
Association between the Prognostic Nutritional Index and Chronic Microvascular Complications in Patients with Type 2 Diabetes Mellitus


Abstract
:1. Introduction
2. Materials and Methods
3. Results
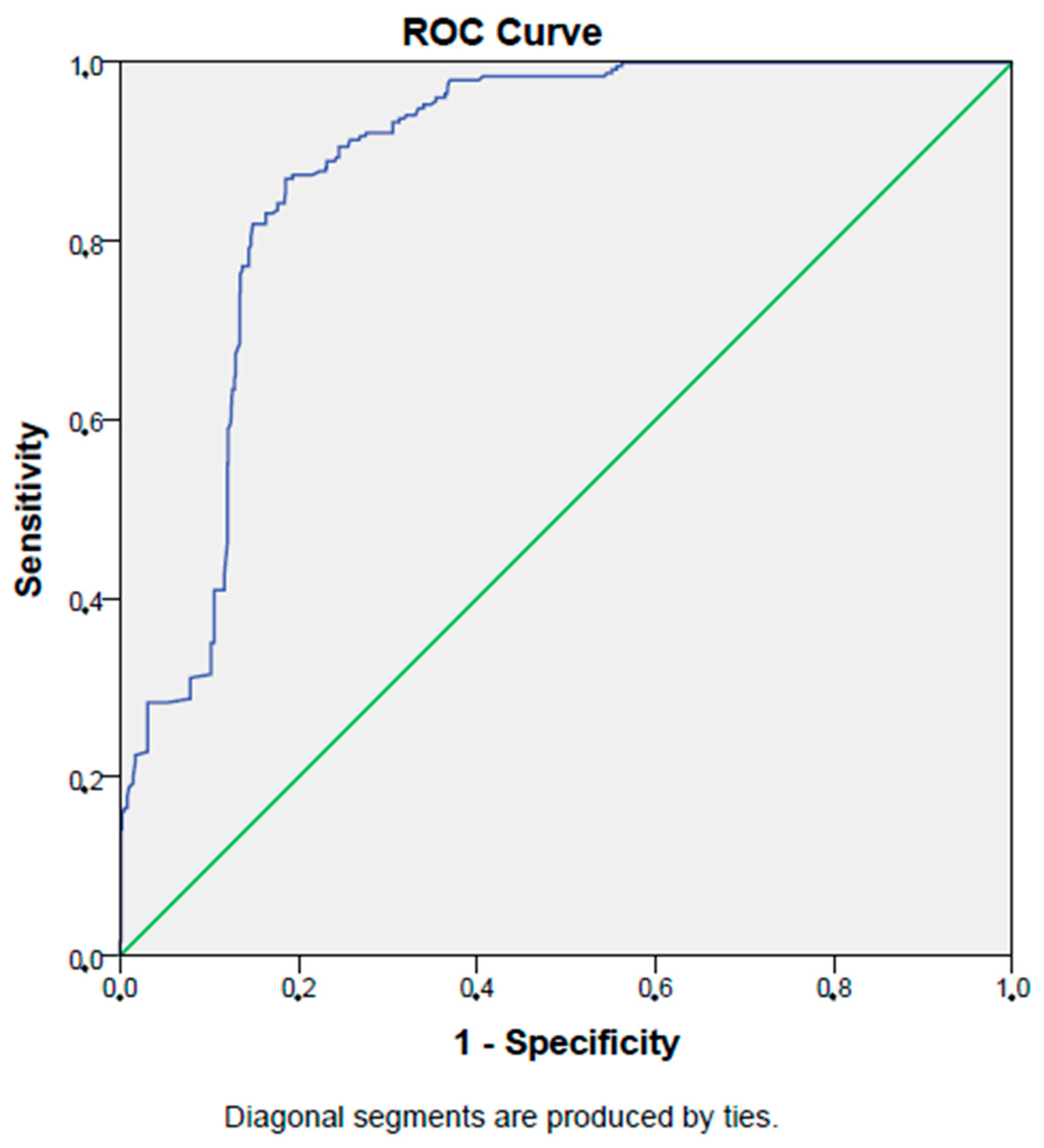
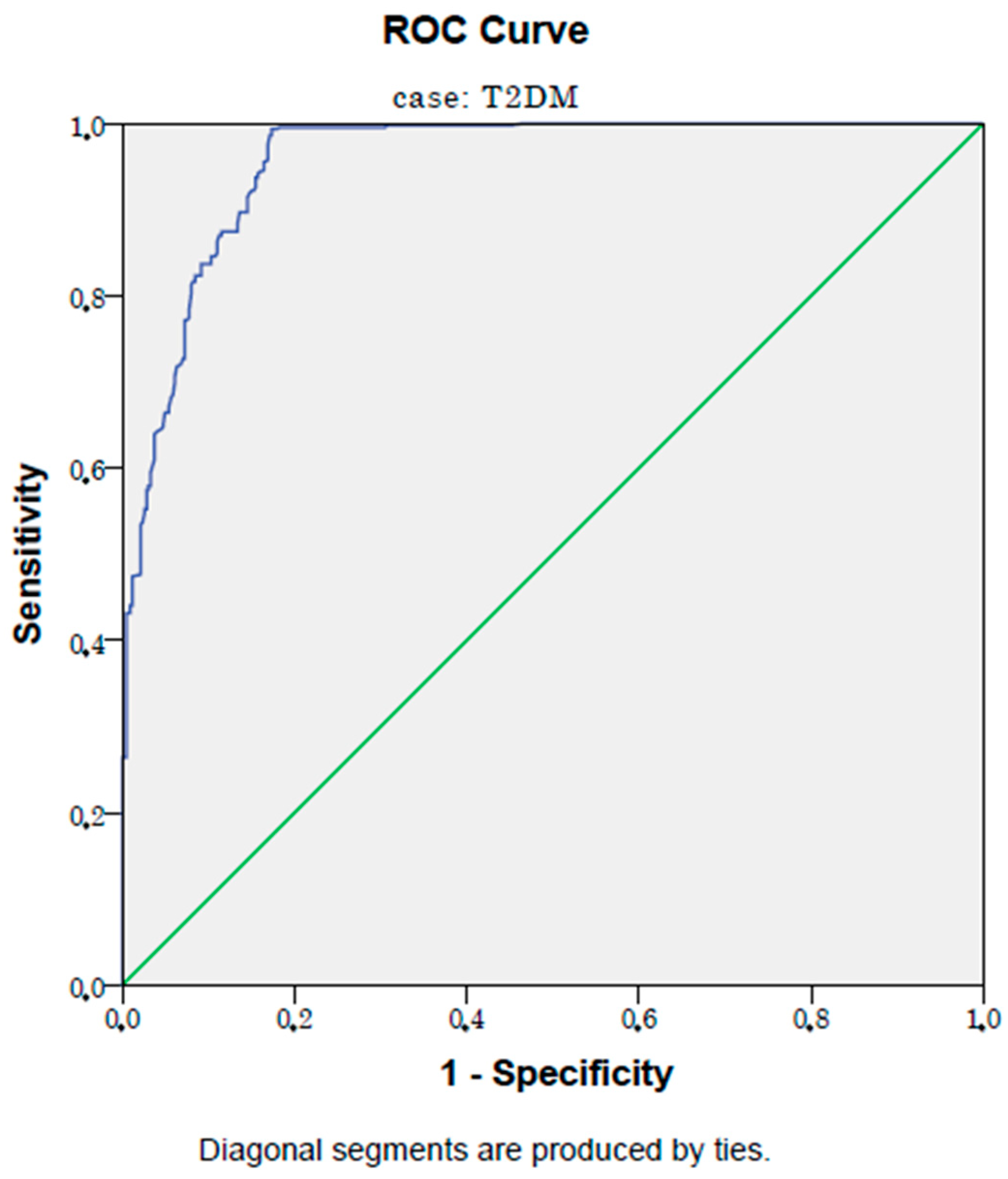
3.1. Analyses of the Data of Diabetic and Control Subjects
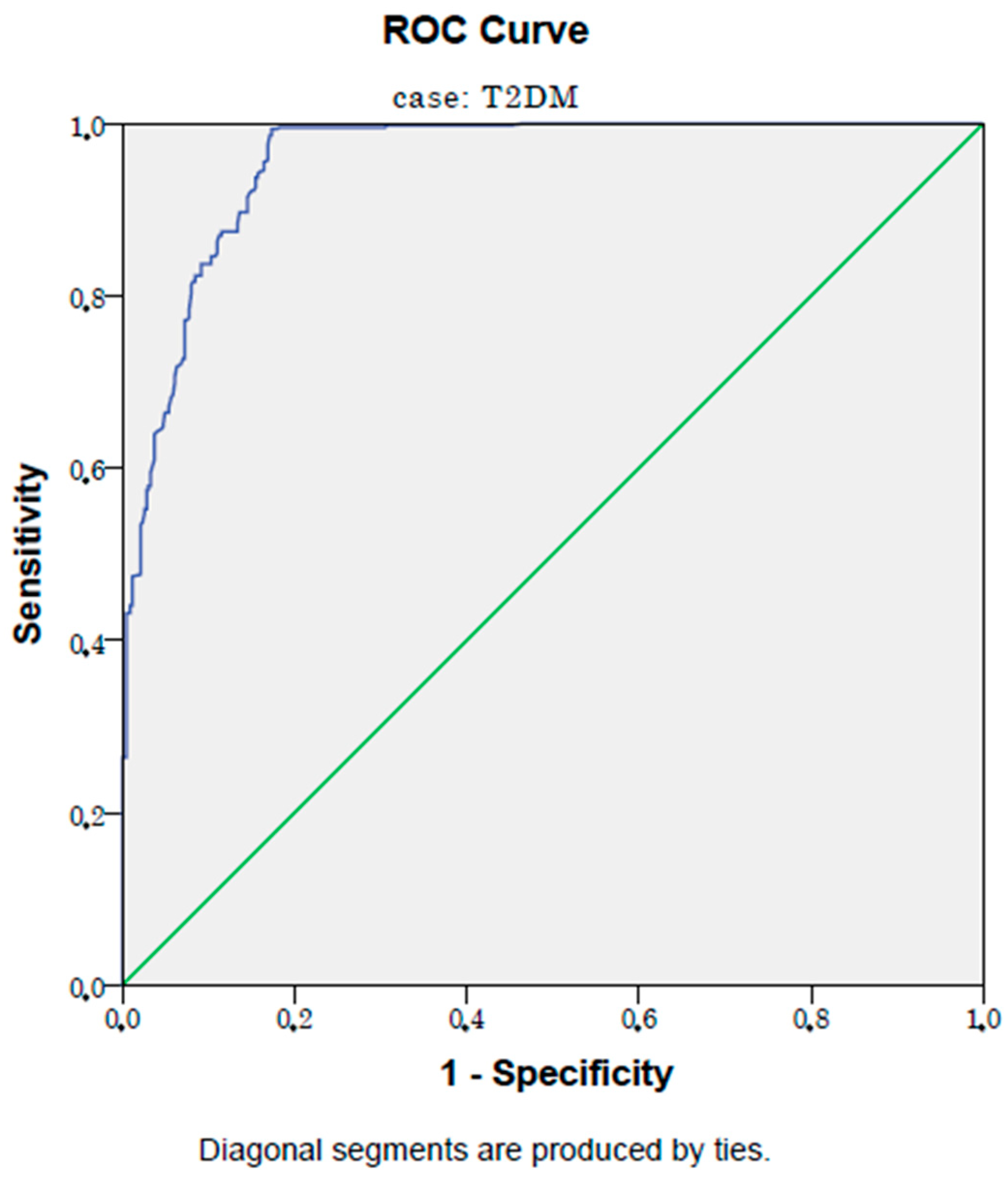
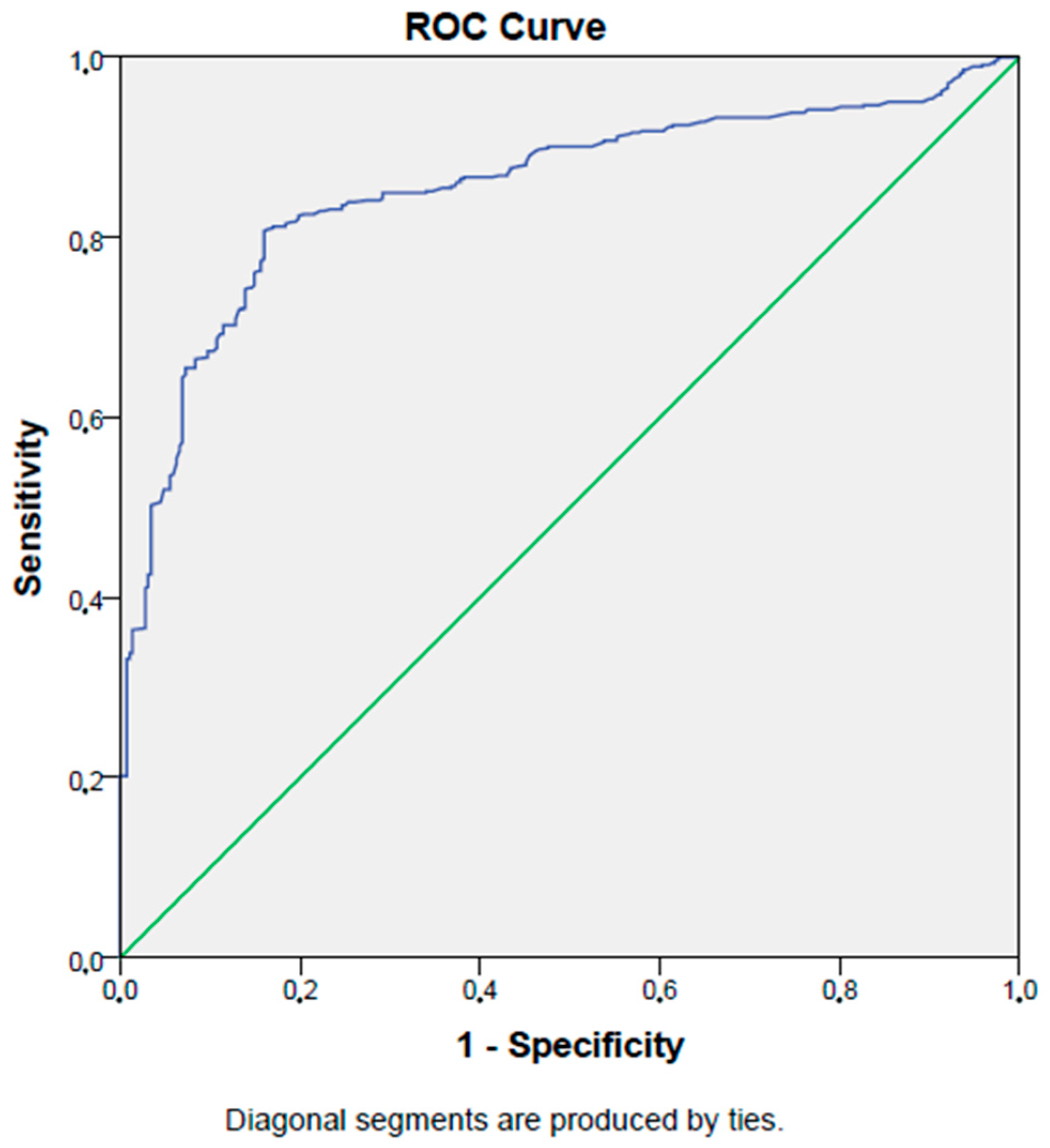
3.2. Analyses of the Data of Diabetic Subjects with/without Microvascular Complications and Control Subjects
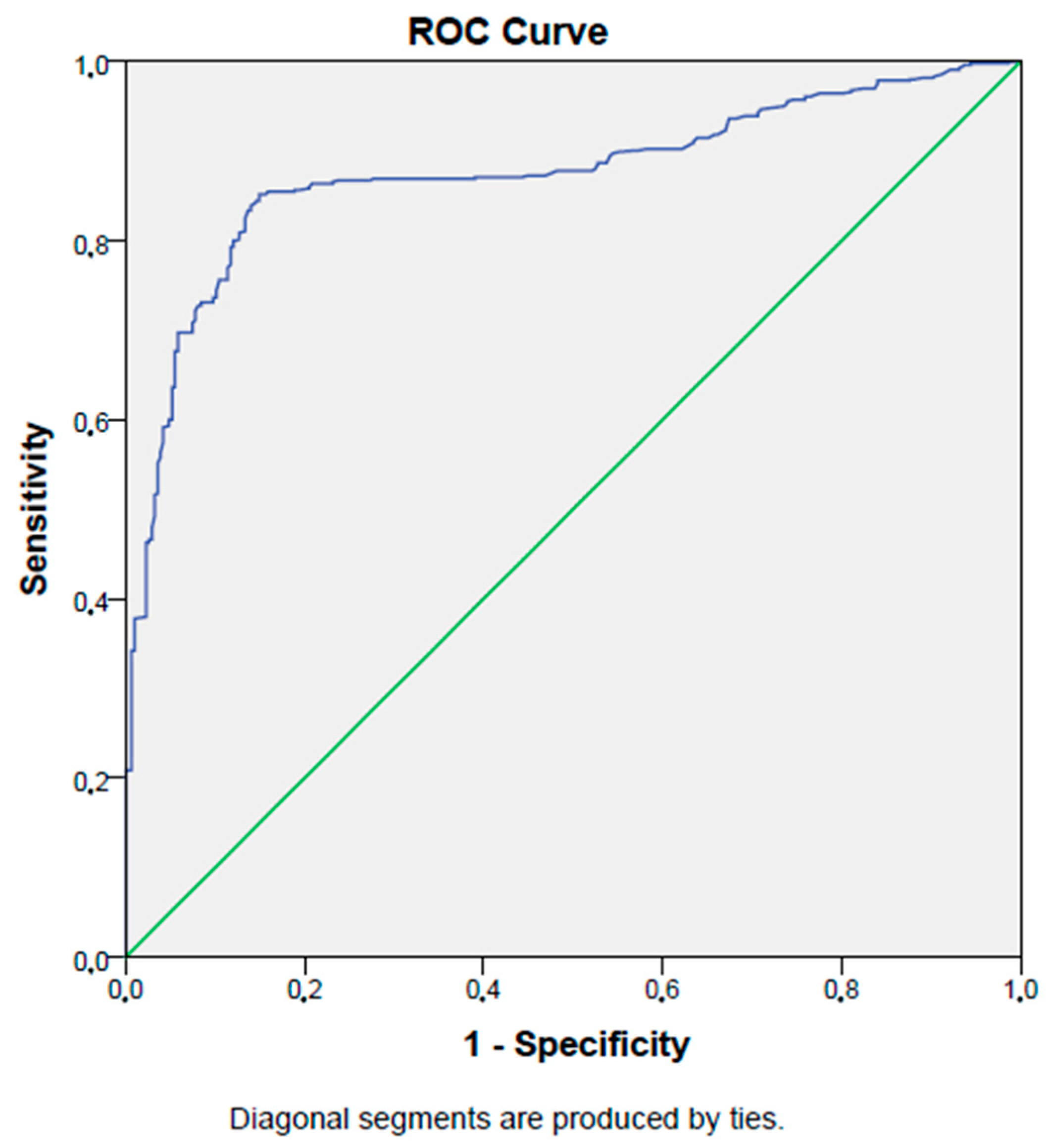
3.3. Analyses of the Data of Diabetic Subjects with/without Diabetic Nephropathy
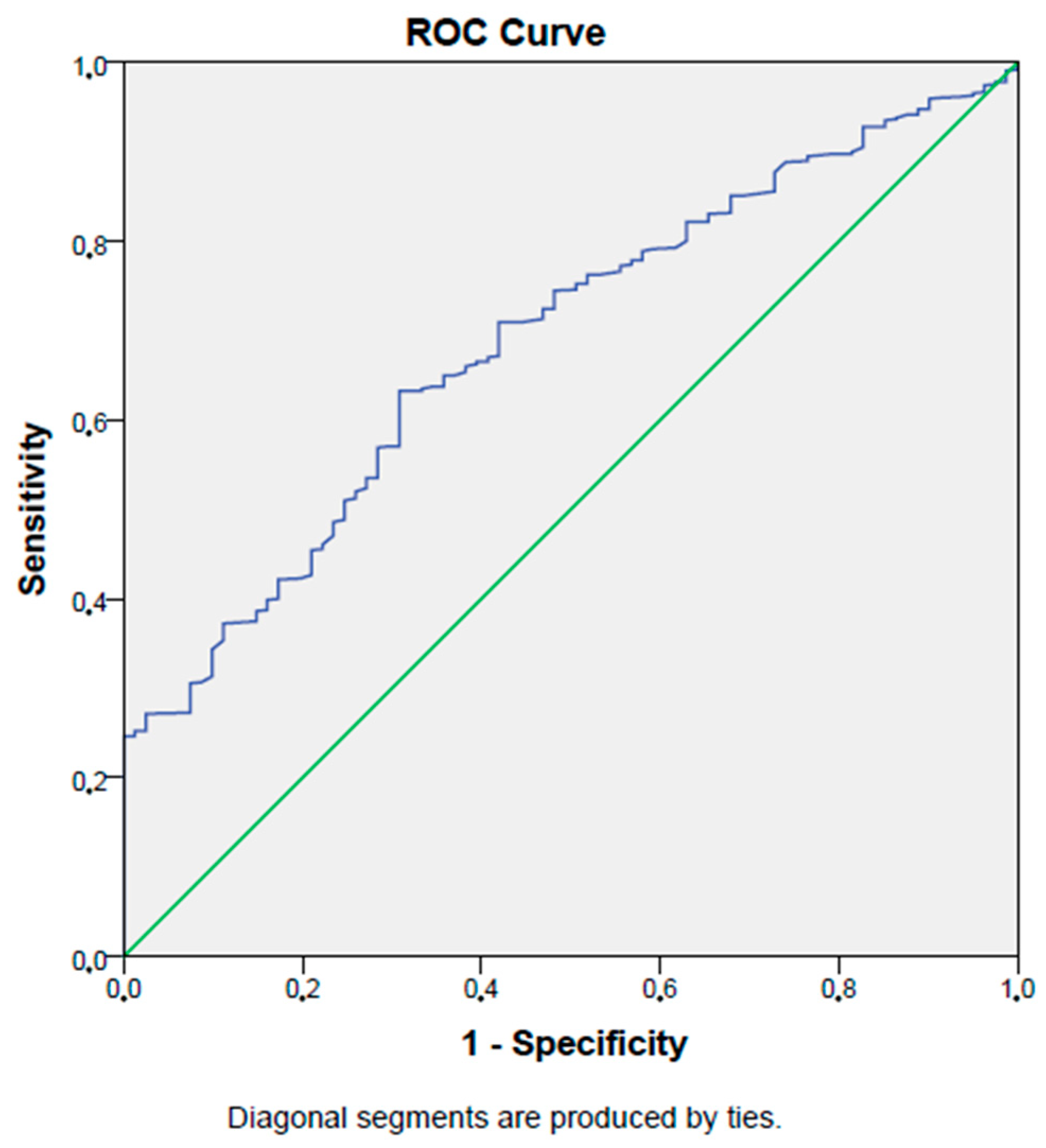
3.4. Analyses of the Data of Diabetic Subjects with/without Diabetic Retinopathy
3.5. Analyses of the Data of Diabetic Subjects with/without Diabetic Neuropathy
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Demirkol, M.E.; Aktas, G.; Alisik, M.; Yis, O.M.; Kaya, M.; Kocadag, D. Is the prognostic nutritional index a predictor of COVID-19 related hospitalizations and mortality? Malawi Med. J. 2023, 35, 15–21. [Google Scholar] [CrossRef]
- Kocak, M.Z.; Aktas, G.; Erkus, E.; Yis, O.M.; Duman, T.T.; Atak, B.M.; Savli, H. Neuregulin-4 is associated with plasma glucose and increased risk of type 2 diabetes mellitus. Swiss Med. Wkly. 2019, 149, w20139. [Google Scholar] [CrossRef] [PubMed]
- Demirkol, M.E.; Aktas, G. C-reactive protein to LymphocytE count ratio could be a reliable mArkeR of thyroiditis; the CLEAR-T study. Precis. Med. Sci. 2022, 11, 31–34. [Google Scholar] [CrossRef]
- Oguntibeju, O.O. Type 2 diabetes mellitus, oxidative stress and inflammation: Examining the links. Int. J. Physiol. Pathophysiol. Pharmacol. 2019, 11, 45–63. [Google Scholar] [PubMed]
- Guarner, V.; Rubio-Ruiz, M.E. Low-grade systemic inflammation connects aging, metabolic syndrome and cardiovascular disease. Interdiscip. Top. Gerontol. 2015, 40, 99–106. [Google Scholar] [CrossRef]
- Keeter, W.C.; Moriarty, A.K.; Galkina, E.V. Role of neutrophils in type 2 diabetes and associated atherosclerosis. Int. J. Biochem. Cell Biol. 2021, 141, 106098. [Google Scholar] [CrossRef]
- Castrillo, A.; Joseph, S.B.; Vaidya, S.A.; Haberland, M.; Fogelman, A.M.; Cheng, G.; Tontonoz, P. Crosstalk between LXR and toll-like receptor signaling mediates bacterial and viral antagonism of cholesterol metabolism. Mol. Cell 2003, 12, 805–816. [Google Scholar] [CrossRef]
- Badawi, A.; Klip, A.; Haddad, P.; Cole, D.E.; Bailo, B.G.; El-Sohemy, A.; Karmali, M. Type 2 diabetes mellitus and inflammation: Prospects for biomarkers of risk and nutritional intervention. Diabetes Metab. Syndr. Obes. Targets Ther. 2010, 3, 173–186. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, Y.; Zhang, X.; Zhang, T. Pretreatment prognostic nutritional index as a prognostic factor in lung cancer: Review and meta-analysis. Clin. Chim. Acta Int. J. Clin. Chem. 2018, 486, 303–310. [Google Scholar] [CrossRef]
