
Swiss Pilot Low-Dose CT Lung Cancer Screening Study: First Baseline Screening Results
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
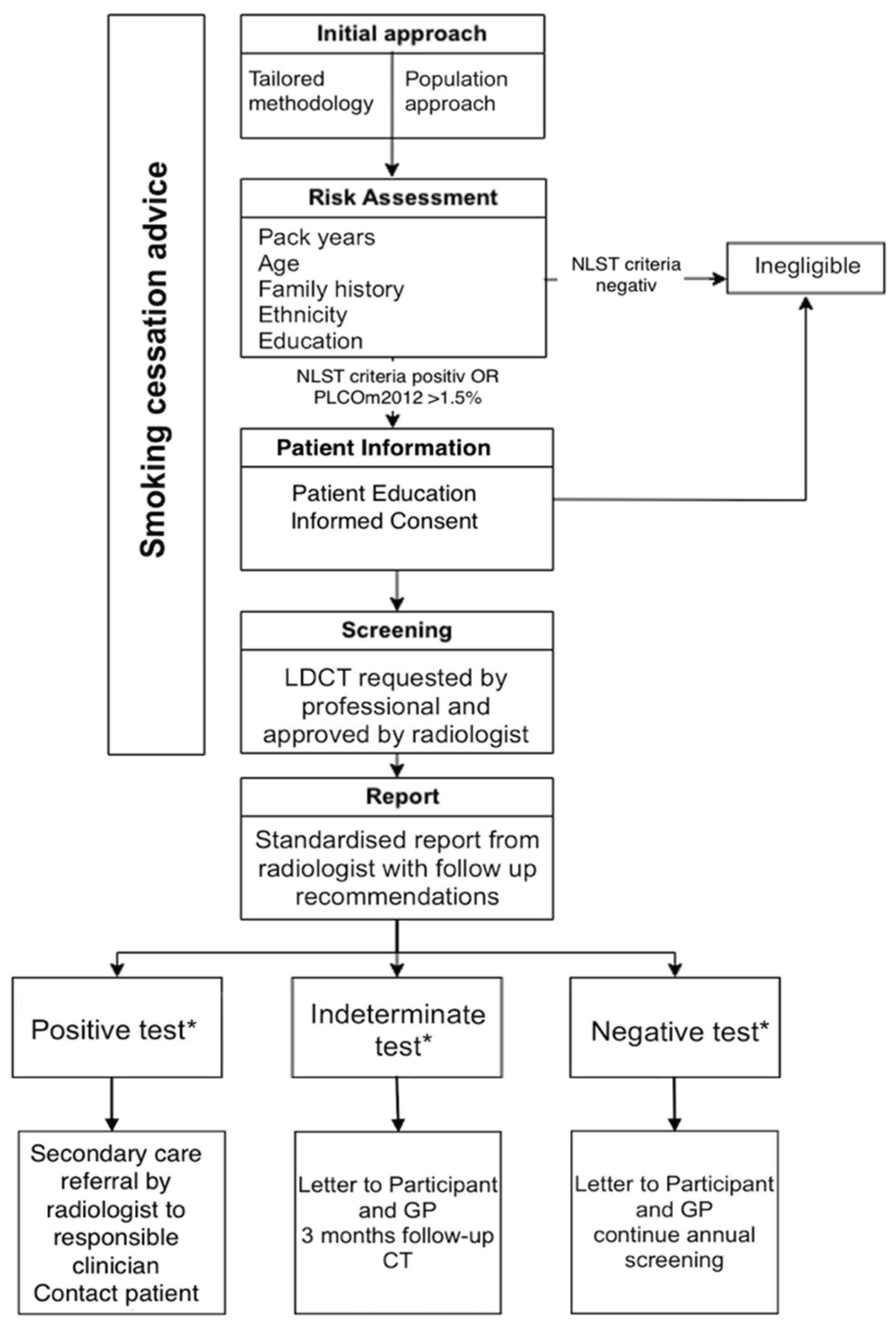
2.1. Study Design
2.2. Inclusion Criteria
- Age from 55 to 74 years;
- Willingness and ability to undergo LDCT;
- >30 packs years;
- Current or former smoker who quit smoking ≤ 15 years ago;
- No previous diagnosis of lung cancer;
- No major medical problems;
- No CT scan in the last 18 months;
- No haemoptysis or weight loss > 7 kg in the last year.
