
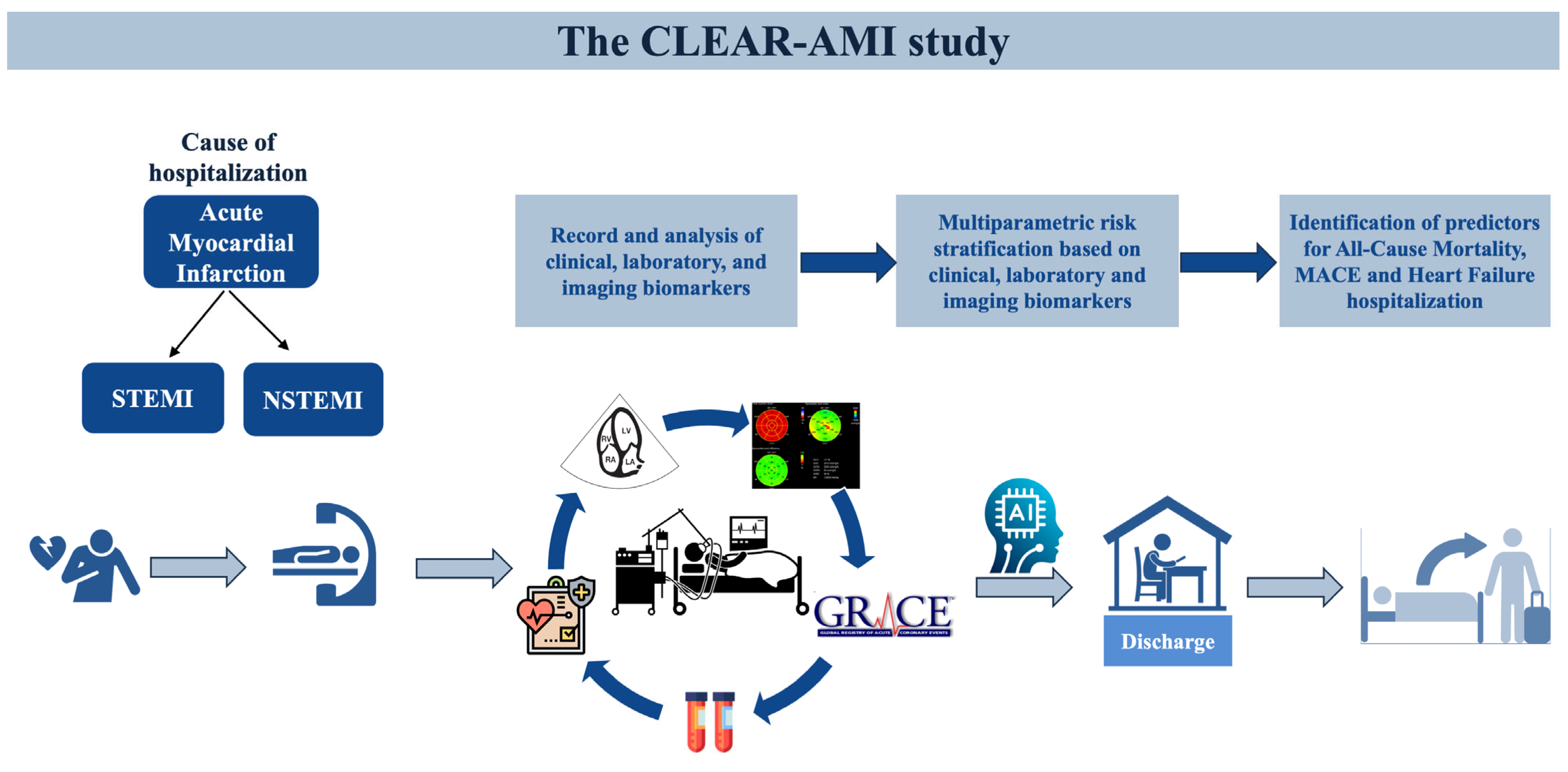
Prognostic Implications of Clinical, Laboratory and Echocardiographic Biomarkers in Patients with Acute Myocardial Infarction—Rationale and Design of the ‘‘CLEAR-AMI Study’’


 ,
,  , ,
, ,  , ,
, , 
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
Study Design and Population
3. Data Collection and Study Procedures
3.1. Echocardiographic Analysis
3.2. Statistical Analysis
4. Discussion and Expected Results
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AMI | acute myocardial infarction |
| NSTEMI | Non-ST-segment elevation myocardial infarction |
| STEMI | ST-segment elevation myocardial infarction |
| GLS | global longitudinal strain |
| GRACE | Global Registry of Acute Coronary Events |
| SYNTAX | Synergy Between Percutaneous Coronary Intervention with Taxus and Coronary Artery Bypass Graft Surgery |
| ΤΙΜΙ | Thrombolysis in Myocardial Infarction |
| LVGCW | left ventricle global constructive work |
| LVGWW | left ventricle global wasted work |
| LV | left ventricle |
| LVEF | left ventricular ejection fraction |
| RV | right ventricle |
| PADP | pulmonary artery diastolic pressure |
| PAMP | pulmonary artery mean pressure |
| PASP | pulmonary artery systolic pressure |
| MACE | Major Adverse Cardiovascular Event |
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2020, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Vernon, S.T.; Coffey, S.; Bhindi, R.; Hoo, S.Y.S.; I Nelson, G.; Ward, M.R.; Hansen, P.S.; Asrress, K.N.; Chow, C.K.; Celermajer, D.S.; et al. Increasing proportion of ST elevation myocardial infarction patients with coronary atherosclerosis poorly explained by standard modifiable risk factors. Eur. J. Prev. Cardiol. 2017, 24, 1824–1830. [Google Scholar] [CrossRef] [PubMed]
- Frangogiannis, N.G. The inflammatory response in myocardial injury, repair, and remodelling. Nat. Rev. Cardiol. 2014, 11, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Russo, I.; Frangogiannis, N.G. Inflammation as a therapeutic target in myocardial infarction: Learning from past failures to meet future challenges. Transl. Res. 2016, 167, 152–166. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Progress and challenges in translating the biology of atherosclerosis. Nature 2011, 473, 317–325. [Google Scholar] [CrossRef]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC: Cardiovasc. Imaging 2018, 11 Pt 1, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Munk, K.; Andersen, N.H.; Terkelsen, C.J.; Bibby, B.M.; Johnsen, S.P.; Bøtker, H.E.; Nielsen, T.T.; Poulsen, S.H. Global left ventricular longitudinal systolic strain for early risk assessment in patients with acute myocardial infarction treated with primary percutaneous intervention. J. Am. Soc. Echocardiogr. 2012, 25, 644–651. [Google Scholar] [CrossRef]
- Antoni, M.L.; Mollema, S.A.; Delgado, V.; Atary, J.Z.; Borleffs, C.J.; Boersma, E.; Holman, E.R.; van der Wall, E.E.; Schalij, M.J.; Bax, J.J. Prognostic importance of strain and strain rate after acute myocardial infarction. Eur. Heart J. 2010, 31, 1640–1647. [Google Scholar] [CrossRef]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.H.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure-strain loop area: A non-invasive index of myocardial work. Eur. Heart J. 2012, 33, 724–733. [Google Scholar] [CrossRef]