- Kim, S.I.; Kim, S.J.; Kim, S.J.; Cho, D.S. Prognostic nutritional index and prognosis in renal cell carcinoma: A systematic review and meta-analysis. Urol. Oncol. 2021, 39, 623–630. [Google Scholar] [CrossRef]
- Nozoe, T.; Kohno, M.; Iguchi, T.; Mori, E.; Maeda, T.; Matsukuma, A.; Ezaki, T. The prognostic nutritional index can be a prognostic indicator in colorectal carcinoma. Surg. Today 2012, 42, 532–535. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; North, B.V.; Sharma, R. A novel, externally validated inflammation-based prognostic algorithm in hepatocellular carcinoma: The prognostic nutritional index (PNI). Br. J. Cancer 2012, 106, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Nozoe, T.; Ninomiya, M.; Maeda, T.; Matsukuma, A.; Nakashima, H.; Ezaki, T. Prognostic nutritional index: A tool to predict the biological aggressiveness of gastric carcinoma. Surg. Today 2010, 40, 440–443. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Deng, H.; Wang, Y.; Chen, L.; Gu, X.; Wang, X. Predictive value of the prognostic nutritional index for the severity of coronavirus disease 2019. Nutrition 2021, 84, 111123. [Google Scholar] [CrossRef] [PubMed]
- Wada, H.; Dohi, T.; Miyauchi, K.; Jun, S.; Endo, H.; Doi, S.; Konishi, H.; Naito, R.; Tsuboi, S.; Ogita, M.; et al. Relationship between the prognostic nutritional index and long-term clinical outcomes in patients with stable coronary artery disease. J. Cardiol. 2018, 72, 155–161. [Google Scholar] [CrossRef]
- Park, S.; Kang, H.J.; Jeon, J.H.; Kim, M.J.; Lee, I.K. Recent advances in the pathogenesis of microvascular complications in diabetes. Arch. Pharmacal Res. 2019, 42, 252–262. [Google Scholar] [CrossRef]
- Kocak, M.Z.; Aktas, G.; Duman, T.T.; Atak, B.M.; Savli, H. Is Uric Acid elevation a random finding or a causative agent of diabetic nephropathy? Rev. Assoc. Medica Bras. 2019, 65, 1155–1160. [Google Scholar] [CrossRef]
- Pérez-Morales, R.E.; Del Pino, M.D.; Valdivielso, J.M.; Ortiz, A.; Mora-Fernández, C.; Navarro-González, J.F. Inflammation in Diabetic Kidney Disease. Nephron 2019, 143, 12–16. [Google Scholar] [CrossRef]
- Aktas, G.; Yilmaz, S.; Kantarci, D.B.; Duman, T.T.; Bilgin, S.; Balci, S.B.; Atak Tel, B.M. Is serum uric acid-to-HDL cholesterol ratio elevation associated with diabetic kidney injury? Postgrad. Med. 2023, 135, 519–523. [Google Scholar] [CrossRef]
