

Human Albumin Infusion in Critically Ill and Perioperative Patients: Narrative Rapid Review of Meta-Analyses from the Last Five Years

Abstract
:1. Introduction
2. Materials and Methods
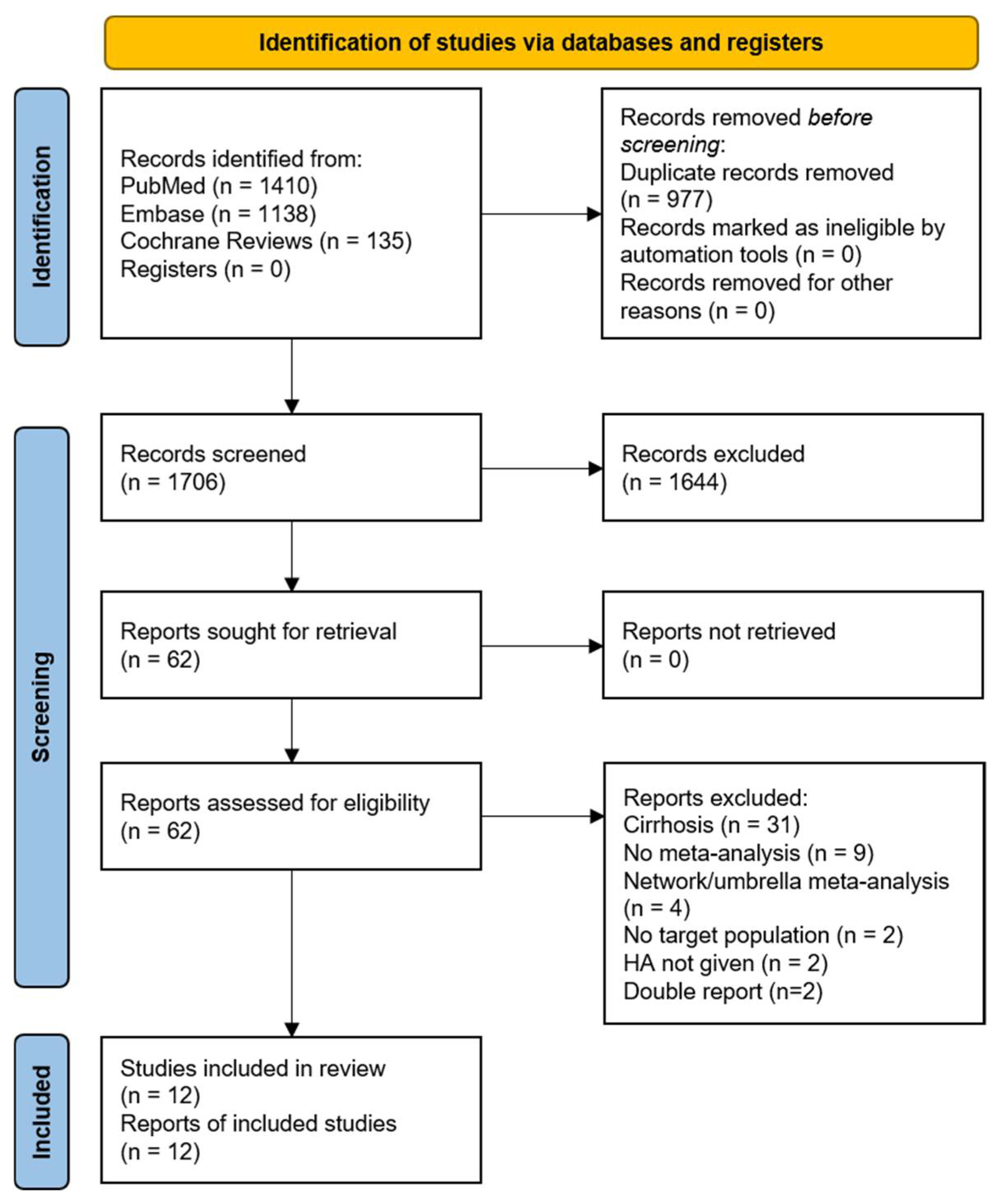
2.1. Search Strategy
2.2. Study Selection and Data Extraction
2.3. Methodological Quality Assessment
2.4. Level of Evidence
- Convincing evidence: (1) statistical significance at p < 0.001; (2) no small study effects or large between-study heterogeneity; and (3) concordance between the effect estimate of the largest study and the summary effect of the random-effects meta-analyses.
