



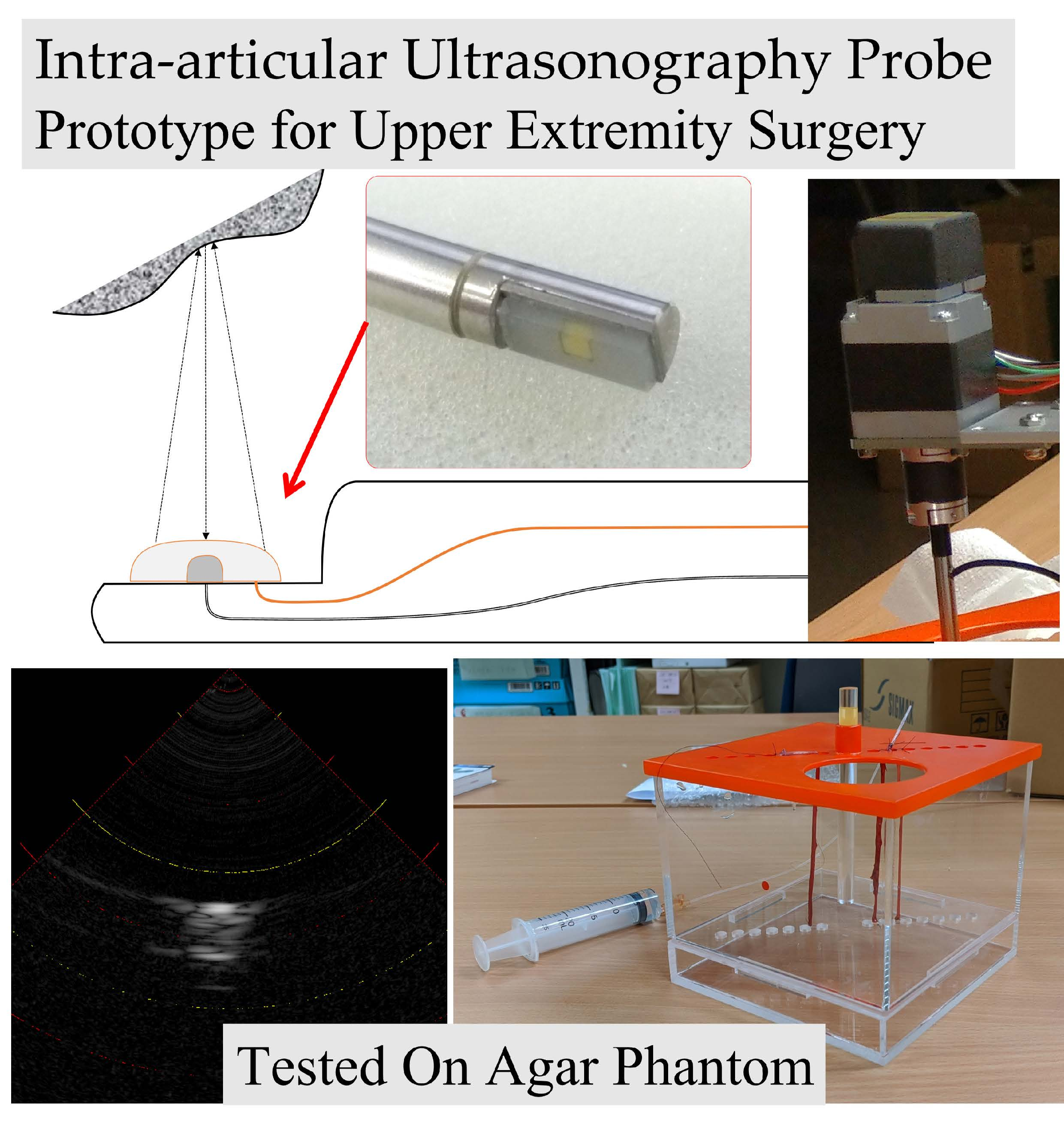
Intra-Articular Ultrasonography Probe for Minimally Invasive Upper Extremity Arthroscopic Surgery: A Phantom Study


Abstract
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
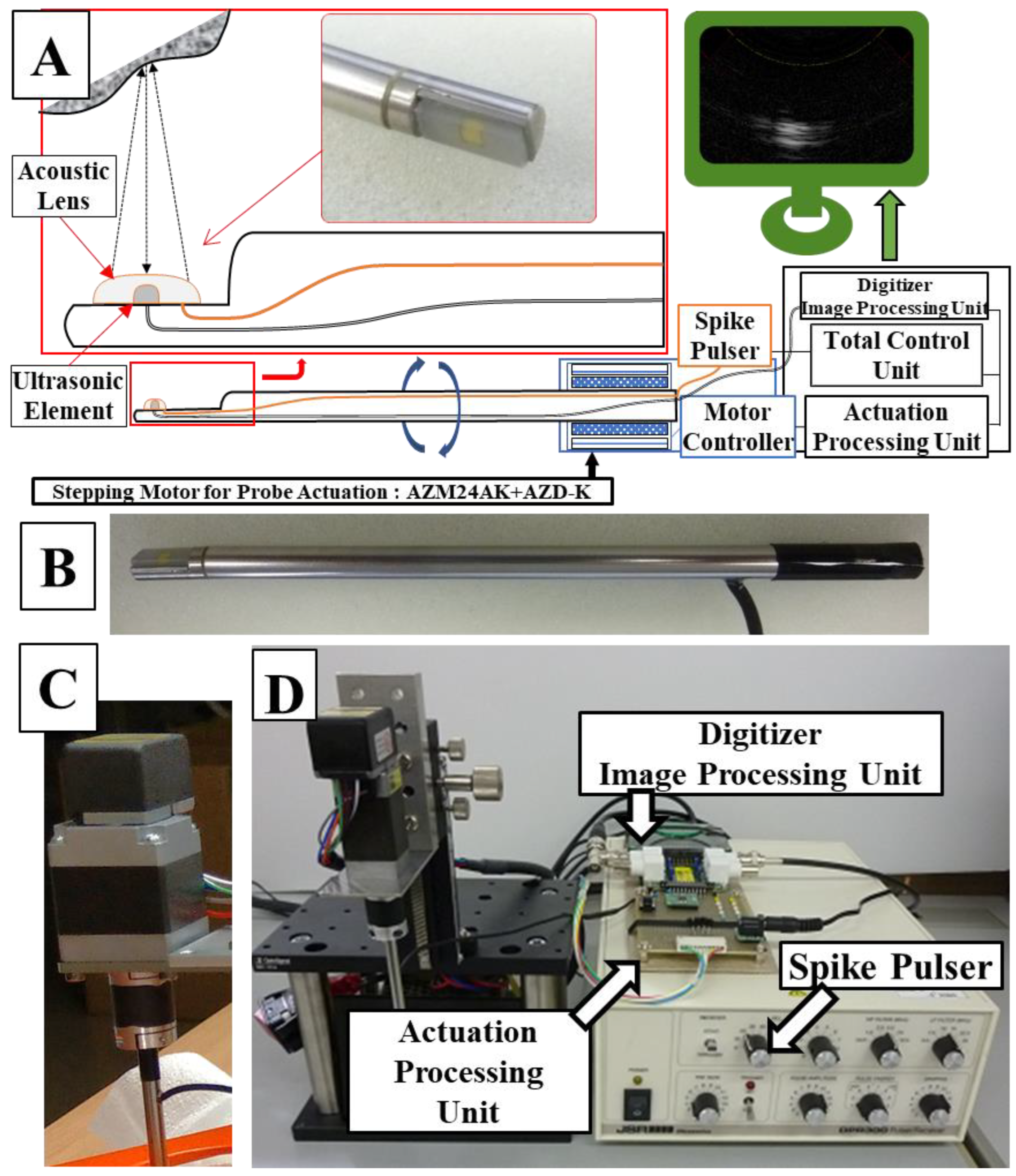
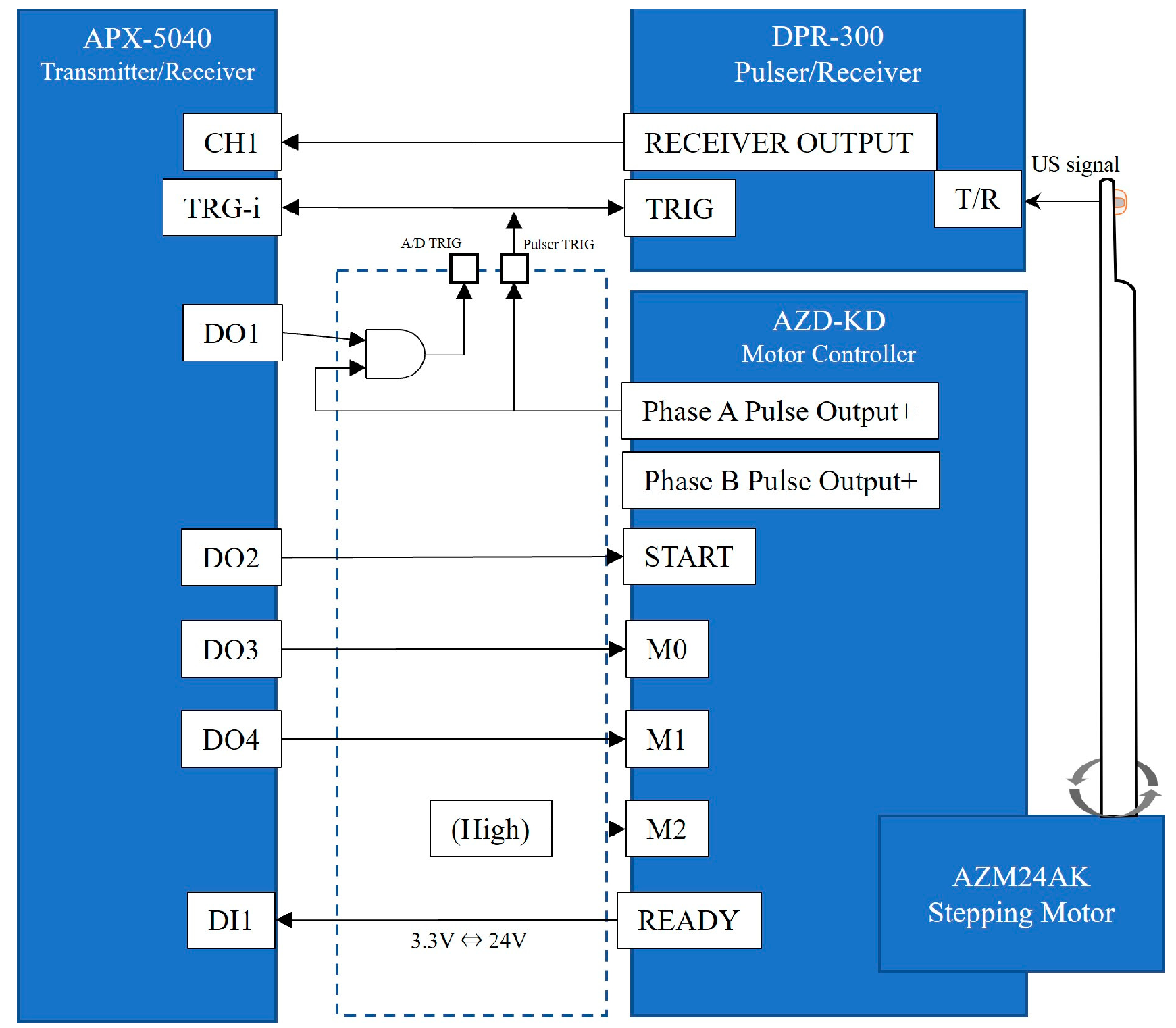
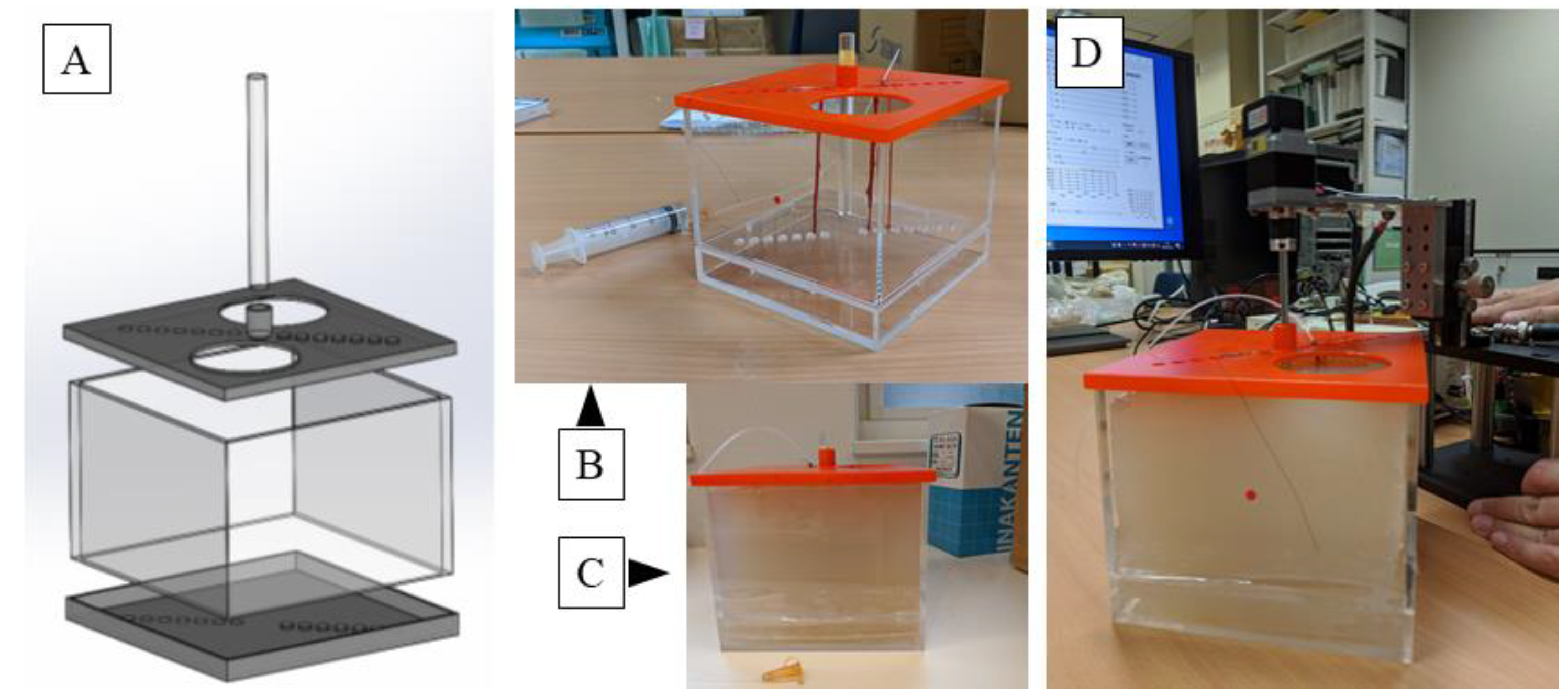
2.1. Setup of an Arthroscopic Ultrasonography Probe System
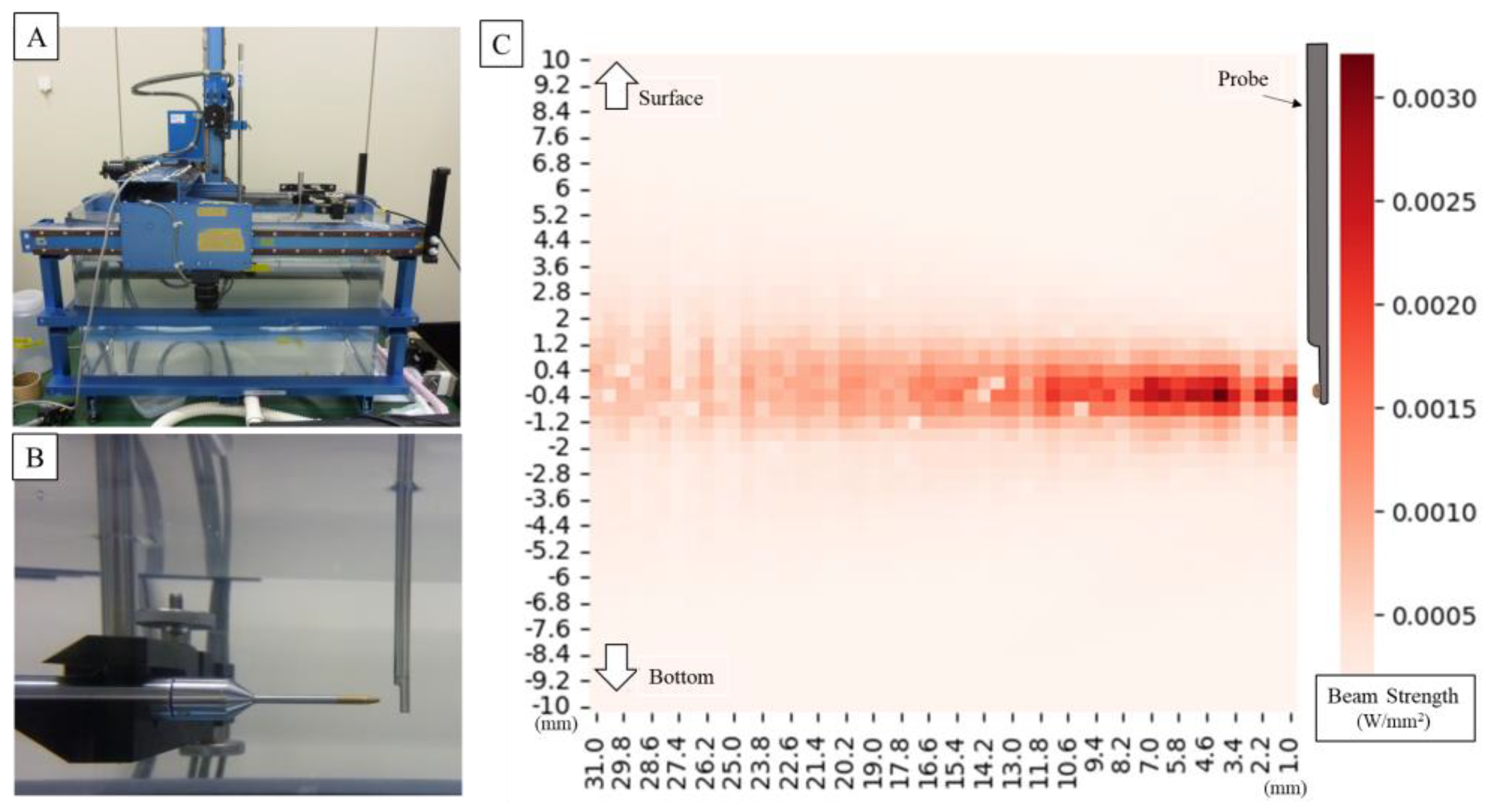
2.2. Evaluation of the System under Acoustic Measuring
2.3. Verification of the System Using a Phantom
3. Results
3.1. Probe Sound Field Property Measurement
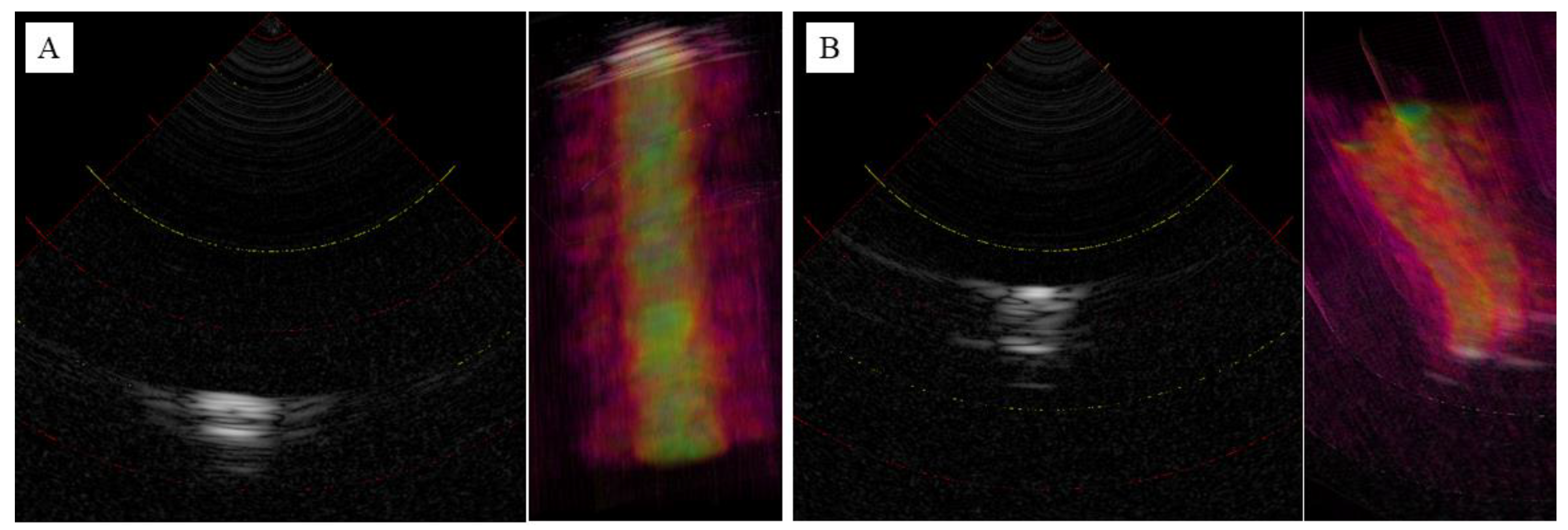
3.2. Observation of the Agar Phantom
4. Discussion
5. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Randelli, P.; Dejour, D.; van Dijk, C.N.; Denti, M.; Seil, R. Arthroscopy: Basic to Advanced; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Ahmed, A.F.; Alzobi, O.Z.; Hantouly, A.T.; Toubasi, A.; Farsakoury, R.; Alkhelaifi, K.; Zikria, B. Complications