- Bilgin, S.; Kurtkulagi, O.; Atak Tel, B.M.; Duman, T.T.; Kahveci, G.; Khalid, A.; Aktas, G. Does C-reactive protein to serum Albumin Ratio correlate with diabEtic nephropathy in patients with Type 2 dIabetes MEllitus? The CARE TIME study. Prim. Care Diabetes 2021, 15, 1071–1074. [Google Scholar] [CrossRef]
- Dieter, B.P.; McPherson, S.M.; Afkarian, M.; de Boer, I.H.; Mehrotra, R.; Short, R.; Barbosa-Leiker, C.; Alicic, R.Z.; Meek, R.L.; Tuttle, K.R. Serum amyloid a and risk of death and end-stage renal disease in diabetic kidney disease. J. Diabetes Its Complicat. 2016, 30, 1467–1472. [Google Scholar] [CrossRef] [PubMed]
- Yeo, E.S.; Hwang, J.Y.; Park, J.E.; Choi, Y.J.; Huh, K.B.; Kim, W.Y. Tumor necrosis factor (TNF-alpha) and C-reactive protein (CRP) are positively associated with the risk of chronic kidney disease in patients with type 2 diabetes. Yonsei Med. J. 2010, 51, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Vincent, A.M.; Callaghan, B.C.; Smith, A.L.; Feldman, E.L. Diabetic neuropathy: Cellular mechanisms as therapeutic targets. Nature reviews. Neurology 2011, 7, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Román-Pintos, L.M.; Villegas-Rivera, G.; Rodríguez-Carrizalez, A.D.; Miranda-Díaz, A.G.; Cardona-Muñoz, E.G. Diabetic Polyneuropathy in Type 2 Diabetes Mellitus: Inflammation, Oxidative Stress, and Mitochondrial Function. J. Diabetes Res. 2016, 2016, 3425617. [Google Scholar] [CrossRef]
- Herder, C.; Lankisch, M.; Ziegler, D.; Rathmann, W.; Koenig, W.; Illig, T.; Döring, A.; Thorand, B.; Holle, R.; Giani, G.; et al. Subclinical inflammation and diabetic polyneuropathy: MONICA/KORA Survey F3 (Augsburg, Germany). Diabetes Care 2009, 32, 680–682. [Google Scholar] [CrossRef]
- Azenabor, A.; Ogbera, A.O.; Adejumo, N.E.; Adejare, A.O. Acute phase reactant dynamics and incidence of microvascular dysfunctions in type 2 diabetes mellitus. J. Res. Med. Sci. Off. J. Isfahan Univ. Med. Sci. 2011, 16, 1298–1305. [Google Scholar]
- Aktas, G. Serum C-Reactive Protein to Albumin Ratio as a Reliable Marker of Diabetic Neuropathy in Type 2 Diabetes Mellitus. preprints 2023, 2023060202. [Google Scholar] [CrossRef]
- Zubair, M.; Malik, A.; Ahmad, J. Plasma adiponectin, IL-6, hsCRP, and TNF-α levels in subject with diabetic foot and their correlation with clinical variables in a North Indian tertiary care hospital. Indian J. Endocrinol. Metab. 2012, 16, 769–776. [Google Scholar] [CrossRef]
- Juranek, J.K.; Geddis, M.S.; Song, F.; Zhang, J.; Garcia, J.; Rosario, R.; Yan, S.F.; Brannagan, T.H.; Schmidt, A.M. RAGE deficiency improves postinjury sciatic nerve regeneration in type 1 diabetic mice. Diabetes 2013, 62, 931–943. [Google Scholar] [CrossRef]
