
Patients Hospitalized for COVID-19 in the Periods of Delta and Omicron Variant Dominance in Greece: Determinants of Severity and Mortality

 , , , , , , ,
, , , , , , ,  , , ,
, , ,  , add
Show full author list
, add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Characterization of Vaccination Status
2.3. Imaging Results
2.4. Assessment of Comorbidities
3. Statistical Analysis
4. Results
4.1. Characteristics of the Study Participants
4.2. Comorbidities in Patients with COVID-19 Hospitalized during the Two Waves of the Pandemic
4.3. Symptoms on Admission during the Two Study Periods
4.4. Laboratory Findings
4.5. Disease Severity and Outcomes during the Two Waves of the Pandemic
4.6. Complications during Hospitalization for COVID-19 in the Two Study Periods
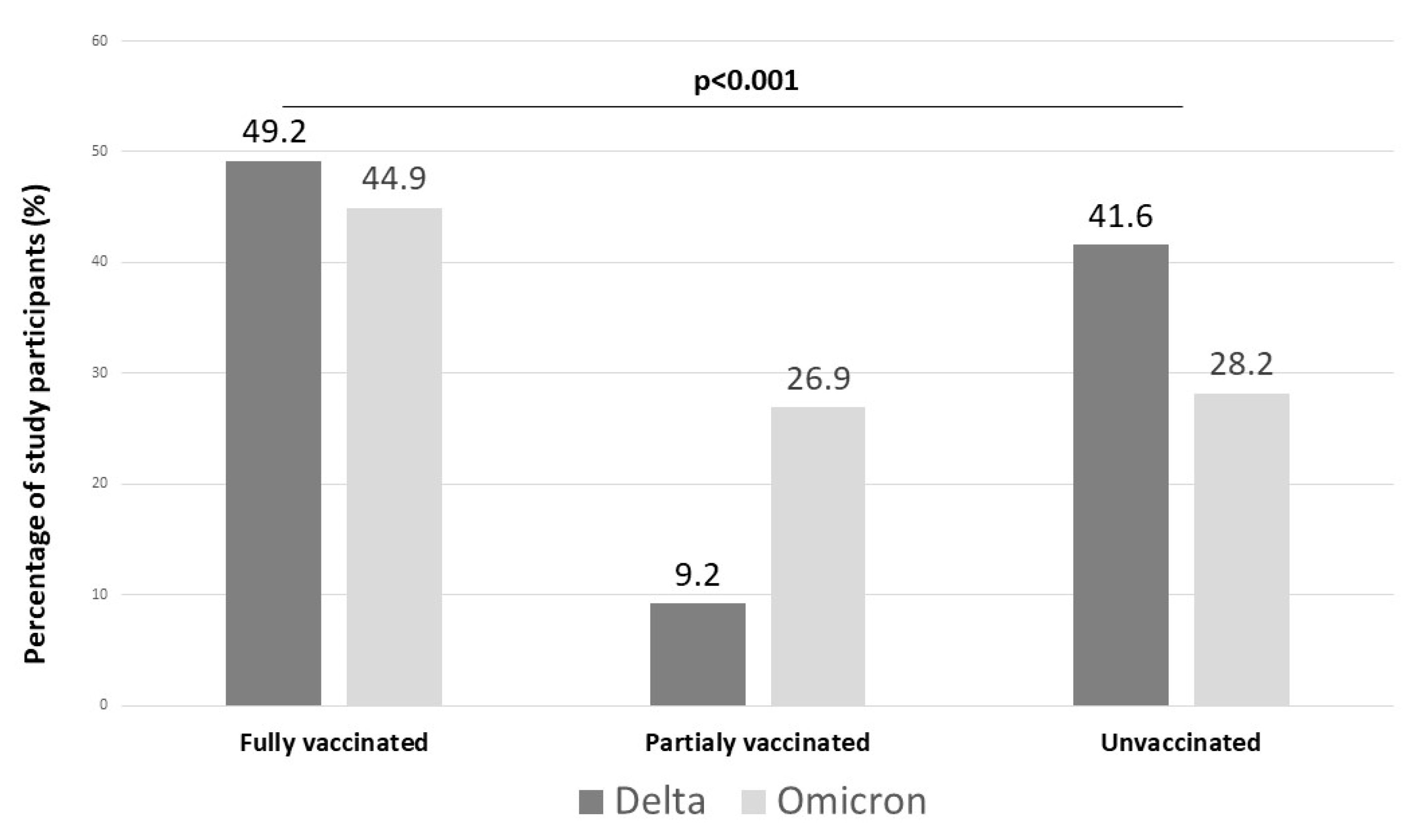
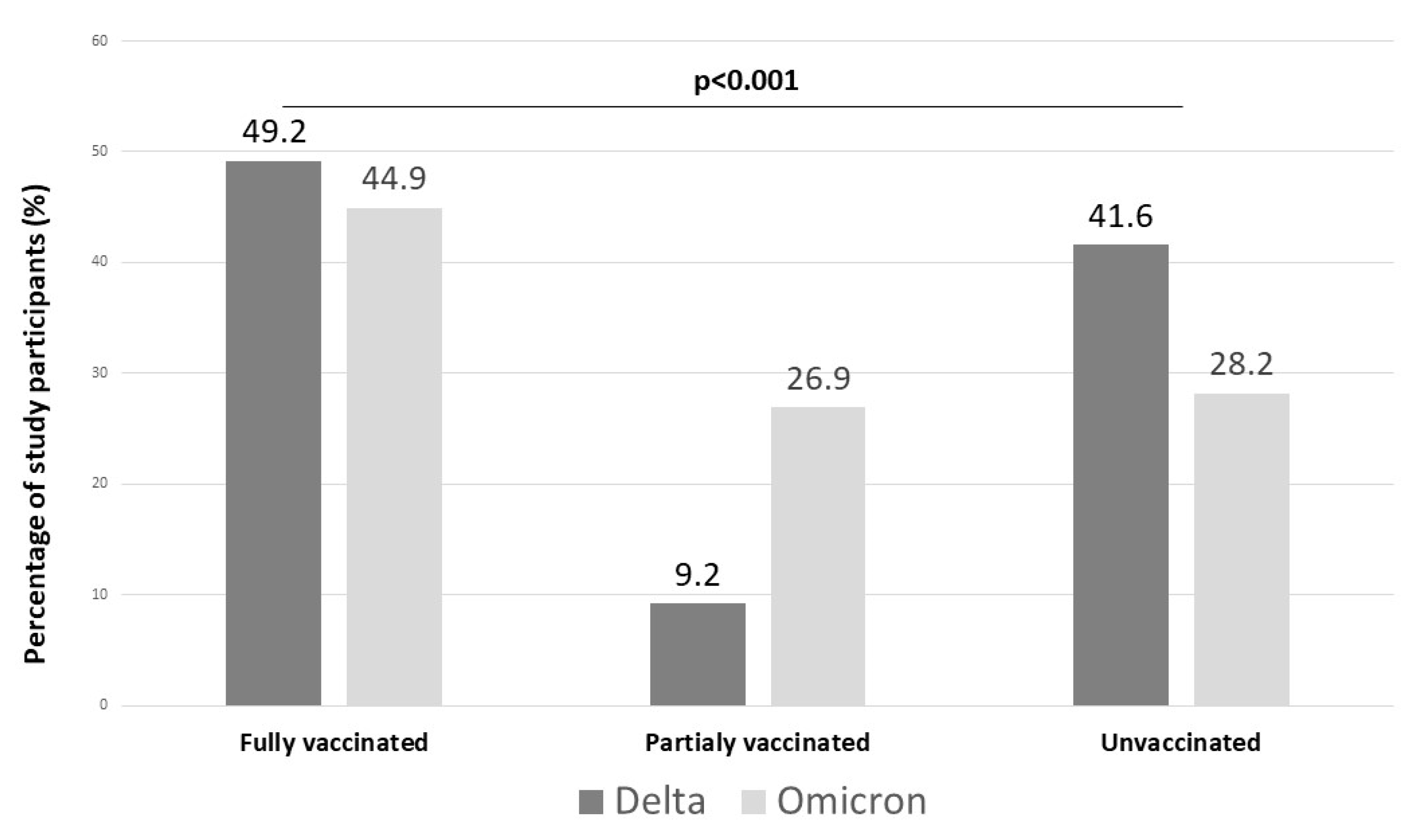
4.7. Vaccination Status during the Two Waves of the Pandemic
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 10 July 2023).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. COVID-19: WHO declares pandemic because of “alarming levels” of spread, severity, and inaction. BMJ 2020, 368, m1036. [Google Scholar] [CrossRef]
- WHO Coronavirus (COVID-19) Dashboard. 2023. Available online: https://covid19.who.int/ (accessed on 14 July 2023).
