
Determination of the Optimal Wavelength of the Hemolysis Index Measurement

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Measuring Instruments and Reagents
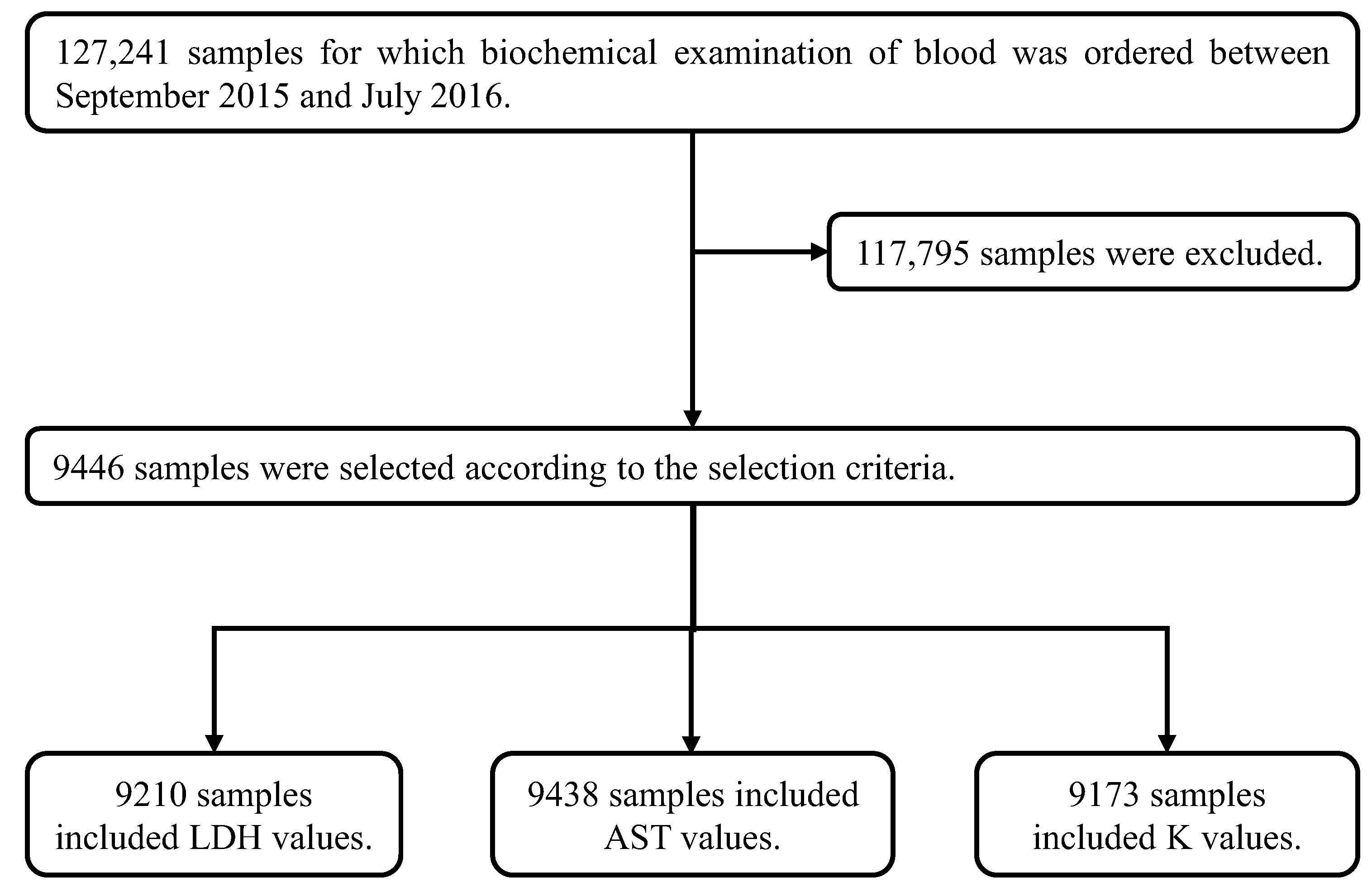
2.2. HI Measurements of Clinical Samples at the Four Different Wavelengths
2.3. Correlation of LDH, AST and K with HI in Clinical Samples
2.4. Statistical Analysis
3. Results
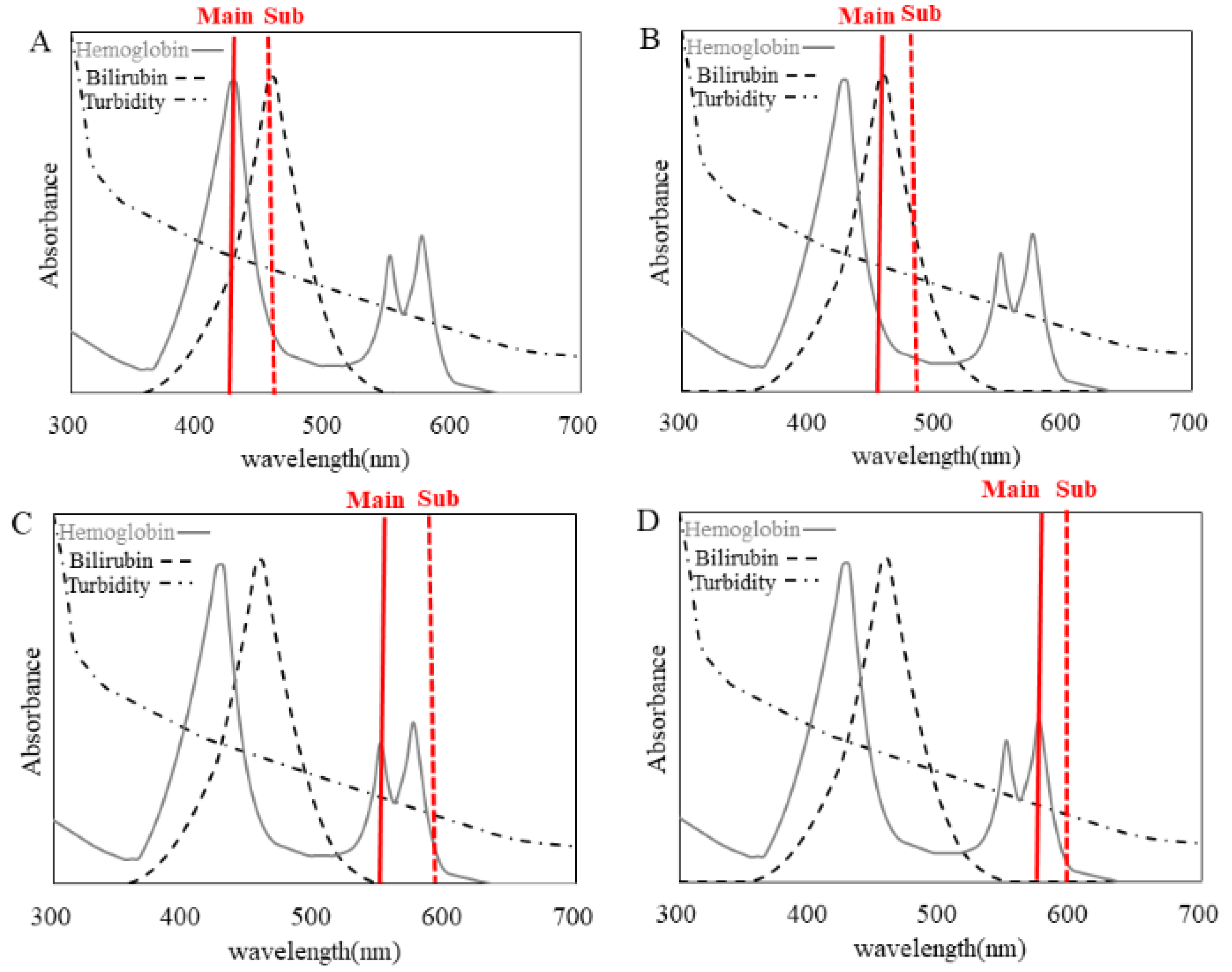
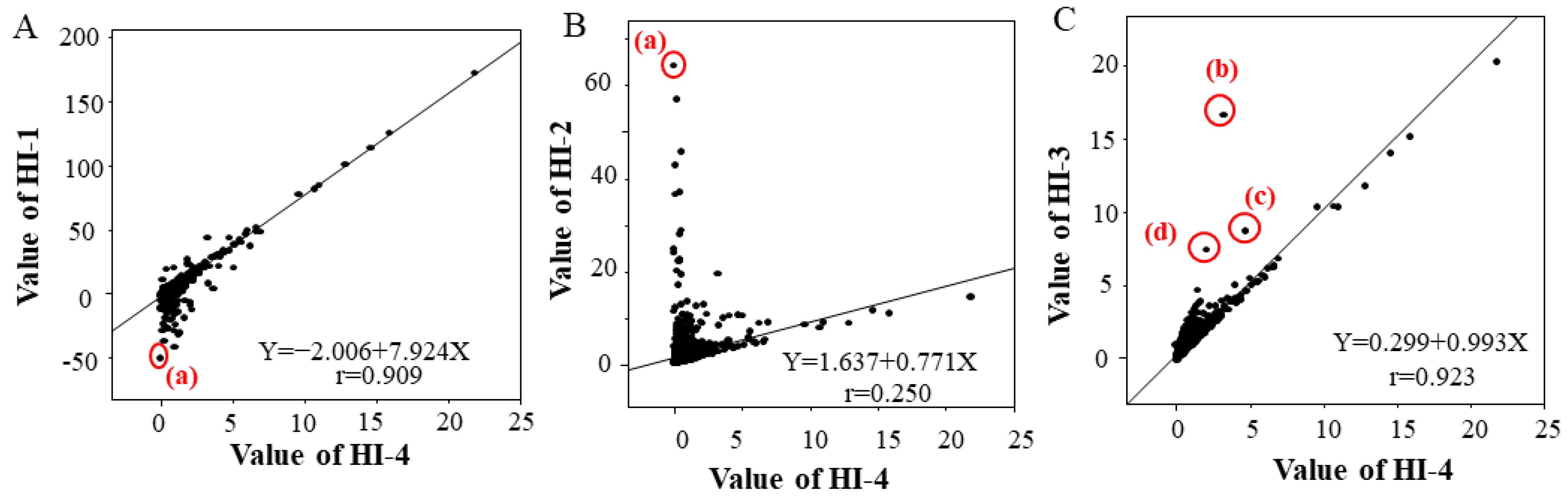
3.1. HI Measurement of Clinical Samples at Different Wavelengths
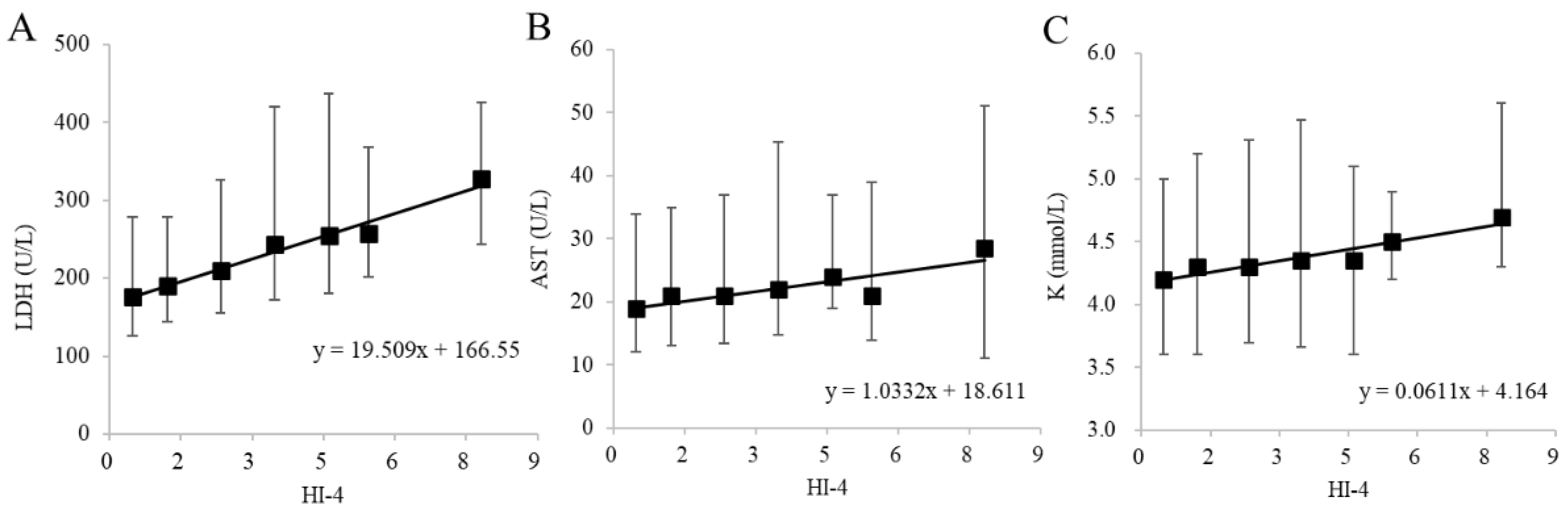
3.2. Correlation of LDH, AST and K with HI in Clinical Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lippi, G.; Blanckaert, N.; Bonini, P.; Green, S.; Kitchen, S.; Palicka, V.; Vassault, A.J.; Plebani, M. Haemolysis: An overview of the leading cause of unsuitable specimens in clinical laboratories. Clin. Chem. Lab. Med. 2008, 46, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Frank, J.J.; Bermes, E.W.; Bickel, M.J.; Watkins, B.F. Effect of in vitro hemolysis on chemical values for serum. Clin. Chem. 1978, 24, 1966–1970. [Google Scholar] [CrossRef]