- Yamakawa, I.; Kojima, H.; Terashima, T.; Katagi, M.; Oi, J.; Urabe, H.; Sanada, M.; Kawai, H.; Chan, L.; Yasuda, H.; et al. Inactivation of TNF-α ameliorates diabetic neuropathy in mice. American journal of physiology. Endocrinol. Metab. 2011, 301, E844–E852. [Google Scholar] [CrossRef]
- Sasongko, M.B.; Wong, T.Y.; Jenkins, A.J.; Nguyen, T.T.; Shaw, J.E.; Wang, J.J. Circulating markers of inflammation and endothelial function, and their relationship to diabetic retinopathy. Diabet. Med. A J. Br. Diabet. Assoc. 2015, 32, 686–691. [Google Scholar] [CrossRef] [PubMed]
- Gustavsson, C.; Agardh, E.; Bengtsson, B.; Agardh, C.D. TNF-alpha is an independent serum marker for proliferative retinopathy in type 1 diabetic patients. J. Diabetes Its Complicat. 2008, 22, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Rajab, H.A.; Baker, N.L.; Hunt, K.J.; Klein, R.; Cleary, P.A.; Lachin, J.; Virella, G.; Lopes-Virella, M.F. The predictive role of markers of Inflammation and endothelial dysfunction on the course of diabetic retinopathy in type 1 diabetes. J. Diabetes Its Complicat. 2015, 29, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Chohno, T.; Uchino, M.; Sasaki, H.; Bando, T.; Takesue, Y.; Ikeuchi, H. Associations Between the Prognostic Nutritional Index and Morbidity/Mortality During Intestinal Resection in Patients with Ulcerative Colitis. World J. Surg. 2018, 42, 1949–1959. [Google Scholar] [CrossRef]
- Kato, H.; Seishima, R.; Nakamura, K.; Matsui, S.; Shigeta, K.; Okabayashi, K.; Kitagawa, Y. The Prognostic Nutritional Index is a Predictive Marker for Postoperative Complications in Patients with Late-Onset Ulcerative Colitis. World J. Surg. 2023. [Google Scholar] [CrossRef]
- Duan, S.; Sun, L.; Zhang, C.; Wu, L.; Nie, G.; Huang, Z.; Xing, C.; Zhang, B.; Yuan, Y. Association of platelet-to-lymphocyte ratio with kidney clinicopathologic features and renal outcomes in patients with diabetic kidney disease. Int. Immunopharmacol. 2021, 93, 107413. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Mukanova, U.; Yessirkepov, M.; Kitas, G.D. The Platelet-to-Lymphocyte Ratio as an Inflammatory Marker in Rheumatic Diseases. Ann. Lab. Med. 2019, 39, 345–357. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef]
- Demirbaş, A.; Kaya İslamoğlu, Z.G. Can decreased monocyte to HDL-cholesterol ratio be a marker indicating the anti-inflammatory effect of the colchicine in Behçet’s disease? A preliminary study. Dermatol. Ther. 2020, 33, e14013. [Google Scholar] [CrossRef]
- Kamrul-Hasan, A.; Mustari, M.; Asaduzzaman, M.; Gaffar, M.A.J.; Chanda, P.K.; Rahman, M.M.; Hannan, M.A.; Akter, F.; Saifuddin, M.; Selim, S. Evaluation of neutrophil–lymphocyte ratio and platelet–lymphocyte ratio as markers of diabetic kidney disease in Bangladeshi patients with type 2 diabetes mellitus. J. Diabetol. 2021, 12, 58–62. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T2DM Group | Control Group | p | ||
