Catestatin—A Potential New Therapeutic Target for Women with Preeclampsia? An Analysis of Maternal Serum Catestatin Levels in Preeclamptic Pregnancies

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Patient Characteristics and Outcomes of the Study Population
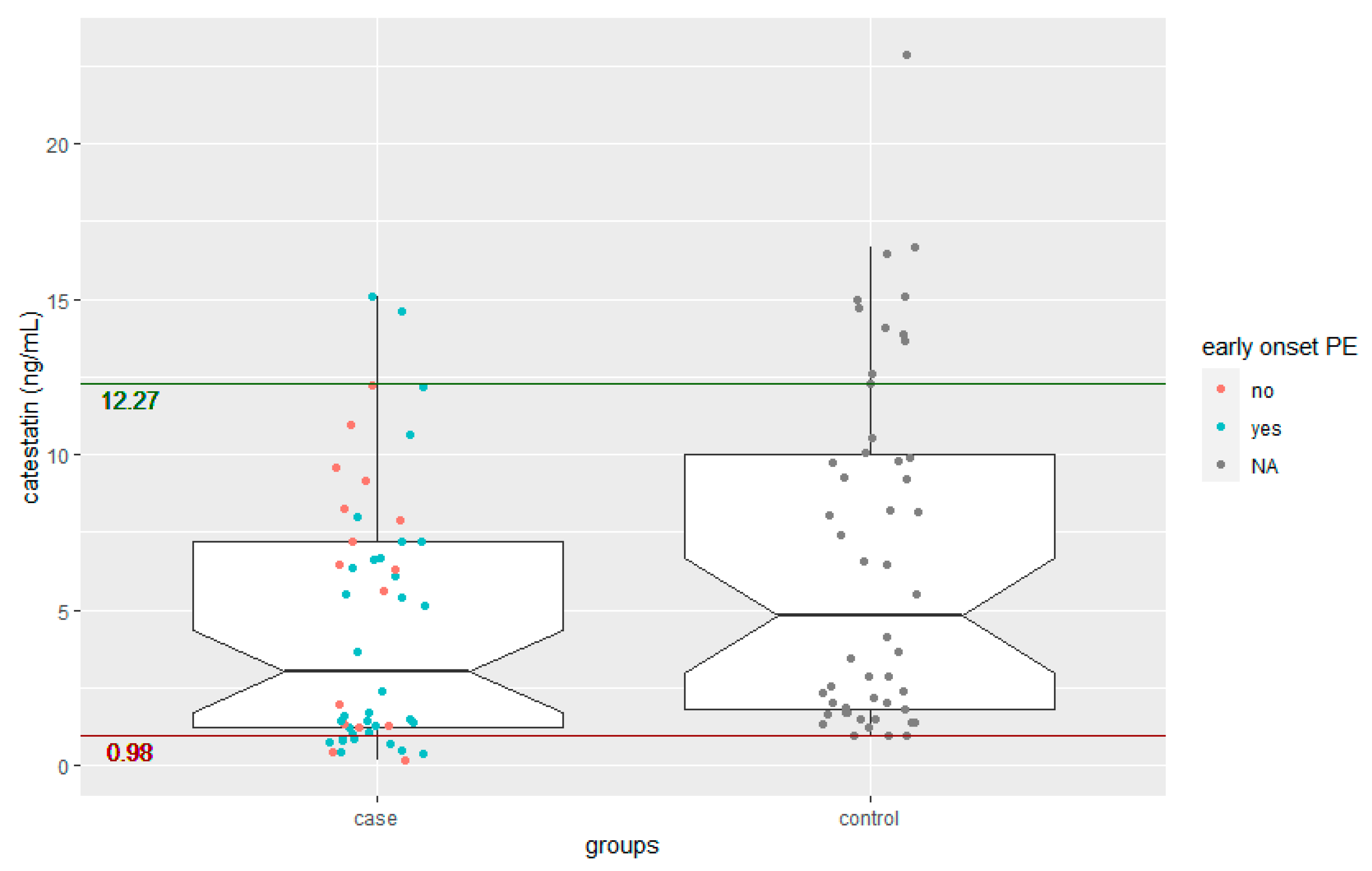
3.2. Catestatin Levels in Women with Preeclampsia
4. Discussion
4.1. Summary of the Key Findings
4.2. Interpretation of the Study Findings and Comparison with Existing Literature
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ARE | asymptotic relative efficiency |
| CgA | chromogranin A |
| CI | confidence interval |
| GA | gestational age |
| HDP | hypertensive disorders of pregnancy |
| IQR | interquartile range |
| IUD | intrauterine death |
| MAP | mean arterial pressure |
| NICU | neonatal intensive care unit |
| PlGF | placental growth factor |
| PE | preeclampsia |
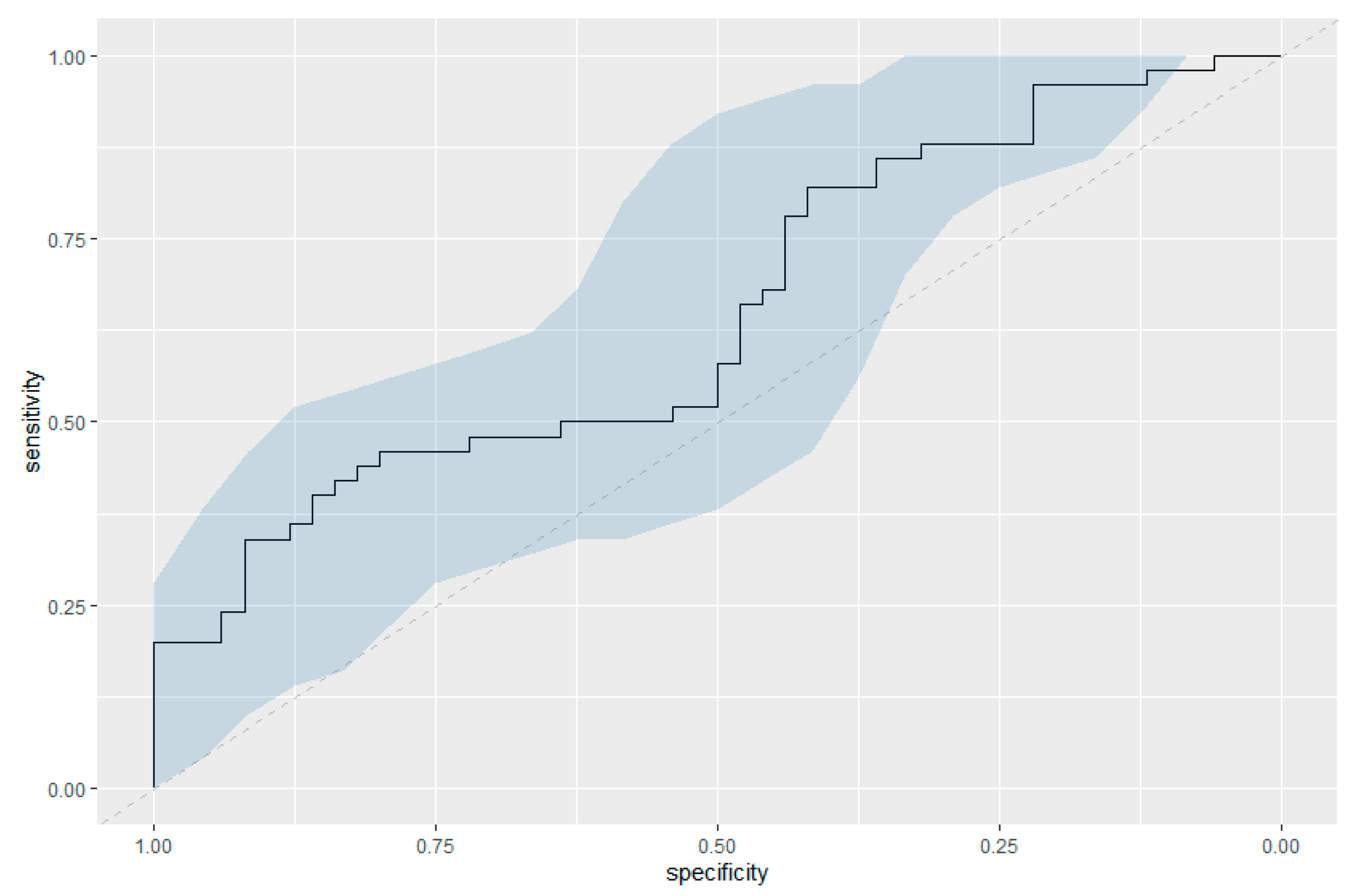
| ROC | receiver operating characteristic |
| SGA | small for gestational age |
| sFlt-1 | soluble fms-like tyrosine kinase-1 |
References
- Mol, B.W.J.; Roberts, C.T.; Thangaratinam, S.; Magee, L.A.; de Groot, C.J.M.; Hofmeyr, G.J. Pre-eclampsia. Lancet 2016, 387, 999–1011. [Google Scholar] [CrossRef]
- Ngoc, N.T.; Merialdi, M.; Abdel-Aleem, H.; Carroli, G.; Purwar, M.; Zavaleta, N.; Campódonico, L.; Ali, M.M.; Hofmeyr, G.J.; Mathai, M.; et al. Causes of stillbirths and early neonatal deaths: Data from 7993 pregnancies in six developing countries. Bull. World Health Organ. 2006, 84, 699–705. [Google Scholar] [CrossRef]
- Tranquilli, A.L.; Dekker, G.; Magee, L.; Roberts, J.; Sibai, B.M.; Steyn, W.; Zeeman, G.G.; Brown, M.A. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy Hypertens. 2014, 4, 97–104. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists; Task Force on Hypertension in Pregnancy. Hypertension in Pregnancy. Executive Summary. Obstet. Gynecol. 2013, 122, 1122–1131. [Google Scholar] [CrossRef] [PubMed]
- Melchiorre, K.; Giorgione, V.; Thilaganathan, B. The placenta and preeclampsia: Villain or victim? Am. J. Obstet. Gynecol. 2022, 226, S954–S962. [Google Scholar] [CrossRef]
- Masini, G.; Foo, L.F.; Tay, J.; Wilkinson, I.B.; Valensise, H.; Gyselaers, W.; Lees, C.C. Preeclampsia has two phenotypes which require different treatment strategies. Am. J. Obstet. Gynecol. 2022, 226, S1006–S1018. [Google Scholar] [CrossRef]