- Caraway, W.T. Chemical and diagnostic specificity of laboratory tests. Effect of hemolysis, lipemia, anticoagulants, medications, contaminants, and other variables. Am. J. Clin. Pathol. 1962, 37, 445–464. [Google Scholar] [CrossRef]
- Kroll, M.H.; Elin, R.J. Interference with clinical laboratory analyses. Clin. Chem. 1994, 40, 1996–2005. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Salvagno, G.L.; Montagnana, M.; Brocco, G.; Guidi, G.C. Influence of hemolysis on routine clinical chemistry testing. Clin. Chem. Lab. Med. 2006, 44, 311–316. [Google Scholar] [CrossRef]
- Liamis, G.; Liberopoulos, E.; Barkas, F.; Elisaf, M. Spurious electrolyte disorders: A diagnostic challenge for clinicians. Am. J. Nephrol. 2013, 38, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R. Discrepancy between visual and spectrophotometric assessment of sample haemolysis. Ann. Clin. Biochem. 2002, 39, 521–522. [Google Scholar] [CrossRef]
- Glick, M.R.; Ryder, K.W.; Glick, S.J.; Woods, J.R. Unreliable visual estimation of the incidence and amount of turbidity, hemolysis, and icterus in serum from hospitalized patients. Clin. Chem. 1989, 35, 837–839. [Google Scholar] [CrossRef]
- Lippi, G.; Giavarina, D.; Gelati, M.; Salvagno, G.L. Reference range of hemolysis index in serum and lithium-heparin plasma measured with two analytical platforms in a population of unselected outpatients. Clin. Chim. Acta 2014, 429, 143–146. [Google Scholar] [CrossRef]
- Bonini, P.; Plebani, M.; Ceriotti, F.; Rubboli, F. Errors in laboratory medicine. Clin. Chem. 2002, 48, 691–698. [Google Scholar] [CrossRef]
- Jay, D.E.; Provasek, D. Characterization and mathematical correction of hemolysis interference in selected Hitachi 717 assays. Clin. Chem. 1993, 39, 1804–1810. [Google Scholar] [CrossRef]
- Marques-Garcia, F.; Jung, D.H.H.; Pérez, S.E. Impact of individualized hemolysis management based on biological variation cut-offs in a clinical laboratory. Ann. Lab. Med. 2022, 42, 169–177. [Google Scholar] [CrossRef]
- Zou, J.; Nolan, D.K.; LaFiore, A.R.; Scott, M.G. Estimating the effects of hemolysis on potassium and LDH laboratory results. Clin. Chim. Acta 2013, 421, 60–61. [Google Scholar] [CrossRef]
- Koseoglu, M.; Hur, A.; Atay, A.; Cuhadar, S. Effects of hemolysis interference on routine biochemistry parameters. Biochem. Med. 2011, 21, 79–85. [Google Scholar] [CrossRef]
- Yucel, D.; Dalva, K. Effect of in vitro hemolysis on 25 common biochemical tests. Clin. Chem. 1992, 38, 575–577. [Google Scholar] [CrossRef]
- Ishiguro, A.; Nishioka, M.; Morishige, A.; Kawano, R.; Kobayashi, T.; Fujinaga, A.; Takagi, F.; Kogo, T.; Morikawa, Y.; Okayama, N.; et al. What is the best wavelength for the measurement of hemolysis index? Clin. Chim. Acta 2020, 510, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Japanese Committee for Clinical Laboratory Standards (JCCLS). Common-Use Reference Intervals in Japan. Available online: https://www.jccls.org/wp-content/uploads/2022/10/kijyunhani20221031.pdf (accessed on 27 July 2023).