2.3. Recruitment
2.4. Image Acquisition/Reporting
2.5. Ethical Statement
2.6. Primary and Secondary Endpoint
2.7. Statistical Analysis
3. Results
3.1. Participant Cohort
3.2. Radiation Dose
3.3. Lung-RADS Findings
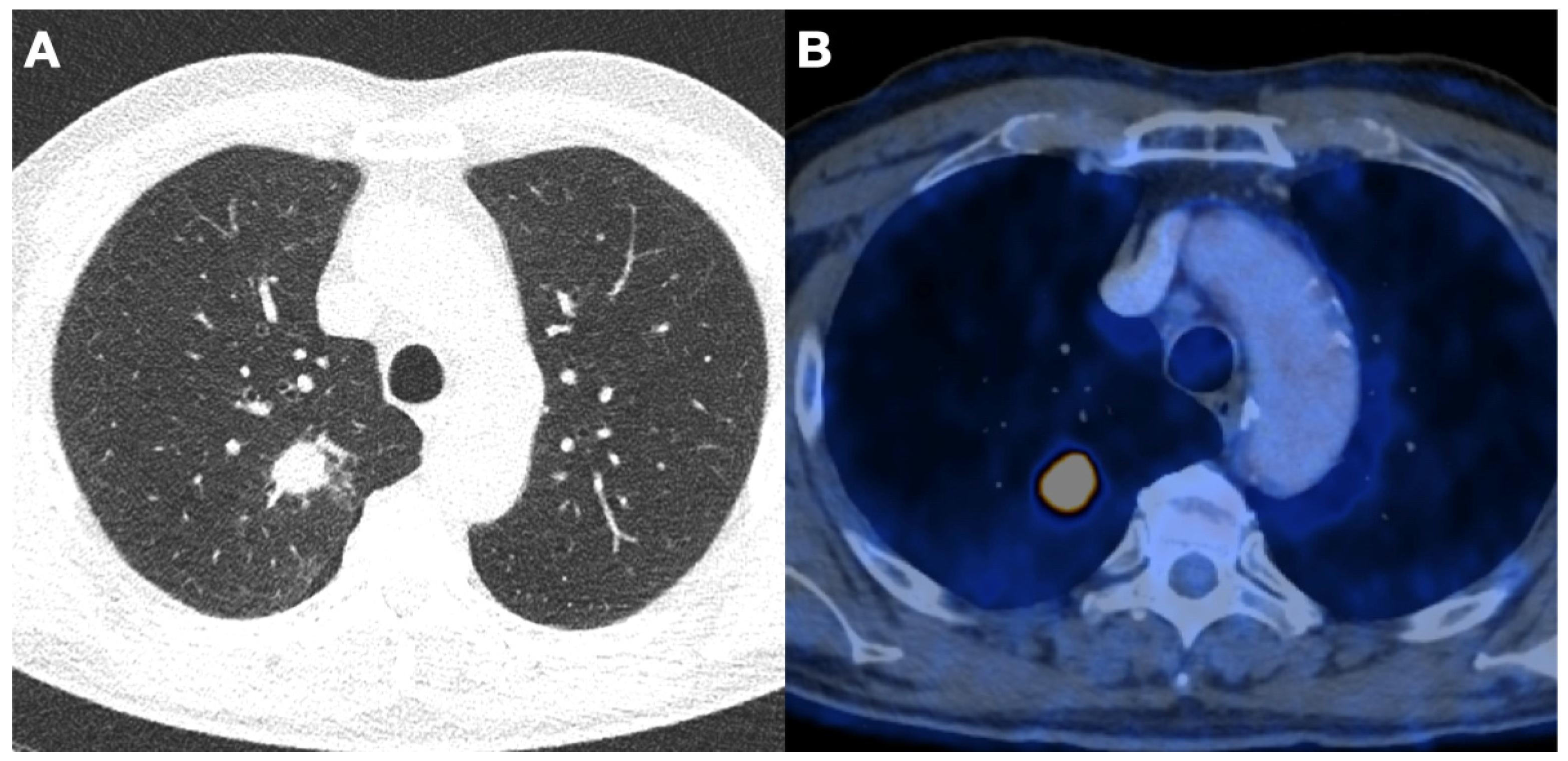
3.4. Detected Lung Cancer
3.5. Incidental Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Adamek, M.; Szablowska-Siwik, S.; Peled, N.; Rzyman, W.; Grodzki, W.; Czyzewski, D. Low-dose computed-tomography lung cancer screening: The first European recommendations from the European Society of Radiology and European Respiratory Society. Pol. Arch. Med. Wewn. 2015, 125, 607–609. [Google Scholar] [PubMed]
- Chopra, I.; Chopra, A.; Bias, T.K. Reviewing risks and benefits of low-dose computed tomography screening for lung cancer. Postgrad. Med. 2016, 128, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Force, U.S.P.S.T. Lung cancer screening: Recommendation statement. Ann. Intern. Med. 2004, 140, 738–739. [Google Scholar] [CrossRef]
- Jonas, D.E.; Reuland, D.S.; Reddy, S.M.; Nagle, M.; Clark, S.D.; Weber, R.P.; Enyioha, C.; Malo, T.L.; Brenner, A.T.; Armstrong, C.; et al. Screening for Lung Cancer With Low-Dose Computed Tomography: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2021, 325, 971–987. [Google Scholar] [CrossRef]
- de Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- National Lung Screening Trial Research, T.; Aberle, D.R.; Adams, A.M.; Berg, C.D.; Black, W.C.; Clapp, J.D.; Fagerstrom, R.M.; Gareen, I.F.; Gatsonis, C.; Marcus, P.M.; et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef]