of Elbow Arthroscopic Surgery: A Systematic Review and Meta-analysis. Orthop. J. Sports Med. 2022, 10, 23259671221137863. [Google Scholar] [CrossRef] [PubMed]
- Atesok, K.; Doral, M.N.; Whipple, T.; Mann, G.; Mei-Dan, O.; Atay, O.A.; Beer, Y.; Lowe, J.; Soudry, M.; Schemitsch, E.H. Arthroscopy-assisted fracture fixation. Knee Surg. Sports Traumatol. Arthrosc. 2011, 19, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Beredjiklian, P.K.; Bozentka, D.J.; Leung, Y.L.; Monaghan, B.A. Complications of wrist arthroscopy. J. Hand Surg. Am. 2004, 29, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Stetson, W.B.; Vogeli, K.; Chung, B.; Hung, N.J.; Stevanovic, M.; Morgan, S. Avoiding Neurological Complications of Elbow Arthroscopy. Arthrosc. Tech. 2018, 7, e717–e724. [Google Scholar] [CrossRef] [PubMed]
- Harrison, W.D.; Tonge, X.; Bhalaik, V. Avoiding complications in elbow arthroscopy. J. Arthrosc. Joint Surg. 2019, 6, 42–47. [Google Scholar] [CrossRef]
- Tsenkov, T.; Dimitrov, N. A systematic review of elbow arthroscopy complications: Complications, risk factors, and safety tips. Int. Orthop. 2022, 46, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Temporin, K.; Miyoshi, Y.; Miyamura, S.; Oura, K.; Shimada, K. Risk of nerve injury during elbow arthroscopy: Ultrasonographic evaluation of preoperative patients. J. Shoulder Elbow Surg. 2023, 32, 486–491. [Google Scholar] [CrossRef]
- Shiode, R.; Oka, K.; Shigi, A.; Miyamura, S.; Tanaka, H.; Mae, T.; Murase, T. Arthroscopic Debridement of Elbow Osteoarthritis Using CT-Based Computer-Aided Navigation Systems Is Accurate. Arthrosc. Sports Med. Rehabil. 2021, 3, e1687–e1696. [Google Scholar] [CrossRef]
- Unglaub, F.; Spies, C. Augmented reality-based navigation system for wrist arthroscopy: Feasibility. J. Wrist Surg. 2014, 3, 66. [Google Scholar] [CrossRef][Green Version]
