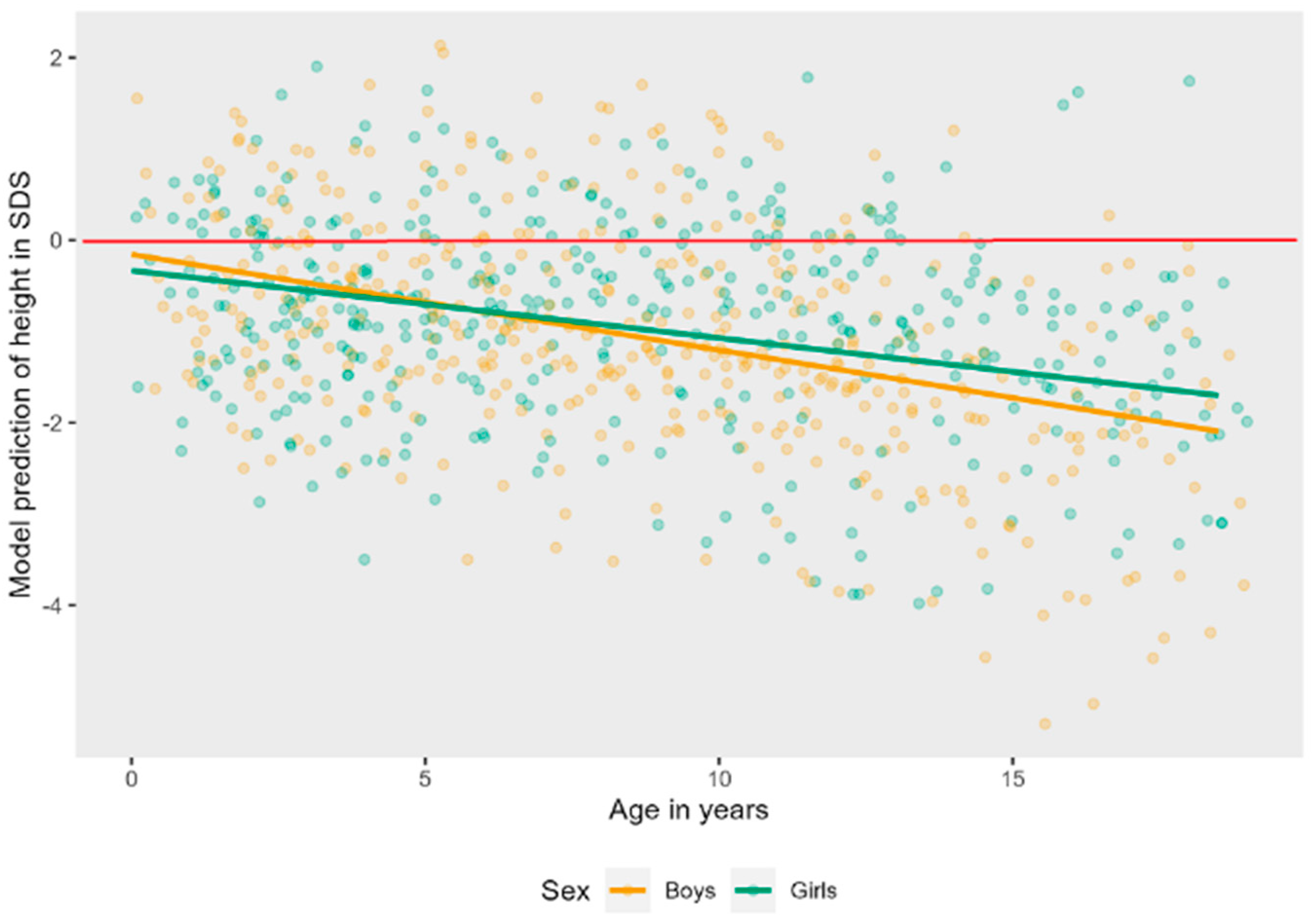
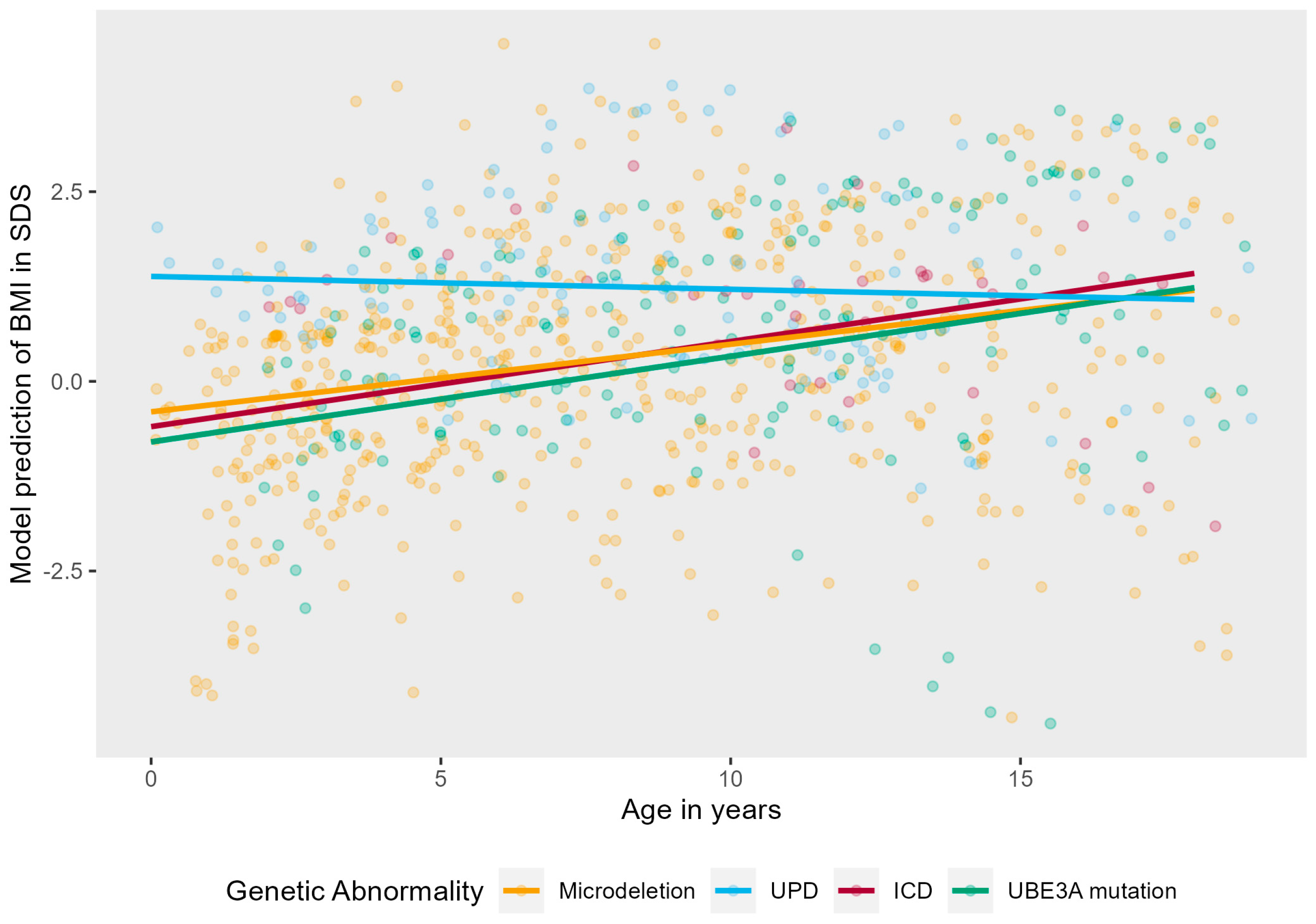
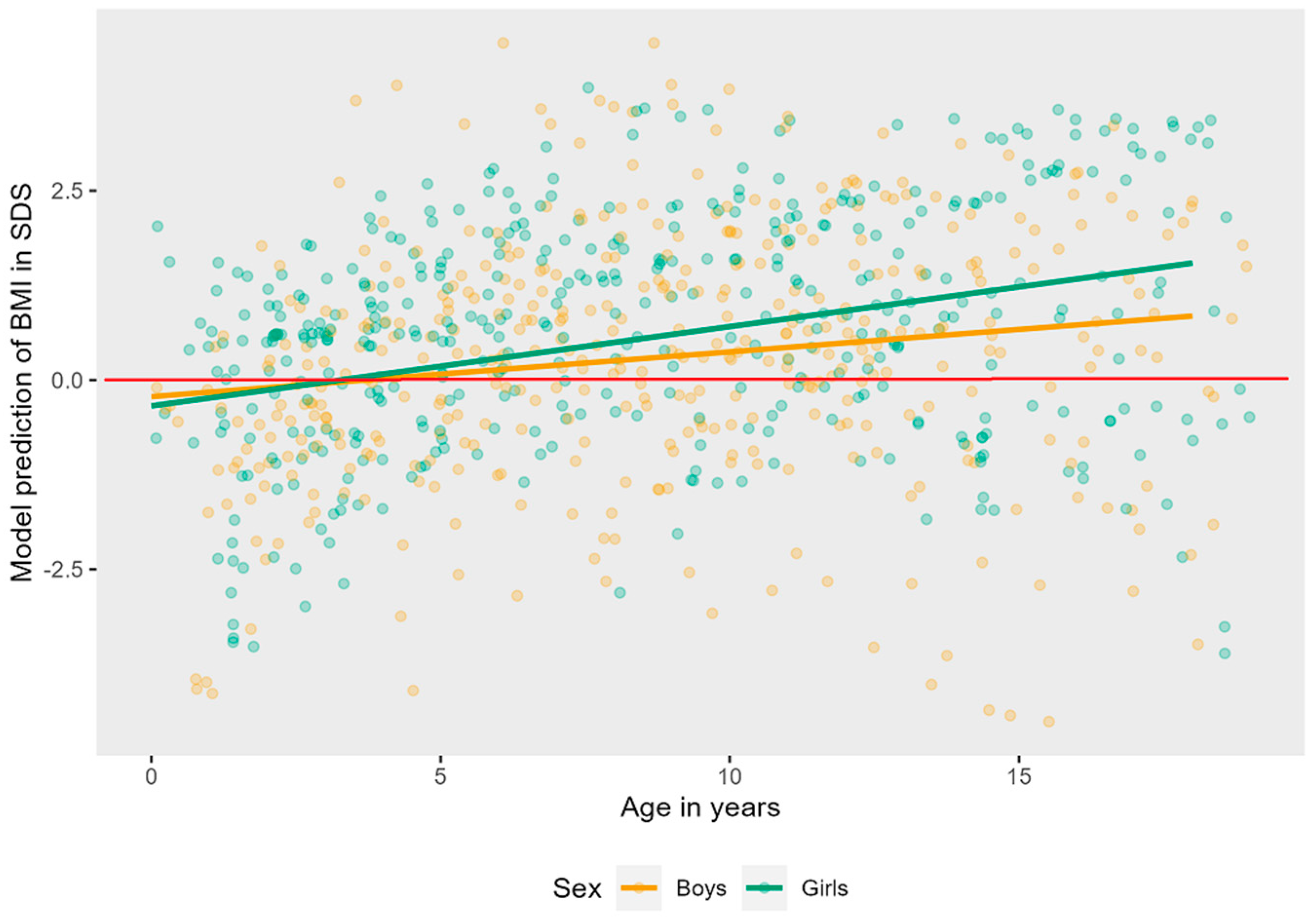
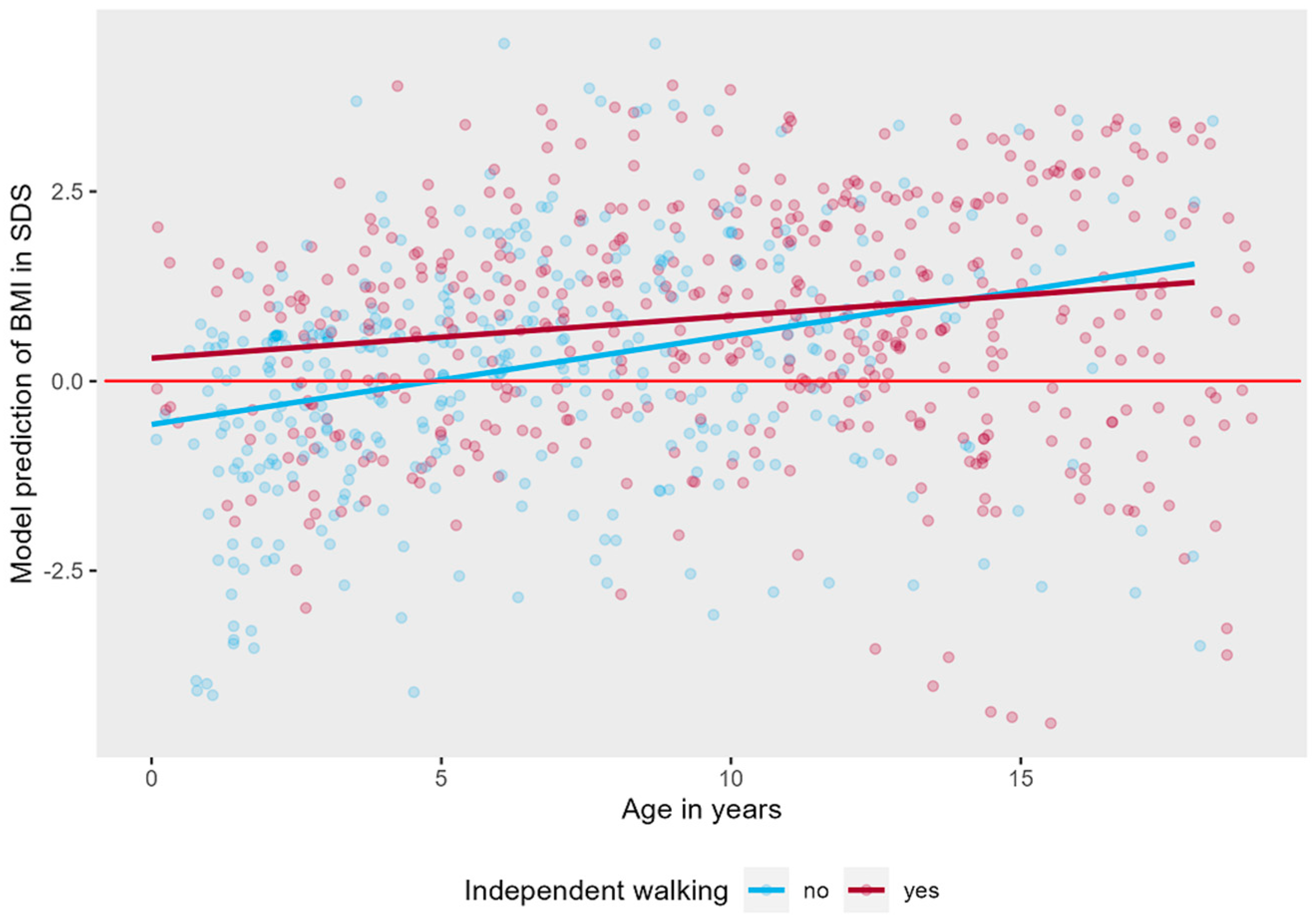
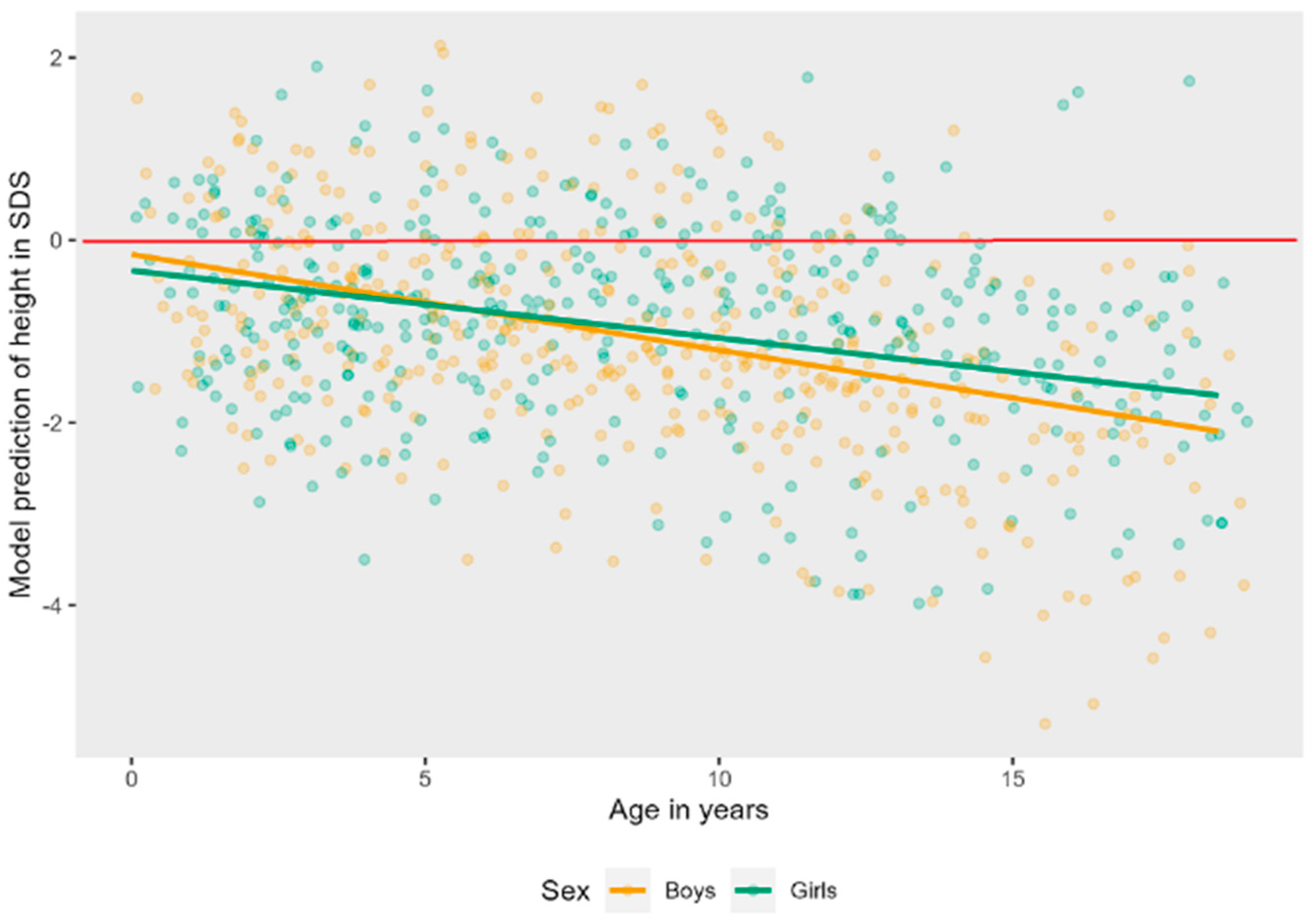
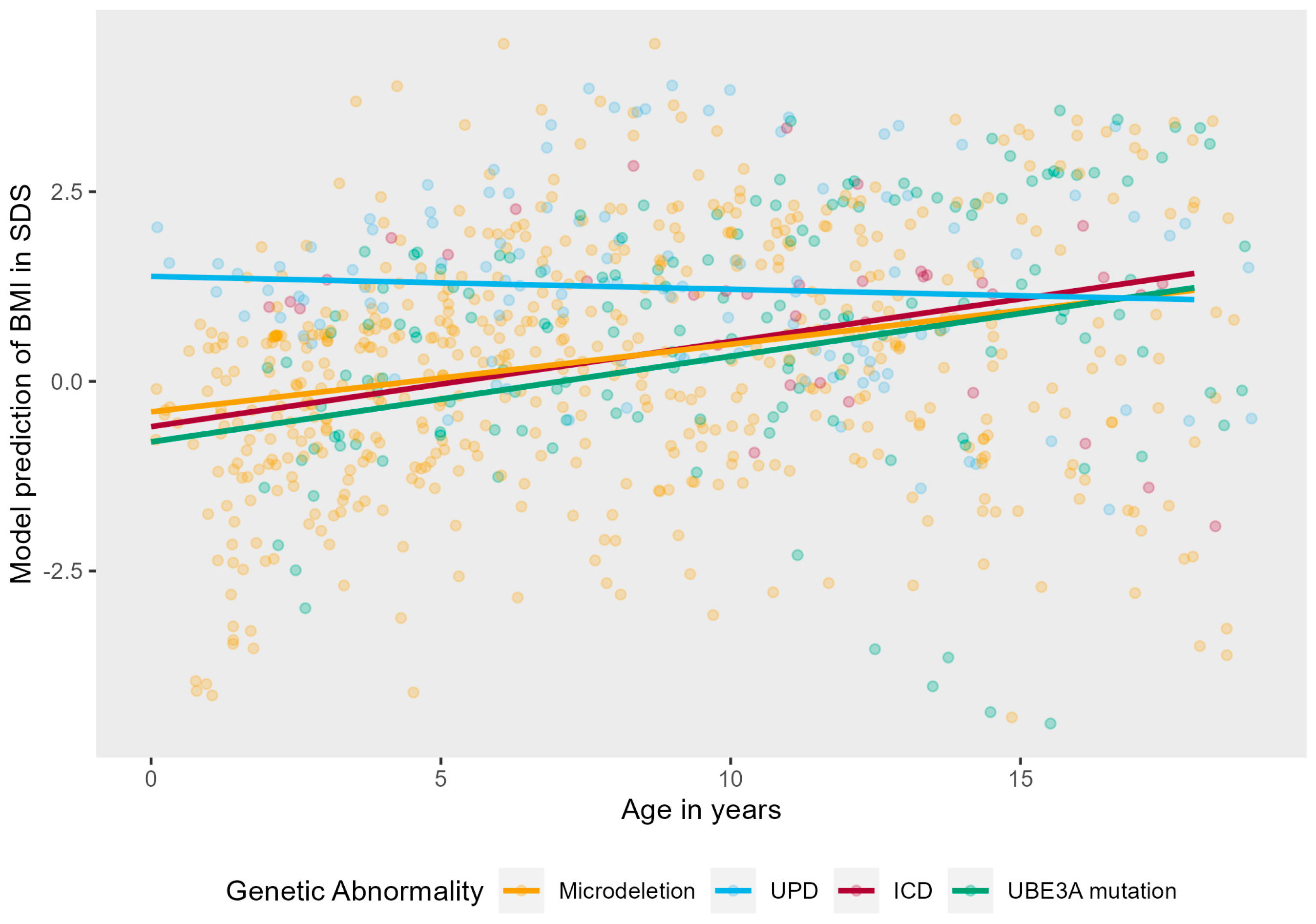
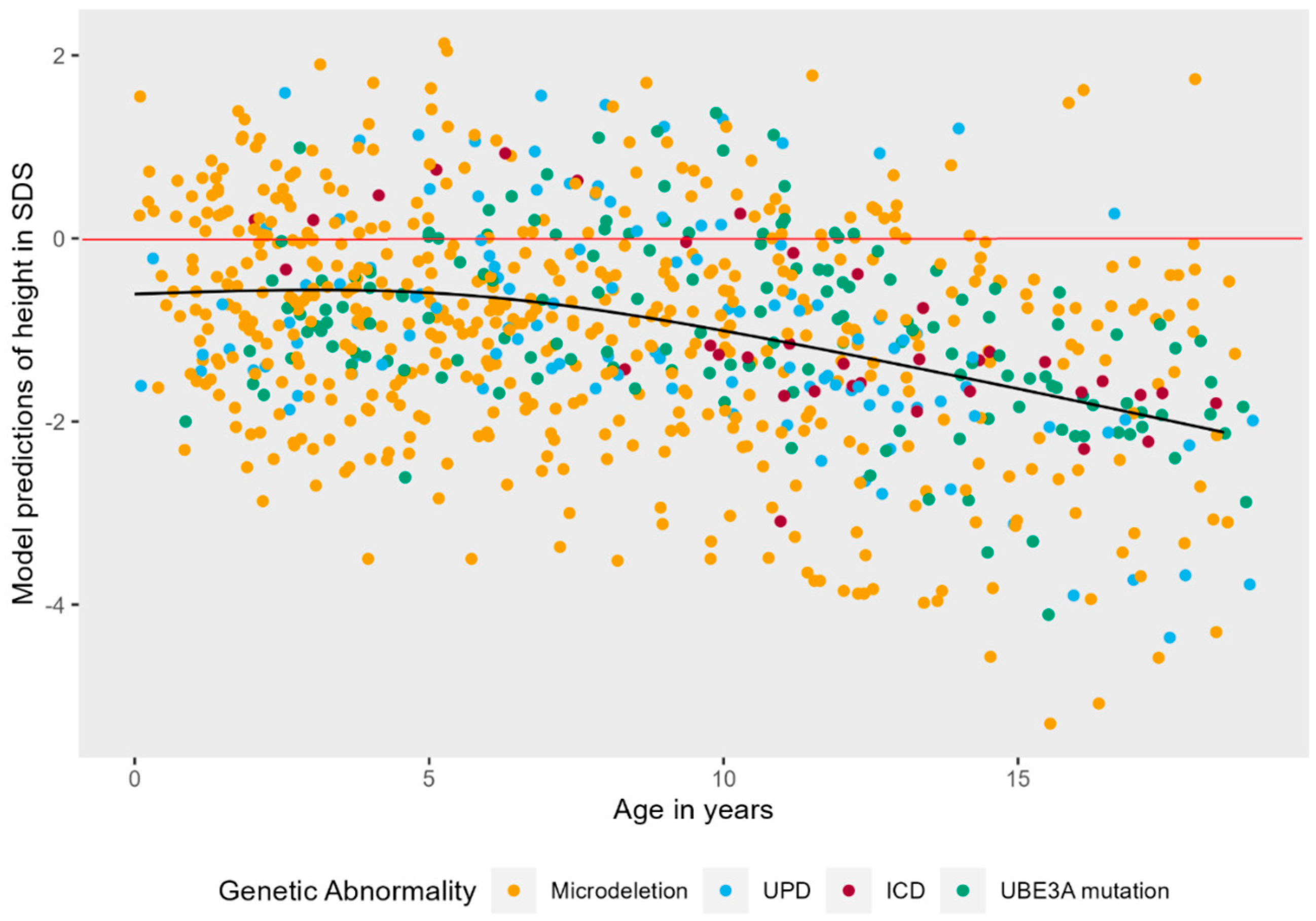
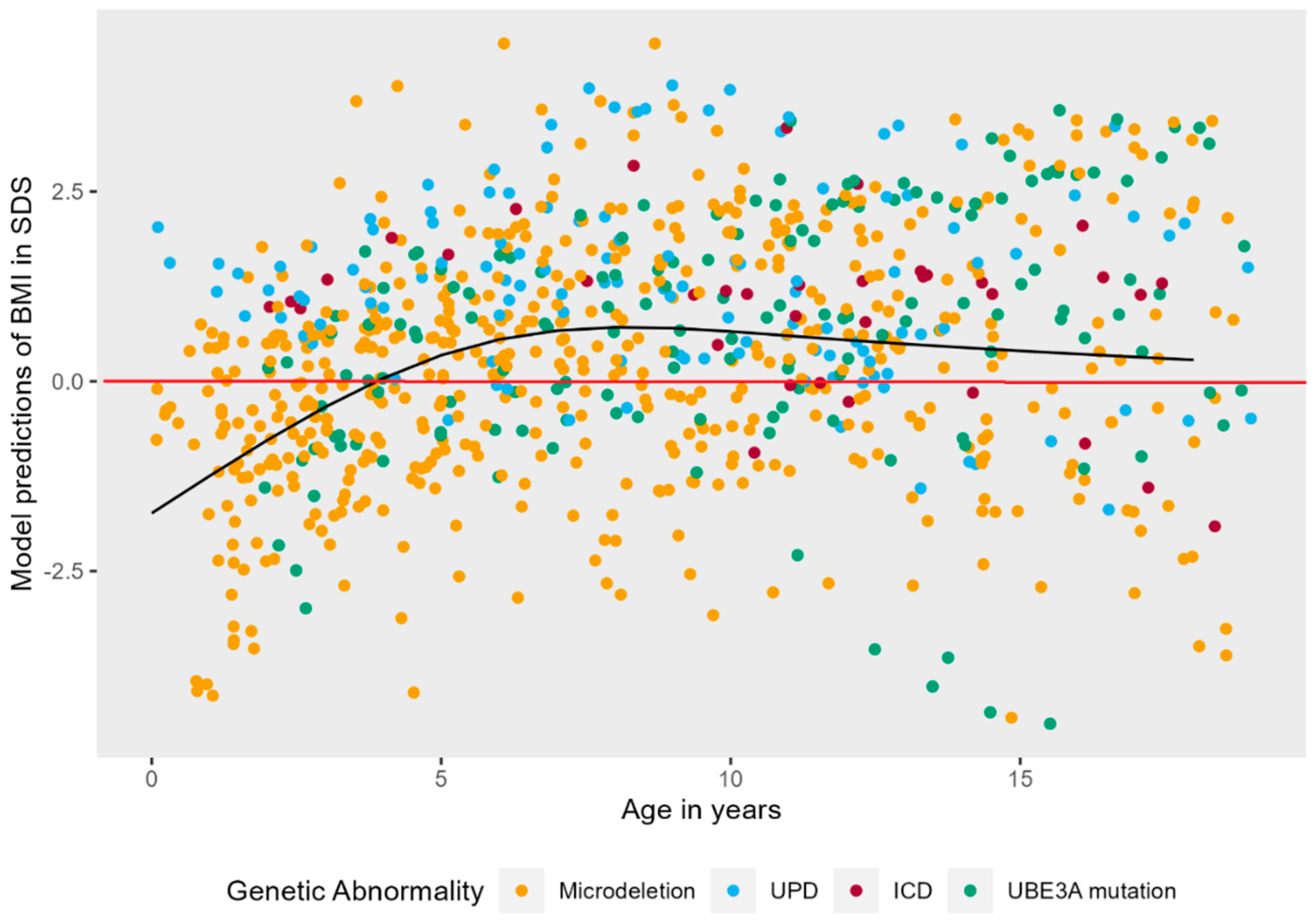
3.4. Growth: Longitudinal Results
3.5. Puberty
3.6. Tube Feeding
4. Discussion
4.1. Hyperphagia
4.2. Growth
4.3. Puberty
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | Mean | SD | |
|---|---|---|---|
| 1. How upset does your child generally become when denied a desired food? | 53 | 2.75 | 1.21 |
| 2. How often does your child try to bargain or manipulate to get more food at meals? | 53 | 3.19 | 1.70 |
| 3. Once your child has food on their mind, how easy is it for you or others to re-direct your child away from food to other things? | 53 | 2.96 | 1.34 |
| 4. How often does your child forage through the trash for food? | 53 | 1.30 | 0.91 |
| 5. How often does your child get up at night to food seek? | 53 | 1.10 | 0.49 |
| 6. How persistent is your child in asking or looking for food after being told “no” or “no more”? | 53 | 2.63 | 1.22 |