- Aleem, A.; Akbar Samad, A.B.; Vaqar, S. Emerging Variants of SARS-CoV-2 and Novel Therapeutics Against Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19); StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Shiehzadegan, S.; Alaghemand, N.; Fox, M.; Venketaraman, V. Analysis of the Delta Variant B.1.617.2 COVID-19. Clin. Pract. 2021, 11, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.J.; Guo, H.; Luo, G. Omicron variant (B.1.1.529) of SARS-CoV-2, a global urgent public health alert! J. Med. Virol. 2022, 94, 1255–1256. [Google Scholar] [CrossRef] [PubMed]
- Karim, S.S.A.; Karim, Q.A. Omicron SARS-CoV-2 variant: A new chapter in the COVID-19 pandemic. Lancet 2021, 398, 2126–2128. [Google Scholar] [CrossRef] [PubMed]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Bakakos, A.; Koukaki, E.; Ampelioti, S.; Ioannidou, I.; Papaioannou, A.I.; Loverdos, K.; Koutsoukou, A.; Rovina, N. The Real Impact of Age on Mortality in Critically Ill COVID-19 Patients. J. Pers. Med. 2023, 13, 908. [Google Scholar] [CrossRef] [PubMed]
- Shi, C.; Wang, L.; Ye, J.; Gu, Z.; Wang, S.; Xia, J.; Xie, Y.; Li, Q.; Xu, R.; Lin, N. Predictors of mortality in patients with coronavirus disease 2019: A systematic review and meta-analysis. BMC Infect. Dis. 2021, 21, 663. [Google Scholar] [CrossRef] [PubMed]
- Modes, M.E.; Directo, M.P.; Melgar, M.; Johnson, L.R.; Yang, H.; Chaudhary, P.; Bartolini, S.; Kho, N.; Noble, P.W.; Isonaka, S.; et al. Clinical Characteristics and Outcomes Among Adults Hospitalized with Laboratory-Confirmed SARS-CoV-2 Infection During Periods of B.1.617.2 (Delta) and B.1.1.529 (Omicron) Variant Predominance—One Hospital, California, 15 July–23 September 2021, and 21 December 2021–27 January 2022. Morb. Mortal. Wkly. Rep. 2022, 71, 217–223. [Google Scholar] [CrossRef]
- Ward, I.L.; Bermingham, C.; Ayoubkhani, D.; Gethings, O.J.; Pouwels, K.B.; Yates, T.; Khunti, K.; Hippisley-Cox, J.; Banerjee, A.; Walker, A.S.; et al. Risk of COVID-19 related deaths for SARS-CoV-2 omicron (B.1.1.529) compared with delta (B.1.617.2): Retrospective cohort study. BMJ 2022, 378, e070695. [Google Scholar] [CrossRef] [PubMed]
- Yüce, M.; Filiztekin, E.; Özkaya, K.G. COVID-19 diagnosis—A review of current methods. Biosens. Bioelectron. 2021, 172, 112752. [Google Scholar] [CrossRef] [PubMed]
- Mendis, S.; Puska, P.; Norrving, B.; World Health Organization; World Heart Federation; World Stroke Organization. Global Atlas on Cardiovascular Disease Prevention and Control; Mendis, S., Puska, P., Norrving, B., Eds.; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Arkoudis, N.A.; Tsochatzis, A.; Argentos, S.; Kontopoulou, C.; Mademli, M.; Spiliopoulos, S.; Oikonomopoulos, N. CT in patients with COVID-19: Imaging patterns, disease extent and evolution; our experience in a Greek reference University Hospital. Hell. J. Radiol. 2021, 6, 6–12. [Google Scholar]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Liang, W.H.; Zhao, Y.; Liang, H.R.; Chen, Z.S.; Li, Y.M.; Liu, X.Q.; Chen, R.C.; Tang, C.L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron. Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- Koch, D.G.; Speiser, J.L.; Durkalski, V.; Fontana, R.J.; Davern, T.; McGuire, B.; Stravitz, R.T.; Larson, A.M.; Liou, I.; Fix, O.; et al. The Natural History of Severe Acute Liver Injury. Am. J. Gastroenterol. 2017, 112, 1389–1396. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, R.B.; Botelho, B.G.; Hollanda, J.V.G.; Ferreira, L.V.L.; Junqueira de Andrade, L.Z.; Oei, S.; Mello, T.S.; Muxfeldt, E.S. COVID-19 and the cardiovascular system: A comprehensive review. J. Hum. Hypertens. 2021, 35, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Chen, T.; Mui, D.; Ferrari, V.; Jagasia, D.; Scherrer-Crosbie, M.; Chen, Y.; Han, Y. Cardiovascular manifestations and treatment considerations in COVID-19. Heart 2020, 106, 1132–1141. [Google Scholar] [CrossRef]
- Ozdalga, E.; Ahuja, N.; Sehgal, N.; Hom, J.; Weng, Y.; Pinsky, B.; Schulman, K.A.; Collins, W. Detailed characterization of hospitalized patients infected with the Omicron variant of SARS-CoV-2. J. Intern. Med. 2022, 292, 385–387. [Google Scholar] [CrossRef] [PubMed]
- Argun Barış, S.; Boyacı, H.; Akhan, S.; Mutlu, B.; Deniz, M.; Başyiğit, İ. Charlson Comorbidity Index in Predicting Poor Clinical Outcomes and Mortality in Patients with COVID-19. Turk. Thorac. J. 2022, 23, 145–153. [Google Scholar] [CrossRef]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, F.; Myers, J.; Basu, D.; Tintinger, G.; Ueckermann, V.; Mathebula, M.; Ramlall, R.; Spoor, S.; de Villiers, T.; Van der Walt, Z.; et al. Decreased severity of disease during the first global omicron variant covid-19 outbreak in a large hospital in tshwane, south africa. Int. J. Infect. Dis. 2022, 116, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Jassat, W.; Abdool Karim, S.S.; Mudara, C.; Welch, R.; Ozougwu, L.; Groome, M.J.; Govender, N.; von Gottberg, A.; Wolter, N.; Wolmarans, M.; et al. Clinical severity of COVID-19 in patients admitted to hospital during the omicron wave in South Africa: A retrospective observational study. Lancet Glob. Health 2022, 10, e961–e969. [Google Scholar] [CrossRef] [PubMed]
- Wolter, N.; Jassat, W.; Walaza, S.; Welch, R.; Moultrie, H.; Groome, M.; Amoako, D.G.; Everatt, J.; Bhiman, J.N.; Scheepers, C.; et al. Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: A data linkage study. Lancet 2022, 399, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.; Yu, N.; Cai, S.; Zhou, J.; Sheng, J.; Liu, K.; Zhou, H.; Guo, Y.; Niu, G. Quantitative computed tomography analysis for stratifying the severity of Coronavirus Disease 2019. J. Pharm. Anal. 2020, 10, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Grodecki, K.; Lin, A.; Cadet, S.; McElhinney, P.A.; Razipour, A.; Chan, C.; Pressman, B.; Julien, P.; Maurovich-Horvat, P.; Gaibazzi, N.; et al. Quantitative Burden of COVID-19 Pneumonia on Chest CT Predicts Adverse Outcomes: A Post-Hoc Analysis of a Prospective International Registry. Radiol. Cardiothorac. Imaging 2020, 2, e200389. [Google Scholar] [CrossRef]