- Suggestive evidence: (1) statistical significance of random effects at p < 0.05; (2) 95% PI included the null hypothesis; and (3) no small study effects or large between-study heterogeneity.
- Weak evidence: (1) statistical significance of random effects at p < 0.05; (2) small study effects or large between-study heterogeneity were found.
- Non-significant association: There was no statistical significance for the random effect of the meta-analysis (p > 0.05).
3. Results
3.1. Major Findings from Meta-Analyses
3.1.1. Critical Illness
3.1.2. Sepsis
3.1.3. Cardiac Surgery
3.1.4. Diuretic Response
3.1.5. Acute Brain Injury
3.1.6. Hypoalbuminemia, Burns, and Kidney Replacement Therapy
3.2. Methodological Quality of Meta-Analyses
- A meta-analysis by Lewis et al. [23] combined HA and fresh frozen plasma as natural colloids despite their significant pharmacological differences, which may confound the interpretation of the results, indicating that the choice between colloids and crystalloids does not significantly impact mortality.
- A meta-analysis by Lee et al. [18] from Taiwan focused on patients receiving diuretic therapy. The effectiveness of combination therapy was influenced by factors such as baseline serum albumin levels, prescribed HA infusion doses, and renal function.
- In the second ‘low-quality’ meta-analysis by Zou et al. [15], the use of HA was compared with crystalloids in a larger number of patients with septic shock. As described, the analysis did not find a decrease in all-cause mortality in patients treated with HA compared to those treated with crystalloids.
3.3. Level of Evidence of Human Albumin Associations with Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Horváthy, D.B.; Simon, M.; Schwarz, C.M.; Masteling, M.; Vácz, G.; Hornyák, I.; Lacza, Z. Serum Albumin as a Local Therapeutic Agent in Cell Therapy and Tissue Engineering. BioFactors 2017, 43, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.C.; Deutschman, C.S. The Multiple Organ Dysfunction Syndrome: Syndrome, Metaphor, and Unsolved Clinical Challenge. Crit. Care Med. 2021, 49, 1402–1413. [Google Scholar] [CrossRef] [PubMed]
- Gatta, A.; Verardo, A.; Bolognesi, M. Hypoalbuminemia. Intern. Emerg. Med. 2012, 7 (Suppl. S3), S193–S199. [Google Scholar] [CrossRef]
- Vincent, J.-L.; Dubois, M.-J.; Navickis, R.J.; Wilkes, M.M. Hypoalbuminemia in Acute Illness: Is There a Rationale for Intervention? A Meta-Analysis of Cohort Studies and Controlled Trials. Ann. Surg. 2003, 237, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Mayerhöfer, T.; Wiedermann, C.J.; Joannidis, M. Use of albumin: State of the art. Med. Klin. Intensivmed. Notfmed 2021, 116, 655–664. [Google Scholar] [CrossRef]
- Vincent, J.L.; De Backer, D.; Wiedermann, C.J. Fluid Management in Sepsis: The Potential Beneficial Effects of Albumin. J. Crit. Care 2016, 35, 161–167. [Google Scholar] [CrossRef]
- Garcia-Martinez, R.; Caraceni, P.; Bernardi, M.; Gines, P.; Arroyo, V.; Jalan, R. Albumin: Pathophysiologic Basis of Its Role in the Treatment of Cirrhosis and Its Complications. Hepatology 2013, 58, 1836–1846. [Google Scholar] [CrossRef]
- Bernardi, M.; Angeli, P.; Claria, J.; Moreau, R.; Gines, P.; Jalan, R.; Caraceni, P.; Fernandez, J.; Gerbes, A.L.; O’Brien, A.J.; et al. Albumin in Decompensated Cirrhosis: New Concepts and Perspectives. Gut 2020, 69, 1127–1138. [Google Scholar] [CrossRef]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the Management of Patients with Decompensated Cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef]