| 7. Outside of normal meal times, how much time does your child spend talking about food or engaged in food-related behaviors? | 53 | 1.75 | 1.13 |
| 8. How often does your child try to steal food (that you are aware of?) | 53 | 2.76 | 1.64 |
| 9. When others try to stop your child from talking about food or engaging in food-related behaviors, does it leads to distress or being upset? | 53 | 1.81 | 1.11 |
| 10. How clever or fast is your child in obtaining food? | 53 | 3.13 | 1.39 |
| 11. To what extent to food-related thoughts, talk, or behavior interfere with your child’s normal daily routines, self-care, school, or work? | 53 | 1.64 | 0.94 |


| Girls (N (%)) | Boys (N (%)) | Total (N (%)) | |
|---|---|---|---|
| Prepubertal | 27 (40.3) | 32 (41.0) | 59 (40.7) |
| Early | 3 (4.5) | - | 3 (2.1) |
| Normal | 33 (49.2) | 38 (48.7) | 71 (49.0) |
| Late | 4 (6.0) | 8 (10.3) | 12 (8.3) |
| Total | 67 | 78 | 145 |
| Total Score (11–55) | Behavior (5–25) | Drive (4–20) | Severity (2–10) | |
|---|---|---|---|---|
| AS (this study) N = 53 | 25.1 (9.0) | 11.5 (4.4) | 10.2 (3.9) | 3.4 (1.8) |
| AS (Mertz, 2014 [9]) N = 39 # | 21.8 | 10.0 | 8.7 | 3.1 |