- Mansour, M.M.; Azzazy, H.M.; Kazmierczak, S.C. Correction factors for estimating potassium concentrations in samples with in vitro hemolysis: A detriment to patient safety. Arch. Pathol. Lab. Med. 2009, 133, 960–966. [Google Scholar] [CrossRef]
- Owens, H.; Siparsky, G.; Bajaj, L.; Hampers, L.C. Correction of factitious hyperkalemia in hemolyzed specimens. Am. J. Emerg. Med. 2005, 23, 872–875. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, A.M.; Bargnoux, A.S.; Kuster, N.; Cristol, J.P.; Badiou, S. Determination of hemolysis cut-offs for biochemical and immunochemical analytes according to their value. Clin. Chem. Lab. Med. 2020, 58, 1232–1241. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Cadamuro, J.; von Meyer, A.; Simundic, A.M.; European Federation of Clinical Chemistry and Laboratory Medicine (EFLM) Working Group for Preanalytical Phase (WG-PRE). Practical recommendations for managing hemolyzed samples in clinical chemistry testing. Clin. Chem. Lab. Med. 2018, 56, 718–727. [Google Scholar] [CrossRef]
- Lowe, G.; Stike, R.; Pollack, M.; Bosley, J.; O'Brien, P.; Hake, A.; Landis, G.; Billings, N.; Gordon, P.; Manzella, S.; et al. Nursing blood specimen collection techniques and hemolysis rates in an emergency department: Analysis of venipuncture versus intravenous catheter collection techniques. J. Emerg. Nurs. 2008, 34, 26–32. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Abbreviation *1 | Analyte Name | Unit | Method | Product Name | Reagent Manufacturer |
|---|---|---|---|---|---|
| LDH | Lactate dehydrogenase | U/L | Enzymatic method *2 | L-type LD.J | FUJIFILM Wako Pure Chemical Co., Ltd. Osaka City, Osaka, Japan |
| AST | Aspartate aminotransferase | U/L | Enzymatic method *2 | L-type AST.J2 | FUJIFILM Wako Pure Chemical Co., Ltd. Osaka City, Osaka, Japan |
| ALT | Alanine aminotransferase | U/L | Enzymatic method *2 | L-type ALT.J2 | FUJIFILM Wako Pure Chemical Co., Ltd. Osaka City, Osaka, Japan |
| GGT | γ-glutamyltransferase | U/L | Enzymatic method *2 | Quick Auto Neo γ-GT JS | Shino-Test Corp. Chiyoda, Tokyo, Japan |
| TP | Total proteins | g/dL | Biuret method | Aqua-auto Kainos TP-II | Kainos Laboratories, Inc. Bunkyo, Tokyo, Japan |
| ALB | Albumin | g/dL | Advanced BCP method | Aqua-auto Kainos ALB | Kainos Laboratories, Inc. Bunkyo, Tokyo, Japan |
| TG | Triglyceride | mg/dL | FG eliminating enzyme method | Determiner L TG II | Minaris Medical Co., Ltd. Chuo, Tokyo, Japan |
| TC | Total cholesterol | mg/dL | Cholesterol oxidase method | Determiner L TC II | Minaris Medical Co., Ltd. Chuo, Tokyo, Japan |
| HDL-C | HDL cholesterol | mg/dL | Selective inhibition method | MetaboLead HDL-C | Minaris Medical Co., Ltd. Chuo, Tokyo, Japan |