- HakanSaner, F.; Stueben, B.-O.; Hoyer, D.P.; Broering, D.C.; Bezinover, D. Use or Misuse of Albumin in Critical Ill Patients. Diseases 2023, 11, 68. [Google Scholar]
- Cook, D.J.; Mulrow, C.D.; Haynes, R.B. Systematic Reviews: Synthesis of Best Evidence for Clinical Decisions. Ann. Intern. Med. 1997, 126, 376–380. [Google Scholar] [CrossRef] [PubMed]
- Hamel, C.; Michaud, A.; Thuku, M.; Skidmore, B.; Stevens, A.; Nussbaumer-Streit, B.; Garritty, C. Defining Rapid Reviews: A Systematic Scoping Review and Thematic Analysis of Definitions and Defining Characteristics of Rapid Reviews. J. Clin. Epidemiol. 2021, 129, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.S.; Bassett, P. Crystalloids vs. Colloids for Fluid Resuscitation in the Intensive Care Unit: A Systematic Review and Meta-Analysis. J. Crit. Care 2019, 50, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A Critical Appraisal Tool for Systematic Reviews That Include Randomised or Non-Randomised Studies of Healthcare Interventions, or Both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef]
- Zou, Y.; Ma, K.; Xiong, J.B.; Xi, C.H.; Deng, X.J. Comparison of the Effects of Albumin and Crystalloid on Mortality among Patients with Septic Shock: Systematic Review with Meta-Analysis and Trial Sequential Analysis. Sao Paulo Med. J. Rev. Paul. Med. 2018, 136, 421–432. [Google Scholar] [CrossRef]
- Geng, L.; Tian, X.; Gao, Z.; Mao, A.; Feng, L.; He, C. Different Concentrations of Albumin Versus Crystalloid in Patients with Sepsis and Septic Shock: A Meta-Analysis of Randomized Clinical Trials. J. Intensive Care Med. 2023, 38, 679–689. [Google Scholar] [CrossRef]
- Wei, L.; Li, D.; Sun, L. The Comparison of Albumin and 6% Hydroxyethyl Starches (130/0.4) in Cardiac Surgery: A Meta-Analysis of Randomized Controlled Clinical Trials. BMC Surg. 2021, 21, 342. [Google Scholar] [CrossRef]
- Lee, T.H.; Kuo, G.; Chang, C.H.; Huang, Y.T.; Yen, T.H.; Lee, C.-C.; Fan, P.C.; Chen, J.-J. Diuretic Effect of Co-Administration of Furosemide and Albumin in Comparison to Furosemide Therapy Alone: An Updated Systematic Review and Meta-Analysis. PLoS ONE 2021, 16, e0260312. [Google Scholar] [CrossRef]
- Huang, Y.; Xiao, Z. Albumin Therapy for Acute Ischemic Stroke: A Meta-Analysis. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 2021, 42, 2713–2719. [Google Scholar] [CrossRef]
- Itagaki, Y.; Yoshida, N.; Banno, M.; Momosaki, R.; Yamada, K.; Hayakawa, M. Efficacy of Albumin with Diuretics in Mechanically Ventilated Patients with Hypoalbuminemia: A Systematic Review and Meta-Analysis. Medicine 2022, 101, e30276. [Google Scholar] [CrossRef]
- Keshavarz, H.; Skubas, N.; Callum, J.; Fergusson, D.; Wu, B. Shehata Intravenous Albumin in Adult Cardiac Surgery: A Meta-Analysis. Vox Sang. 2021, 116, 183. [Google Scholar] [CrossRef]
- Chamarthi, G.; Loy, J.L.; Norton, H.F.; Bejjanki, H.; Mohandas, R. Is There a Role for Concomitant Administration of Albumin and Diuretics? A Meta-Analysis. J. Am. Soc. Nephrol. 2019, 30, 614. [Google Scholar]
- Lewis, S.R.; Pritchard, M.W.; Evans, D.J.; Butler, A.R.; Alderson, P.; Smith, A.F.; Roberts, I. Colloids versus Crystalloids for Fluid Resuscitation in Critically Ill People. Cochrane Database Syst. Rev. 2018, 8, CD000567. [Google Scholar] [CrossRef]