| PWS (Dykens, 2007 [12]) N = 153 | 27.9 | 13.6 (4.5) | 12.3 (3.3) | 4.6 (1.6) |
| PWS (Zorn, 2022 [11]) N = 649 * | 27.0 | |||
| BBS (Zorn, 2022 [11]) N= 13 | 27.6 (9.0) | 12.5 (4.1) | 11.2 (4.1) | 3.8 (1.5) |
| LEPR (Zorn, 2022 [11]) N = 8 | 32.0 (9.3) | 13.4 (3.9) | ||
| MC4R (Zorn, 2022 [11]) N = 7 | 31.4 (5.4) | 11.9 (2.3) | ||
| Alström (Zorn, 2022 [11]) N = 23 | 27 (13) | - | - | - |
| 16p11.2del (Zorn, 2022 [11]) N = 5 | 21.4 (5.5) | 8.8 (2.2) | 10.0 (3.1) | 2.6 (0.9) |
References
- Williams, C.A.; Beaudet, A.L.; Clayton-Smith, J.; Knoll, J.H.; Kyllerman, M.; Laan, L.A.; Magenis, R.E.; Moncla, A.; Schinzel, A.A.; Summers, J.A.; et al. Angelman syndrome 2005: Updated consensus for diagnostic criteria. Am. J. Med. Genet. A 2006, 140, 413–418. [Google Scholar] [CrossRef]
- Bindels-de Heus, K.; Mous, S.E.; Ten Hooven-Radstaake, M.; van Iperen-Kolk, B.M.; Navis, C.; Rietman, A.B.; Ten Hoopen, L.W.; Brooks, A.S.; Encore Expertise Center for AS; Elgersma, Y.; et al. An overview of health issues and development in a large clinical cohort of children with Angelman syndrome. Am. J. Med. Genet. A 2020, 182, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Mertz, L.G.; Christensen, R.; Vogel, I.; Hertz, J.M.; Nielsen, K.B.; Gronskov, K.; Ostergaard, J.R. Angelman syndrome in Denmark. birth incidence, genetic findings, and age at diagnosis. Am. J. Med. Genet. A 2013, 161A, 2197–2203. [Google Scholar] [CrossRef]
- Kishino, T.; Lalande, M.; Wagstaff, J. UBE3A/E6-AP mutations cause Angelman syndrome. Nat. Genet. 1997, 15, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Beygo, J.; Buiting, K.; Ramsden, S.C.; Ellis, R.; Clayton-Smith, J.; Kanber, D. Update of the EMQN/ACGS best practice guidelines for molecular analysis of Prader-Willi and Angelman syndromes. Eur. J. Hum. Genet. 2019, 27, 1326–1340. [Google Scholar] [CrossRef] [PubMed]
- Lossie, A.C.; Whitney, M.M.; Amidon, D.; Dong, H.J.; Chen, P.; Theriaque, D.; Hutson, A.; Nicholls, R.D.; Zori, R.T.; Williams, C.A.; et al. Distinct phenotypes distinguish the molecular classes of Angelman syndrome. J. Med. Genet. 2001, 38, 834–845. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.H.; Bacino, C.A.; Skinner, S.A.; Anselm, I.; Barbieri-Welge, R.; Bauer-Carlin, A.; Beaudet, A.L.; Bichell, T.J.; Gentile, J.K.; Glaze, D.G.; et al. Angelman syndrome: Mutations influence features in early childhood. Am. J. Med. Genet. A 2011, 155A, 81–90. [Google Scholar] [CrossRef]
