
Rehabilitation of Peripheral Neuropathies: From Lexical Analysis of the Literature to Identification of Clinical Protocols

 ,
,  , and
, and 
Abstract
:
1. Introduction
2. Materials and Methods
3. Results
3.1. General Results
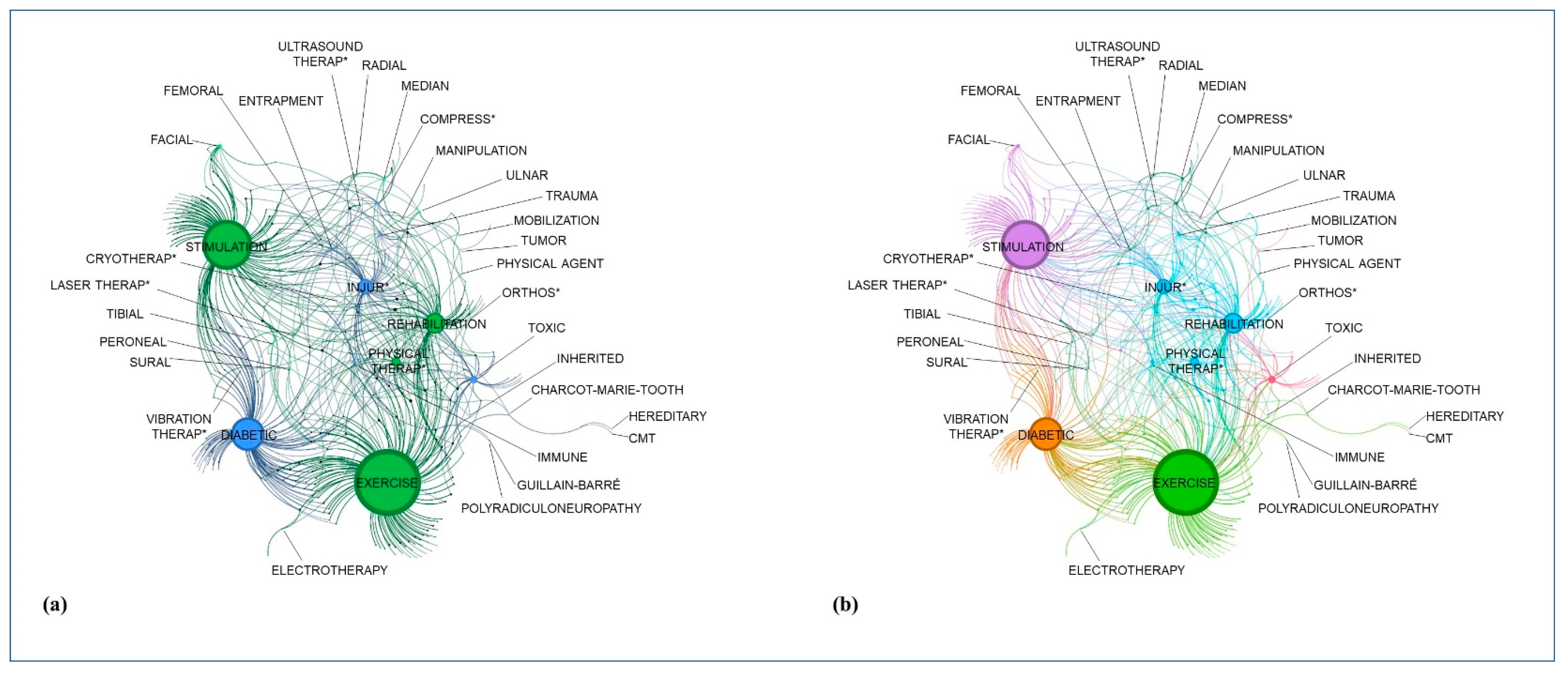
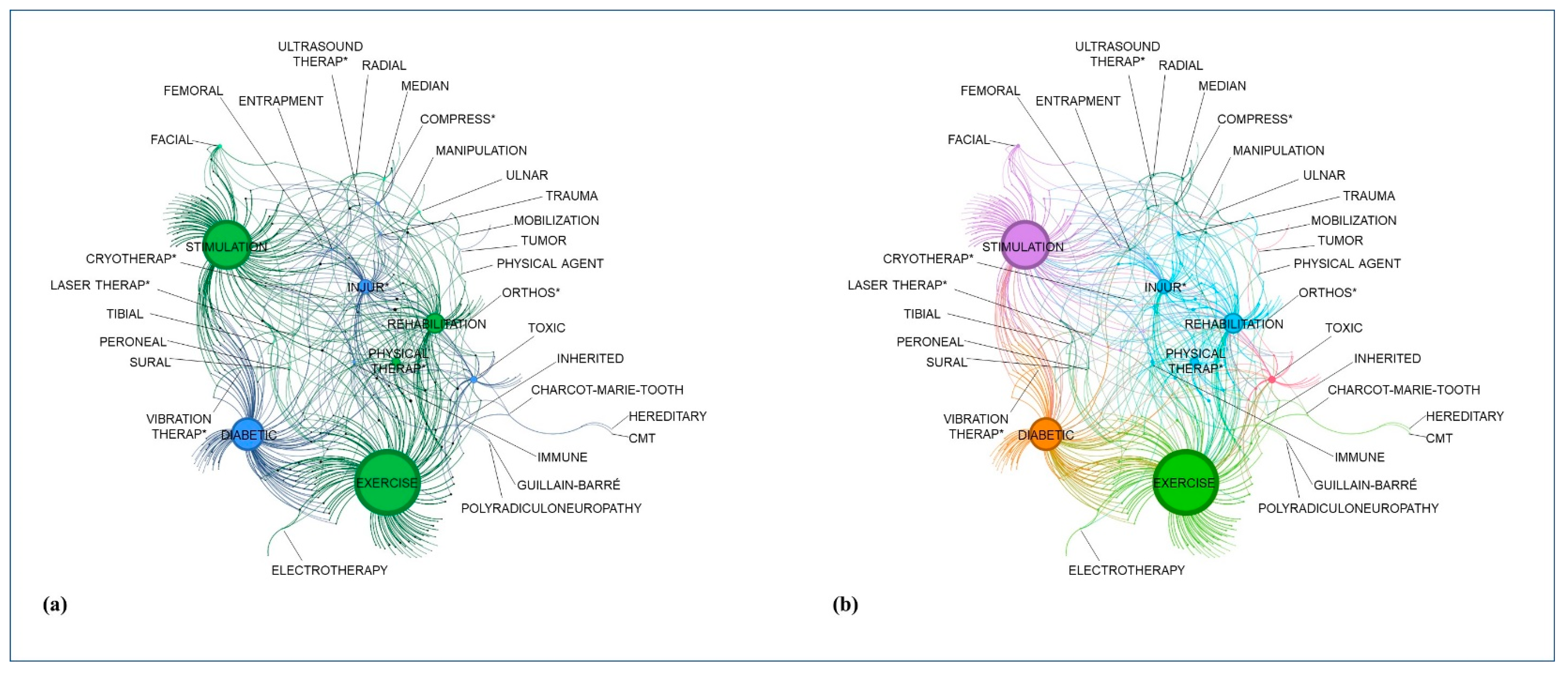
3.2. Lexical Network Based on Graph-Theory
3.3. Relative Results of the Single Searches
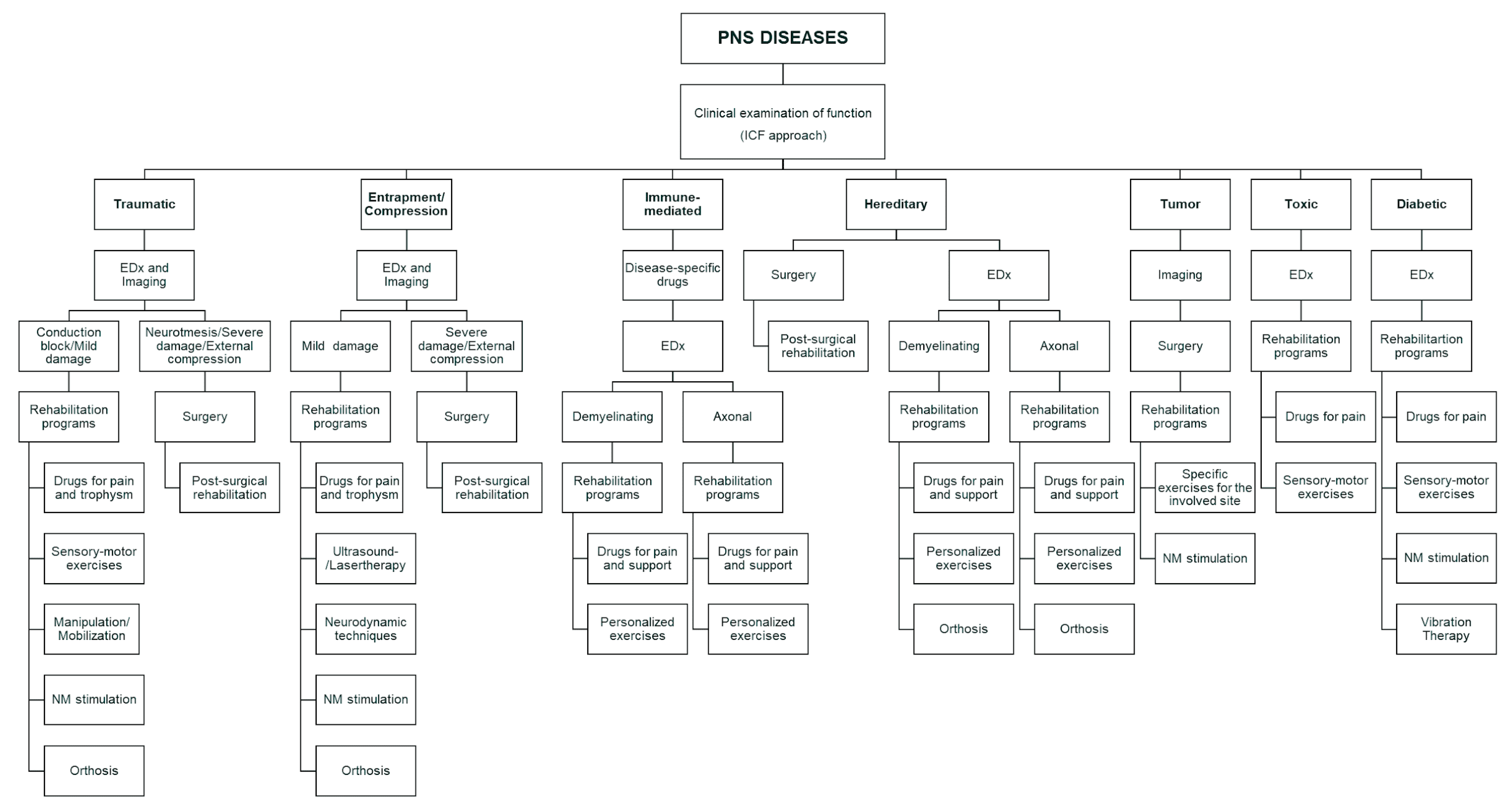
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- England, J.D.; Asbury, A.K. Peripheral neuropathy. Lancet 2004, 363, 2151–2161. [Google Scholar] [CrossRef]
- Alkandari, M.; Hollywood, A. People’s experiences living with peripheral neuropathy: A qualitative study. Front. Pain Res. (Lausanne) 2023, 4, 1162405. [Google Scholar] [CrossRef]
- Vallat, J.M.; Mathis, S. Pathology explains various mechanisms of auto-immune inflammatory peripheral neuropathies. Brain Pathol. 2023, e13184. [Google Scholar] [CrossRef]
- Masingue, M.; Fernández-Eulate, G.; Debs, R.; Tard, C.; Labeyrie, C.; Leonard-Louis, S.; Dhaenens, C.M.; Masson, M.A.; Latour, P.; Stojkovic, T. Strategy for genetic analysis in hereditary neuropathy. Rev. Neurol. (Paris) 2023, 179, 10–29. [Google Scholar] [CrossRef]
- Barnes, S.L.; Miller, T.A.; Simon, N.G. Traumatic peripheral nerve injuries: Diagnosis and management. Curr. Opin. Neurol. 2022, 35, 718–727. [Google Scholar] [CrossRef] [PubMed]
- Bosch-Queralt, M.; Fledrich, R.; Stassart, R.M. Schwann cell functions in peripheral nerve development and repair. Neurobiol. Dis. 2023, 176, 105952. [Google Scholar] [CrossRef]
- Hao, Y.; Collins, C. Intrinsic mechanisms for axon regeneration: Insights from injured axons in Drosophila. Curr. Opin. Genet. Dev. 2017, 44, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Fisse, A.L.; Fiegert, S.; Stoykova, Z.; Brünger, J.; Athanasopoulos, D.; Grüter, T.; Motte, J.; Gold, R.; Pitarokoili, K. Increased muscle echointensity correlates with clinical disability and muscle strength in chronic inflammatory demyelinating polyneuropathy. Eur. J. Neurol. 2021, 28, 1698–1705. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Shan, Q.; Ling, M.; Ni, X.A.; Mao, S.S.; Yu, B.; Cao, Q.Q. Identification of key genes involved in axon regeneration and Wallerian degeneration by weighted gene co-expression network analysis. Neural Regen. Res. 2022, 17, 911–919. [Google Scholar] [CrossRef]