- Siemens, K.; Donnelly, P.; Hunt, B.J.; Carter, M.J.; Murdoch, I.A.; Tibby, S.M. Evaluating the Impact of Cardiopulmonary Bypass Priming Fluids on Bleeding after Pediatric Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Cardiothorac. Vasc. Anesth. 2022, 36, 1584–1594. [Google Scholar] [CrossRef]
- Wiedermann, C.J. Use of Hyperoncotic Human Albumin Solution in Severe Traumatic Brain Injury Revisited—A Narrative Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2662. [Google Scholar] [CrossRef]
- Schmidt, A.P.; Bilotta, F. Hydroxyethyl Starch for Perioperative Fluid Management: A Critical Appraisal. Braz. J. Anesthesiol. 2023. epub ahead of printing. [Google Scholar] [CrossRef] [PubMed]
- Oddo, M.; Poole, D.; Helbok, R.; Meyfroidt, G.; Stocchetti, N.; Bouzat, P.; Cecconi, M.; Geeraerts, T.; Martin-Loeches, I.; Quintard, H.; et al. Fluid Therapy in Neurointensive Care Patients: ESICM Consensus and Clinical Practice Recommendations. Intensive Care Med. 2018, 44, 449–463. [Google Scholar] [CrossRef]
- Wiedermann, C.J. Phases of Fluid Management and the Roles of Human Albumin Solution in Perioperative and Critically Ill Patients. Curr. Med. Res. Opin. 2020, 36, 1961–1973. [Google Scholar] [CrossRef]
- Wiedermann, C.J. Moderator Effect of Hypoalbuminemia in Volume Resuscitation and Plasma Expansion with Intravenous Albumin Solution. Int. J. Mol. Sci. 2022, 23, 14175. [Google Scholar] [CrossRef]
- Cartotto, R.; Callum, J. A Review of the Use of Human Albumin in Burn Patients. J. Burn. Care Res. 2012, 33, 702–717. [Google Scholar] [CrossRef]
- Macedo, E.; Karl, B.; Lee, E.; Mehta, R.L. A Randomized Trial of Albumin Infusion to Prevent Intradialytic Hypotension in Hospitalized Hypoalbuminemic Patients. Crit. Care 2021, 25, 18. [Google Scholar] [CrossRef] [PubMed]
- Wiedermann, C.J. Human Albumin and 6% Hydroxyethyl Starches (130/0.4) in Cardiac Surgery: A Meta-Analysis Revisited. BMC Surg. 2022, 22, 140. [Google Scholar] [CrossRef] [PubMed]
- Joannidis, M.; Wiedermann, C.J.; Ostermann, M. Ten Myths about Albumin. Intensive Care Med. 2022, 48, 602–605. [Google Scholar] [CrossRef] [PubMed]
- Gomez, H.; Priyanka, P.; Bataineh, A.; Keener, C.M.; Clermont, G.; Kellum, J.A. Effects of 5% Albumin plus Saline versus Saline Alone on Outcomes from Large-Volume Resuscitation in Critically Ill Patients. Crit. Care Med. 2020, 49, 79–90. [Google Scholar] [CrossRef]
- Finfer, S.; Bellomo, R.; Boyce, N.; French, J.; Myburgh, J.; Norton, R. Safe Study Investigators A Comparison of Albumin and Saline for Fluid Resuscitation in the Intensive Care Unit. N. Engl. J. Med. 2004, 350, 2247–2256. [Google Scholar] [CrossRef] [PubMed]
- Caironi, P.; Tognoni, G.; Masson, S.; Fumagalli, R.; Pesenti, A.; Romero, M.; Fanizza, C.; Caspani, L.; Faenza, S.; Grasselli, G.; et al. Albumin Replacement in Patients with Severe Sepsis or Septic Shock. N. Engl. J. Med. 2014, 370, 1412–1421. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensiv. Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico. Efficacy of Albumin Replacement and Balanced Solution in Patients with Septic Shock (the ALBIOSS-BALANCED Trial): A 2-by-2 Factorial, Investigator-Initiated, Open- Label, Multicenter, Randomized, Controlled Trial. 2021. Available online: https://clinicaltrials.gov/ (accessed on 9 September 2023).