- Yamamoto, M.; Tawara, T.; Oyama, S.; Murakami, Y.; Yokota, H.; Hirata, H. Augmented Reality-enhanced Elbow Arthroscopy. J. Hand Surg. 2017, 42, S51–S52. [Google Scholar] [CrossRef][Green Version]
- Ge, X.; Ge, X.; Wang, C.; Liu, Q.; Wang, B.; Chen, L.; Cheng, K.; Qin, M. Application of ultrasound in avoiding radial nerve injury during elbow arthroscopy: A retrospective follow-up study. BMC Musculoskelet. Disord. 2022, 23, 1126. [Google Scholar] [CrossRef] [PubMed]
- Liukkonen, J.; Hirvasniemi, J.; Joukainen, A.; Penttila, P.; Viren, T.; Saarakkala, S.; Kroger, H.; Jurvelin, J.S.; Toyras, J. Arthroscopic ultrasound technique for simultaneous quantitative assessment of articular cartilage and subchondral bone: An in vitro and in vivo feasibility study. Ultrasound Med. Biol. 2013, 39, 1460–1468. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.R.; Fowlkes, J.B.; Abramowicz, J.S.; Church, C.C. Ultrasound biosafety considerations for the practicing sonographer and sonologist. J. Ultrasound Med. 2009, 28, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, C.; Mathoulin, C. Complications of Wrist Arthroscopy: A Multicenter Study Based on 10,107 Arthroscopies. J. Wrist Surg. 2016, 5, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Wilkens, S.C.; Bargon, C.A.; Mohamadi, A.; Chen, N.C.; Coert, J.H. A systematic review and meta-analysis of arthroscopic assisted techniques for thumb carpometacarpal joint osteoarthritis. J. Hand Surg. Eur. Vol. 2018, 43, 1098–1105. [Google Scholar] [CrossRef] [PubMed]
- Benson, L.S.; Bare, A.A.; Nagle, D.J.; Harder, V.S.; Williams, C.S.; Visotsky, J.L. Complications of endoscopic and open carpal tunnel release. Arthroscopy 2006, 22, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, Z.S.; Yao, J. Complications of Wrist and Hand Arthroscopy. Hand Clin. 2017, 33, 831–838. [Google Scholar] [CrossRef]
- Bhatia, D.N.; Bain, G.I.; Poehling, G.G.; Graves, B.R. Arthroscopy and Endoscopy of the Elbow, Wrist and Hand; Springer: Berlin/Heidelberg, Germany, 2022. [Google Scholar]
- Mhaskar, V.A.; Agrahari, H.; Maheshwari, J. Ultrasound guided arthroscopic meniscus surgery. J. Ultrasound. 2023, 26, 577–581. [Google Scholar] [CrossRef]
- Liukkonen, J.; Lehenkari, P.; Hirvasniemi, J.; Joukainen, A.; Viren, T.; Saarakkala, S.; Nieminen, M.T.; Jurvelin, J.S.; Toyras, J. Ultrasound arthroscopy of human knee cartilage and subchondral bone in vivo. Ultrasound Med. Biol. 2014, 40, 2039–2047. [Google Scholar] [CrossRef]
- Spahn, G.; Felmet, G.; Hofmann, G.O. Traumatic and degenerative cartilage lesions: Arthroscopic differentiation using near-infrared spectroscopy (NIRS). Arch. Orthop. Trauma. Surg. 2013, 133, 997–1002. [Google Scholar] [CrossRef]
- Yamamoto, M.; Oyama, S.; Otsuka, S.; Murakami, Y.; Yokota, H.; Hirata, H. Experimental pilot study for augmented reality-enhanced elbow arthroscopy. Sci. Rep. 2021, 11, 4650. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oyama, S.; Niimi, N.; Mori, M.; Hirata, H. Intra-Articular Ultrasonography Probe for Minimally Invasive Upper Extremity Arthroscopic Surgery: A Phantom Study. J. Clin. Med. 2023, 12, 5727. https://doi.org/10.3390/jcm12175727
Oyama S, Niimi N, Mori M, Hirata H. Intra-Articular Ultrasonography Probe for Minimally Invasive Upper Extremity Arthroscopic Surgery: A Phantom Study. Journal of Clinical Medicine. 2023; 12(17):5727. https://doi.org/10.3390/jcm12175727
Chicago/Turabian StyleOyama, Shintaro, Nobuo Niimi, Masato Mori, and Hitoshi Hirata. 2023. "Intra-Articular Ultrasonography Probe for Minimally Invasive Upper Extremity Arthroscopic Surgery: A Phantom Study" Journal of Clinical Medicine 12, no. 17: 5727. https://doi.org/10.3390/jcm12175727
APA StyleOyama, S., Niimi, N., Mori, M., & Hirata, H. (2023). Intra-Articular Ultrasonography Probe for Minimally Invasive Upper Extremity Arthroscopic Surgery: A Phantom Study. Journal of Clinical Medicine, 12(17), 5727. https://doi.org/10.3390/jcm12175727