- Telleman, J.A.; Herraets, I.J.; Goedee, H.S.; van Asseldonk, J.T.; Visser, L.H. Ultrasound scanning in the diagnosis of peripheral neuropathies. Pract. Neurol. 2021, 21, 186–195. [Google Scholar] [CrossRef]
- Padua, L.; Coraci, D.; Erra, C.; Pazzaglia, C.; Paolasso, I.; Loreti, C.; Caliandro, P.; Hobson-Webb, L.D. Carpal tunnel syndrome: Clinical features, diagnosis, and management. Lancet Neurol. 2016, 15, 1273–1284. [Google Scholar] [CrossRef]
- Yan, J.; Zhou, R.; Liu, B.; Xu, Y.; Cao, X. Plexiform schwannomas of the sciatic nerve:a case report and review of the literature. Heliyon 2023, 9, e18020. [Google Scholar] [CrossRef]
- Yang, H.; Dong, Y.; Wang, Z.; Lai, J.; Yao, C.; Zhou, H.; Alhaskawi, A.; Hasan Abdullah Ezzi, S.; Kota, V.G.; Hasan Abdulla Hasan Abdulla, M.; et al. Traumatic neuromas of peripheral nerves: Diagnosis, management and future perspectives. Front. Neurol. 2023, 13, 1039529. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.S.; Jain, S.A. Challenges in Nerve Repair and Reconstruction. Hand Clin. 2023, 39, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Shastri, A.; Al Aiyan, A.; Kishore, U.; Farrugia, M.E. Immune-Mediated Neuropathies: Pathophysiology and Management. Int. J. Mol. Sci. 2023, 24, 7288. [Google Scholar] [CrossRef]
- McCombe, P.A.; Hardy, T.A.; Nona, R.J.; Greer, J.M. Sex differences in Guillain Barré syndrome, chronic inflammatory demyelinating polyradiculoneuropathy and experimental autoimmune neuritis. Front. Immunol. 2022, 13, 1038411. [Google Scholar] [CrossRef]
- Fonseca, M.C.; Marazzi-Diniz, P.H.S.; Leite, M.F.; Ehrlich, B.E. Calcium signaling in chemotherapy-induced neuropathy. Cell Calcium 2023, 113, 102762. [Google Scholar] [CrossRef]
- Behl, T.; Yadav, H.N.; Sharma, P.L. Alcoholic Neuropathy: Involvement of Multifaceted Signalling Mechanisms. Curr. Mol. Pharmacol. 2021, 14, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Berciano, J.; García, A.; Gallardo, E.; Peeters, K.; Pelayo-Negro, A.L.; Álvarez-Paradelo, S.; Gazulla, J.; Martínez-Tames, M.; Infante, J.; Jordanova, A. Intermediate Charcot-Marie-Tooth disease: An electrophysiological reappraisal and systematic review. J. Neurol. 2017, 264, 1655–1677. [Google Scholar] [CrossRef]