- Melchiorre, K.; Sutherland, G.R.; Liberati, M.; Thilaganathan, B. Preeclampsia Is Associated With Persistent Postpartum Cardiovascular Impairment. Hypertension 2011, 58, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Melchiorre, K.; Sutherland, G.; Sharma, R.; Nanni, M.; Thilaganathan, B. Mid-gestational maternal cardiovascular profile in preterm and term pre-eclampsia: A prospective study. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 496–504. [Google Scholar] [CrossRef]
- Melchiorre, K.; Sutherland, G.R.; Baltabaeva, A.; Liberati, M.; Thilaganathan, B. Maternal cardiac dysfunction and remodeling in women with preeclampsia at term. Hypertension 2011, 57, 85–93. [Google Scholar] [CrossRef]
- Melchiorre, K.; Sharma, R.; Thilaganathan, B. Cardiovascular implications in preeclampsia: An overview. Circulation 2014, 130, 703–714. [Google Scholar] [CrossRef]
- Brown, C.M.; Garovic, V.D. Drug treatment of hypertension in pregnancy. Drugs 2014, 74, 283–296. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.; Scholten, R.R.; Kingdom, J.C.; Floras, J.S.; Parker, J.D. Should Maternal Hemodynamics Guide Antihypertensive Therapy in Preeclampsia? Hypertension 2018, 71, 550–556. [Google Scholar] [CrossRef]
- Mahata, S.K.; O’Connor, D.T.; Mahata, M.; Yoo, S.H.; Taupenot, L.; Wu, H.; Gill, B.M.; Parmer, R.J. Novel autocrine feedback control of catecholamine release. A discrete chromogranin a fragment is a noncompetitive nicotinic cholinergic antagonist. J. Clin. Investig. 1997, 100, 1623–1633. [Google Scholar] [CrossRef]
- Theurl, M.; Schgoer, W.; Albrecht, K.; Jeschke, J.; Egger, M.; Beer, A.G.; Vasiljevic, D.; Rong, S.; Wolf, A.M.; Bahlmann, F.H.; et al. The neuropeptide catestatin acts as a novel angiogenic cytokine via a basic fibroblast growth factor-dependent mechanism. Circ. Res. 2010, 107, 1326–1335. [Google Scholar] [CrossRef] [PubMed]
- Helle, K.B. The chromogranin A-derived peptides vasostatin-I and catestatin as regulatory peptides for cardiovascular functions. Cardiovasc. Res. 2010, 85, 9–16. [Google Scholar] [CrossRef]