|---|---|---|---|---|
| Sex | Women (n, %) | 416 (48%) | 73 (29%) | <0.001 |
| Men (n, %) | 457 (52%) | 181 (71%) | ||
| Smoking | Yes (n, %) | 187 (21%) | 28 (11%) | <0.001 |
| No (n, %) | 688 (79%) | 226 (89%) | ||
| Alcohol consumption | Yes (n, %) | 56 (6%) | 0 (0%) | <0.001 |
| No (n, %) | 817 (94%) | 254 (100%) | ||
| Mean ± SD | ||||
| Age (years) | 57.7 ± 10.6 | 47.2 ± 13.8 | <0.001 | |
| Hb (g/dL) | 13.8 ± 1.9 | 13.9 ± 1.4 | 0.39 | |
| Htc (%) | 40.5 ± 5.4 | 41.5 ± 4.1 | 0.08 | |
| Median (min–max) | ||||
| PNI (%) | 51.6 (30.1–73.8) | 64.8 (49.4–76) | <0.001 | |
| Height (m) | 1.64 (1.35–1.9) | 1.67 (1.52–1.87) | 0.1 | |
| Weight (kg) | 86 (45–150) | 72 (55–136) | <0.001 | |
| Waist circumference (cm) | 105 (75–160) | 95 (65–144) | <0.001 | |
| BMI (kg/m2) | 31.1 (16.6–55.4) | 27.6 (18.3–49.4) | <0.001 | |
| Systolic blood pressure (mmHg) | 120 (90–200) | 120 (100–180) | 0.12 | |
| Diastolic blood pressure (mmHg) | 75 (50–110) | 80 (50–105) | 0.11 | |
| Leukocyte count (k/mm3) | 7.2 (4.2–14.4) | 5.5 (4–14.1) | 0.1 | |
| Platelet count (k/mm3) | 230 (154–441) | 239 (151–374) | 0.64 | |
| Albumin (g/dL) | 4 (1.8–5.6) | 4.4 (3.9–5.4) | <0.001 | |
| C-reactive protein (mg/L) | 4.1 (0.1–25) | 2.4 (0.1–12) | <0.001 | |
| HbA1c (%) | 7.6 (5.9–17.2) | 5.4 (4.8–6.4) | <0.001 | |
| Glucose (mg/dL) | 142 (65–565) | 93 (69–117) | <0.001 | |
| Urea (mg/dL) | 32 (13–258) | 26 (13–62) | <0.001 | |
| Creatinine (mg/dL) | 0.8 (0.39–3.93) | 0.69 (0.4–1.3) | 0.09 | |
| eGFR (%) | 102 (14–111) | 114 (58–118) | <0.001 | |
| AST (U/L) | 19 (6–97) | 18 (9–35) | 0.15 | |
| ALT (U/L) | 23 (6–96) | 19 (6–58) | 0.11 | |
| Total cholesterol (mg/dL) | 204 (50–378) | 194 (114–290) | <0.001 | |
| LDL-cholesterol (mg/dL) | 125 (21–244) | 112 (49–192) | <0.001 | |
| HDL-cholesterol (mg/dL) | 44 (13–92) | 48 (21–85) | <0.001 | |
| Triglyceride (mg/dL) | 156 (47–1050) | 124 (52–680) | <0.001 | |
| p | OR | 95% CI | |
|---|---|---|---|
| Age | 0.53 | 0.98 | 0.93–1.04 |
| Gender | 0.48 | 1.7 | 0.39–7.36 |
| PNI | <0.001 | 1.46 | 1.27–1.68 |
| Waist circumference | 0.87 | 0.99 | 0.91–1.08 |
| BMI | 0.01 | 0.72 | 0.55–0.94 |
| C-reactive protein | 0.44 | 1.01 | 0.87–1.39 |
| HbA1c | <0.001 | 0.096 | 0.03–0.29 |
| Fasting glucose | <0.001 | 0.87 | 0.82–0.94 |
| Serum creatinine | 0.04 | 62.8 | 1.21–324 |
| eGFR | 0.001 | 1.09 | 1.03–1.14 |
| T2DM with Microvascular Complications | T2DM without Microvascular Complications | Control Group | p | ||
|---|---|---|---|---|---|
| Sex | Women (n, %) | 253 (59%) | 163 (36.5%) | 73 (29%) | <0.001 |
| Men (n, %) | 173 (41%) | 284 (63.5%) | 181 (71%) | ||
| Mean ± SD | |||||