- Kolarić, V.; Svirčević, V.; Bijuk, R.; Zupančič, V. Chronic complications of diabetes and quality of life. Acta Clin. Croat. 2022, 61, 520–527. [Google Scholar] [CrossRef]
- Meregalli, C.; Monza, L.; Jongen, J.L.M. A mechanistic understanding of the relationship between skin innervation and chemotherapy-induced neuropathic pain. Front. Pain Res. (Lausanne) 2022, 3, 1066069. [Google Scholar] [CrossRef]
- Singh, D.; Gray, J.; Laura, M.; Reilly, M.M. Charcot neuroarthropathy in patients with Charcot Marie Tooth Disease. Foot Ankle Surg. 2021, 27, 865–868. [Google Scholar] [CrossRef]
- Arslan, D.; Ünal Çevik, I. Interactions between the painful disorders and the autonomic nervous system. Agri 2022, 34, 155–165. (In English) [Google Scholar] [CrossRef]
- Alonge, P.; Di Stefano, V.; Lupica, A.; Gangitano, M.; Torrente, A.; Pignolo, A.; Maggio, B.; Iacono, S.; Gentile, F.; Brighina, F. Clinical and Neurophysiological Follow-Up of Chronic Inflammatory Demyelinating Polyneuropathy Patients Treated with Subcutaneous Immunoglobulins: A Real-Life Single Center Study. Brain Sci. 2022, 13, 10. [Google Scholar] [CrossRef]
- Lucchetta, M.; Briani, C.; Liotta, G.A.; Martinoli, C.; Coraci, D.; Padua, L. Ultrasonographic Tinel sign: Comment. Muscle Nerve 2010, 41, 570–571. [Google Scholar] [CrossRef] [PubMed]
- Coraci, D.; Luchetti, R.; Paolasso, I.; Santilli, V.; Padua, L. Intermittent ulnar nerve compression due to accessory abductor digiti minimi muscle: Crucial diagnostic role of nerve ultrasound. Muscle Nerve 2015, 52, 463–464. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, F. Peripheral Neuropathy in Diabetes: What Can MRI Do? Diabetes 2023, 72, 1060–1069. [Google Scholar] [CrossRef] [PubMed]
- Zheng, D.; Wu, Z.; Li, L.; Chen, S.; Chang, J. Research advances and trends in the surgical treatment of carpal tunnel syndrome from 2003 to 2022: A CiteSpace-based bibliometric analysis. Front. Neurol. 2023, 14, 1124407. [Google Scholar] [CrossRef]