- Mahata, S.K.; Mahata, M.; Fung, M.M.; O’Connor, D.T. Catestatin: A multifunctional peptide from chromogranin A. Regul. Pept. 2010, 162, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, B.P.; Mahata, S.K.; O’Connor, D.T.; Ziegler, M.G. Mechanism of cardiovascular actions of the chromogranin A fragment catestatin in vivo. Peptides 1998, 19, 1241–1248. [Google Scholar] [CrossRef] [PubMed]
- Mahapatra, N.R.; O’Connor, D.T.; Vaingankar, S.M.; Hikim, A.P.; Mahata, M.; Ray, S.; Staite, E.; Wu, H.; Gu, Y.; Dalton, N.; et al. Hypertension from targeted ablation of chromogranin A can be rescued by the human ortholog. J. Clin. Investig. 2005, 115, 1942–1952. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, D.T.; Kailasam, M.T.; Kennedy, B.P.; Ziegler, M.G.; Yanaihara, N.; Parmer, R.J. Early decline in the catecholamine release-inhibitory peptide catestatin in humans at genetic risk of hypertension. J. Hypertens. 2002, 20, 1335–1345. [Google Scholar] [CrossRef] [PubMed]
- Zeisler, H.; Llurba, E.; Chantraine, F.; Vatish, M.; Staff, A.C.; Sennström, M.; Olovsson, M.; Brennecke, S.P.; Stepan, H.; Allegranza, D.; et al. Predictive Value of the sFlt-1:PlGF Ratio in Women with Suspected Preeclampsia. N. Engl. J. Med. 2016, 374, 13–22. [Google Scholar] [CrossRef]
- Herraiz, I.; Simón, E.; Gómez-Arriaga, P.I.; Martínez-Moratalla, J.M.; García-Burguillo, A.; Jiménez, E.A.; Galindo, A. Angiogenesis-Related Biomarkers (sFlt-1/PLGF) in the Prediction and Diagnosis of Placental Dysfunction: An Approach for Clinical Integration. Int. J. Mol. Sci. 2015, 16, 19009–19026. [Google Scholar] [CrossRef] [PubMed]
- Herraiz, I.; Llurba, E.; Verlohren, S.; Galindo, A. Update on the Diagnosis and Prognosis of Preeclampsia with the Aid of the sFlt-1/PlGF Ratio in Singleton Pregnancies. Fetal Diagn. Ther. 2018, 43, 81–89. [Google Scholar] [CrossRef]
- Llurba, E.; Crispi, F.; Verlohren, S. Update on the pathophysiological implications and clinical role of angiogenic factors in pregnancy. Fetal Diagn. Ther. 2015, 37, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Maynard, S.E.; Min, J.Y.; Merchan, J.; Lim, K.H.; Li, J.; Mondal, S.; Libermann, T.A.; Morgan, J.P.; Sellke, F.W.; Stillman, I.E.; et al. Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia. J. Clin. Investig. 2003, 111, 649–658. [Google Scholar] [CrossRef]