| Age (years) | 59.3 ± 10.5 | 56.2 ± 10.4 | 47.2 ± 13.8 | <0.001 | |
| Hb (g/dL) | 13.1 ± 1.7 | 14.4 ± 2 | 13.9 ± 1.4 | <0.001 | |
| Median (min–max) | |||||
| PNI (%) | 42.8 (30.1–62.5) | 57.6 (43.1–73.8) | 64.8 (49.4–76) | <0.001 | |
| Height (m) | 1.6 (1.4–1.9) | 1.66 (1.35–1.85) | 1.67 (1.53–1.87) | 0.099 | |
| Weight (kg) | 80 (45–150) | 90 (58–123) | 72 (55–136) | <0.001 | |
| Waist circumference (cm) | 105 (75–160) | 107 (82–137) | 95 (65–144) | <0.001 | |
| BMI (kg/m2) | 30.5 (16.6–55.4) | 31.3 (20.6–46.1) | 27.6 (18.3–49.4) | <0.001 | |
| Systolic BP (mmHg) | 120 (90–200) | 125 (95–180) | 120 (100–180) | 0.11 | |
| Diastolic BP (mmHg) | 75 (50–110) | 80 (50–110) | 80 (50–105) | 0.44 | |
| Leukocyte count (k/mm3) | 7 (4.2–14.4) | 7.7 (4.2–13.7) | 5.5 (4–14.1) | 0.066 | |
| Htc (%) | 39 (25–52) | 42 (25–51) | 42 (37–51) | 0.037 | |
| Platelet count (k/mm3) | 248 (154–441) | 219 (158–423) | 239 (151–374) | 0.15 | |
| Albumin (g/dL) | 3.2 (1.8–4.7) | 4.4 (3.1–5.6) | 4.4 (3.9–5.4) | <0.001 | |
| C-reactive protein (mg/L) | 6.8 (0.1–25) | 2.7 (0.1–17) | 2.4 (0.1–12) | <0.001 | |
| HbA1c (%) | 8.2 (5.9–17.2) | 7.4 (6.1–15.9) | 5.4 (4.8–6.4) | <0.001 | |
| Glucose (mg/dL) | 170 (65–565) | 127 (70–514) | 93 (69–117) | <0.001 | |
| Urea (mg/dL) | 32.1 (15–258) | 32.1 (13–86) | 26 (13–62) | 0.057 | |
| Creatinine (mg/dL) | 0.8 (0.5–3.93) | 0.77 (0.39–1.87) | 0.49 (0.4–1.3) | 0.19 | |
| eGFR (%) | 96 (14–110) | 101 (45–111) | 114 (58–118) | 0.044 | |
| AST (U/L) | 18 (6–97) | 20 (8–53) | 18 (9–35) | 0.23 | |
| ALT (U/L) | 19 (6–96) | 26 (6–94) | 19 (6–58) | 0.21 | |
| Total cholesterol (mg/dL) | 192 (50–318) | 212 (50–378) | 194 (114–290) | 0.028 | |
| LDL-cholesterol (mg/dL) | 112 (21–202) | 129 (42–244) | 112 (49–192) | 0.019 | |
| HDL-cholesterol (mg/dL) | 46 (13–92) | 43 (17–77) | 48 (21–85) | 0.038 | |
| Triglyceride (mg/dL) | 152 (47–1050) | 171 (50–856) | 124 (52–680) | <0.001 | |
| T2DM with Diabetic Nephropathy | T2DM without Diabetic Nephropathy | p | ||
|---|---|---|---|---|
| Sex | Women (n, %) | 164 (53%) | 252 (44.5%) | 0.01 |
| Men (n, %) | 143 (47%) | 314 (55.5%) | ||
| Median (min–max) | ||||
| Age (years) | 57 (36–87) | 60 (29–89) | 0.42 | |
| Hb (g/dL) | 13.1 (7.8–17.6) | 14 (6.7–17.9) | <0.001 | |
| Htc (%) | 39 (25–52) | 41 (22–56) | <0.001 | |
| PNI (%) | 43 (30–63) | 56 (36–74) | <0.001 | |
| Height (m) | 1.6 (1.4–1.9) | 1.65 (1.35–1.85) | 0.14 | |
| Weight (kg) | 79 (45.5–150) | 90 (58–123) | <0.001 | |
| Waist circumference (cm) | 102 (75–160) | 108 (82–148) | <0.001 | |
| BMI (kg/m2) | 30 (17–49) | 33 (21–55) | <0.001 | |
| Systolic blood pressure (mmHg) | 120 (90–200) | 130 (95–180) | 0.07 | |
| Diastolic blood pressure (mmHg) | 75 (50–110) | 75 (50–110) | 0.48 | |