- Cornblath, D.R.; van Doorn, P.A.; Hartung, H.P.; Merkies, I.S.J.; Katzberg, H.D.; Hinterberger, D.; Clodi, E.; ProCID Investigators. Safety and Tolerability of Intravenous Immunoglobulin in Chronic Inflammatory Demyelinating Polyneuropathy: Results of the ProCID Study. Drug Saf. 2023, 46, 835–845. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, Y.; Takashima, H. The Current State of Charcot-Marie-Tooth Disease Treatment. Genes 2023, 14, 1391. [Google Scholar] [CrossRef] [PubMed]
- Coraci, D.; Giovannini, S.; Loreti, C.; Fusco, A.; Padua, L. Management of neuropathic pain: A graph theory-based presentation of literature review. Breast J. 2020, 26, 581–582. [Google Scholar] [CrossRef] [PubMed]
- Didangelos, T.; Karlafti, E.; Kotzakioulafi, E.; Kontoninas, Z.; Margaritidis, C.; Giannoulaki, P.; Kantartzis, K. Efficacy and Safety of the Combination of Superoxide Dismutase, Alpha Lipoic Acid, Vitamin B12, and Carnitine for 12 Months in Patients with Diabetic Neuropathy. Nutrients 2020, 12, 3254. [Google Scholar] [CrossRef] [PubMed]
- Seon, C.; Lee, D.H.; Kwon, B.I.; Yu, J.S.; Park, S.K.; Woo, Y.; Kim, J.H. Neural mechanisms of acupuncture for peripheral facial nerve palsy: A protocol for systematic review and meta analysis. Medicine (Baltimore) 2023, 102, e33642. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.W.; Justice, D.; Chung, K.C.; Yang, L.J. A systematic review of evaluation methods for neonatal brachial plexus palsy: A review. J. Neurosurg. Pediatr. 2013, 12, 395–405. [Google Scholar] [CrossRef]
- Fernández-Pérez, P.; Leirós-Rodríguez, R.; Marqués-Sánchez, M.P.; Martínez-Fernández, M.C.; de Carvalho, F.O.; Maciel, L.Y.S. Effectiveness of physical therapy interventions in women with dyspareunia: A systematic review and meta-analysis. BMC Womens Health 2023, 23, 387. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Randhawa, K.; Côté, P.; Optima Collaboration. The Effectiveness of Physical Agents for Lower-Limb Soft Tissue Injuries: A Systematic Review. J. Orthop. Sports Phys. Ther. 2016, 46, 523–554. [Google Scholar] [CrossRef]
- Piscosquito, G.; Reilly, M.M.; Schenone, A.; Fabrizi, G.M.; Cavallaro, T.; Santoro, L.; Vita, G.; Quattrone, A.; Padua, L.; Gemignani, F.; et al. Is overwork weakness relevant in Charcot-Marie-Tooth disease? J. Neurol. Neurosurg. Psychiatry 2014, 85, 1354–1358. [Google Scholar] [CrossRef]