- Navickis, R.J.; Haynes, G.R.; Wilkes, M.M. Effect of Hydroxyethyl Starch on Bleeding after Cardiopulmonary Bypass: A Meta-Analysis of Randomized Trials. J. Thorac. Cardiovasc. Surg. 2012, 144, 223–230. [Google Scholar] [CrossRef]
- Talvasto, A.; Ilmakunnas, M.; Raivio, P.; Vlasov, H.; Hiippala, S.; Suojaranta, R.; Wilkman, E.; Petäjä, L.; Helve, O.; Juvonen, T.; et al. Albumin Infusion and Blood Loss After Cardiac Surgery. Ann. Thorac. Surg. 2023, 116, 392–399. [Google Scholar] [CrossRef]
- Skhirtladze, K.; Base, E.M.; Lassnigg, A.; Kaider, A.; Linke, S.; Dworschak, M.; Hiesmayr, M.J. Comparison of the Effects of Albumin 5%, Hydroxyethyl Starch 130/0.4 6%, and Ringer’s Lactate on Blood Loss and Coagulation after Cardiac Surgery. Br. J. Anaesth. 2014, 112, 255–264. [Google Scholar] [CrossRef]
- Kheirabadi, B.S.; Miranda, N.; Terrazas, I.B.; Gonzales, M.D.; Grimm, R.C.; Dubick, M.A. Does Small-Volume Resuscitation with Crystalloids or Colloids Influence Hemostasis and Survival of Rabbits Subjected to Lethal Uncontrolled Hemorrhage? J. Trauma. Acute Care Surg. 2017, 82, 156–164. [Google Scholar] [CrossRef]
- Wilcox, C.S.; Testani, J.M.; Pitt, B. Pathophysiology of Diuretic Resistance and Its Implications for the Management of Chronic Heart Failure. Hypertension 2020, 76, 1045–1054. [Google Scholar] [PubMed]
- Zampieri, F.G.; Machado, F.R.; Biondi, R.S.; Freitas, F.G.R.; Veiga, V.C.; Figueiredo, R.C.; Lovato, W.J.; Amêndola, C.P.; Serpa-Neto, A.; Paranhos, J.L.R.; et al. Effect of Intravenous Fluid Treatment With a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial. JAMA 2021, 326, 818–829. [Google Scholar] [CrossRef]
- Cooper, D.J.; Myburgh, J.; Heritier, S.; Finfer, S.; Bellomo, R.; Billot, L.; Murray, L.; Vallance, S.; SAFE-TBI Investigators. Australian and New Zealand Intensive Care Society Clinical Trials Group Albumin Resuscitation for Traumatic Brain Injury: Is Intracranial Hypertension the Cause of Increased Mortality? J. Neurotrauma 2013, 30, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Iguchi, N.; Kosaka, J.; Bertolini, J.; May, C.N.; Lankadeva, Y.R.; Bellomo, R. Differential Effects of Isotonic and Hypotonic 4% Albumin Solution on Intracranial Pressure and Renal Perfusion and Function. Crit. Care Resusc. J. Australas. Acad. Crit. Care Med. 2018, 20, 48–53. [Google Scholar]

{kind=link}
| Study | Year | Country | Population | Trials | Patients | Intervention vs. Comparison | Outcomes | Results | Methodological Quality * |
|---|---|---|---|---|---|---|---|---|---|
| Critical Illness | |||||||||
| Lewis et al. [23] | 2018 | United Kingdom | Critically ill receiving fluid volume replacement in hospital or emergency out-of-hospital settings | 22 | 13,047 | Natural colloids (HA and FFP) vs. crystalloid (isotonic or hypertonic) | Mortality, need for blood transfusion, need for KRT | Little or no difference in mortality, little or no difference in need for KRT, uncertain evidence for blood transfusions. | High |
| Martin and Bassett [13] | 2019 | United States | Critically ill receiving fluid resuscitation in intensive care units | 18 | 10,600 | HA vs. crystalloid | Hemodynamics (MAP, CVP, CI) at end of fluid challenge), mortality | HA more efficient than crystalloids at stabilizing resuscitation endpoints. | Critically low |