- Butcher, S.C.; Fortuni, F.; Montero-Cabezas, J.M.; Abou, R.; El Mahdiui, M.; van der Bijl, P.; van der Velde, E.T.; Ajmone Marsan, N.; Bax, J.J.; Delgado, V. Right ventricular myocardial work: Proof-of-concept for non-invasive assessment of right ventricular function. Eur. Heart J. Cardiovasc. Imaging 2021, 22, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Gerber, Y.; Weston, S.A.; Enriquez-Sarano, M.; Jaffe, A.S.; Manemann, S.M.; Jiang, R.; Roger, V.L. Contemporary Risk Stratification After Myocardial Infarction in the Community: Performance of Scores and Incremental Value of Soluble Suppression of Tumorigenicity-2. J. Am. Heart Assoc. 2017, 6, e005958. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed]
- Chen, T.; Guestrin, C. XGBoost: A scalable tree boosting system. In Proceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography the European Association of Cardiovascular Imaging . Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2016, 17, 1321–1360. [Google Scholar] [CrossRef]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; Hua, L.; Handschumacher, M.D.; Chandrasekaran, K.; Solomon, S.D.; Louie, E.K.; Schiller, N.B. Guidelines for the echocardiographic assessment of the right heart in adults: A report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J. Am. Soc. Echocardiogr. 2010, 23, 685–713, quiz 786–788. [Google Scholar]
- Aduen, J.F.; Castello, R.; Lozano, M.M.; Hepler, G.N.; Keller, C.A.; Alvarez, F.; Safford, R.E.; Crook, J.E.; Heckman, M.G.; Burger, C.D. An alternative echocardiographic method to estimate mean pulmonary artery pressure: Diagnostic and clinical implications. J. Am. Soc. Echocardiogr. 2009, 22, 814–819. [Google Scholar] [CrossRef]
- Lustosa, R.P.; Butcher, S.C.; van der Bijl, P.; El Mahdiui, M.; Montero-Cabezas, J.M.; Kostyukevich, M.V.; Rocha De Lorenzo, A.; Knuuti, J.; Ajmone Marsan, N.; Bax, J.J.; et al. Global Left Ventricular Myocardial Work Efficiency and Long-Term Prognosis in Patients After ST-Segment-Elevation Myocardial Infarction. Circ. Cardiovasc. Imaging 2021, 14, e012072. [Google Scholar] [CrossRef]
- Butcher, S.C.; Lustosa, R.P.; Abou, R.; Marsan, N.A.; Bax, J.J.; Delgado, V. Prognostic implications of left ventricular myocardial work index in patients with ST-segment elevation myocardial infarction and reduced left ventricular ejection fraction. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 699–707. [Google Scholar] [CrossRef]
- Keskin, M.; Uzun, A.O.; Hayıroğlu, M.; Kaya, A.; Çınar, T.; Kozan, Ö. The association of right ventricular dysfunction with in-hospital and 1-year outcomes in anterior myocardial infarction. Int. J. Cardiovasc. Imaging 2019, 35, 77–85. [Google Scholar] [CrossRef]