- Coraci, D.; Capobianco, S.V.; Romano, M.; Calvaruso, S.; Vecchio, M.; Giovannini, S.; Loreti, C.; Fusco, A.; Masiero, S.; Santilli, V.; et al. Neuropathic Pain and Ultrasonography: A Multiperspective Literature Evaluation. Diagnostics 2021, 11, 1705. [Google Scholar] [CrossRef]
- Panathoop, A.; Saengsuwan, J.; Vichiansiri, R. Effects of repetitive peripheral magnetic stimulation vs. conventional therapy in the management of carpal tunnel syndrome: A pilot randomized controlled trial. PeerJ 2023, 11, e15398. [Google Scholar] [CrossRef]
- Rayegani, S.M.; Moradi-Joo, M.; Raeissadat, S.A.; Bahrami, M.H.; Seyed-Nezhad, M.; Heidari, S. Effectiveness of Low-Level Laser Therapy compared to Ultrasound in Patients With Carpal Tunnel Syndrome: A Systematic Review and Meta-analysis. J. Lasers Med. Sci. 2019, 10, S82–S89. [Google Scholar] [CrossRef]
- Nuñez de Arenas-Arroyo, S.; Martínez-Vizcaíno, V.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Reina-Gutierrez, S.; Torres-Costoso, A. The Effect of Neurodynamic Techniques on the Dispersion of Intraneural Edema: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public. Health 2022, 19, 14472. [Google Scholar] [CrossRef]
- Sim, S.E.; Gunasagaran, J.; Goh, K.J.; Ahmad, T.S. Short-term clinical outcome of orthosis alone vs combination of orthosis, nerve, and tendon gliding exercises and ultrasound therapy for treatment of carpal tunnel syndrome. J. Hand Ther. 2019, 32, 411–416. [Google Scholar] [CrossRef]
- Shah, N.; Shrivastava, M.; Kumar, S.; Nagi, R.S. Supervised, individualised exercise reduces fatigue and improves strength and quality of life more than unsupervised home exercise in people with chronic Guillain-Barré syndrome: A randomised trial. J. Physiother. 2022, 68, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.L.; Chang, S.T. The effects of intravascular photobiomodulation on sleep disturbance caused by Guillain-Barré syndrome after Astrazeneca vaccine inoculation: Case report and literature review. Medicine (Baltimore) 2022, 101, e28758. [Google Scholar] [CrossRef]