- Brennan, M.L.; Adam, M.P.; Seaver, L.H.; Myers, A.; Schelley, S.; Zadeh, N.; Hudgins, L.; Bernstein, J.A. Increased body mass in infancy and early toddlerhood in Angelman syndrome patients with uniparental disomy and imprinting center defects. Am. J. Med. Genet. A 2015, 167A, 142–146. [Google Scholar] [CrossRef]
- Mertz, L.G.; Christensen, R.; Vogel, I.; Hertz, J.M.; Ostergaard, J.R. Eating behavior, prenatal and postnatal growth in Angelman syndrome. Res. Dev. Disabil. 2014, 35, 2681–2690. [Google Scholar] [CrossRef]
- Welham, A.; Lau, J.; Moss, J.; Cullen, J.; Higgs, S.; Warren, G.; Wilde, L.; Marr, A.; Cook, F.; Oliver, C. Are Angelman and Prader-Willi syndromes more similar than we thought? Food-related behavior problems in Angelman, Cornelia de Lange, fragile X, Prader-Willi and 1p36 deletion syndromes. Am. J. Med. Genet. A 2015, 167A, 572–578. [Google Scholar] [CrossRef]
- Zorn, S.; Schnurbein, J.; Schirmer, M.; Brandt, S.; Wabitsch, M. Measuring hyperphagia in patients with monogenic and syndromic obesity. Appetite 2022, 178, 106161. [Google Scholar] [CrossRef] [PubMed]