- Aberle, D.R. Implementing lung cancer screening: The US experience. Clin. Radiol. 2017, 72, 401–406. [Google Scholar] [CrossRef]
- ECHAlliance. Croatia First to Introduce Early Screening for Lung Cancer. Available online: https://echalliance.com/croatia-first-to-introduce-early-screening-for-lung-cancer/ (accessed on 20 January 2020).
- Rzyman, W.; Didkowska, J.; Dziedzic, R.; Grodzki, T.; Orlowski, T.; Szurowska, E.; Langfort, R.; Biernat, W.; Kowalski, D.; Dyszkiewicz, W.; et al. Consensus statement on a screening programme for the detection of early lung cancer in Poland. Adv. Respir. Med. 2018, 86, 53–74. [Google Scholar] [CrossRef]
- Nahorecki, A.; Chabowski, M.; Kuzniar, T.; Kedzierski, B.; Jazwiec, P.; Szuba, A.; Janczak, D. Low-dose computer tomography as a screening tool for lung cancer in a high risk population. Adv. Exp. Med. Biol. 2015, 852, 31–37. [Google Scholar] [CrossRef]
- Crosbie, P.A.; Balata, H.; Evison, M.; Atack, M.; Bayliss-Brideaux, V.; Colligan, D.; Duerden, R.; Eaglesfield, J.; Edwards, T.; Elton, P.; et al. Implementing lung cancer screening: Baseline results from a community-based ‘Lung Health Check’ pilot in deprived areas of Manchester. Thorax 2019, 74, 405–409. [Google Scholar] [CrossRef]
- Suisse, C. Heath-Pocket Statistics. Available online: https://www.bfs.admin.ch/bfs/en/home/statistics/health.assetdetail.24131868.html (accessed on 24 February 2023).