- Bralewska, M.; Biesiada, L.; Grzesiak, M.; Rybak-Krzyszkowska, M.; Huras, H.; Gach, A.; Pietrucha, T.; Sakowicz, A. Chromogranin A demonstrates higher expression in preeclamptic placentas than in normal pregnancy. BMC Pregnancy Childbirth 2021, 21, 680. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Fetal Growth Restriction: ACOG Practice Bulletin, Number 227. Obstet. Gynecol. 2021, 137, e16–e28. [Google Scholar] [CrossRef]
- Kaplan, S.H. Asymptotic relative efficiency. Am. J. Occup. Ther. 1986, 40, 433. [Google Scholar] [CrossRef][Green Version]
- Melchiorre, K.; Thilaganathan, B.; Giorgione, V.; Ridder, A.; Memmo, A.; Khalil, A. Hypertensive Disorders of Pregnancy and Future Cardiovascular Health. Front. Cardiovasc. Med. 2020, 7, 59. [Google Scholar] [CrossRef] [PubMed]
- Mahata, S.K.; Kiranmayi, M.; Mahapatra, N.R. Catestatin: A Master Regulator of Cardiovascular Functions. Curr. Med. Chem. 2018, 25, 1352–1374. [Google Scholar] [CrossRef] [PubMed]
- Tüten, N.; Güralp, O.; Gök, K.; Hamzaoglu, K.; Oner, Y.O.; Makul, M.; Bulut, H.; Irmak, K.; Tüten, A.; Malik, E. Serum catestatin level is increased in women with preeclampsia. J. Obstet. Gynaecol. 2021, 42, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Özalp, M.; Yaman, H.; Demir, Ö.; Aytekin Garip, S.; Aran, T.; Osmanağaoğlu, M.A. The role of maternal serum catestatin in the evaluation of preeclampsia and fetal cardiac functions. Turk. J. Obstet. Gynecol. 2021, 18, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Valensise, H.; Vasapollo, B.; Gagliardi, G.; Novelli, G.P. Early and Late Preeclampsia. Hypertension 2008, 52, 873–880. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All (n = 100) | Preeclampsia (n = 50) | Control (n = 50) | p-Value | |
|---|---|---|---|---|
| Maternal age in years, median (IQR) | 30.5 (26.00–36.00) | 33 (27.25–37.00) | 29.5 (26.00–34.00) | 0.0576 |
| BMI at booking, kg/m2, median (IQR) | 27.3 (24.20–31.68) | 29.4 (25.88–34.05) | 26.05 (23.53–29.08) | 0.002 |
| nulliparity, n (%) | 51 (51%) | 32 (64%) | 19 (38%) | 0.0164 |
| Catestatin in ng/mL, median (IQR) | 3.92 (1.43–9.18) | 3.03 (1.24–7.21) | 4.82 (1.82–10.02) | 0.01 |
| MAP at sampling in mmHg, median (IQR) | 104.00 (83.50–128.84) | 128.00 (114.25–135.5) | 83.33 (76.67–87.33) | <0.0001 |
| GA at sampling in weeks, median (IQR) | 31.89 (27.36–34.86) | 32 (28–34.96) | 31.93 (27.04–34.57) | 0.607 |
| GA at delivery in weeks, median (IQR) | 37.57 (32.89–39.71) | 32.79 (28.93–36.11) | 39.71 (38.57–40.00) | <0.0001 |