- Engström, A.E.; Vis, M.M.; Bouma, B.J.; van den Brink, R.B.; Baan, J., Jr.; Claessen, B.E.; Kikkert, W.J.; Sjauw, K.D.; Meuwissen, M.; Koch, K.T.; et al. Right ventricular dysfunction is an independent predictor for mortality in ST- elevation myocardial infarction patients presenting with cardiogenic shock on admission. Eur. J. Heart Fail. 2010, 12, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Anavekar, N.S.; Skali, H.; Bourgoun, M.; Ghali, J.K.; Kober, L.; Maggioni, A.P.; McMurray, J.J.; Velazquez, E.; Califf, R.; Pfeffer, M.A.; et al. Usefulness of right ventricular fractional area change to predict death, heart failure, and stroke following myocardial infarction (from the VALIANT ECHO Study). Am. J. Cardiol. 2008, 101, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Park, J.J.; Park, J.B.; Cho, G.Y. Prognostic Value of Biventricular Strain in Risk Stratifying in Patients with Acute Heart Failure. J. Am. Heart Assoc. 2018, 7, e009331. [Google Scholar] [CrossRef] [PubMed]
- Bosch, L.; Lam, C.S.P.; Gong, L.; Chan, S.P.; Sim, D.; Yeo, D.; Jaufeerally, F.; Leong, K.T.G.; Ong, H.Y.; Ng, T.P.; et al. Right ventricular dysfunction in left- sided heart failure with preserved versus reduced ejection fraction. Eur. J. Heart Fail. 2017, 19, 1664–1671. [Google Scholar] [CrossRef] [PubMed]
- Antoni, M.L.; Scherptong, R.W.; Atary, J.Z.; Boersma, E.; Holman, E.R.; van der Wall, E.E.; Schalij, M.J.; Bax, J.J. Prognostic value of right ventricular function in patients after acute myocardial infarction treated with primary percutaneous coronary intervention. Circ. Cardiovasc. Imaging 2010, 3, 264–271. [Google Scholar] [CrossRef]
- Radwan, H.; Hussein, E.M.; Refaat, H. Short- and long-term prognostic value of right ventricular function in patients with first acute ST elevation myocardial infarction treated by primary angioplasty. Echocardiography 2021, 38, 249–260. [Google Scholar] [CrossRef]
- Park, S.J.; Park, J.H.; Lee, H.S.; Kim, M.S.; Park, Y.K.; Park, Y.; Kim, Y.J.; Lee, J.H.; Choi, S.W.; Jeong, J.O.; et al. Impaired RV global longitudinal strain is associated with poor long-term clinical outcomes in patients with acute inferior STEMI. JACC Cardiovasc. Imaging 2015, 8, 161–169. [Google Scholar] [CrossRef]
- Entman, M.L.; Smith, C.W. Postreperfusion inflammation: A model for reaction to injury in cardiovascular disease. Cardiovasc. Res. 1994, 28, 1301–1311. [Google Scholar] [CrossRef]
- Frangogiannis, N.G.; Smith, C.W.; Entman, M.L. The inflammatory response in myocardial infarction. Cardiovasc. Res. 2002, 53, 31–47. [Google Scholar] [CrossRef]
- Ong, S.-B.; Hernandez-Resendiz, S.; Crespo-Avilan, G.E.; Mukhametshina, R.T.; Kwek, X.-Y.; Cabrera-Fuentes, H.A.; Hausenloy, D.J. Inflammation following acute myocardial infarction: Multiple players, dynamic roles, and novel therapeutic opportunities. PharmacolTher 2018, 186, 73–87. [Google Scholar] [CrossRef]
- Tiller, C.; Reindl, M.; Holzknecht, M.; Lechner, I.; Schwaiger, J.; Brenner, C.; Mayr, A.; Klug, G.; Bauer, A.; Metzler, B.; et al. Association of plasma interleukin-6 with infarct size, reperfusion injury, and adverse remodelling after ST-elevation myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2022, 11, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Stalikas, N.; Papazoglou, A.S.; Karagiannidis, E.; Panteris, E.; Moysidis, D.; Daios, S.; Anastasiou, V.; Patsiou, V.; Koletsa, T.; Sofidis, G.; et al. Association of stress induced hyperglycemia with angiographic findings and clinical outcomes in patients with ST-elevation myocardial infarction. Cardiovasc. Diabetol. 2022, 21, 140. [Google Scholar] [CrossRef]