| Leukocyte count (k/mm3) | 7.2 (4.2–14.4) | 7.2 (4.2–14) | 0.28 | |
| Platelet count (k/mm3) | 266 (154–441) | 220 (151–374) | <0.001 | |
| Albumin (g/dL) | 3.2 (1.8–4.7) | 4.4 (2.9–5.6) | <0.001 | |
| C-reactive protein (mg/L) | 6.5 (0.1–25) | 3.4 (0.1–25) | <0.001 | |
| HbA1c (%) | 8.9 (5.9–17.2) | 7.4 (5.9–15.9) | <0.001 | |
| Glucose (mg/dL) | 180 (65–565) | 129 (66–514) | <0.001 | |
| Urea (mg/dL) | 32 (15–258) | 32 (13–222) | 0.61 | |
| Creatinine (mg/dL) | 0.8 (0.39–3.93) | 0.78 (0.54–1.5) | 0.99 | |
| eGFR (%) | 95 (14–111) | 102 (58–110) | <0.001 | |
| AST (U/L) | 17 (6–97) | 20 (6–58) | 0.21 | |
| ALT (U/L) | 19 (6–96) | 23 (6–94) | 0.56 | |
| Total cholesterol (mg/dL) | 202 (52–318) | 204 (50–378) | 0.01 | |
| LDL-cholesterol (mg/dL) | 112 (29–202) | 126 (21–244) | 0.003 | |
| HDL-cholesterol (mg/dL) | 47 (13–92) | 43 (14–80) | <0.001 | |
| Triglyceride (mg/dL) | 152 (47–411) | 166 (50–1050) | 0.006 | |
| T2DM with Diabetic Retinopathy | T2DM without Diabetic Retinopathy | p | ||
|---|---|---|---|---|
| Sex | Women (n, %) | 60 (74%) | 356 (45%) | <0.001 |
| Men (n, %) | 21 (26%) | 436 (55%) | ||
| Median (min–max) | ||||
| Age (years) | 56 (46–89) | 60 (29–86) | 0.66 | |
| Hb (g/dL) | 13.2 (6.7–16.9) | 13.7 (8.5–17.9) | <0.001 | |
| Htc (%) | 36 (22–49) | 40 (25–56) | <0.001 | |
| PNI (%) | 43.3 (36.3–59.8) | 52.7 (30.1–73.8) | <0.001 | |
| Height (m) | 1.61 (1.44–1.76) | 1.65 (1.35–1.9) | 0. 001 | |
| Weight (kg) | 80 (55–120) | 86 (46–150) | 0.65 | |
| Waist circumference (cm) | 107 (82–148) | 105 (75–160) | 0.15 | |
| BMI (kg/m2) | 32.3 (22.2–55.4) | 31.1 (16.6–49) | 0.19 | |
| Systolic blood pressure (mmHg) | 130 (100–170) | 120 (90–200) | 0.09 | |
| Diastolic blood pressure (mmHg) | 80 (60–110) | 75 (50–110) | 0.2 | |
| Leukocyte count (k/mm3) | 7.1 (4.6–14) | 7.2 (4.2–14.4) | 0.19 | |
| Platelet count (k/mm3) | 225 (151–441) | 235 (154–374) | 0.25 | |
| Albumin (g/dL) | 3.2 (2.9–4.7) | 4.1 (1.8–5.6) | <0.001 | |
| C-reactive protein (mg/L) | 8.1 (0.1–25) | 3.6 (0.1–17) | <0.001 | |
| HbA1c (%) | 9.3 (6.1–14.8) | 7.4 (5.9–17.2) | <0.001 | |
| Glucose (mg/dL) | 196 (66–439) | 136 (65–565) | <0.001 | |
| Urea (mg/dL) | 39 (20–222) | 32 (13–258) | 0.07 | |
| Creatinine (mg/dL) | 0.79 (0.5–3.4) | 0.8 (0.39–3.93) | 0.7 | |
| eGFR (%) | 100 (14–110) | 102 (15–111) | 0.054 | |
| AST (U/L) | 17 (6–45) | 18 (7–97) | 0.56 | |
| ALT (U/L) | 18 (6–42) | 23 (12–94) | 0.48 | |
| Total cholesterol (mg/dL) | 196 (50–318) | 205 (50–378) | 0.34 | |
| LDL-cholesterol (mg/dL) | 125 (21–197) | 124 (42–244) | 0.49 | |
| HDL-cholesterol (mg/dL) | 44 (14–80) | 44 (13–92) | 0.58 | |
| Triglyceride (mg/dL) | 143 (50–358) | 157 (47–1050) | 0.68 | |
| T2DM with Diabetic Neuropathy | T2DM without Diabetic Neuropathy | p | ||