- Harrigan, S.P.; Wilton, J.; Chong, M.; Abdia, Y.; Velasquez Garcia, H.; Rose, C.; Taylor, M.; Mishra, S.; Sander, B.; Hoang, L.; et al. Clinical Severity of Severe Acute Respiratory Syndrome Coronavirus 2 Omicron Variant Relative to Delta in British Columbia, Canada: A Retrospective Analysis of Whole-Genome Sequenced Cases. Clin. Infect. Dis. 2023, 76, e18–e25. [Google Scholar] [CrossRef] [PubMed]
- Barh, D.; Tiwari, S.; Rodrigues Gomes, L.G.; Ramalho Pinto, C.H.; Andrade, B.S.; Ahmad, S.; Aljabali, A.A.A.; Alzahrani, K.J.; Banjer, H.J.; Hassan, S.S.; et al. SARS-CoV-2 Variants Show a Gradual Declining Pathogenicity and Pro-Inflammatory Cytokine Stimulation, an Increasing Antigenic and Anti-Inflammatory Cytokine Induction, and Rising Structural Protein Instability: A Minimal Number Genome-Based Approach. Inflammation 2023, 46, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Trofin, F.; Nastase, E.V.; Roșu, M.F.; Bădescu, A.C.; Buzilă, E.R.; Miftode, E.G.; Manciuc, D.C.; Dorneanu, O.S. Inflammatory Response in COVID-19 Depending on the Severity of the Disease and the Vaccination Status. Int. J. Mol. Sci. 2023, 24, 8550. [Google Scholar] [CrossRef]
- Iqbal, S.; Khan, S.; Qureshi, M.A.; Sayeed, M.A.; Khan, B.A.; Zaheer, S.; Faruqui, H.; Rajput, A.W. Clinical and Biochemical Characteristics of COVID-19 Patients During the Delta-Omicron Wave with Risk Assessment of Adverse Outcomes. J. Coll. Physicians Surg. Pak. 2023, 33, 297–302. [Google Scholar] [CrossRef]
- Ali, M.A.M.; Spinler, S.A. COVID-19 and thrombosis: From bench to bedside. Trends Cardiovasc. Med. 2021, 31, 143–160. [Google Scholar] [CrossRef]
- Hanff, T.C.; Mohareb, A.M.; Giri, J.; Cohen, J.B.; Chirinos, J.A. Thrombosis in COVID-19. Am. J. Hematol. 2020, 95, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.P.; Darbousset, R.; Schoenwaelder, S.M. Thromboinflammation: Challenges of therapeutically targeting coagulation and other host defense mechanisms. Blood 2019, 133, 906–918. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Wang, L. COVID-19 and cardiovascular diseases. J. Mol. Cell Biol. 2021, 13, 161–167. [Google Scholar] [CrossRef]
- Ulloa, A.C.; Buchan, S.A.; Daneman, N.; Brown, K.A. Estimates of SARS-CoV-2 Omicron Variant Severity in Ontario, Canada. JAMA 2022, 327, 1286–1288. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Xiang, G.; Xie, L.; Chen, Z.; Hao, S.; Fu, C.; Wu, Q.; Liu, X.; Li, S. Clinical risk factors for mortality of hospitalized patients with COVID-19: Systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 2723–2735. [Google Scholar] [CrossRef]
- Gungor, B.; Atici, A.; Baycan, O.F.; Alici, G.; Ozturk, F.; Tugrul, S.; Asoglu, R.; Cevik, E.; Sahin, I.; Barman, H.A. Elevated D-dimer levels on admission are associated with severity and increased risk of mortality in COVID-19: A systematic review and meta-analysis. Am. J. Emerg. Med. 2021, 39, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Zhan, H.; Chen, H.; Liu, C.; Cheng, L.; Yan, S.; Li, H.; Li, Y. Diagnostic Value of D-Dimer in COVID-19: A Meta-Analysis and Meta-Regression. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211010976. [Google Scholar] [CrossRef]