- Oprescu, N.; Micheu, M.M.; Scafa-Udriste, A.; Popa-Fotea, N.-M.; Dorobantu, M. Inflammatory markers in acute myocardial infarction and the correlation with the severity of coronary heart disease. Ann. Med. 2021, 53, 1041–1047. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Liu, E.; Morrow, D.A.; Heller, E.; McCarroll, R.; Wiegand, R.; Berriz, G.F.; Roth, F.P.; Gerszten, R.E.; R, M.; et al. Metabolomic identification of novel biomarkers of myocardial ischemia. Circulation 2005, 112, 3868–3875. [Google Scholar] [CrossRef]
- Ali, S.E.; Farag, M.A.; Holvoet, P.; Hanafi, R.S.; Gad, M.Z. A Comparative Metabolomics Approach Reveals Early Biomarkers for Metabolic Response to Acute Myocardial Infarction. Sci. Rep. 2016, 6, 36359. [Google Scholar] [CrossRef]
- Seropian, I.M.; Sonnino, C.; Van Tassell, B.W.; Biasucci, L.M.; Abbate, A. Inflammatory markers in ST-elevation acute myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 382–395. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, E.; Moysidis, D.V.; Papazoglou, A.S.; Panteris, E.; Deda, O.; Stalikas, N.; Sofidis, G.; Kartas, A.; Bekiaridou, A.; Giannakoulas, G.; et al. Prognostic significance of metabolomic biomarkers in patients with diabetes mellitus and coronary artery disease. Cardiovasc. Diabetol. 2022, 21, 70. [Google Scholar] [CrossRef] [PubMed]
- Mittas, N.; Chatzopoulou, F.; Kyritsis, K.A.; Papagiannopoulos, C.I.; Theodoroula, N.F.; Papazoglou, A.S.; Karagiannidis, E.; Sofidis, G.; Moysidis, D.V.; Stalikas, N.; et al. A Risk-Stratification Machine Learning Framework for the Prediction of Coronary Artery Disease Severity: Insights From the GESS Trial. Front. Cardiovasc. Med. 2021, 8, 812182. [Google Scholar] [CrossRef]
- Moysidis, D.V.; Daios, S.; Anastasiou, V.; Liatsos, A.C.; Papazoglou, A.S.; Karagiannidis, E.; Kamperidis, V.; Makedou, K.; Thisiadou, A.; Karalazou, P.; et al. Correction: Association of clinical, laboratory and imaging biomarkers with the occurrence of acute myocardial infarction in patients without standard modifiable risk factors—Rationale and design of the “Beyond-SMuRFs Study”. BMC Cardiovasc. Disord. 2023, 23, 207. [Google Scholar] [CrossRef]
- Granger, C.B.; Goldberg, R.J.; Dabbous, O.; Pieper, K.S.; Eagle, K.A.; Cannon, C.P.; Van de Werf, F.; Avezum, A.; Goodman, S.G.; Flather, M.D.; et al. Predictors of hospital mortality in the global registry of acute coronary events. Arch. Intern. Med. 2003, 163, 2345–2353. [Google Scholar] [CrossRef]
- Fox, K.A.A.; FitzGerald, G.; Puymirat, E.; Huang, W.; Carruthers, K.; Simon, T.; Coste, P.; Monsegu, J.; Gabriel Steg, P.; Danchin, N.; et al. Should patients with acute coronary disease be stratified for management according to their risk? Derivation, external validation and outcomes using the updated GRACE risk score. BMJ Open 2014, 4, e004425. [Google Scholar] [CrossRef] [PubMed]