- Dykens, E.M.; Maxwell, M.A.; Pantino, E.; Kossler, R.; Roof, E. Assessment of hyperphagia in Prader-Willi syndrome. Obesity 2007, 15, 1816–1826. [Google Scholar] [CrossRef] [PubMed]
- Lister, N.B.; Baur, L.A.; Felix, J.F.; Hill, A.J.; Marcus, C.; Reinehr, T.; Summerbell, C.; Wabitsch, M. Child and adolescent obesity. Nat. Rev. Dis. Prim. 2023, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- TNO Groeidiagrammen. 2022. Available online: https://www.tno.nl/nl/gezond/werk-jeugd-gezondheid/jeugd/eerste-1000-dagen-kind/groeidiagrammen-groeicalculators/ (accessed on 5 April 2021).
- Schundeln, M.M.; Marschke, L.; Bauer, J.J.; Hauffa, P.K.; Schweiger, B.; Fuhrer-Sakel, D.; Lahner, H.; Poeppel, T.D.; Kiewert, C.; Hauffa, B.P.; et al. A Piece of the Puzzle: The Bone Health Index of the BoneXpert Software Reflects Cortical Bone Mineral Density in Pediatric and Adolescent Patients. PLoS ONE 2016, 11, e0151936. [Google Scholar] [CrossRef] [PubMed]
- IBM. IBM SPSS Statistics for Windows, Version 25.0; IBM: Armonk, NY, USA, 2017.
- R. Core Team. R: A Language and Environment for Statistical Computing; R. Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 19 January 2023).