| Delivery before 37 weeks of gestation | 42 (42%) | 41 (82%) | 1 (2%) | <0.0001 |
| SGA, n (%) | 33 (32%) | 31 (62%) | 2 (4%) | <0.0001 |
| Birthweight centile, median (IQR) | 30.00 (5.00–58.00) | 6.00 (2.00–18.75) | 52.00 (32.50–76.75) | 0.0191 |
| Mode of delivery | ||||
| Vaginal delivery, n (%) | 37 (37%) | 3 (9%) | 30 (60%) | 0.1006 |
| Primary cesarean, n (%) | 54 (54%) | 30 (88%) | 14 (28%) | |
| Secondary cesarean, n (%) | 9 (9%) | 1 (3%) | 6 (12%) | |
| Pregnancy outcome | ||||
| Live birth, n (%) | 96 (96%) | 30 (88%) | 50 (100%) | 0.042 |
| IUD, n (%) | 1 (1%) | 1 (3%) | 0 (0%) | |
| NND < 1 week postpartum, n (%) | 3 (3%) | 3 (9%) | 0 (0%) | |
| NICU admission, n (%) | 32 (32%) | 31 (94%) | 0 (0%) | <0.0001 |
| Maternal age in years, median (IQR) | 30.5 (26.00–36.00) | 33 (27.25–37.00) | 29.5 (26.00–34.00) | 0.0576 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmrich, P.; Schirwani-Hartl, N.; Haberl, C.; Haslinger, P.; Heinzl, F.; Zeisler, H.; Binder, J. Catestatin—A Potential New Therapeutic Target for Women with Preeclampsia? An Analysis of Maternal Serum Catestatin Levels in Preeclamptic Pregnancies. J. Clin. Med. 2023, 12, 5931. https://doi.org/10.3390/jcm12185931
Palmrich P, Schirwani-Hartl N, Haberl C, Haslinger P, Heinzl F, Zeisler H, Binder J. Catestatin—A Potential New Therapeutic Target for Women with Preeclampsia? An Analysis of Maternal Serum Catestatin Levels in Preeclamptic Pregnancies. Journal of Clinical Medicine. 2023; 12(18):5931. https://doi.org/10.3390/jcm12185931
Chicago/Turabian StylePalmrich, Pilar, Nawa Schirwani-Hartl, Christina Haberl, Peter Haslinger, Florian Heinzl, Harald Zeisler, and Julia Binder. 2023. "Catestatin—A Potential New Therapeutic Target for Women with Preeclampsia? An Analysis of Maternal Serum Catestatin Levels in Preeclamptic Pregnancies" Journal of Clinical Medicine 12, no. 18: 5931. https://doi.org/10.3390/jcm12185931
APA StylePalmrich, P., Schirwani-Hartl, N., Haberl, C., Haslinger, P., Heinzl, F., Zeisler, H., & Binder, J. (2023). Catestatin—A Potential New Therapeutic Target for Women with Preeclampsia? An Analysis of Maternal Serum Catestatin Levels in Preeclamptic Pregnancies. Journal of Clinical Medicine, 12(18), 5931. https://doi.org/10.3390/jcm12185931