- Karadeniz, M.; Duran, M.; Akyel, A.; Yarlıoğlueş, M.; Öcek, A.H.; Çelik, I.E.; Kılıç, A.; Yalcin, A.A.; Ergün, G.; Murat, S.N. High Sensitive CRP level is associated with intermediate and high syntax score in patients with acute coronary syndrome. Int. Heart J. 2015, 56, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Milano, S.S.; Júnior, O.V.d.M.; Bordin, A.A.S.; Marques, G.L. C-reactive protein is a predictor of mortality in ST-segment elevation acute myocardial infarction. Int. J. Cardiovasc. Sci. 2019, 32, 118–124. [Google Scholar] [CrossRef]
- Raposeiras-Roubín, S.; Pardal, C.B.; Janeiro, B.R.; Abu-Assi, E.; García-Acuña, J.M.; González-Juanatey, J.R. High-sensitivity C-reactive protein is a predictor of in-hospital cardiac events in acute myocardial infarction independently of GRACE risk score. Angiology 2012, 63, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Rauch, B.; Davos, C.H.; Doherty, P.; Saure, D.; Metzendorf, M.-I.; Salzwedel, A.; Völler, H.; Jensen, K.; Schmid, J.-P. The Prognostic Effect of Cardiac Rehabilitation in the Era of Acute Revascularisation and Statin Therapy: A Systematic Review and Meta-Analysis of Randomized and Non-Randomized Studies—The Cardiac Rehabilitation Outcome Study (CROS). Eur. J. Prev. Cardiol. 2016, 23, 1914–1939. [Google Scholar] [CrossRef]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J. Am. Coll. Cardiol. 2016, 67, 1–12. [Google Scholar] [CrossRef]
- Lee, J.-H.; Kim, J.; Sun, B.J.; Jee, S.J.; Park, J.-H. Effect of Cardiac Rehabilitation on Left Ventricular Diastolic Function in Patients with Acute Myocardial Infarction. J. Clin. Med. 2021, 10, 2088. [Google Scholar] [CrossRef]

{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daios, S.; Anastasiou, V.; Moysidis, D.V.; Didagelos, M.; Papazoglou, A.S.; Stalikas, N.; Zegkos, T.; Karagiannidis, E.; Skoura, L.; Kaiafa, G.; et al. Prognostic Implications of Clinical, Laboratory and Echocardiographic Biomarkers in Patients with Acute Myocardial Infarction—Rationale and Design of the ‘‘CLEAR-AMI Study’’. J. Clin. Med. 2023, 12, 5726. https://doi.org/10.3390/jcm12175726
Daios S, Anastasiou V, Moysidis DV, Didagelos M, Papazoglou AS, Stalikas N, Zegkos T, Karagiannidis E, Skoura L, Kaiafa G, et al. Prognostic Implications of Clinical, Laboratory and Echocardiographic Biomarkers in Patients with Acute Myocardial Infarction—Rationale and Design of the ‘‘CLEAR-AMI Study’’. Journal of Clinical Medicine. 2023; 12(17):5726. https://doi.org/10.3390/jcm12175726
Chicago/Turabian StyleDaios, Stylianos, Vasileios Anastasiou, Dimitrios V. Moysidis, Matthaios Didagelos, Andreas S. Papazoglou, Nikolaos Stalikas, Thomas Zegkos, Efstratios Karagiannidis, Lemonia Skoura, Georgia Kaiafa, and et al. 2023. "Prognostic Implications of Clinical, Laboratory and Echocardiographic Biomarkers in Patients with Acute Myocardial Infarction—Rationale and Design of the ‘‘CLEAR-AMI Study’’" Journal of Clinical Medicine 12, no. 17: 5726. https://doi.org/10.3390/jcm12175726
APA StyleDaios, S., Anastasiou, V., Moysidis, D. V., Didagelos, M., Papazoglou, A. S., Stalikas, N., Zegkos, T., Karagiannidis, E., Skoura, L., Kaiafa, G., Makedou, K., Ziakas, A., Savopoulos, C., & Kamperidis, V. (2023). Prognostic Implications of Clinical, Laboratory and Echocardiographic Biomarkers in Patients with Acute Myocardial Infarction—Rationale and Design of the ‘‘CLEAR-AMI Study’’. Journal of Clinical Medicine, 12(17), 5726. https://doi.org/10.3390/jcm12175726