- Wallace, A.; Pietrusz, A.; Dewar, E.; Dudziec, M.; Jones, K.; Hennis, P.; Sterr, A.; Baio, G.; Machado, P.M.; Laurá, M.; et al. Community exercise is feasible for neuromuscular diseases and can improve aerobic capacity. Neurology 2019, 92, e1773–e1785. [Google Scholar] [CrossRef] [PubMed]
- Pires, A.P.B.Á.; Silva, T.R.; Torres, M.S.; Diniz, M.L.; Tavares, M.C.; Gonçalves, D.U. Galvanic vestibular stimulation and its applications: A systematic review. Braz. J. Otorhinolaryngol. 2022, 88, S202–S211. [Google Scholar] [CrossRef] [PubMed]
- Tamburin, S.; Park, S.B.; Schenone, A.; Mantovani, E.; Hamedani, M.; Alberti, P.; Yildiz-Kabak, V.; Kleckner, I.R.; Kolb, N.; Mazzucchelli, M.; et al. Rehabilitation, exercise, and related non-pharmacological interventions for chemotherapy-induced peripheral neurotoxicity: Systematic review and evidence-based recommendations. Crit. Rev. Oncol. Hematol. 2022, 171, 103575. [Google Scholar] [CrossRef]
- van Netten, J.J.; Sacco, I.C.N.; Lavery, L.; Monteiro-Soares, M.; Paton, J.; Rasmussen, A.; Raspovic, A.; Bus, S.A. Clinical and biomechanical effectiveness of foot-ankle exercise programs and weight-bearing activity in people with diabetes and neuropathy: A systematic review and meta-analysis. Diabetes Metab. Res. Rev. 2023, e3649. [Google Scholar] [CrossRef]
- Chandrashekhar, R.; Wang, H.; Dionne, C.; James, S.; Burzycki, J. Wearable Focal Muscle Vibration on Pain, Balance, Mobility, and Sensation in Individuals with Diabetic Peripheral Neuropathy: A Pilot Study. Int. J. Environ. Res. Public. Health 2021, 18, 2415. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed]
- Ross, M.; Kargl, C.K.; Ferguson, R.; Gavin, T.P.; Hellsten, Y. Exercise-induced skeletal muscle angiogenesis: Impact of age, sex, angiocrines and cellular mediators. Eur. J. Appl. Physiol. 2023, 123, 1415–1432. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.D. Efficacy of tendon and nerve gliding exercises for carpal tunnel syndrome: A systematic review of randomized controlled trials. J. Phys. Ther. Sci. 2015, 27, 2645–2648. [Google Scholar] [CrossRef] [PubMed]
- Coraci, D.; Loreti, C.; Padua, L. Peripheral Nerve Blocks for Hand Procedures. N. Engl. J. Med. 2018, 379, 2181–2182. [Google Scholar] [CrossRef]