- Bates, D.; Maechler, M.; Bolker, B.M.; Walker, S.C. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Ma, V.K.; Mao, R.; Toth, J.N.; Fulmer, M.L.; Egense, A.S.; Shankar, S.P. Prader-Willi and Angelman Syndromes: Mechanisms and Management. Appl. Clin. Genet. 2023, 16, 41–52. [Google Scholar]
- Freitas, A.; Albuquerque, G.; Silva, C.; Oliveira, A. Appetite-Related Eating Behaviours: An Overview of Assessment Methods, Determinants and Effects on Children’s Weight. Ann. Nutr. Metab. 2018, 73, 19–29. [Google Scholar] [CrossRef]
- de Assis, L.V.M.; Oster, H. The circadian clock and metabolic homeostasis: Entangled networks. Cell. Mol. Life Sci. 2021, 78, 4563–4587. [Google Scholar] [CrossRef]
- Andermann, M.L.; Lowell, B.B. Toward a Wiring Diagram Understanding of Appetite Control. Neuron 2017, 95, 757–778. [Google Scholar] [CrossRef]
- Murray, S.; Tulloch, A.; Gold, M.S.; Avena, N.M. Hormonal and neural mechanisms of food reward, eating behaviour and obesity. Nat. Rev. Endocrinol. 2014, 10, 540–552. [Google Scholar] [CrossRef]
- Shi, S.Q.; Bichell, T.J.; Ihrie, R.A.; Johnson, C.H. Ube3a imprinting impairs circadian robustness in Angelman syndrome models. Curr. Biol. 2015, 25, 537–545. [Google Scholar] [CrossRef]
- Kolbe, I.; Leinweber, B.; Brandenburger, M.; Oster, H. Circadian clock network desynchrony promotes weight gain and alters glucose homeostasis in mice. Mol. Metab. 2019, 30, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Bindels-de Heus, K.G.C.B.; Hooven-Radstaake, M.T.; Legerstee, J.S.; Hoopen, L.W.T.; Encore Expertisecenter for AS; Dieleman, G.C.; Moll, H.A.; Mous, S.E.; de Wit, M.Y. Sleep problems in children with Angelman Syndrome: The effect of a behavioral intervention program. Res. Dev. Disabil. 2023, 135, 104444. [Google Scholar] [CrossRef] [PubMed]
- Viho, E.M.G.; Punt, M.; Distel, B.; Houtman, R.; Kroon, J.; Elgersma, Y.; Meijer, O.C. The Hippocampal Response to Acute Corticosterone Elevation Is Altered in a Mouse Model for Angelman Syndrome. Int. J. Mol. Sci. 2022, 24, 303. [Google Scholar] [CrossRef]
- Heald, M.; Adams, D.; Oliver, C. Profiles of atypical sensory processing in Angelman, Cornelia de Lange and Fragile X syndromes. J. Intellect. Disabil. Res. 2020, 64, 117–130. [Google Scholar] [CrossRef]
- Miller, J.L.; Lynn, C.H.; Driscoll, D.C.; Goldstone, A.P.; Gold, J.A.; Kimonis, V.; Dykens, E.; Butler, M.G.; Shuster, J.J.; Driscoll, D.J. Nutritional Phases in Prader-Willi Syndrome. Am. J. Med. Genet. Part A 2011, 155a, 1040–1049. [Google Scholar] [CrossRef]
- Fan, H.C.; Wang, S.Y.; Peng, Y.J.; Lee, H.S. Valproic Acid Impacts the Growth of Growth Plate Chondrocytes. Int. J. Environ. Res. Public Health 2020, 17, 3675. [Google Scholar] [CrossRef] [PubMed]
- CBS. Centraal Bureau Voor Statistiek. 2021. Available online: https://www.cbs.nl/nl-nl/cijfers/detail/81565NED?q=gewicht%20kinderen (accessed on 26 July 2023).
- den Besten, I.; Jong, R.F.; Geerts-Haages, A.; Bruggenwirth, H.T.; Koopmans, M.; Encore Expertise Center for AS; Brooks, A.; Elgersma, Y.; Festen, D.A.M.; Valstar, M.J. Clinical aspects of a large group of adults with Angelman syndrome. Am. J. Med. Genet. A 2021, 185, 168–181. [Google Scholar] [CrossRef]
- Lopez, S.J.; Segal, D.J.; LaSalle, J.M. UBE3A: An E3 Ubiquitin Ligase with Genome-Wide Impact in Neurodevelopmental Disease. Front. Mol. Neurosci. 2018, 11, 476. [Google Scholar] [CrossRef]
- van Woerden, G.M.; Harris, K.D.; Hojjati, M.R.; Gustin, R.M.; Qiu, S.; de Avila Freire, R.; Jiang, Y.H.; Elgersma, Y.; Weeber, E.J. Rescue of neurological deficits in a mouse model for Angelman syndrome by reduction of alphaCaMKII inhibitory phosphorylation. Nat. Neurosci. 2007, 10, 280–282. [Google Scholar] [CrossRef]
- Alsaif, M.; Elliot, S.A.; MacKenzie, M.L.; Prado, C.M.; Field, C.J.; Haqq, A.M. Energy Metabolism Profile in Individuals with Prader-Willi Syndrome and Implications for Clinical Management: A Systematic Review. Adv. Nutr. 2017, 8, 905–915. [Google Scholar] [CrossRef]
- Fisher, K.; Keng, J.; Ziegler, J. Nutrition Assessment and Intervention in a Pediatric Patient with Angelman Syndrome: A Case Presentation Highlighting Clinical Challenges and Evidence-Based Solutions. Lifestyle Genom. 2020, 13, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Duis, J.; Nespeca, M.; Summers, J.; Bird, L.; Bindels-de Heus, K.G.C.B.; Valstar, M.J.; de Wit, M.Y.; Navis, C.; Ten Hooven-Radstaake, M.; van Iperen-Kolk, B.M.; et al. A multidisciplinary approach and consensus statement to establish standards of care for Angelman syndrome. Mol. Genet. Genomic Med. 2022, 10, e1843. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.; Grocott, O.; Parkin, K.; Larson, A.; Thibert, R.L. Angelman syndrome in adolescence and adulthood: A retrospective chart review of 53 cases. Am. J. Med. Genet. A 2018, 176, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Brix, N.; Ernst, A.; Lauridsen, L.L.B.; Parner, E.; Stovring, H.; Olsen, J.; Henriksen, T.B.; Ramlau-Hansen, C.H. Timing of puberty in boys and girls: A population-based study. Paediatr. Perinat. Epidemiol. 2019, 33, 70–78. [Google Scholar] [CrossRef]
- Wood, C.L.; Lane, L.C.; Cheetham, T. Puberty: Normal physiology (brief overview). Best. Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101265. [Google Scholar] [CrossRef]
- Lengtegroei. 2019. Available online: https://www.jgzrichtlijnen.nl/alle-richtlijnen/richtlijn/?richtlijn=48&rlpag=2775 (accessed on 26 July 2023).