| Itagaki et al. [20] | 2022 | Japan | Critically ill with hypoalbuminemia receiving mechanical ventilation | 3 | 129 | HA with diuretics vs. placebo or no diuretics | Hypotensive events, duration of mechanical ventilation, all-cause mortality | Reduced number of days on mechanical ventilation, reduced hypotensive events, and improved P/F ratio at 24 h, no effect on all-cause mortality at 30 days. | Low |
| Sepsis | |||||||||
| Zou et al. [15] | 2018 | China | Septic shock | 6 | 3088 | HA vs. crystalloid | Mortality | No decrease in all-cause mortality, according to trial sequential analysis, could be false negative. | Low |
| Geng et al. [16] | 2023 | China | Severe sepsis or septic shock | 8 | 8606 | HA vs. crystalloid | Mortality | Trend toward reduced 90-day mortality of septic patients, significantly reduced mortality of septic shock patients, particularly with 20% HA. | Critically low |
| Cardiothoracic surgery | |||||||||
| Keshavarz et al. [21] | 2021 | Canada | Adult cardiothoracic surgery | 48 | n.d. | HA vs. no HA or alternative solutions for infusion or bypass prime | Mortality, kidney failure, hospital LOS, ICU LOS, blood loss | No effects on mortality, kidney failure, hospital LOS, ICU LOS, and blood loss. | Critically low |
| Siemens et al. [24] | 2022 | United Kingdom | Pediatric cardiac surgery | 12 | 881 | HA vs. FFP, HES, crystalloids, gelatin, or HA (lower concentration) as alternative solution for cardiopulmonary bypass prime | Blood loss, transfusion requirement, coagulation parameters, ventilation duration, ICU LOS, hospital LOS, mortality | No differences in blood loss (other outcomes not assessed because of heterogeneity risk of bias). | Critically low |
| Wei et al. [17] | 2021 | China | Adult cardiac surgery | 10 | 1567 | HA vs. 6% HES 130/0.4 | Mortality, AKI, KRT, hospital LOS, ICU LOS, blood loss, transfusion requirement, volume of infusion | Higher blood loss in HA group, no differences in transfusion requirement or other outcomes. | Critically low |
| Diuretic Resistance | |||||||||
| Chamarthi et al. [22] | 2019 | United States | Diuretic therapy in hypoalbuminemia | 9 | n.d. | HA plus diuretic vs. diuretic alone | Urine output, sodium excretion | Increased urine volume in HA group at 8 h, no difference after 24 h. | Critically low |
| Lee et al. [18] | 2021 | Taiwan | Diuretic therapy | 13 | 422 | HA plus diuretic vs. diuretic alone | Urine output, sodium excretion | Enhanced diuresis and natriuresis with advantages with baseline serum albumin levels lower than 2.5 g/dL, higher HA doses, and impaired renal function. | High |
| Acute Brain Injury | |||||||||
| Huang et al. [19] | 2021 | China | Ischemic stroke | 4 | 1611 | HA during the acute phase vs. no HA | Neurological outcome | No beneficial effect on the long-term neurological function, risk of pulmonary edema. | Critically low |
| Wiedermann [25] | 2022 | Italy | Severe TBI | 4 | 320 | ICP-targeted HA vs. CPP-targeted or standard therapy with no HA | Mortality | Reduced mortality but high risk of bias. | Critically low |