- Karimi, A.; Shobeiri, P.; Kulasinghe, A.; Rezaei, N. Novel Systemic Inflammation Markers to Predict COVID-19 Prognosis. Front. Immunol. 2021, 12, 741061. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, C.; Mao, Z.; Xiao, M.; Wang, L.; Qi, S.; Zhou, F. Predictive values of neutrophil-to-lymphocyte ratio on disease severity and mortality in COVID-19 patients: A systematic review and meta-analysis. Crit. Care 2020, 24, 647. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Li, P.; Ye, X.; Huang, X.; Feng, B.; Ji, T.; Chen, Z.; Li, F.; Zhang, Y.; Luo, K.; et al. Longitudinal Peripheral Blood Transcriptional Analysis Reveals Molecular Signatures of Disease Progression in COVID-19 Patients. J. Immunol. 2021, 206, 2146–2159. [Google Scholar] [CrossRef] [PubMed]
- Pranshu, K.; Shahul, A.; Singh, S.; Kuwal, A.; Sonigra, M.; Dutt, N. Predictors of mortality among hospitalized patients with COVID-19: A single-centre retrospective analysis. Can. J. Respir. Ther. 2022, 58, 98–102. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | Total (n = 979) | Delta (n = 433) | Omicron (n = 546) | p Value | ||
|---|---|---|---|---|---|---|
| Age (median, IQR) | 67 (54, 81) | 65 (51, 77) | 70 (55, 83) | <0.001 | ||
| Gender (n, %) | Female | 452 (46.2%) | 212 (49%) | 240 (44%) | 0.119 | |
| Male | 527 (53.8%) | 221 (51%) | 306 (56%) | |||
| Obesity (BMI > 30 kg/m2) (n, %) | 145 (14.8%) | 61 (14.1%) | 84 (15.4%) | 0.614 | ||
| Smoking habit (n, %) | Never | 519 (53%) | 257 (59.4%) | 262 (48%) | 0.002 | |
| Current | 184 (18.8%) | 70 (16.2%) | 114 (20.9%) | |||
| Former | 276 (28.2%) | 106 (24.5%) | 170 (31.1%) | |||
| Comorbidities | Total (n = 979) | Delta (n = 433) | Omicron (n = 546) | p-Value |
|---|---|---|---|---|
| Diabetes | 206 (21%) | 79 (18.2%) | 127 (23.3%) | 0.056 |
| COPD | 99 (10.1%) | 37 (8.5%) | 62 (11.4%) | 0.147 |
| Asthma | 59 (6%) | 25 (5.8%) | 34 (6.2%) | 0.767 |
| IPF | 13 (1.3%) | 2 (0.5%) | 11 (2%) | 0.035 |
| Dementia | 138 (14.1%) | 46 (10.6%) | 92 (16.8%) | 0.005 |
| Cancer | 88 (9%) | 30 (6.9%) | 58 (10.6%) | 0.181 |
| Cardiovascular disease | 572 (58.4%) | 233 (53.8%) | 339 (62.1%) | 0.009 |
| Connective tissue disease | 37 (3.8%) | 10 (2.3%) | 27 (4.9%) | 0.032 |
| Chronic kidney disease | 52 (5.3%) | 16 (3.7%) | 36 (6.6%) | 0.045 |
| Chronic treatment with immunosuppressive drugs | 76 (7.8%) | 22 (5.1%) | 54 (9.9%) | 0.005 |
| Charlson Comorbidity Index (median, IQR) | 3 (1, 5) | 3 (0, 5) | 4 (1, 6) | <0.001 |
| Parameters | Total (n = 979) | Delta (n = 433) | Omicron (n = 546) | p-Value |
|---|---|---|---|---|
| WBC (×103/μL) | 6.7 (5.0, 9.5) | 6.7 (4.8, 9.2) | 6.8 (5.2, 9.7) | 0.047 |
| Lymphocytes (×103/μL) | 1.0 (0.7, 1.5) | 1.01 (0.7, 1.38) | 1.05 (0.7, 1.54) | 0.114 |
| Neutrophils (×103/μL) | 4.8 (3.3, 7.4) | 4.7 (3.3, 7.4) | 4.8 (3.3, 7.4) | 0.513 |
| Platelets (×103/μL) | 200 (158,260) | 199 (158, 263) | 200 (158, 258) | 0.608 |
| Neutrophil/lymphocyte ratio | 4.4 (2.8, 8.8) | 4.4 (2.9, 8.4) | 4.5, (2.6, 9.0) | 0.826 |
| Platelet/lymphocyte ratio | 194.2 (130.9, 289.3) | 198.9 (140.2, 284.9) | 188.9 (123.3, 295.9) | 0.086 |