- Lawaetz, J.G.; Hagen, C.P.; Mieritz, M.G.; Blomberg Jensen, M.; Petersen, J.H.; Juul, A. Evaluation of 451 Danish boys with delayed puberty: Diagnostic use of a new puberty nomogram and effects of oral testosterone therapy. J. Clin. Endocrinol. Metab. 2015, 100, 1376–1385. [Google Scholar] [CrossRef]
- Hannema, S.E. Werkboek Kinderendocrinologie/Late Puberteit Jongens. 2022. Available online: https://nvk.medonline.nl/kinderendocrinologie/late-of-geen-verschijnselen-van-puberteit-jongen/ (accessed on 26 July 2023).

| Genotype | Deletion | Non-Deletion | Mean/Total |
|---|---|---|---|
| N (% of total group = 145) | 89 (61) | 56 (39) | 145 |
| UPD (% of total group) | 18 (12) | ||
| ICD (% of total group) | 5 (3) | ||
| UBE3A (% of total group) | 33 (23) | ||
| Sex (m/f) | 51/38 | 27/29 | 78/67 |
| UPD | 8/10 | ||
| ICD | 3/2 | ||
| UBE3A | 16/17 | ||
| Mean age years (SD) | 9.7 (6.2) | 11.6 (6.1) | 10.5 (6.2) |
| Birth weight SDS (SD) **# | −0.46 (1.0) | −0.80 (1.4) | −0.59 (1.2) |
| UPD | −0.22 (1.1) | ||
| ICD | 1.03 (0.8) | ||
| UBE3A | −1.39 (1.2) | ||
| Epilepsy (N (% of subgroup)) * | 77 (87) | 33 (59) | 110 (76) |
| ASM (N (% of subgroup)) * | 75 (84) | 31 (55) | 104 (71) |
| Valproic acid | 36 (40) | 12 (21) | 48 (33) |
| Independent walking | |||
| (N (% of subgroup)) * | 34 (38) | 48 (86) | 82 (57) |
| Genotype | Deletion (n = 31) | Non-Deletion (n = 22) | Total Group (n = 53) |
|---|---|---|---|
| Total score (SD) # (range 11–55) | 25.3 (9.6) | 24.8 (8.2) | 25.1 (9.0) |
| UPD-ICD | 26.3 (8.6) | ||
| UBE3A | 23.5 (8.0) | ||
| Subscale behavior (SD) (range 5–25) | 11.6 (4.8) | 11.4 (4.0) | 11.5 (4.4) |
| Subscale drive (SD) (range 4–20) | 10.5 (4.0) | 9.8 (3.7) | 10.2 (3.9) |
| Subscale severity (SD) (range 2–10) | 3.3 (1.9) | 3.6 (1.7) | 3.4 (1.8) |
| Genotype | Deletion | Non-Deletion | Total Group | N |
|---|---|---|---|---|
| Height SDS (SD) | −1.23 (1.4) | −1.13 (1.1) | −1.19 (1.3) | 144 |
| UPD | −1.18 (1.4) | |||
| ICD | −1.24 (1.0) | |||
| UBE3A | −1.07 (1.0) | |||
| BMI-SDS (SD) * | 0.37 (1.7) | 1.03 (1.5) | 0.63 (1.7) | 135 |
| UPD | 1.43 (1.4) | |||
| ICD | 0.83 (1.7) | |||
| UBE3A | 0.82 (1.5) | |||
| BMI ≥ 1 SDS (N (% of subgroup)) * | 25 (30) | 33 (62) | 58 (43) | |
| Overweight (BMI ≥ 1–<2 SDS) (N (% of subgroup)) * | 10 (12) | 21 (40) | 31 (23) | |
| Obesity (BMI ≥ 2 SDS) (N (% of subgroup)) | 15 (18) | 12 (22) | 27 (20) | 135 |
| Target height SDS (SD) | 0.20 (0.1) | 0.06 (0.1) | 0.07 (0.87) | 133 |
| Height—Target height SDS (SD) | −1.32 (1.4) | −1.26 (1.1) | −1.30 (1.3) | 133 |
| Age at menarche in years (SD) | 11.8 (2.4) | 11.4 (1.2) | 11.6 (1.9) | 25 |
| Onset of puberty (N (% of subgroup)) | ||||
| Prepubertal | 41 (46) | 18 (32) | 59 (41) | |
| Early | 3 (3) | 0 | 3 (2) | |
| Normal | 40 (45) | 31 (55) | 71 (49) | |
| Late | 5 (6) | 7 (13) | 12 (8) | 145 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bindels-de Heus, K.G.C.B.; Hagenaar, D.A.; Dekker, I.; van der Kaay, D.C.M.; Kerkhof, G.F.; ENCORE Expertise Center for AS; Elgersma, Y.; de Wit, M.-C.Y.; Mous, S.E.; Moll, H.A. Hyperphagia, Growth, and Puberty in Children with Angelman Syndrome. J. Clin. Med. 2023, 12, 5981. https://doi.org/10.3390/jcm12185981
Bindels-de Heus KGCB, Hagenaar DA, Dekker I, van der Kaay DCM, Kerkhof GF, ENCORE Expertise Center for AS, Elgersma Y, de Wit M-CY, Mous SE, Moll HA. Hyperphagia, Growth, and Puberty in Children with Angelman Syndrome. Journal of Clinical Medicine. 2023; 12(18):5981. https://doi.org/10.3390/jcm12185981
Chicago/Turabian StyleBindels-de Heus, Karen G. C. B., Doesjka A Hagenaar, Ilonka Dekker, Danielle C. M. van der Kaay, Gerthe F. Kerkhof, ENCORE Expertise Center for AS, Ype Elgersma, Marie-Claire Y. de Wit, Sabine E. Mous, and Henriette A. Moll. 2023. "Hyperphagia, Growth, and Puberty in Children with Angelman Syndrome" Journal of Clinical Medicine 12, no. 18: 5981. https://doi.org/10.3390/jcm12185981
APA StyleBindels-de Heus, K. G. C. B., Hagenaar, D. A., Dekker, I., van der Kaay, D. C. M., Kerkhof, G. F., ENCORE Expertise Center for AS, Elgersma, Y., de Wit, M.-C. Y., Mous, S. E., & Moll, H. A. (2023). Hyperphagia, Growth, and Puberty in Children with Angelman Syndrome. Journal of Clinical Medicine, 12(18), 5981. https://doi.org/10.3390/jcm12185981