| Type of Patients | Outcome | Study | Type of Study | Studies | Patients (Intervention/Comparator) | Type of Metrics | Effect Size (95% CI) | Effect Size p–Value | Heterogeneity p–Value (I2) | Egger | Small Study Effect | Effect Size Concordance with Largest Study |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-significant association (p > 0.05) | ||||||||||||
| Critically ill | Mortality | Lewis et al. [23] | RCT | 20 | 6021/7026 | random | 0.98 (0.92, 1.06) $ | 0.63 | 0.38 (6.61) | n.d. | no | n.a. |
| Martin and Bassett [13] | RCT | 14 | 5240/5240 | random | 1.02 (0.96, 1.10) & | 0.49 | 0.60 (0) | 0.25 | no | n.a. | ||
| Renal (kidney failure) | Lewis et al. [23] | RCT | 2 | 1506/1522 | random | 1.11 (0.96, 1.27) $ | 0.15 | 0.45 (0) | n.d. | n.d. | n.a. | |
| Transfusion | Lewis et al. [23] | RCT | 3 | 130/160 | random | 1.31 (0.95; 1.80) & | 0.10 | 0.56 (0) | n.d. | n.d. | n.a. | |
| Infusion Volume | Martin and Bassett [13] | RCT | 5 | 555/566 | random | 1985 (−401, 4372) ‡ | 0.10 | <0.001 (94) | 0.31 | no | n.a. | |
| Septic shock | Mortality | Zou et al. [15] | RCT | 6 | 1282/1806 | random | 0.91 (0.83, 1.00) | 0.05 | 0.63 (0) | n.d. | n.d. | n.a. |
| Sepsis | Mortality | Geng et al. [16] | RCT | 8 | 2302/2808 | fixed | 0.91 (0.80, 1.02) & | 0.11 | 0.64 (0) | n.d. | n.d. | n.a. |
| Surgery | Mortality | Keshavarz et al. [21] | RCT | 8 | 606/617 | random | 0.01 (−0.01, 0.02) † | n.d. | n.d. | n.d. | n.d. | n.a. |
| Wei et al. [17] | RCT | 3 | 163/171 | fixed | 0.56 (0.16, 2.02) & | 0.46 | 0.41 (0) | n.d. | n.d. | n.a. | ||
| Renal (kidney failure) | Keshavarz et al. [21] | RCT | 3 | 169/170 | random | −0.03 (−0.22, 0.15) † | n.d. | n.d. | n.d. | n.d. | n.a. | |
| Renal (AKI) | Wei et al. [17] | RCT | 2 | 90/87 | random | 1.25 (1.00, 1.75) $ | 0.05 | 0.99 (0) | n.d. | n.d. | n.a. | |
| Renal (KRT) | Wei et al. [17] | RCT | 2 | 148/150 | random | 0.67 (0.08, 5.75) $ | 0.72 | 0.18 (44) | n.d. | n.d. | n.a. | |
| LOS (hospital) | Keshavarz et al. [21] | RCT | 9 | 510/529 | random | −0.04 (−0.20, 0.12) ‡ | n.d. | n.d. | n.d. | n.d. | n.a. | |
| Wei et al. [17] | RCT | 4 | 172/176 | fixed | −0.11 (−0.32, 0.10) ‡ | 0.32 | 0.33 (13) | n.d. | n.d. | n.a. | ||
| LOS (ICU) | Keshavarz et al. [21] | RCT | 4 | 250/259 | random | 0.02 (−0.20, 0.24) ‡ | n.d. | n.d. | n.d. | n.d. | n.a. | |
| Wei et al. [17] | RCT | 6 | 235/243 | fixed | −0.18 (−0.36, 0.00) ‡,§ | 0.05 § | 0.59 (0) | n.d. | n.d. | n.a. | ||
| Blood loss | Keshavarz et al. [21] | RCT | 10 | 515/543 | random | −0.16 (−0.34, 0.01) ‡ | n.d. | n.d. | n.d. | n.d. | n.a. | |
| Siemens et al. [24] | RCT | 2 | 100/116 | random | 4.51 (−1.18,10.19) | 0.12 | 0.03 (80) | n.d. | n.d. | n.a. | ||
| Transfusion | Wei et al. [17] | RCT | 7 | 287/292 | fixed | 1.11 (0.95, 1.27) $ | 0.20 | 0.19 (31) | n.d. | n.d. | n.a. | |
| Infusion volume | Wei et al. [17] | RCT | 7 | 284/295 | fixed | 0.04 (−0.12, 0.20) ‡ | 0.64 | 0.50 (0) | n.d. | n.d. | n.a. | |
| Mechanical ventilation (hypoalbuminemia) | Mortality | Itagaki et al. [20] | RCT | 3 | 66/63 | random | 1.00 (0.45; 1.23) $ | 1.00 | 0.30 (17) | n.d. | n.d. | n.a. |
| Duration of ventilation | Itagaki et al. [20] | RCT | 2 | 46/43 | fixed | −0.34 (1.00; 1.31) $ | 0.69 | 0.45 (0) | n.d. | n.d. | n.a. | |
| Ischemic stroke | Neurological outcome | Huang et al. [19] | RCT | 4 | 807/804 | fixed | 1.04 (0,85; 1.27) & | 0.72 | 0.65 (0) | n.d. | n.d. | n.a. |