| PCT (ng/mL) | 0.07 (0.03, 0.16) | 0.08 (0.05, 0.17) | 0.06 (0.02,0.16) | 0.005 |
| Ferritin (ng/mL) | 254 (136, 541) | 301 (159, 644) | 239 (128, 473) | 0.002 |
| D-dimer (mg/L) | 0.73 (0.43, 1.43) | 0.74 (0.44, 1.35) | 0.73 (0.42, 1.51) | 0.401 |
| CRP (mg/L) | 35.7 (13.3, 87.7) | 40.4 (16.7, 98.5) | 31.8 (11.9, 81.7) | 0.003 |
| LDH (U/L) | 266 (211, 344) | 277 (221, 375) | 255 (205, 320) | <0.001 |
| Symptoms | ||||
| Dyspnea N (%) | 449 (45.9%) | 201 (46.4%) | 248 (45.4%) | 0.755 |
| Anosmia N (%) | 123 (12.6%) | 52 (12%) | 71 (13%) | 0.641 |
| Cough N (%) | 401 (41%) | 186 (43%) | 215 (39.4%) | 0.258 |
| Fatigue N (%) | 374 (38.2%) | 171 (39.5%) | 203 (37.25%) | 0.460 |
| Fever N (%) | 382 (39%) | 193 (44.6%) | 189 (34.6%) | 0.002 |
| Headache N (%) | 171 (17.5%) | 70 (16.2%) | 101 (18.5%) | 0.340 |
| GI symptoms N (%) | 174 (17.85) | 62 (14.3%) | 112 (20.5%) | 0.012 |
| Parameters | Total (n = 979) | Delta (n = 433) | Omicron (n = 546) | p-Value |
|---|---|---|---|---|
| Length of hospital stay (days) | 8 (5, 12) | 8 (6, 13) | 7 (5, 12) | 0.001 |
| PaO2/FiO2 ratio | 319 (263, 366) | 314 (257, 360) | 322 (269, 368) | 0.053 |
| Max FiO2 | 0.32 (0.24, 0.50) | 0.32 (0.24, 0.50) | 0.31 (0.24, 0.50) | 0.840 |
| Admission to ICU | 56 (5.7%) | 28 (6.5%) | 28 (5.1%) | 0.37 |
| Death | 139 (14.2%) | 54 (12.5%) | 85 (15.6%) | 0.168 |
| Extent of disease (Co.V.A.Sc) * | Total (n = 606) | Delta (n = 293) | Omicron (n = 313) | 0.001 |
| 1–10% | 254 (41.8%) | 92 (31.3%) | 162 (51.8%) | |
| 11–25% | 129 (21.3%) | 69 (23.5%) | 60 (19.2%) | |
| 26–50% | 114 (18.8%) | 71 (24.2%) | 43 (13.7%) | |
| 51–75% | 71 (11.7%) | 44 (15.0%) | 27 (8.6%) | |
| >75% | 38 (6.3%) | 17 (5.8%) | 21 (6.7%) |
| Events during Hospitalization | Total (n = 979) | Delta (n = 433) | Omicron (n = 546) | p-Value |
|---|---|---|---|---|
| CV event | 72 (7.4%) | 15 (3.5%) | 57 (10.4%) | <0.001 |
| PE | 35 (3.6%) | 13 (3%) | 22 (4%) | 0.387 |
| DVT | 10 (1%) | 0 (0%) | 10 (1.8%) | 0.005 |
| AKI | 127 (13%) | 46 (10.6%) | 81 (14.8%) | 0.051 |
| ALI | 91 (9.3%) | 30 (6.9%) | 61 (11.2%) | 0.023 |
| (A) | ||||||
|---|---|---|---|---|---|---|
| Variables | Univariate Analysis | Multivariate Analysis | ||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 1.052 | 1.032–1.073 | <0.001 | 1.047 | 1.004–1.092 | 0.032 |
| Gender | 0.961 | 0.564–1.638 | 0.883 | |||
| Obesity | 0.737 | 0.316–1.723 | 0.481 | |||
| CCI | 1.390 | 1.260–1.533 | <0.001 | 1.088 | 0.909–1.302 | 0.358 |
| Chronic treatment with immunosuppressive drugs | 1.876 | 0.747–4.709 | 0.180 | |||
| N/L ratio | 1.059 | 1.043–1.075 | <0.001 | 1.046 | 1.015–1.078 | 0.004 |
| D-dimer on admission | 1.089 | 1.033–1.148 | 0.001 | 1.092 | 1.018–1.172 | 0.014 |
| CRP on admission | 1.010 | 1.007–1.013 | <0.001 | 1.003 | 0.998–1.008 | 0.222 |
| CV event during hospitalization | 5.906 | 2.783–12.534 | <0.001 | 3.911 | 1.088–14.052 | 0.037 |
| AKI during hospitalization | 8.842 | 5.162–15.129 | <0.001 | 4.341 | 1.576–11.960 | 0.005 |
| ALI during hospitalization | 3.651 | 1.882–0.994 | <0.001 | 1.071 | 0.308–3.722 | 0.914 |
| PaO2/FiO2 on admission | 0.991 | 0.988–0.994 | <0.001 | 1.002 | 0.996–1.007 | 0.576 |