| LDL-C | LDL cholesterol | mg/dL | Selective solubilization method | MetaboLead LDL-C | Minaris Medical Co., Ltd. Chuo, Tokyo, Japan |
| UN | Urea nitrogen | mg/dL | Urease GLDH method | Aqua-auto Kainos UN-II | Kainos Laboratories, Inc. Bunkyo, Tokyo, Japan |
| UA | Uric acid | mg/dL | Uricase–POD method | Determiner L UA | Minaris Medical Co., Ltd. Chuo, Tokyo, Japan |
| CRE | Creatinine | mg/dL | Enzymatic method | Cygnus Auto CRE | Shino-Test Corp. Chiyoda, Tokyo, Japan |
| T-BIL | Total bilirubin | mg/dL | Vanadate oxidation method | Total Bilirubin E HA | FUJIFILM Wako Pure Chemical Co., Ltd. Osaka City, Osaka, Japan |
| K | Potassium | mmol/L | Ion-selective electrode method | EA08M *3 | A & T Co., Ltd. Yokohama City, Kanagawa, Japan |
| Sample No. | (a) | (b) | (c) | (d) |
|---|---|---|---|---|
| Picture of serum |  |  |  |  |
| TG (mg/dL) | 167.6 | 684.8 | 480.6 | 1230.9 |
| TC (mg/dL) | 141.7 | 100.9 | 224.4 | 210.3 |
| HDL-C (mg/dL) | 8.7 | 44.6 | 25.4 | 21.6 |
| LDL-C (mg/dL) | 31.2 | 22.8 | 138.9 | 5.9 |
| T-BIL (mg/dL) | 28.1 | 1.2 | 0.4 | 0.67 |
| Item | Male | Female |
|---|---|---|
| Age (years) | 18–70 | |
| TP (g/dL) | 6.4–8.1 | |
| ALB (g/dL) | 3.7–5.1 | |
| CRE (mg/dL) | 0.60–1.15 | 0.40–0.85 |
| UA (mg/dL) | 3.5–8.2 | 2.5–6.0 |
| ALT (U/L) | 10–45 | 7–27 |
| GGT (U/L) | 13–70 | 9–36 |
| UN (mg/dL) | 7–24 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishiguro, A.; Nishioka, M.; Morishige, A.; Yoneshiro, M.; Shinkawa, K.; Fujinaga, A.; Kobayashi, T.; Suehiro, Y.; Yamasaki, T. Determination of the Optimal Wavelength of the Hemolysis Index Measurement. J. Clin. Med. 2023, 12, 5864. https://doi.org/10.3390/jcm12185864
Ishiguro A, Nishioka M, Morishige A, Yoneshiro M, Shinkawa K, Fujinaga A, Kobayashi T, Suehiro Y, Yamasaki T. Determination of the Optimal Wavelength of the Hemolysis Index Measurement. Journal of Clinical Medicine. 2023; 12(18):5864. https://doi.org/10.3390/jcm12185864
Chicago/Turabian StyleIshiguro, Akiyo, Mitsuaki Nishioka, Akihiro Morishige, Mai Yoneshiro, Kanae Shinkawa, Aki Fujinaga, Toshihiko Kobayashi, Yutaka Suehiro, and Takahiro Yamasaki. 2023. "Determination of the Optimal Wavelength of the Hemolysis Index Measurement" Journal of Clinical Medicine 12, no. 18: 5864. https://doi.org/10.3390/jcm12185864
APA StyleIshiguro, A., Nishioka, M., Morishige, A., Yoneshiro, M., Shinkawa, K., Fujinaga, A., Kobayashi, T., Suehiro, Y., & Yamasaki, T. (2023). Determination of the Optimal Wavelength of the Hemolysis Index Measurement. Journal of Clinical Medicine, 12(18), 5864. https://doi.org/10.3390/jcm12185864