| Diuretic resistance | Urine output (ml increase at 24 h) | Chamarthi et al. [22] | n.d. | 9 | n.d. | n.d. | 385 (−141.92, 911.68) ‡ | n.d. | n.d. | n.d. | n.d. | n.a. |
| Weak evidence (p < 0.05, significant heterogeneity p < 0.05) | ||||||||||||
| Critically ill | Hemodynamics (MAP max) | Martin and Bassett [13] | RCT | 6 | 5175/3774 | random | −3.5 (−6.71, −0.36) ‡ | <0.001 | <0.001 (91) | 0.21 | no | n.a. |
| Hemodynamics (CVP max) | Martin and Bassett [13] | RCT | 7 | 5187/3786 | random | −2.0 (−3.0, −1.1) ‡ | <0.001 | <0.001 (82) | 0.10 | no | n.a. | |
| Diuretic resistance | Urine output (ml increase per hour) | Lee et al. [18] | RCT | 14 | 223/220 | random | 31.45 (19.30, 43.59) | n.d. | <0.01 (87) | n.d. | no | n.a. |
| Urine output (ml increase at 8 h) | Chamarthi et al. [22] | n.d. | 9 | n.d. | n.d. | 315 (183.04, 448.33) ‡ | n.d. | n.d. | n.d. | n.d. | n.a. | |
| Sodium excretion (meq increase, 8 h) | Chamarthi et al. [22] | n.d. | 9 | n.d. | n.d. | 27 (7.46, 46.59) ‡ | n.d. | n.d. | n.d. | n.d. | n.a. | |
| Sodium excretion (meq increase per hour) | Lee et al. [18] | RCT | 11 | 233/233 | random | 1.76 (0.83, 2.69) | n.d. | <0.01 (92) | n.d. | no | n.t. | |
| Suggestive evidence (effect size p < 0.05, I2 p-value > 0.05) | ||||||||||||
| Septic shock | Mortality | Geng et al. [16] | RCT | 7 | 1488/1994 | fixed | 0.85 (0.74, 0.99) & | 0.04 | 0.60 (0) | n.d. | n.d. | yes |
| Severe TBI | Mortality | Wiedermann [25] | OBS/RCT | 1/3 | 165/155 | random | 0.42 (0.24; 0.73) $ | 0.002 | 0.18 (38.6) | 0.65 | n.d. | yes |
| Surgery | Blood loss | Wei et al. [17] | RCT | 6 | 216/222 | fixed | 0.22 (0.03, 0.41) ‡ | 0.02 | 0.60 (0) | n.d. | no | yes |
| Mechanical ventilation (hypoalbuminemia) | Hypotensive events | Itagaki et al. [20] | RCT | 3 | 66/63 | random | 0.34 (0.15; 0.81) $ | 0.01 | 0.91 (0) | n.d. | n.d. | yes |
| Convincing evidence (p < 0.001, no heterogeneity, concordance between the effect estimate of the largest study and the summary effect of the random-effects meta-analyses) | ||||||||||||
| Critically ill | Cardiac index (end of fluid challenge) | Martin and Bassett [13] | RCT | 7 | 130/132 | random | −0.61 (−0.87, −0.34) ” | <0.001 | 0.36 (15) | 0.65 | no | yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wiedermann, C.J. Human Albumin Infusion in Critically Ill and Perioperative Patients: Narrative Rapid Review of Meta-Analyses from the Last Five Years. J. Clin. Med. 2023, 12, 5919. https://doi.org/10.3390/jcm12185919
Wiedermann CJ. Human Albumin Infusion in Critically Ill and Perioperative Patients: Narrative Rapid Review of Meta-Analyses from the Last Five Years. Journal of Clinical Medicine. 2023; 12(18):5919. https://doi.org/10.3390/jcm12185919
Chicago/Turabian StyleWiedermann, Christian J. 2023. "Human Albumin Infusion in Critically Ill and Perioperative Patients: Narrative Rapid Review of Meta-Analyses from the Last Five Years" Journal of Clinical Medicine 12, no. 18: 5919. https://doi.org/10.3390/jcm12185919
APA StyleWiedermann, C. J. (2023). Human Albumin Infusion in Critically Ill and Perioperative Patients: Narrative Rapid Review of Meta-Analyses from the Last Five Years. Journal of Clinical Medicine, 12(18), 5919. https://doi.org/10.3390/jcm12185919