- Kramer, M.; Grimm, A.; Winter, N.; Dörner, M.; Grundmann-Hauser, K.; Stahl, J.H.; Wittlinger, J.; Kegele, J.; Kronlage, C.; Willikens, S. Nerve Ultrasound as Helpful Tool in Polyneuropathies. Diagnostics 2021, 11, 211. [Google Scholar] [CrossRef] [PubMed]
- Nampo, F.K.M.; Cavalheri, V.; Dos Santos Soares, F.; de Paula Ramos, S.; Camargo, E.A. Low-level phototherapy to improve exercise capacity and muscle performance: A systematic review and meta-analysis. Lasers Med. Sci. 2016, 31, 1957–1970. [Google Scholar] [CrossRef] [PubMed]
- Tahir, S.; Baig, M.O.; Rathore, F.A.; Aslam, H. The emerging role of focal muscle vibration in rehabilitation of neurological disorders. J. Pak. Med. Assoc. 2022, 72, 2126–2128. [Google Scholar] [PubMed]
- Szewczyk, A.K.; Jamroz-Wiśniewska, A.; Haratym, N.; Rejdak, K. Neuropathic pain and chronic pain as an underestimated interdisciplinary problem. Int. J. Occup. Med. Environ. Health 2022, 35, 249–264. [Google Scholar] [CrossRef]
- Deogaonkar, M. Peripheral Neuromodulation for Chronic Pain. Neurol. India 2020, 68, S224–S230. [Google Scholar] [CrossRef]
- Burgess, L.C.; Venugopalan, L.; Badger, J.; Street, T.; Alon, G.; Jarvis, J.C.; Wainwright, T.W.; Everington, T.; Taylor, P.; Swain, I.D. Effect of neuromuscular electrical stimulation on the recovery of people with COVID-19 admitted to the intensive care unit: A narrative review. J. Rehabil. Med. 2021, 53, jrm00164. [Google Scholar] [CrossRef]
- Carlson Strother, C.; Dittman, L.E.; Spinner, R.J.; Bishop, A.T.; Shin, A.Y. Surgical management of peroneal nerve injuries. Acta Neurochir. (Wien) 2023, 165, 2573–2580. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Most Frequent Words | |||
|---|---|---|---|
| rehabilitation teherapies | disease | nerve | |
| physical agent | entrapment | ulnar | |
| physical therapy | toxic | peroneal | |
| exercise | toxic | femoral | |
| manipulation | entrapment | radial | |
| mobilization | entrapment | radial | |
| electrotherapy | diabetic | median | |
| lasertherapy | entrapment | median | |
| ultrasound therapy | entrapment | radial | |
| stimulation | diabetic | tibial | |
| vibration therapy | diabetic | ||