|---|---|---|---|---|
| Sex | Women (n, %) | 184 (64%) | 232 (40%) | <0.001 |
| Men (n, %) | 104 (36%) | 353 (60%) | ||
| Median (min–max) | ||||
| Age (years) | 58.5 (41–87) | 60 (29–89) | 0.02 | |
| Hb (g/dL) | 13.2 (7.8–16.9) | 14 (6.7–17.9) | <0.001 | |
| Htc (%) | 39 (25–49) | 41 (22–56) | <0.001 | |
| PNI (%) | 43.3 (36.3–59.8) | 52.7 (30.1–73.8) | <0.001 | |
| Height (m) | 1.6 (1.44–1.82) | 1.66 (1.35–1.9) | <0.001 | |
| Weight (kg) | 81 (48–120) | 90 (46–150) | <0.001 | |
| Waist circumference (cm) | 105 (75–132) | 106 (78–160) | 0.053 | |
| BMI (kg/m2) | 30.5 (16.6–46.3) | 31.2 (18.9–55.4) | 0.31 | |
| Systolic blood pressure (mmHg) | 120 (90–180) | 125 (90–200) | 0.16 | |
| Diastolic blood pressure (mmHg) | 70 (50–110) | 80 (50–110) | 0.09 | |
| Leukocyte count (k/mm3) | 6.9 (4.2–14) | 7.5 (4.2–14.4) | 0.11 | |
| Platelet count (k/mm3) | 250 (155–441) | 222 (151–374) | 0.08 | |
| Albumin (g/dL) | 3.2 (1.8–4.6) | 4.4 (2.9–5.6) | <0.001 | |
| C-reactive protein (mg/L) | 9.5 (0.1–25) | 2.1 (0.1–21) | <0.001 | |
| HbA1c (%) | 8.3 (5.9–16.5) | 7.4 (6.1–17.2) | <0.001 | |
| Glucose (mg/dL) | 180 (66–565) | 128 (65–514) | <0.001 | |
| Urea (mg/dL) | 32 (17–222) | 32 (13–258) | 0.16 | |
| Creatinine (mg/dL) | 0.82 (0.6–3.4) | 0.79 (0.39–3.93) | 0.97 | |
| eGFR (%) | 99.8 (14–105) | 105 (15–111) | 0.001 | |
| AST (U/L) | 19 (6–69) | 19 (8–97) | 0.14 | |
| ALT (U/L) | 20 (6–94) | 23 (14–74) | 0.11 | |
| Total cholesterol (mg/dL) | 187 (52–318) | 206 (50–378) | <0.001 | |
| LDL-cholesterol (mg/dL) | 112 (21–200) | 129 (29–244) | <0.001 | |
| HDL-cholesterol (mg/dL) | 46 (13–87) | 43 (17–92) | <0.001 | |
| Triglyceride (mg/dL) | 153 (47–1050) | 160 (50–856) | 0.74 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aktas, G. Association between the Prognostic Nutritional Index and Chronic Microvascular Complications in Patients with Type 2 Diabetes Mellitus. J. Clin. Med. 2023, 12, 5952. https://doi.org/10.3390/jcm12185952
Aktas G. Association between the Prognostic Nutritional Index and Chronic Microvascular Complications in Patients with Type 2 Diabetes Mellitus. Journal of Clinical Medicine. 2023; 12(18):5952. https://doi.org/10.3390/jcm12185952
Chicago/Turabian StyleAktas, Gulali. 2023. "Association between the Prognostic Nutritional Index and Chronic Microvascular Complications in Patients with Type 2 Diabetes Mellitus" Journal of Clinical Medicine 12, no. 18: 5952. https://doi.org/10.3390/jcm12185952
APA StyleAktas, G. (2023). Association between the Prognostic Nutritional Index and Chronic Microvascular Complications in Patients with Type 2 Diabetes Mellitus. Journal of Clinical Medicine, 12(18), 5952. https://doi.org/10.3390/jcm12185952