| Extent of disease on chest CT | 2.165 | 1.556–3.016 | <0.001 | 1.902 | 1.194–3.030 | 0.007 |
| (B) | ||||||
| Variables | Univariate Analysis | Multivariate Analysis | ||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 1.054 | 1.036–1.072 | <0.001 | 1.009 | 0.971–1.049 | 0.638 |
| Gender | 0.771 | 0.504–1.180 | 0.231 | |||
| Obesity | 0.324 | 0.131–0.801 | 0.015 | 0.095 | 0.007–1.220 | 0.071 |
| CCI | 1.422 | 1.312–1.542 | <0.001 | 1.096 | 0.893–1.345 | 0.380 |
| Chronic treatment with immunosuppressive drugs | 1.379 | 0.732–2.597 | 0.320 | |||
| N/L ratio | 1.053 | 1.039–1.067 | <0.001 | 1.017 | 0.970–1.067 | 0.484 |
| D-dimer on admission | 1.069 | 1.043–1.097 | <0.001 | 1.057 | 0.997–1.121 | 0.063 |
| CRP on admission | 1.008 | 1.006–1.010 | <0.001 | 1.003 | 0.997–1.009 | 0.339 |
| CV event during hospitalization | 8.226 | 5.326–12.705 | <0.001 | 3.490 | 1.247–9.767 | 0.017 |
| AKI during hospitalization | 10.097 | 6.557–15.550 | <0.001 | 0.951 | 0.277–3.273 | 0.937 |
| ALI during hospitalization | 4.770 | 3.044–7.475 | <0.001 | 4.890 | 1.616–14.791 | 0.005 |
| PaO2/FiO2 on admission | 0.989 | 0.987–0.991 | <0.001 | 0.993 | 0.987–0.998 | 0.013 |
| Extent of disease on chest CT | 2.377 | 1.816–3.109 | 0.001 | 1.289 | 0.852–1.949 | 0.230 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karageorgou, V.; Papaioannou, A.I.; Kallieri, M.; Blizou, M.; Lampadakis, S.; Sfika, M.; Krouskos, A.; Papavasileiou, V.; Strakosha, F.; Vandorou, K.T.; et al. Patients Hospitalized for COVID-19 in the Periods of Delta and Omicron Variant Dominance in Greece: Determinants of Severity and Mortality. J. Clin. Med. 2023, 12, 5904. https://doi.org/10.3390/jcm12185904
Karageorgou V, Papaioannou AI, Kallieri M, Blizou M, Lampadakis S, Sfika M, Krouskos A, Papavasileiou V, Strakosha F, Vandorou KT, et al. Patients Hospitalized for COVID-19 in the Periods of Delta and Omicron Variant Dominance in Greece: Determinants of Severity and Mortality. Journal of Clinical Medicine. 2023; 12(18):5904. https://doi.org/10.3390/jcm12185904
Chicago/Turabian StyleKarageorgou, Vagia, Andriana I. Papaioannou, Maria Kallieri, Myrto Blizou, Stefanos Lampadakis, Maria Sfika, Antonios Krouskos, Vasileios Papavasileiou, Franceska Strakosha, Kalliopi Theoni Vandorou, and et al. 2023. "Patients Hospitalized for COVID-19 in the Periods of Delta and Omicron Variant Dominance in Greece: Determinants of Severity and Mortality" Journal of Clinical Medicine 12, no. 18: 5904. https://doi.org/10.3390/jcm12185904
APA StyleKarageorgou, V., Papaioannou, A. I., Kallieri, M., Blizou, M., Lampadakis, S., Sfika, M., Krouskos, A., Papavasileiou, V., Strakosha, F., Vandorou, K. T., Siozos, P., Moustaka Christodoulou, M., Kontonasiou, G., Apollonatou, V., Antonogiannaki, E. M., Kyriakopoulos, C., Aggelopoulou, C., Chronis, C., Kostikas, K., ... Loukides, S. (2023). Patients Hospitalized for COVID-19 in the Periods of Delta and Omicron Variant Dominance in Greece: Determinants of Severity and Mortality. Journal of Clinical Medicine, 12(18), 5904. https://doi.org/10.3390/jcm12185904