| orthosis | entrapment | peroneal | |
| nerves | facial | stimulation; exercise; physical therapy | |
| median | stimulation; mobilization; exercise | ||
| ulnar | stimulation; mobilization; exercise | ||
| radial | stimulation; mobilization; exercise | ||
| peroneal | stimulation; exercise; orthosis | ||
| tibial | stimulation; exercise; mobilization | ||
| sural | stimulation; exercise | ||
| femoral | stimulation; mobilization; exercise | ||
| disesases | diabetic | exercise; stimulation; physical therapy | |
| entrapment | orthosis; exercise; stimulation | ||
| hereditary | exercise; physical therapy; orthosis | ||
| immune | exercise; physical therapy | ||
| toxic | exercise; physical therapy | ||
| tumor | stimulation; exercise; physical therapy | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coraci, D.; Romano, M.; Ragazzo, L.; Restivo, D.A.; Cipriani, M.; Gottardello, F.; Pizzolato, M.; Maccarone, M.C.; Masiero, S. Rehabilitation of Peripheral Neuropathies: From Lexical Analysis of the Literature to Identification of Clinical Protocols. J. Clin. Med. 2023, 12, 5879. https://doi.org/10.3390/jcm12185879
Coraci D, Romano M, Ragazzo L, Restivo DA, Cipriani M, Gottardello F, Pizzolato M, Maccarone MC, Masiero S. Rehabilitation of Peripheral Neuropathies: From Lexical Analysis of the Literature to Identification of Clinical Protocols. Journal of Clinical Medicine. 2023; 12(18):5879. https://doi.org/10.3390/jcm12185879
Chicago/Turabian StyleCoraci, Daniele, Marcello Romano, Lisa Ragazzo, Domenico Antonio Restivo, Martina Cipriani, Federica Gottardello, Martina Pizzolato, Maria Chiara Maccarone, and Stefano Masiero. 2023. "Rehabilitation of Peripheral Neuropathies: From Lexical Analysis of the Literature to Identification of Clinical Protocols" Journal of Clinical Medicine 12, no. 18: 5879. https://doi.org/10.3390/jcm12185879
APA StyleCoraci, D., Romano, M., Ragazzo, L., Restivo, D. A., Cipriani, M., Gottardello, F., Pizzolato, M., Maccarone, M. C., & Masiero, S. (2023). Rehabilitation of Peripheral Neuropathies: From Lexical Analysis of the Literature to Identification of Clinical Protocols. Journal of Clinical Medicine, 12(18), 5879. https://doi.org/10.3390/jcm12185879