- Observatory, S.H. Tobacco Consumption. Available online: https://ind.obsan.admin.ch/en/indicator/monam/tobacco-consumption-age-15 (accessed on 30 November 2022).
- Tomonaga, Y.; Ten Haaf, K.; Frauenfelder, T.; Kohler, M.; Kouyos, R.D.; Shilaih, M.; Lorez, M.; de Koning, H.J.; Schwenkglenks, M.; Puhan, M.A. Cost-effectiveness of low-dose CT screening for lung cancer in a European country with high prevalence of smoking-A modelling study. Lung Cancer 2018, 121, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Tammemagi, M.C.; Ruparel, M.; Tremblay, A.; Myers, R.; Mayo, J.; Yee, J.; Atkar-Khattra, S.; Yuan, R.; Cressman, S.; English, J.; et al. USPSTF2013 versus PLCOm2012 lung cancer screening eligibility criteria (International Lung Screening Trial): Interim analysis of a prospective cohort study. Lancet Oncol. 2022, 23, 138–148. [Google Scholar] [CrossRef]
- Field, J.K.; Duffy, S.W.; Baldwin, D.R.; Brain, K.E.; Devaraj, A.; Eisen, T.; Green, B.A.; Holemans, J.A.; Kavanagh, T.; Kerr, K.M.; et al. The UK Lung Cancer Screening Trial: A pilot randomised controlled trial of low-dose computed tomography screening for the early detection of lung cancer. Health Technol. Assess. 2016, 20, 1–146. [Google Scholar] [CrossRef] [PubMed]
- Minerva, E.M.; Tessitore, A.; Cafarotti, S.; Patella, M. Urban-Rural Disparities in the Lung Cancer Surgical Treatment Pathway: The Paradox of a Rich, Small Region. Front. Surg. 2022, 9, 884048. [Google Scholar] [CrossRef] [PubMed]
- Damhus, C.S.; Quentin, J.G.; Malmqvist, J.; Siersma, V.; Brodersen, J. Psychosocial consequences of a three-month follow-up after receiving an abnormal lung cancer CT-screening result: A longitudinal survey. Lung Cancer 2021, 155, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, J.F.; Siersma, V.; Malmqvist, J.; Brodersen, J. Psychosocial consequences of false positives in the Danish Lung Cancer CT Screening Trial: A nested matched cohort study. BMJ Open 2020, 10, e034682. [Google Scholar] [CrossRef]
- Yankaskas, B.C.; Cleveland, R.J.; Schell, M.J.; Kozar, R. Association of recall rates with sensitivity and positive predictive values of screening mammography. AJR Am. J. Roentgenol. 2001, 177, 543–549. [Google Scholar] [CrossRef]
- National Lung Screening Trial Research, T. Lung Cancer Incidence and Mortality with Extended Follow-up in the National Lung Screening Trial. J. Thorac. Oncol. 2019, 14, 1732–1742. [Google Scholar] [CrossRef]
- Arcadi, T.; Maffei, E.; Sverzellati, N.; Mantini, C.; Guaricci, A.I.; Tedeschi, C.; Martini, C.; La Grutta, L.; Cademartiri, F. Coronary artery calcium score on low-dose computed tomography for lung cancer screening. World J. Radiol. 2014, 6, 381–387. [Google Scholar] [CrossRef]
- Fan, L.; Fan, K. Lung cancer screening CT-based coronary artery calcification in predicting cardiovascular events: A systematic review and meta-analysis. Medicine (Baltimore) 2018, 97, e10461. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.T.; Onuma, O.K.; Massaro, J.M.; D’Agostino Sr, R.B.; O’Donnell, C.J.; Hoffmann, U. Lung Cancer Screening Eligibility in the Community: Cardiovascular Risk Factors, Coronary Artery Calcification, and Cardiovascular Events. Circulation 2016, 134, 897–899. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, T.; Kober, L.; Abdulla, J.; Pedersen, J.H.; Wille, M.M.; Dirksen, A.; Kofoed, K.F. Coronary artery calcification detected in lung cancer screening predicts cardiovascular death. Scand. Cardiovasc. J. 2015, 49, 159–167. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Subject Demographic/Socioeconomic Characteristic Risk Evaluation | Results | |
|---|---|---|
| Demographics/Socioeconomics | ||
| Gender (Number, (%)) | ||
| Male | 65 (58) | |
| Female | 47 (42) | |
| Age (Median, (p25–75%)) | 61.5 (57.0–67.0) | |
| Ethnicity (Number, (%)) | ||
| Black | 0 (0) | |
| Hispanic | 2 (2) | |
| Asian | 0 (0) | |
| White | 110 (98) | |
| Other (included mixed race) | 0 (0) | |
| Education Level (Number, (%)) | ||
| Less than high-school | 1 (1) | |
| High-school | 17 (15) | |
| Post high-school training | 35 (31) | |
| College degree | 41 (37) | |
| Postgraduate/Professional | 18 (16) | |
| Risk Evaluation | ||
| BMI (Median, (p25–75%)) | 25.6 (23.3–28.0) | |
| Smoking status (Number, (%)) | ||
| current | 85 (76) | |
| former | 27 (24) | |
| Pack years (Median, (p25–75%)) | 45 (38–57) | |
| History of COPD, Emphysema or Chron. Bronchitis (Number, (%)) | 16 (14) | |
| PCLOm 2012 (Mean (SD)) | 3.7 (2.5) | |
| Screening Results | ||
|---|---|---|
| LUNG-RADS | Results | |
| 0 (Number, (%)) | 0 (0) | |
| 1 (Number, (%)) | 62 (55) | |
| 2 (Number, (%)) | 29 (26) | |
| 3 (Number, (%)) | 14 (13) | |
| 4a (Number, (%)) | 3 (3) | |
| 4b (Number, (%)) | 4 (4) | |
| Carcinomas (Number, (%)) | 4 (4) | |
| Adenocarcinoma | 3 (3) | |
| Squamous cell carcinoma | 1 (1) | |
| Incidental Findings | ||
| Coronary Sclerosis (Number, (%)) | ||
| non | 32 (29) | |
| mild | 38 (34) | |
| moderate | 32 (29) | |
| severe | 10 (10) | |
| Emphysema (Number, (%)) | 36 (32) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jungblut, L.; Etienne, H.; Zellweger, C.; Matter, A.; Patella, M.; Frauenfelder, T.; Opitz, I. Swiss Pilot Low-Dose CT Lung Cancer Screening Study: First Baseline Screening Results. J. Clin. Med. 2023, 12, 5771. https://doi.org/10.3390/jcm12185771
Jungblut L, Etienne H, Zellweger C, Matter A, Patella M, Frauenfelder T, Opitz I. Swiss Pilot Low-Dose CT Lung Cancer Screening Study: First Baseline Screening Results. Journal of Clinical Medicine. 2023; 12(18):5771. https://doi.org/10.3390/jcm12185771
Chicago/Turabian StyleJungblut, Lisa, Harry Etienne, Caroline Zellweger, Alessandra Matter, Miriam Patella, Thomas Frauenfelder, and Isabelle Opitz. 2023. "Swiss Pilot Low-Dose CT Lung Cancer Screening Study: First Baseline Screening Results" Journal of Clinical Medicine 12, no. 18: 5771. https://doi.org/10.3390/jcm12185771
APA StyleJungblut, L., Etienne, H., Zellweger, C., Matter, A., Patella, M., Frauenfelder, T., & Opitz, I. (2023). Swiss Pilot Low-Dose CT Lung Cancer Screening Study: First Baseline Screening Results. Journal of Clinical Medicine, 12(18), 5771. https://doi.org/10.3390/jcm12185771